
Novel EVI5::BRAF Gene Fusion in Infantile Fibrosarcoma: A Case Report and Review of Literature

 ,
,
Abstract
1. Introduction
2. Case Presentation
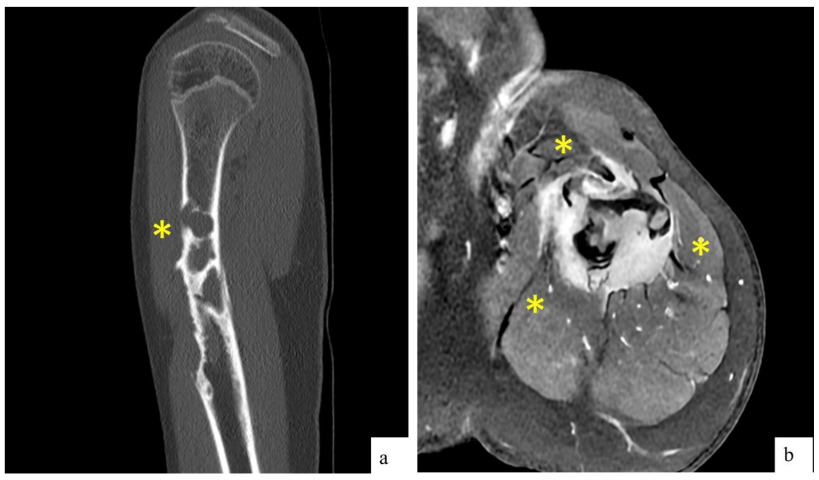
2.1. Clinical and Radiological Findings
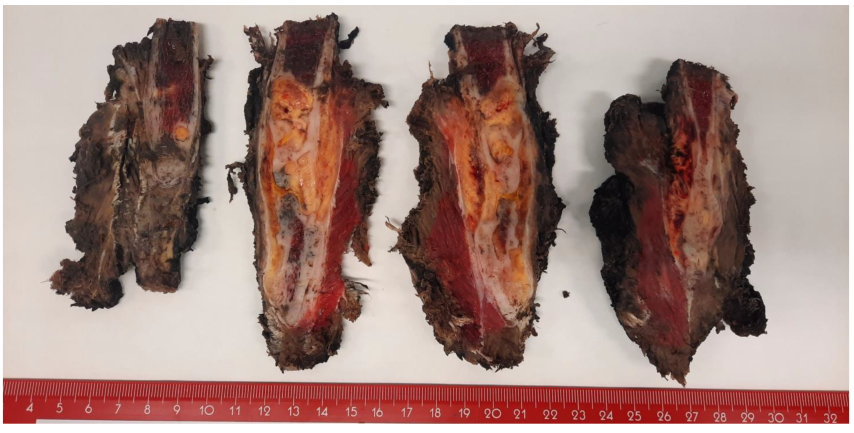
2.2. Macroscopic Findings
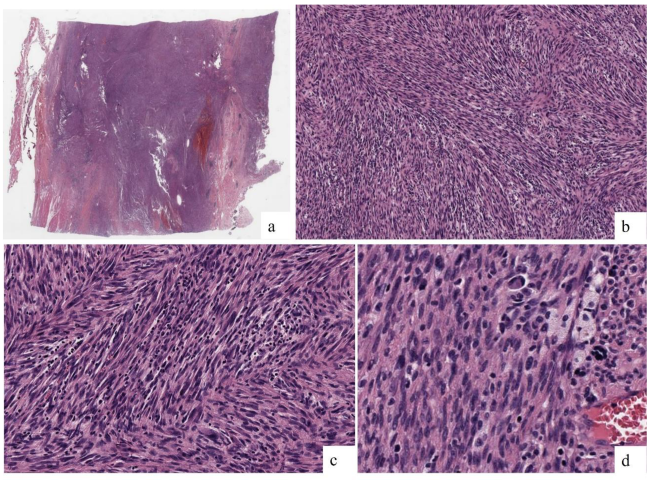
2.3. Microscopic Findings
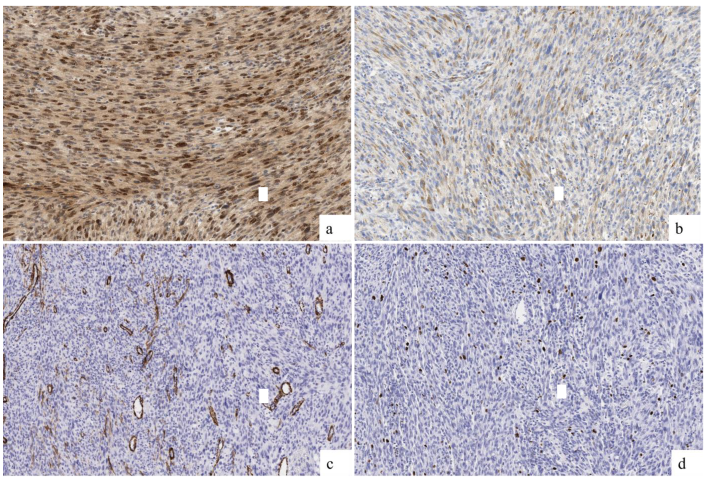
2.4. Immunohistochemical Findings
2.5. Fluorescence In Situ Hybridization (FISH) and Next-Generation Sequencing (NGS) Results
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IFS | Infantile Fibrosarcoma |
| ETV6 | ETS Variant Transcription Factor 6 |
| NTRK3 | Neurotrophic Receptor Tyrosine Kinase 3 |
| NTRK1 | Neurotrophic Receptor Tyrosine Kinase 1 |
| NTRK2 | Neurotrophic Receptor Tyrosine Kinase 2 |
| RET | Rearranged During Transfection Proto-Oncogene |
| MET | MET Proto-Oncogene, Receptor Tyrosine Kinase |
| RAF1 | RAF Proto-Oncogene Serine/Threonine-Protein Kinase 1 |
| BRAF | B-Raf Proto-Oncogene Serine/Threonine-Protein Kinase |
| MRI | Magnetic Resonance Imaging |
| FD | Fibrous Dysplasia |
