
Assessing Urinary Para-Hydroxyphenylacetic Acid as a Biomarker Candidate in Neuroendocrine Neoplasms

 ,
,  , , , ,
, , , ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Results
2.1. Population Characteristics and Death Outcome
2.2. Differences in Biochemical Markers Levels
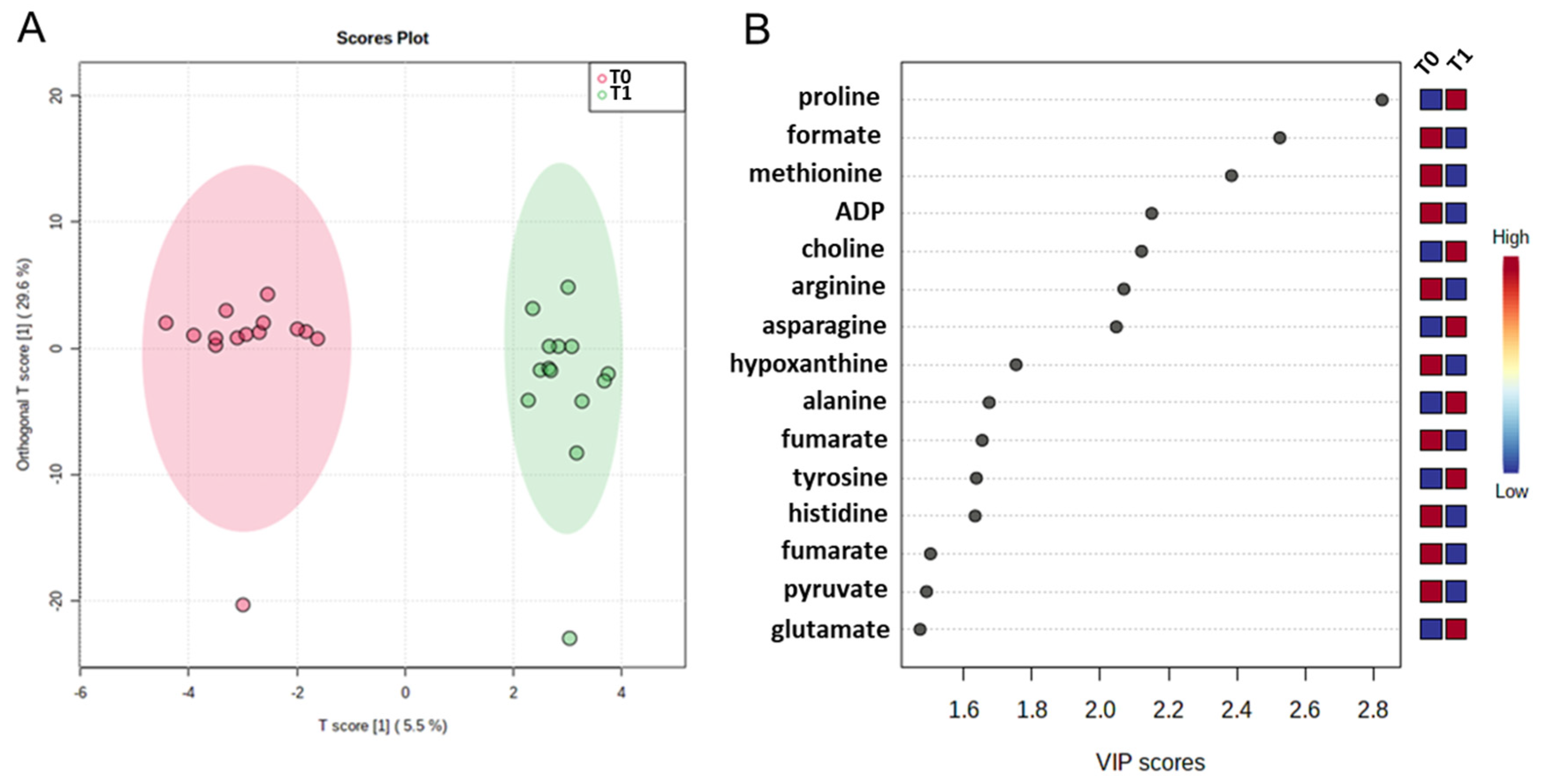
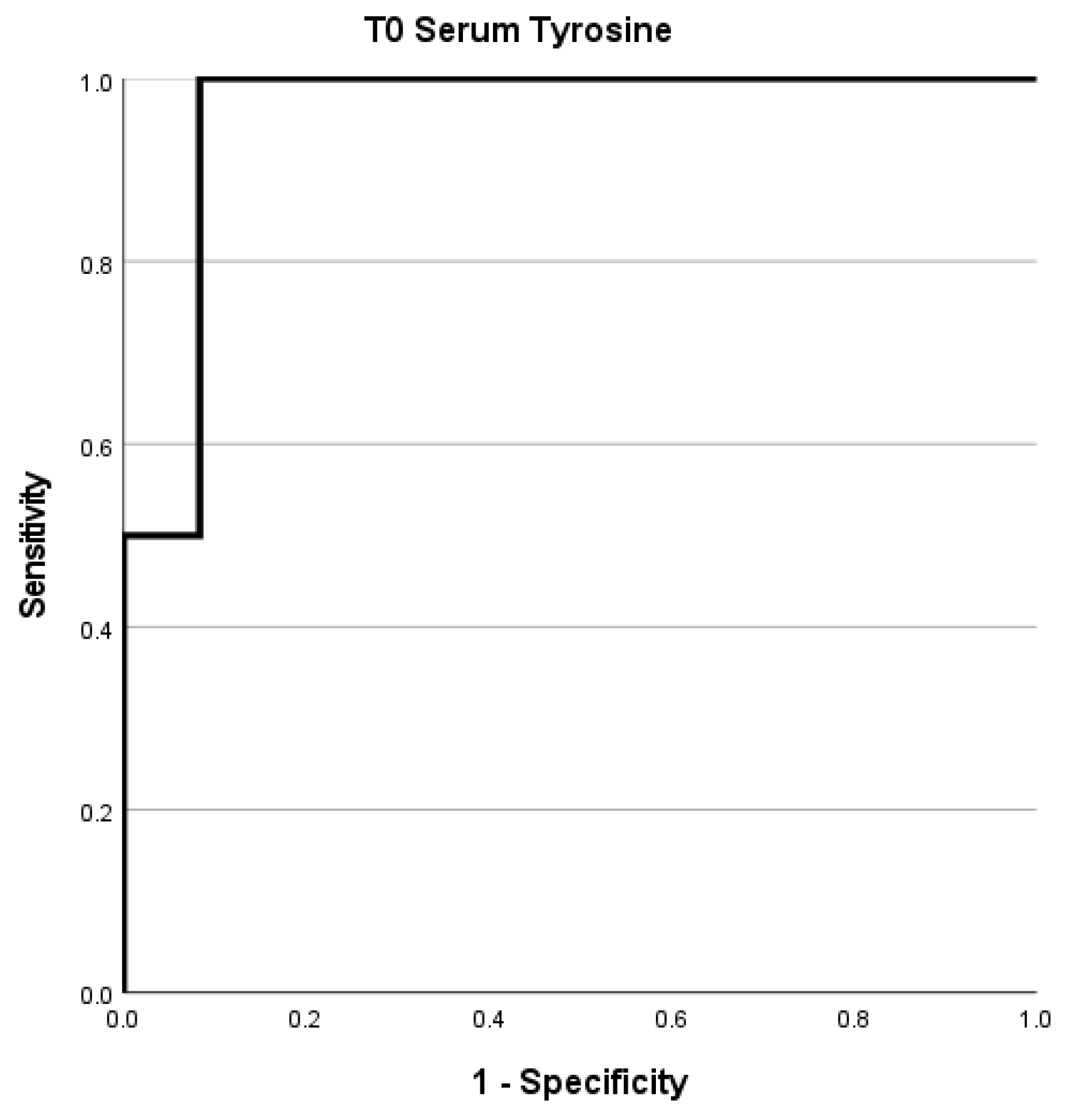
2.3. Metabolomic Profiling: The Role of Tyrosine
3. Discussion
4. Materials and Methods
4.1. Study Population and Sample Collection
4.2. Biochemical Markers
4.3. Serum 1H-NMR Spectroscopy and Data Processing
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Modlin, I.M.; Oberg, K.; Chung, D.C.; Jensen, R.T.; de Herder, W.W.; Thakker, R.V.; Caplin, M.; Delle Fave, G.; Kaltsas, G.A.; Krenning, E.P.; et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008, 9, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed]
- Bartolomei, M.; Berruti, A.; Falconi, M.; Fazio, N.; Ferone, D.; Lastoria, S.; Pappagallo, G.; Seregni, E.; Versari, A. Clinical Management of Neuroendocrine Neoplasms in Clinical Practice: A Formal Consensus Exercise. Cancers 2022, 14, 2501. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. Endocrine and Neuroendocrine Tumours, Volume 8. Available online: https://tumourclassification.iarc.who.int (accessed on 4 January 2024).
