

Beta-Amyloid Peptide in Tears: An Early Diagnostic Marker of Alzheimer’s Disease Correlated with Choroidal Thickness

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Results
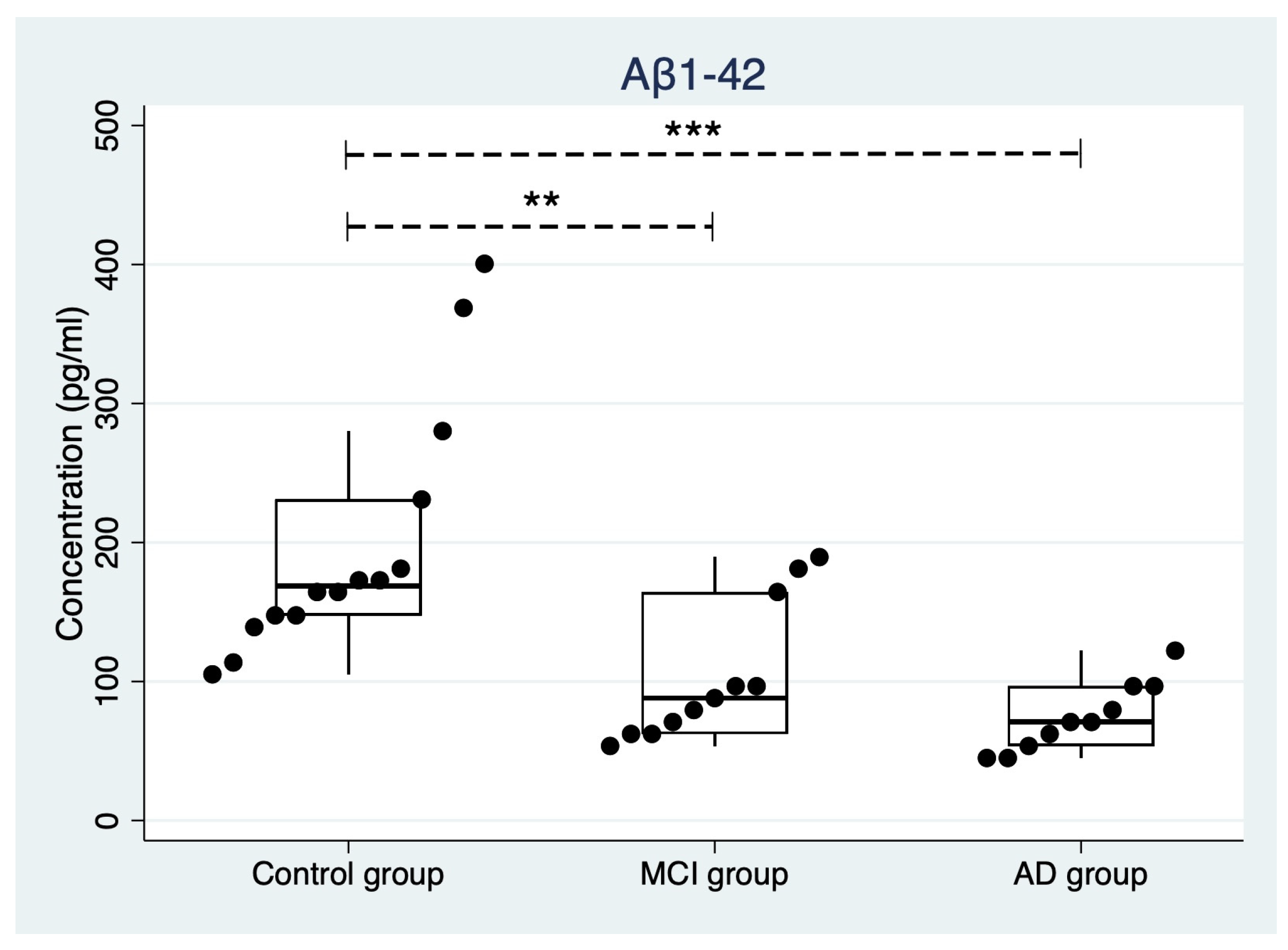
