
Diagnostic Accuracy of Leucine-Rich α-2-Glycoprotein 1 as a Non-Invasive Salivary Biomarker in Pediatric Appendicitis




Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics and Clinical Data of the Patients
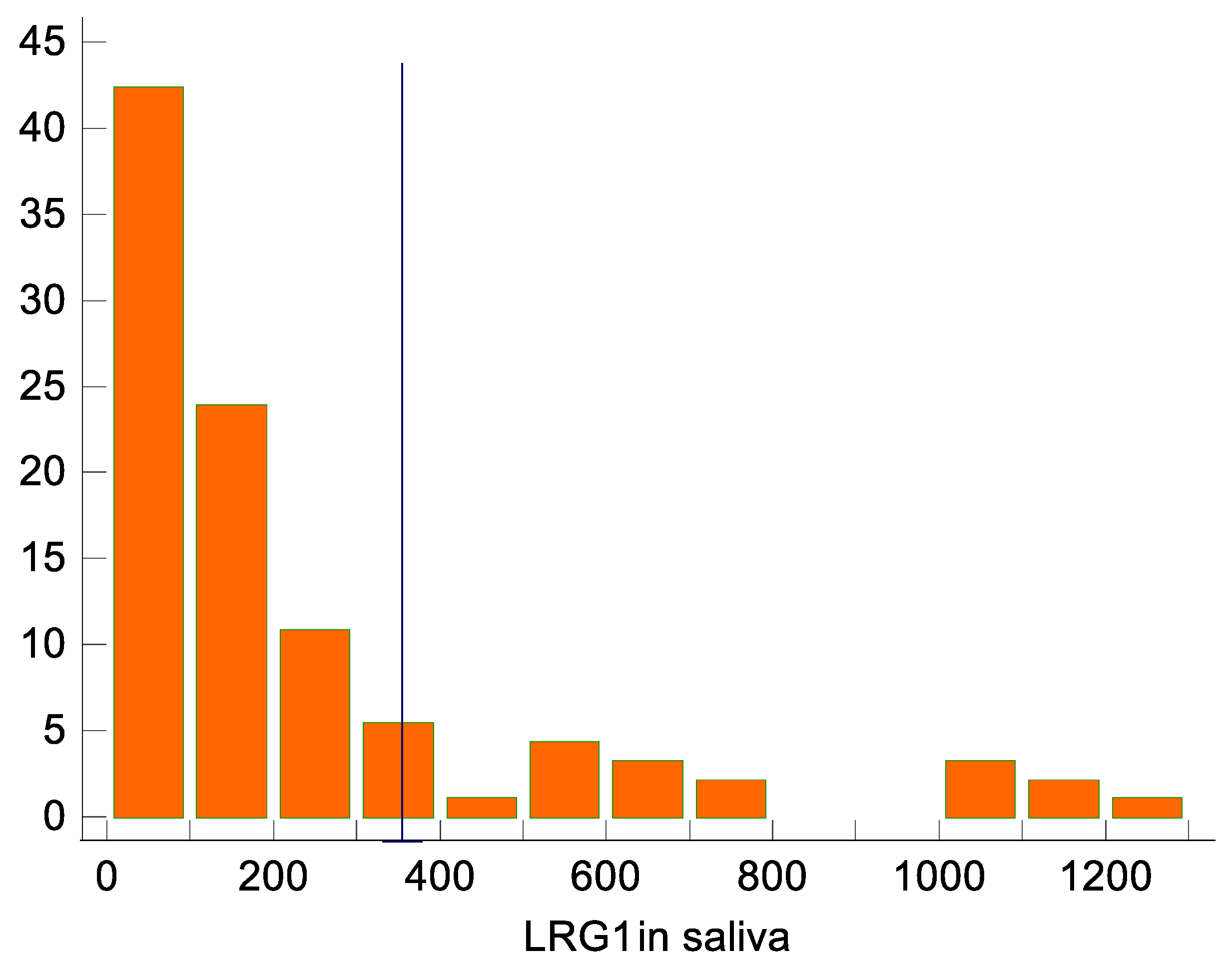
2.2. LRG1 from Saliva as a Biomarker of Acute Appendicitis
2.3. Other Factors Associated with Acute Appendicitis
3. Discussion
4. Materials and Methods
4.1. Study Design and Setting
4.2. Study Protocol
4.3. Blood Collection and Preparation
4.4. Saliva LRG1 Collection
4.5. Saliva LRG1 Analysis
4.6. Final Diagnosis of Patients
4.7. Sample Size Calculation
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pogorelić, Z.; Mihanović, J.; Ninčević, S.; Lukšić, B.; Elezović Baloević, S.; Polašek, O. Validity of appendicitis inflammatory response score in distinguishing perforated from non-perforated appendicitis in children. Children 2021, 8, 309. [Google Scholar] [CrossRef] [PubMed]
- Podany, A.B. Acute appendicitis in pediatric patients: An updated narrative review. J. Clin. Gastroenterol. Treat 2017, 3, 42. [Google Scholar] [CrossRef]
- Glass, C.; Rangel, S. Overview and diagnosis of acute appendicitis in children. Semin. Pediatr. Surg. 2016, 25, 198–203. [Google Scholar] [CrossRef]
- Stringer, M. Acute appendicitis. J. Paediatr. Child Health 2017, 53, 1071–1076. [Google Scholar] [CrossRef]
- Pogorelic, Z.; Buljubasic, M.; Susnjar, T.; Jukic, M.; Pericic, T.P.; Juric, I. Comparison of open and laparoscopic appendectomy in children: A 5-year single center experience. Indian Pediatr. 2019, 56, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Benabbas, R.; Hanna, M.; Shah, J.; Sinert, R. Diagnostic accuracy of history, physical examination, laboratory tests, and point-of-care ultrasound for pediatric acute appendicitis in the emergency department: A systematic review and meta-analysis. Acad. Emerg. Med. 2017, 24, 523–551. [Google Scholar] [CrossRef]
- Bhangu, A.; Søreide, K.; Di Saverio, S.; Assarsson, J.H.; Drake, F.T. Acute appendicitis: Modern understanding of pathogenesis, diagnosis, and management. Lancet 2015, 386, 1278–1287. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Domjanović, J.; Jukić, M.; Poklepović Peričić, T. Acute appendicitis in children younger than five years of age: Diagnostic challenge for pediatric surgeons. Surg. Infect. 2020, 21, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Almaramhy, H.H. Acute appendicitis in young children less than 5 years: Review article. J. Pediatr. 2017, 43, 15. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Anand, S.; Žuvela, T.; Singh, A.; Križanac, Z.; Krishnan, N. Incidence of complicated appendicitis during the COVID-19 pandemic versus the pre-pandemic period: A systematic review and meta-analysis of 2782 pediatric appendectomies. Diagnostics 2022, 12, 127. [Google Scholar] [CrossRef]