- Kulke, M.H.; Mayer, R.J. Carcinoid tumors. N. Engl. J. Med. 1999, 340, 858–868. [Google Scholar] [CrossRef]
- Marotta, V.; Zatelli, M.; Sciammarella, C.; Ambrosio, M.; Bondanelli, M.; Colao, A.; Faggiano, A. Chromogranin A as circulating marker for diagnosis and management of neuroendocrine neoplasms: More flaws than fame. Endocr.-Relat. Cancer 2018, 25, 18. [Google Scholar] [CrossRef]
- Oberg, K.; Couvelard, A.; Delle Fave, G.; Gross, D.; Grossman, A.; Jensen, R.T.; Pape, U.F.; Perren, A.; Rindi, G.; Ruszniewski, P.; et al. ENETS Consensus Guidelines for Standard of Care in Neuroendocrine Tumours: Biochemical Markers. Neuroendocrinology 2017, 105, 201–211. [Google Scholar] [CrossRef]
- Lenchner, J.R.; Santos, C. Biochemistry, 5 Hydroxyindoleacetic Acid. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Quaedvlieg, P.F.; Lamers, C.B.; Taal, B.G. Carcinoid heart disease: An update. Scand. J. Gastroenterol. Suppl. 2002, 37, 66–71. [Google Scholar] [CrossRef]
- Zuetenhorst, J.M.; Bonfrer, J.M.; Korse, C.M.; Bakker, R.; van Tinteren, H.; Taal, B.G. Carcinoid heart disease: The role of urinary 5-hydroxyindoleacetic acid excretion and plasma levels of atrial natriuretic peptide, transforming growth factor-beta and fibroblast growth factor. Cancer 2003, 97, 1609–1615. [Google Scholar] [CrossRef]
- Khan, M.S.; Caplin, M.E. The use of biomarkers in neuroendocrine tumours. Frontline Gastroenterol. 2013, 4, 175–181. [Google Scholar] [CrossRef]
- Nobels, F.R.; Kwekkeboom, D.J.; Coopmans, W.; Schoenmakers, C.H.; Lindemans, J.; De Herder, W.W.; Krenning, E.P.; Bouillon, R.; Lamberts, S.W. Chromogranin A as serum marker for neuroendocrine neoplasia: Comparison with neuron-specific enolase and the alpha-subunit of glycoprotein hormones. J. Clin. Endocrinol. Metab. 1997, 82, 2622–2628. [Google Scholar] [CrossRef]
- Russo, L.; Grilli, B.; Minopoli, A.; Capozzi, M.; Tafuto, S.; Correra, M.; Trillo, G.; Isgro, M.A.; Cavalcanti, E. A potential prognostic marker in primitive lung neuroendocrine tumor: A case report. Int. J. Biol. Markers 2020, 35, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Soldevilla, B.; Lopez-Lopez, A.; Lens-Pardo, A.; Carretero-Puche, C.; Lopez-Gonzalvez, A.; La Salvia, A.; Gil-Calderon, B.; Riesco-Martinez, M.C.; Espinosa-Olarte, P.; Sarmentero, J.; et al. Comprehensive Plasma Metabolomic Profile of Patients with Advanced Neuroendocrine Tumors (NETs). Diagnostic and Biological Relevance. Cancers 2021, 13, 2634. [Google Scholar] [CrossRef] [PubMed]