| ABC | Aneurysmal Bone Cyst |
| ES | Ewing Sarcoma |
| OS | Osteosarcoma |
| CNB | Core Needle Biopsy |
| CT | Computed Tomography |
| MRI | Magnetic Resonance Imaging |
| NCT | Neoadjuvant Chemotherapy |
| NCRT | Neoadjuvant Radiotherapy |
| LGO | Low-Grade Osteosarcoma |
| IMT | Inflammatory Myofibroblastic Tumor |
| NGS | Next-Generation Sequencing |
| SMA | Smooth Muscle Actin |
| FNLCC | Fédération Nationale des Centres de Lutte Contre le Cancer |
| FISH | Fluorescence In Situ Hybridization |
| SEPT7 | Septin 7 |
| SEPT9 | Septin 9 |
| SEPT11 | Septin 11 |
| ERC1 | ELKS/RAB6-Interacting/CAST Family Member 1 |
| PDE10 | Phosphodiesterase 10 |
| CUX1 | Cut-Like Homeobox 1 |
| EVI5 | Ecotropic Viral Integration Site 5 |
| WHO | World Health Organization |
| MDM2 | Mouse Double Minute 2 Homolog |
| ALK | Anaplastic Lymphoma Kinase |
References
- WHO Classification of Tumours Editorial Board. Paediatric Tumours [Internet]. In WHO Classification of Tumours Series, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022; Volume 7, Available online: https://tumourclassification.iarc.who.int/chapters/44 (accessed on 15 August 2024).