- Fahimi, J.; Herring, A.; Harries, A.; Gonzales, R.; Alter, H. Computed tomography use among children presenting to emergency departments with abdominal pain. Pediatrics 2012, 130, e1069–e1075. [Google Scholar] [CrossRef]
- Hryhorczuk, A.L.; Mannix, R.C.; Taylor, G.A. Pediatric abdominal pain: Use of imaging in the emergency department in the United States from 1999 to 2007. Radiology 2012, 263, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Larson, D.B.; Johnson, L.W.; Schnell, B.M.; Goske, M.J.; Salisbury, S.R.; Forman, H.P. Rising use of CT in child visits to the emergency department in the United States, 1995–2008. Radiology 2011, 259, 793–801. [Google Scholar] [CrossRef]
- Ozkan, S.; Duman, A.; Durukan, P.; Yildirim, A.; Ozbakan, O. The accuracy rate of Alvarado score, ultrasonography, and computerized tomography scan in the diagnosis of acute appendicitis in our center. Niger. J. Clin. Pract. 2014, 17, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Čohadžić, T. A bizarre cause of acute appendicitis in a pediatric patient: An ingested tooth. Children 2023, 10, 108. [Google Scholar] [CrossRef] [PubMed]
- Fawkner-Corbett, D.; Hayward, G.; Alkhmees, M.; Van Den Bruel, A.; Ordóñez-Mena, J.M.; Holtman, G.A. Diagnostic accuracy of blood tests of inflammation in paediatric appendicitis: A systematic review and meta-analysis. BMJ Open 2022, 12, e056854. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Lukšić, A.M.; Mihanović, J.; Đikić, D.; Balta, V. Hyperbilirubinemia as an indicator of perforated acute appendicitis in pediatric population: A prospective study. Surg. Infect. 2021, 22, 1064–1071. [Google Scholar] [CrossRef]
- Anand, S.; Krishnan, N.; Birley, J.R.; Tintor, G.; Bajpai, M.; Pogorelić, Z. Hyponatremia-a new diagnostic marker for complicated acute appendicitis in children: A systematic review and meta-analysis. Children 2022, 9, 1070. [Google Scholar] [CrossRef]
- Kharbanda, A.B.; Rai, A.J.; Cosme, Y.; Liu, K.; Dayan, P.S. Novel serum and urine markers for pediatric appendicitis. Acad. Emerg. Med. 2012, 19, 56–62. [Google Scholar] [CrossRef]
- Demirci, O.L.; Cevik, Y.; Corbacioglu, S.K.; Taner, A. Value of Leucine-rich alpha-2-glycoprotein-1 (LRG-1) on diagnosis of acute appendicitis in female patients with right lower-quadrant abdominal pain. J. Pak. Med. Assoc. 2017, 67, 1383–1386. [Google Scholar]
- Kentsis, A.; Ahmed, S.; Kurek, K.; Brennan, E.; Bradwin, G.; Steen, H.; Bachur, R. Detection and diagnostic value of urine leucine-rich α-2-glycoprotein in children with suspected acute appendicitis. Ann. Emerg. Med. 2012, 60, 78–83.e1. [Google Scholar] [CrossRef] [PubMed]