- La Salvia, A.; Lens-Pardo, A.; Lopez-Lopez, A.; Carretero-Puche, C.; Capdevila, J.; Benavent, M.; Jimenez-Fonseca, P.; Castellano, D.; Alonso, T.; Teule, A.; et al. Metabolomic profile of neuroendocrine tumors identifies methionine, porphyrin, and tryptophan metabolisms as key dysregulated pathways associated with patient survival. Eur. J. Endocrinol. 2024, 190, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Manoharan, J.; Bollmann, C.; Kann, P.H.; Di Fazio, P.; Bartsch, D.K.; Albers, M.B. Gender Differences in Multiple Endocrine Neoplasia Type 1: Implications for Screening? Visc. Med. 2020, 36, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.; Oberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A.; ESMO Guidelines Committee. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Baudin, E.; Gigliotti, A.; Ducreux, M.; Ropers, J.; Comoy, E.; Sabourin, J.C.; Bidart, J.M.; Cailleux, A.F.; Bonacci, R.; Ruffie, P.; et al. Neuron-specific enolase and chromogranin A as markers of neuroendocrine tumours. Br. J. Cancer 1998, 78, 1102–1107. [Google Scholar] [CrossRef]
- Tirosh, A.; Nilubol, N.; Patel, D.; Kebebew, E. Prognostic Utility of 24-Hour Urinary 5-HIAA Doubling Time in Patients with Neuroendocrine Tumors. Endocr. Pract. 2018, 24, 710–717. [Google Scholar] [CrossRef]
- Tsai, H.J.; Hsiao, C.F.; Chang, J.S.; Chen, L.T.; Chao, Y.J.; Yen, C.J.; Shan, Y.S. The Prognostic and Predictive Role of Chromogranin A in Gastroenteropancreatic Neuroendocrine Tumors—A Single-Center Experience. Front. Oncol. 2021, 11, 741096. [Google Scholar] [CrossRef]
- Yu, F.; Fu, J.; Zhang, C.; Wu, W.; Ai, S.; Yao, X.; Meng, Q.; Huang, Y.; Lu, G.; Wang, F.; et al. Use of Chromogranin A for Monitoring Patients with Pancreatic Neuroendocrine Neoplasms. Pancreas 2021, 50, 882–889. [Google Scholar] [CrossRef]
- Arnold, R.; Wilke, A.; Rinke, A.; Mayer, C.; Kann, P.H.; Klose, K.J.; Scherag, A.; Hahmann, M.; Muller, H.H.; Barth, P. Plasma chromogranin A as marker for survival in patients with metastatic endocrine gastroenteropancreatic tumors. Clin. Gastroenterol. Hepatol. 2008, 6, 820–827. [Google Scholar] [CrossRef]
- Chatani, P.D.; Aversa, J.G.; McDonald, J.D.; Khan, T.M.; Keutgen, X.M.; Nilubol, N. Preoperative serum chromogranin-a is predictive of survival in locoregional jejuno-ileal small bowel neuroendocrine tumors. Surgery 2021, 170, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Dodd, D.; Spitzer, M.H.; Van Treuren, W.; Merrill, B.D.; Hryckowian, A.J.; Higginbottom, S.K.; Le, A.; Cowan, T.M.; Nolan, G.P.; Fischbach, M.A.; et al. A gut bacterial pathway metabolizes aromatic amino acids into nine circulating metabolites. Nature 2017, 551, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.A.; Macfarlane, G.T. Enumeration of human colonic bacteria producing phenolic and indolic compounds: Effects of pH, carbohydrate availability and retention time on dissimilatory aromatic amino acid metabolism. J. Appl. Bacteriol. 1996, 81, 288–302. [Google Scholar] [CrossRef] [PubMed]