- Abualola, R.A.; Al-Zaid, T. KIAA1549-BRAF Gene Fusion Spindle Cell Sarcoma with Infantile Fibrosarcoma-Like Pattern in a Pediatric Patient: A Case Report. Cureus 2024, 16, e51981. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, P.; Liu, W.; Zheng, J.; Zhang, H.; Luo, J. Case report: Primary sarcoma of the mandible with a novel SLMAP-BRAF fusion. Front. Oncol. 2024, 14, 1369046. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cecchi, R.; Guptil, D.; Haslett, N.; Hristov, A.; Bledsoe, J.R.; Tsai, H.; DeWitt, J.; Ferris, S.P. Primary CNS histiocytic sarcoma: Two case reports highlighting a novel MIGA2::BRAF gene fusion and genome-wide DNA methylation profiling results. J. Neuropathol. Exp. Neurol. 2024, 83, 882–886. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, G.; Zheng, H.; Jiang, B.; Ju, Y.; Duan, Q.; An, L.; Shi, H. A rare case of primary central nervous system histiocytic sarcoma harboring a novel ARHGAP45::BRAF fusion: A case report and literature review. Brain Tumor Pathol. 2024, 41, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Penning, A.J.; Al-Ibraheemi, A.; Michal, M.; Larsen, B.T.; Cho, S.J.; Lockwood, C.M.; Paulson, V.A.; Liu, Y.J.; Plank, L.; Fritchie, K.; et al. Novel BRAF gene fusions and activating point mutations in spindle cell sarcomas with histologic overlap with infantile fibrosarcoma. Mod. Pathol. 2021, 34, 1530–1540. [Google Scholar] [CrossRef] [PubMed]
- Gourmel, A.; Rouette, A.; Benlimame, N.; El-Jalbout, R.; Dubé, M.; Théorêt, Y.; Piché, N.; Labonté, S.; Sinnett, D.; Cellot, S.; et al. Durable Response to Trametinib in an Infant with ERC1-BRAF Infantile Fibrosarcoma-Like Tumor: A Case Report and Literature Review of BRAF-Altered Infantile Fibrosarcoma-Like Tumors. JCO Precis. Oncol. 2022, 6, e2200200. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.E.; Correa, H.; Benedetti, D.J.; Smith, B.; Sumegi, J.; Bridge, J. Second Report of PDE10A-BRAF Fusion in Pediatric Spindle Cell Sarcoma with Infantile Fibrosarcoma-Like Morphology Suggesting PDE10A-BRAF Fusion Is a Recurrent Event. Pediatr. Dev. Pathol. 2021, 24, 554–558. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kao, Y.C.; Fletcher, C.D.M.; Alaggio, R.; Wexler, L.; Zhang, L.; Sung, Y.S.; Orhan, D.; Chang, W.C.; Swanson, D.; Dickson, B.C.; et al. Recurrent BRAF Gene Fusions in a Subset of Pediatric Spindle Cell Sarcomas: Expanding the Genetic Spectrum of Tumors with Overlapping Features with Infantile Fibrosarcoma. Am. J. Surg. Pathol. 2018, 42, 28–38. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stelzer, G.; Rosen, R.; Plaschkes, I.; Zimmerman, S.; Twik, M.; Fishilevich, S.; Iny Stein, T.; Nudel, R.; Lieder, I.; Mazor, Y.; et al. The GeneCards Suite: From Gene Data Mining to Disease Genome Sequence Analyses. Curr. Protoc. Bioinform. 2016, 54, 1.30.1–1.30.33. [Google Scholar] [CrossRef] [PubMed]
- Liao, X.; Buchberg, A.M.; Jenkins, N.A.; Copeland, N.G. Evi-5, a common site of retroviral integration in AKXD T-cell lymphomas, maps near Gfi-1 on mouse chromosome 5. J. Virol. 1995, 69, 7132–7137. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cai, T.; Zhou, J.; Zeng, Y.; Du, W.; Zhang, Y.; Liu, T.; Fu, Y.; Huang, J.; Qian, Q.; Zhu, J.; et al. EVI5 is an oncogene that regulates the proliferation and metastasis of NSCLC cells. J. Exp. Clin. Cancer Res. 2020, 39, 84. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Ou, J.; Xu, C.; Yi, C.; Xue, F.; Xu, L.; Lai, F.; Tang, J.; Li, S.; Kang, T.; et al. EVI5 is a novel independent prognostic predictor in hepatocellular carcinoma after radical hepatectomy. Oncol. Rep. 2017, 38, 2251–2258. [Google Scholar] [CrossRef] [PubMed]