- Rainer, T.; Leung, L.; Chan, C.; Leung, Y.; Cheng, N.; Lai, P.; Cheung, Y.; Graham, C. Circulating human leucine-rich α-2-glycoprotein 1 mRNA and protein levels to detect acute appendicitis in patients with acute abdominal pain. Clin. Biochem. 2017, 50, 485–490. [Google Scholar] [CrossRef]
- Salö, M.; Roth, B.; Stenström, P.; Arnbjörnsson, E.; Ohlsson, B. Urinary biomarkers in pediatric appendicitis. Pediatr. Surg. Int. 2016, 32, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.-L.; Fan, J.D.; Chen, Y.; Ho, M.F.; Choo, C.S.; Allen, J.; Low, Y.; Jacobsen, A.S.; Nah, S.A. A novel noninvasive appendicitis score with a urine biomarker. J. Pediatr. Surg. 2019, 54, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.-L.; Fan, J.D.; Ho, M.F.; Choo, C.S.C.; Ong, L.Y.; Chen, Y. Salivary biomarker for acute appendicitis in children: A pilot study. Pediatr. Surg. Int. 2020, 36, 621–627. [Google Scholar] [CrossRef]
- Lontra, M.B.; Savaris, R.F.; Cavazzola, L.T.; Maissiat, J. Comparison of leucine-rich alpha-2-glycoprotein-1 (LRG-1) plasma levels between patients with and without appendicitis, a case-controlled study. Sci. Rep. 2021, 11, 5574. [Google Scholar] [CrossRef]
- Kakar, M.; Berezovska, M.M.; Broks, R.; Asare, L.; Delorme, M.; Crouzen, E.; Zviedre, A.; Reinis, A.; Engelis, A.; Kroica, J.; et al. Serum and urine biomarker leucine-rich alpha-2 glycoprotein 1 differentiates pediatric acute complicated and uncomplicated appendicitis. Diagnostics 2021, 11, 860. [Google Scholar] [CrossRef] [PubMed]
- Naka, T.; Fujimoto, M. LRG is a novel inflammatory marker clinically useful for the evaluation of disease activity in rheumatoid arthritis and inflammatory bowel disease. Immunol. Med. 2018, 41, 62–67. [Google Scholar] [CrossRef]
- Serada, S.; Fujimoto, M.; Terabe, F.; Iijima, H.; Shinzaki, S.; Matsuzaki, S.; Ohkawara, T.; Nezu, R.; Nakajima, S.; Kobayashi, T.; et al. Serum leucine-rich alpha-2 glycoprotein is a disease activity biomarker in ulcerative colitis. Inflamm. Bowel Dis. 2012, 18, 2169–2179. [Google Scholar] [CrossRef]
- Saito, K.; Tanaka, T.; Kanda, H.; Ebisuno, Y.; Izawa, D.; Kawamoto, S.; Okubo, K.; Miyasaka, M. Gene expression profiling of mucosal addressin cell adhesion molecule-1+ high endothelial venule cells (HEV) and identification of a leucine-rich HEV glycoprotein as a HEV marker. J. Immunol. 2002, 168, 1050–1059. [Google Scholar] [CrossRef]