- Russell, W.R.; Hoyles, L.; Flint, H.J.; Dumas, M.E. Colonic bacterial metabolites and human health. Curr. Opin. Microbiol. 2013, 16, 246–254. [Google Scholar] [CrossRef]
- Wiggins, T.; Kumar, S.; Markar, S.R.; Antonowicz, S.; Hanna, G.B. Tyrosine, phenylalanine, and tryptophan in gastroesophageal malignancy: A systematic review. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 32–38. [Google Scholar] [CrossRef]
- Miyagi, Y.; Higashiyama, M.; Gochi, A.; Akaike, M.; Ishikawa, T.; Miura, T.; Saruki, N.; Bando, E.; Kimura, H.; Imamura, F.; et al. Plasma free amino acid profiling of five types of cancer patients and its application for early detection. PLoS ONE 2011, 6, e24143. [Google Scholar] [CrossRef]
- Zhang, X.; Xu, L.; Shen, J.; Cao, B.; Cheng, T.; Zhao, T.; Liu, X.; Zhang, H. Metabolic signatures of esophageal cancer: NMR-based metabolomics and UHPLC-based focused metabolomics of blood serum. Biochim. Biophys. Acta 2013, 1832, 1207–1216. [Google Scholar] [CrossRef]
- Adams, C.D.; Richmond, R.; Ferreira, D.L.S.; Spiller, W.; Tan, V.; Zheng, J.; Wurtz, P.; Donovan, J.; Hamdy, F.; Neal, D.; et al. Circulating Metabolic Biomarkers of Screen-Detected Prostate Cancer in the ProtecT Study. Cancer Epidemiol. Biomarkers Prev. 2019, 28, 208–216. [Google Scholar] [CrossRef]
- Grilli, B.; Russo, L.; Barchiesi, V.; Minopoli, A.; Gelzo, M.; Tafuto, S.; De Divitiis, C.; Capozzi, M.; Corso, G.; Cavalcanti, E. Implementation of a Hplc Method for the Evaluation of Urinary 4-Hydroxyphenylacetic Acid in Patients with Neuroendocrine Tumors. Clin. Oncol. Res. 2020, 2, 1–5. [Google Scholar] [CrossRef]
- Pang, Z.; Chong, J.; Zhou, G.; de Lima Morais, D.A.; Chang, L.; Barrette, M.; Gauthier, C.; Jacques, P.E.; Li, S.; Xia, J. MetaboAnalyst 5.0: Narrowing the gap between raw spectra and functional insights. Nucleic Acids Res. 2021, 49, W388–W396. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 14) |
|---|---|
| Age, median (IQR) | 53 (40–61) |
| Gender, n (%) | |
| Female | 11 (79%) |
| Male | 3 (21%) |
| Localization, n (%) | |
| Breast | 1 (7.1%) |
| Extrasurrenalic Paraganglioma | 1 (7.1%) |
| Gastrointestinal | 8 (64%) |
| Lung | 1 (14%) |
| Ovary | 1 (7.1%) |
| BMI, n (%) | |
| <25 | 9 (64%) |
| >25 | 5 (36%) |
| Metastasis, n (%) | |
| No | 6 (43%) |
| Yes | 8 (57%) |
| Outcome, n (%) | |
| Alive | 12 (85.7%) |
| Dead | 2 (14.3%) |
| Patient ID | u-5-HIAA (mg/24 h) | u-pHPAA (µmol/mmol Ucreat) | s-CgA (ng/mL) | s-NSE (ng/mL) | Outcome | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T1/T0 | T0 | T1 | T1/T0 | T0 | T1 | T1/T0 | T0 | T1 | T1/T0 | ||
| 1 | 1.6 | 3.8 | 2.37 | 13.0 | 10.0 | 0.77 | 72.5 | 66.7 | 0.92 | 17.2 | 15.9 | 0.92 | No |