- Vandepoele, K.; Andries, V.; van Roy, F. The NBPF1 promoter has been recruited from the unrelated EVI5 gene before simian radiation. Mol. Biol. Evol. 2009, 26, 1321–1332. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.B.; Polubothu, S.; Bruzos, A.L.; Kelly, G.; Horswell, S.; Sauvadet, A.; Bryant, D.; Zecchin, D.; Riachi, M.; Michailidis, F.; et al. Mosaic BRAF Fusions Are a Recurrent Cause of Congenital Melanocytic Nevi Targetable by MAPK Pathway Inhibition. J. Investig. Dermatol. 2024, 144, 593–600.e7. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, S.; Schmitz, F.; Krieger, A.; Reichardt, B. Appearance of recurrent adult fibrosarcoma of the soft tissue and loco-regional post-treatment changes on MRI follow-up. Eur. J. Plast. Surg. 2021, 44, 97–102. [Google Scholar] [CrossRef]
- Basirinia, G.; Ali, M.; Comelli, A.; Sperandeo, A.; Piana, S.; Alongi, P.; Longo, C.; Di Raimondo, D.; Tuttolomondo, A.; Benfante, V. Theranostic Approaches for Gastric Cancer: An Overview of In Vitro and In Vivo Investigations. Cancers 2024, 16, 3323. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Source | Clone | Staining Pattern |
|---|---|---|---|
| S100 | Dako | Polyclonal | Diffuse (Nuclear) |
| SATB2 | Zeta | ZR167 | Diffuse (Nuclear) |
| Caldesmon | Dako | h_CD | Negative |
| Smooth Muscle Actin | Dako | HHF-35 | Negative |
| Desmin | Dako | D33 | Negative |
| Osteonectin | Leica | G-15-G12 | Focal (Cytoplasmic) |
| GFAP | Dako | Polyclonal | Negative |
| SOX10 | Biocare | BC34 | Negative |
| MelanA | Dako | A103 | Negative |
| HMB45 | Dako | HMB-45 | Negative |
| H3K27me3 | Gennova/Biocare | C36B11 | Not evaluable |
| Ki67 | Dako | MIB-1 | 7% |
| ALK | Dako | ALK1 | Negative |
| Age | Sex | Site | S100 | SMA | SATB2 | Ki67 | Mt | Genetics | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 14 | Male | Left humerus | Weak, focal | Negative | Intense, difusse | 7% | No | EVI5::BRAF | Resection and reconstruction | No evidence of disease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-López, J.; Rubio-Martínez, L.A.; Atarés, M.; Amaya, J.V.; Huart, M.C.; Mayordomo-Aranda, E.; Giner, F. Novel EVI5::BRAF Gene Fusion in Infantile Fibrosarcoma: A Case Report and Review of Literature. Int. J. Mol. Sci. 2025, 26, 1182. https://doi.org/10.3390/ijms26031182
González-López J, Rubio-Martínez LA, Atarés M, Amaya JV, Huart MC, Mayordomo-Aranda E, Giner F. Novel EVI5::BRAF Gene Fusion in Infantile Fibrosarcoma: A Case Report and Review of Literature. International Journal of Molecular Sciences. 2025; 26(3):1182. https://doi.org/10.3390/ijms26031182
Chicago/Turabian StyleGonzález-López, Judith, Luis Alberto Rubio-Martínez, Miryam Atarés, José Vicente Amaya, Maria Carmen Huart, Empar Mayordomo-Aranda, and Francisco Giner. 2025. "Novel EVI5::BRAF Gene Fusion in Infantile Fibrosarcoma: A Case Report and Review of Literature" International Journal of Molecular Sciences 26, no. 3: 1182. https://doi.org/10.3390/ijms26031182
APA StyleGonzález-López, J., Rubio-Martínez, L. A., Atarés, M., Amaya, J. V., Huart, M. C., Mayordomo-Aranda, E., & Giner, F. (2025). Novel EVI5::BRAF Gene Fusion in Infantile Fibrosarcoma: A Case Report and Review of Literature. International Journal of Molecular Sciences, 26(3), 1182. https://doi.org/10.3390/ijms26031182