- Fujimoto, M.; Serada, S.; Suzuki, K.; Nishikawa, A.; Ogata, A.; Nanki, T.; Hattori, K.; Kohsaka, H.; Miyasaka, N.; Takeuchi, T.; et al. Leucine-rich α2 -glycoprotein as a potential biomarker for joint inflammation during anti-interleukin-6 biologic therapy in rheumatoid arthritis. Arthritis Rheumatol. 2015, 67, 2056–2060. [Google Scholar] [CrossRef]
- Shimizu, M.; Nakagishi, Y.; Inoue, N.; Mizuta, M.; Yachie, A. Leucine-rich α2-glycoprotein as the acute-phase reactant to detect systemic juvenile idiopathic arthritis disease activity during anti-interleukin-6 blockade therapy: A case series. Mod. Rheumatol. 2017, 27, 833–837. [Google Scholar] [CrossRef] [PubMed]
- Castagnola, M.; Scarano, E.; Passali, G.; Messana, I.; Cabras, T.; Iavarone, F.; Di Cintio, G.; Fiorita, A.; De Corso, E.; Paludetti, G. Salivary biomarkers and proteomics: Future diagnostic and clinical utilities. Acta Otorhinolaryngol. Ital. 2017, 37, 94–101. [Google Scholar] [CrossRef]
- Hassaneen, M.; Maron, J.L. Salivary diagnostics in pediatrics: Applicability, translatability, and limitations. Front. Public Health 2017, 5, 83. [Google Scholar] [CrossRef]
- Pappa, E.; Kousvelari, E.; Vastardis, H. Saliva in the "Omics" era: A promising tool in paediatrics. Oral Dis. 2019, 25, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Shirai, R.; Hirano, F.; Ohkura, N.; Ikeda, K.; Inoue, S. Up-regulation of the expression of leucine-rich alpha(2)-glycoprotein in hepatocytes by the mediators of acute-phase response. Biochem. Biophys. Res. Commun. 2009, 382, 776–779. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Rak, S.; Mrklić, I.; Jurić, I. Prospective validation of Alvarado score and Pediatric Appendicitis Score for the diagnosis of acute appendicitis in children. Pediatr. Emerg. Care 2015, 31, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Cabras, T.; Iavarone, F.; Manconi, B.; Olianas, A.; Sanna, M.T.; Castagnola, M.; Messana, I. Top-down analytical platforms for the characterization of the human salivary proteome. Bioanalysis 2014, 6, 563–581. [Google Scholar] [CrossRef]
- Romano-Keeler, J.; Wynn, J.L.; Maron, J.L. Great expectorations: The potential of salivary ‘omic’ approaches in neonatal intensive care. J. Perinatol. 2014, 34, 169–173. [Google Scholar] [CrossRef]
- Schulz, B.; Cooper-White, J.; Punyadeera, C.K. Saliva proteome research: Current status and future outlook. Crit. Rev. Biotechnol. 2013, 33, 246–259. [Google Scholar] [CrossRef]
- Cabras, T.; Pisano, E.; Mastinu, A.; Denotti, G.; Pusceddu, P.P.; Inzitari, R.; Fanali, C.; Nemolato, S.; Castagnola, M.; Messana, I. Alterations of the salivary secretory peptidome profile in children affected by type 1 diabetes. Mol. Cell. Proteom. 2010, 9, 2099–2108. [Google Scholar] [CrossRef]