| 2 | 1.7 | 3.7 | 2.18 | 5.0 | 5.0 | 1.00 | 133.6 | 640.4 | 4.79 | 10.5 | 10.0 | 0.95 | No |
| 3 | 66.0 | 125.7 | 1.90 | 11.0 | 27.0 | 2.45 | 593.5 | 407.0 | 0.69 | 15.1 | 13.7 | 0.91 | DP |
| 4 | 1.5 | 3.1 | 2.07 | 21.0 | 13.0 | 0.62 | 32.3 | 26.0 | 0.81 | 18.7 | 16.8 | 0.90 | DP |
| 5 | 2.6 | 11.6 | 4.46 | 10.0 | 36.0 | 3.60 | 74.7 | 25.7 | 0.34 | 12.5 | 15.3 | 1.22 | No |
| 6 | 109.7 | 130.0 | 1.19 | 19.0 | 133.0 | 7.00 | 4550.0 | 6862.0 | 1.51 | 15.4 | 17.4 | 1.13 | Death |
| 7 | 3.9 | 2.6 | 0.67 | 5.0 | 7.0 | 1.40 | 43.0 | 63.1 | 1.47 | 11.9 | 18.5 | 1.55 | DP |
| 8 | 2.7 | 5.2 | 1.96 | 5.0 | 7.0 | 1.40 | 380.3 | 113.0 | 0.30 | 32.4 | 25.6 | 0.79 | DP |
| 9 | 2.3 | 3.8 | 1.65 | 23.0 | 5.0 | 0.22 | 735.0 | 238.0 | 0.32 | 9.7 | 10.5 | 1.08 | DP |
| 10 | 4.2 | 0.8 | 0.19 | 5.0 | 15.0 | 3.00 | 130.9 | 26.3 | 0.20 | 15.4 | 28.5 | 1.85 | DP |
| 11 | 3.5 | 5.6 | 1.60 | 6.0 | 11.0 | 1.83 | 124.4 | 30.7 | 0.25 | 11.9 | 12.5 | 1.05 | No |
| 12 | 3.7 | 1.9 | 0.51 | 3.0 | 4.0 | 1.33 | 84.4 | 71.7 | 0.85 | 16.4 | 15.1 | 0.92 | No |
| 13 | 4.6 | 2.1 | 0.46 | 35.0 | 145.0 | 4.14 | 269.0 | 58.2 | 0.22 | 11.7 | 17.9 | 1.53 | DP |
| 14 | 4.4 | 16.5 | 3.75 | 7.0 | 89.0 | 12.71 | 953.3 | 31890.0 | 33.45 | 12.6 | 56.0 | 4.44 | Death |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Falco, R.; Costantini, S.; Russo, L.; Giannascoli, D.; Minopoli, A.; Clemente, O.; Tafuto, S.; Vitagliano, C.; Di Gennaro, E.; Budillon, A.; et al. Assessing Urinary Para-Hydroxyphenylacetic Acid as a Biomarker Candidate in Neuroendocrine Neoplasms. Int. J. Mol. Sci. 2024, 25, 12317. https://doi.org/10.3390/ijms252212317
de Falco R, Costantini S, Russo L, Giannascoli D, Minopoli A, Clemente O, Tafuto S, Vitagliano C, Di Gennaro E, Budillon A, et al. Assessing Urinary Para-Hydroxyphenylacetic Acid as a Biomarker Candidate in Neuroendocrine Neoplasms. International Journal of Molecular Sciences. 2024; 25(22):12317. https://doi.org/10.3390/ijms252212317
Chicago/Turabian Stylede Falco, Renato, Susan Costantini, Luigi Russo, Denise Giannascoli, Anita Minopoli, Ottavia Clemente, Salvatore Tafuto, Carlo Vitagliano, Elena Di Gennaro, Alfredo Budillon, and et al. 2024. "Assessing Urinary Para-Hydroxyphenylacetic Acid as a Biomarker Candidate in Neuroendocrine Neoplasms" International Journal of Molecular Sciences 25, no. 22: 12317. https://doi.org/10.3390/ijms252212317
APA Stylede Falco, R., Costantini, S., Russo, L., Giannascoli, D., Minopoli, A., Clemente, O., Tafuto, S., Vitagliano, C., Di Gennaro, E., Budillon, A., & Cavalcanti, E. (2024). Assessing Urinary Para-Hydroxyphenylacetic Acid as a Biomarker Candidate in Neuroendocrine Neoplasms. International Journal of Molecular Sciences, 25(22), 12317. https://doi.org/10.3390/ijms252212317