- Abrão, A.L.P.; Falcao, D.P.; de Amorim, R.F.B.; Bezerra, A.C.B.; Pombeiro, G.A.N.; Guimarães, L.J.; Fregni, F.; Silva, L.P.; da Mota, L.M.H. Salivary proteomics: A new adjuvant approach to the early diagnosis of familial juvenile systemic lupus erythematosus. Med. Hypotheses 2016, 89, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Boroumand, M.; Olianas, A.; Cabras, T.; Manconi, B.; Fanni, D.; Faa, G.; Desiderio, C.; Messana, I.; Castagnola, M. Saliva, a bodily fluid with recognized and potential diagnostic applications. J. Sep. Sci. 2021, 44, 3677–3690. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, S.; Olander, B.; Pira, U.; Granström, L. White blood cell count, leucocyte elastase activity, and serum concentrations of interleukin-6 and C-reactive protein after open appendicectomy. Eur. J. Surg. 1997, 163, 123–127. [Google Scholar]
- Stankovic, N.; Surbatovic, M.; Stanojevic, I.; Simić, R.; Djuricic, S.; Milickovic, M.; Grujic, B.; Savic, D.; Marinovic, V.M.; Stankovic, M.; et al. Possible cytokine biomarkers in pediatric acute appendicitis. Ital. J. Pediatr. 2019, 45, 125. [Google Scholar] [CrossRef]
- Yoshizawa, J.M.; Schafer, C.A.; Schafer, J.J.; Farrell, J.J.; Paster, B.J.; Wong, D.T. Salivary biomarkers: Toward future clinical and diagnostic utilities. Clin. Microbiol. Rev. 2013, 26, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Beara, V.; Jukić, M.; Rashwan, H.; Šušnjar, T. A new approach to laparoscopic appendectomy in children-clipless/sutureless Harmonic scalpel laparoscopic appendectomy. Langenbeck’s Arch. Surg. 2022, 407, 779–787. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Rothrock, S.G.; Pagane, J. Acute appendicitis in children: Emergency department diagnosis and management. Ann. Emerg. Med. 2000, 36, 39–51. [Google Scholar] [CrossRef]
- Addiss, D.G.; Shaffer, N.; Fowler, B.S.; Tauxe, R.V. The epidemiology of appendicitis and appendectomy in the United States. Am. J. Epidemiol. 1990, 132, 910–925. [Google Scholar] [CrossRef]
- Anderson, J.E.; Bickler, S.W.; Chang, D.C.; Talamini, M.A. Examining a common disease with unknown etiology: Trends in epidemiology and surgical management of appendicitis in California, 1995–2009. World J. Surg. 2012, 36, 2787–2794. [Google Scholar] [CrossRef] [PubMed]
- Jukić, M.; Tesch, A.; Todorić, J.; Šušnjar, T.; Milunović, K.P.; Barić, T.; Pogorelić, Z. Same-day discharge after laparoscopic appendectomy for simple appendicitis in pediatric patients—Is it possible? Children 2022, 9, 1220. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Acute Appendicitis (n = 46) | Non-Appendicitis (n = 46) | p | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age (years) | 11.4 | 3.3 | 11.8 | 3.0 | 0.602 * |
| Body weight (kg) | 47.4 | 17.1 | 48.0 | 16.1 | 0.861 * |
| Body height (cm) | 154.3 | 19.6 | 154.9 | 16.3 | 0.876 * |
| Gender | n | % | n | % | |
| Male | 33 | 71.7 | 13 | 28.3 | 0.130 ‡ |
| Female | 26 | 56.5 | 20 | 43.5 | |
| Pathohistological Findings | n (%) |
|---|---|
| Phlegmonous appendicitis | 20 (43.5) |
| Gangrenous appendicitis | 16 (34.8) |
| Perforated gangrenous appendicitis | 10 (21.7) |
| Variables | Acute Appendicitis (n = 46) | Non-Appendicitis (n = 46) | p * | ||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | ||
| Duration of symptoms (h) | 25 | (18, 36) | 32.5 | (24, 50) | 0.031 |
| AIR score | 9 | (7, 10) | 3 | (3, 4) | <0.001 |
| Body temperature (°C) | 37.3 | (36.9, 37.6) | 36.8 | (36.6, 36.9) | <0.001 |
| WBC (×109/L) | 14.6 | (12.7, 18.7) | 7.0 | (5.4, 9.0) | <0.001 |
| CRP (mg/dL) | 16.3 | (6.9, 50.4) | 2.2 | (2, 2) | <0.001 |
| Neutrophil count (%) | 84.6 | (79.5, 89.0) | 59.5 | (51.5, 68.6) | <0.001 |
| LRG1 in saliva (ng/dL) | 233.45 | (114.9, 531.2) | 55.95 | (51.5, 117.9) | <0.001 |
| Duration of surgery (min) | 21 | (18, 30) | - | - | - |
| Length of hospital stay (days) | 2 | (1, 3) | 2 | (2, 2) | 0.856 |
| Biomarker | AUC (95% CI) | Youlden Index J | Sensitivity in Population [%] * | |
|---|---|---|---|---|
| J | Sensitivity and specificity [%] | |||
| WBC (×109/L) | 0.94 ** (0.86–0.98) | 0.83 (0.69–0.91) | 95.7, 87.0 | 78.3 |
| CRP (mg/dL) | 0.76 ** (0.65–0.84) | 0.46 (0.27–0.59) | 78.3, 67.4 | 10.9 |
| Neutrophil count (%) | 0.95 ** (0.88–0.98) | 0.78 (0.63–0.87) | 84.8, 93.5 | 65.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tintor, G.; Jukić, M.; Šupe-Domić, D.; Jerončić, A.; Pogorelić, Z. Diagnostic Accuracy of Leucine-Rich α-2-Glycoprotein 1 as a Non-Invasive Salivary Biomarker in Pediatric Appendicitis. Int. J. Mol. Sci. 2023, 24, 6043. https://doi.org/10.3390/ijms24076043
Tintor G, Jukić M, Šupe-Domić D, Jerončić A, Pogorelić Z. Diagnostic Accuracy of Leucine-Rich α-2-Glycoprotein 1 as a Non-Invasive Salivary Biomarker in Pediatric Appendicitis. International Journal of Molecular Sciences. 2023; 24(7):6043. https://doi.org/10.3390/ijms24076043
Chicago/Turabian StyleTintor, Goran, Miro Jukić, Daniela Šupe-Domić, Ana Jerončić, and Zenon Pogorelić. 2023. "Diagnostic Accuracy of Leucine-Rich α-2-Glycoprotein 1 as a Non-Invasive Salivary Biomarker in Pediatric Appendicitis" International Journal of Molecular Sciences 24, no. 7: 6043. https://doi.org/10.3390/ijms24076043
APA StyleTintor, G., Jukić, M., Šupe-Domić, D., Jerončić, A., & Pogorelić, Z. (2023). Diagnostic Accuracy of Leucine-Rich α-2-Glycoprotein 1 as a Non-Invasive Salivary Biomarker in Pediatric Appendicitis. International Journal of Molecular Sciences, 24(7), 6043. https://doi.org/10.3390/ijms24076043