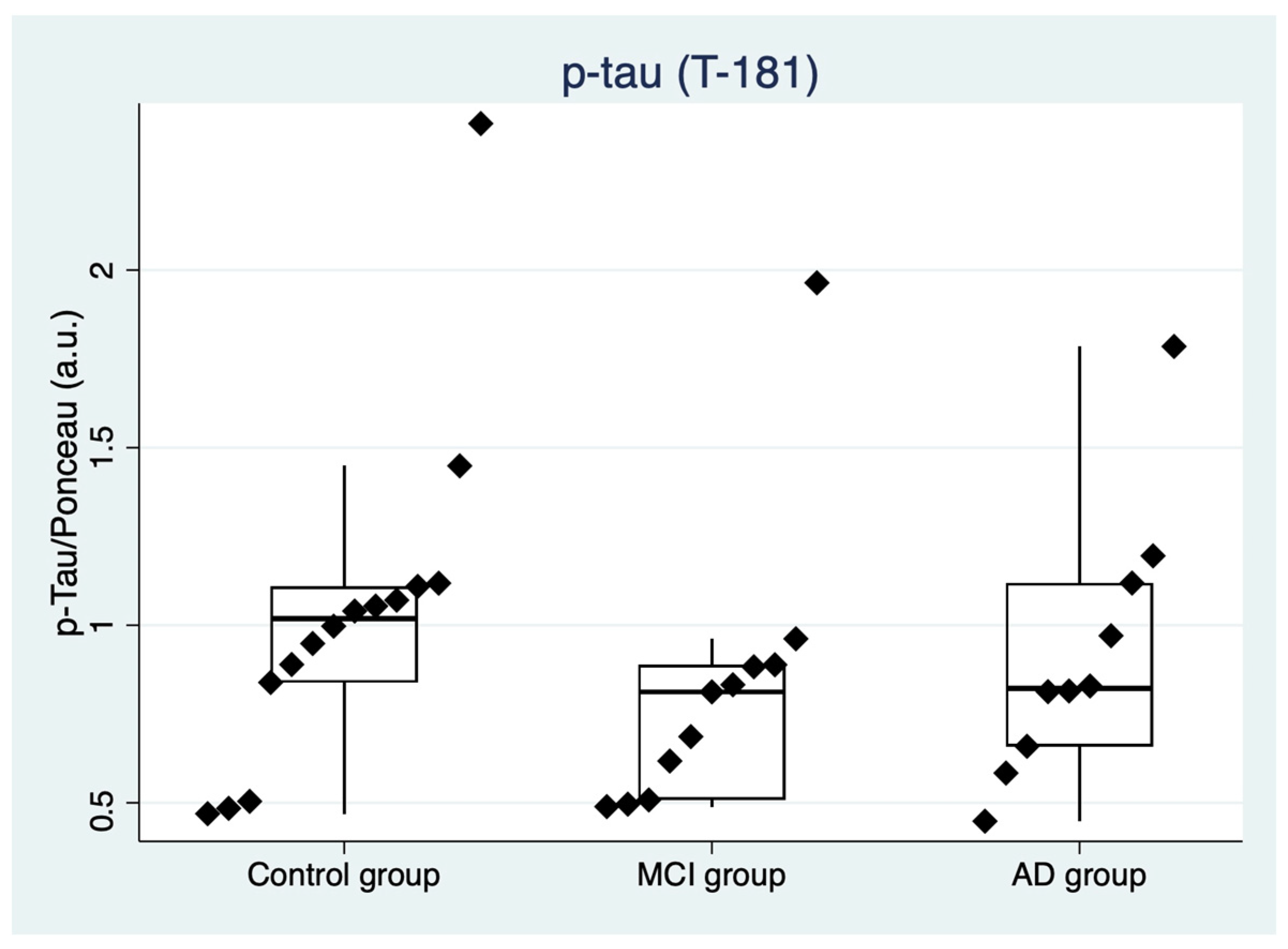
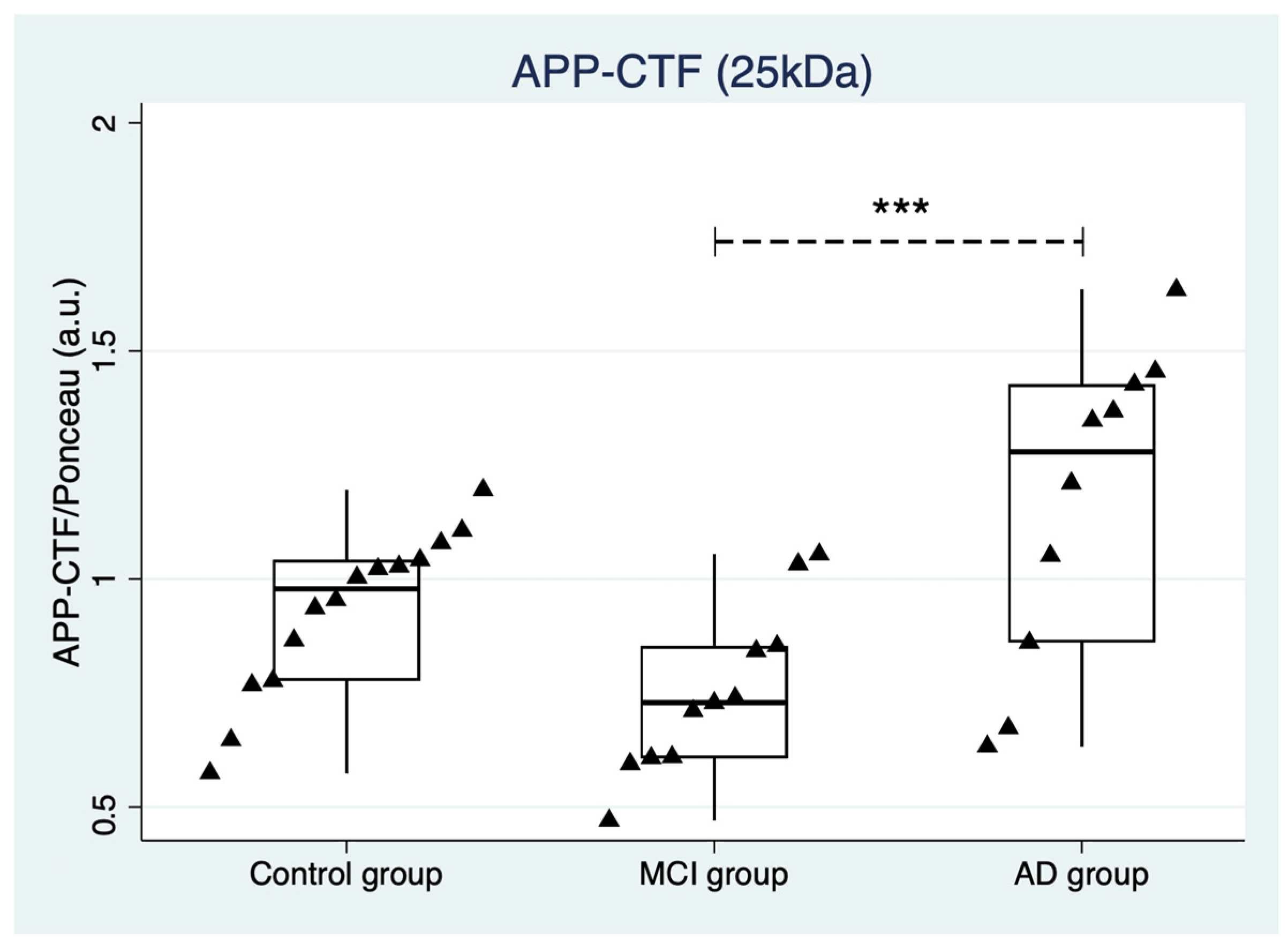
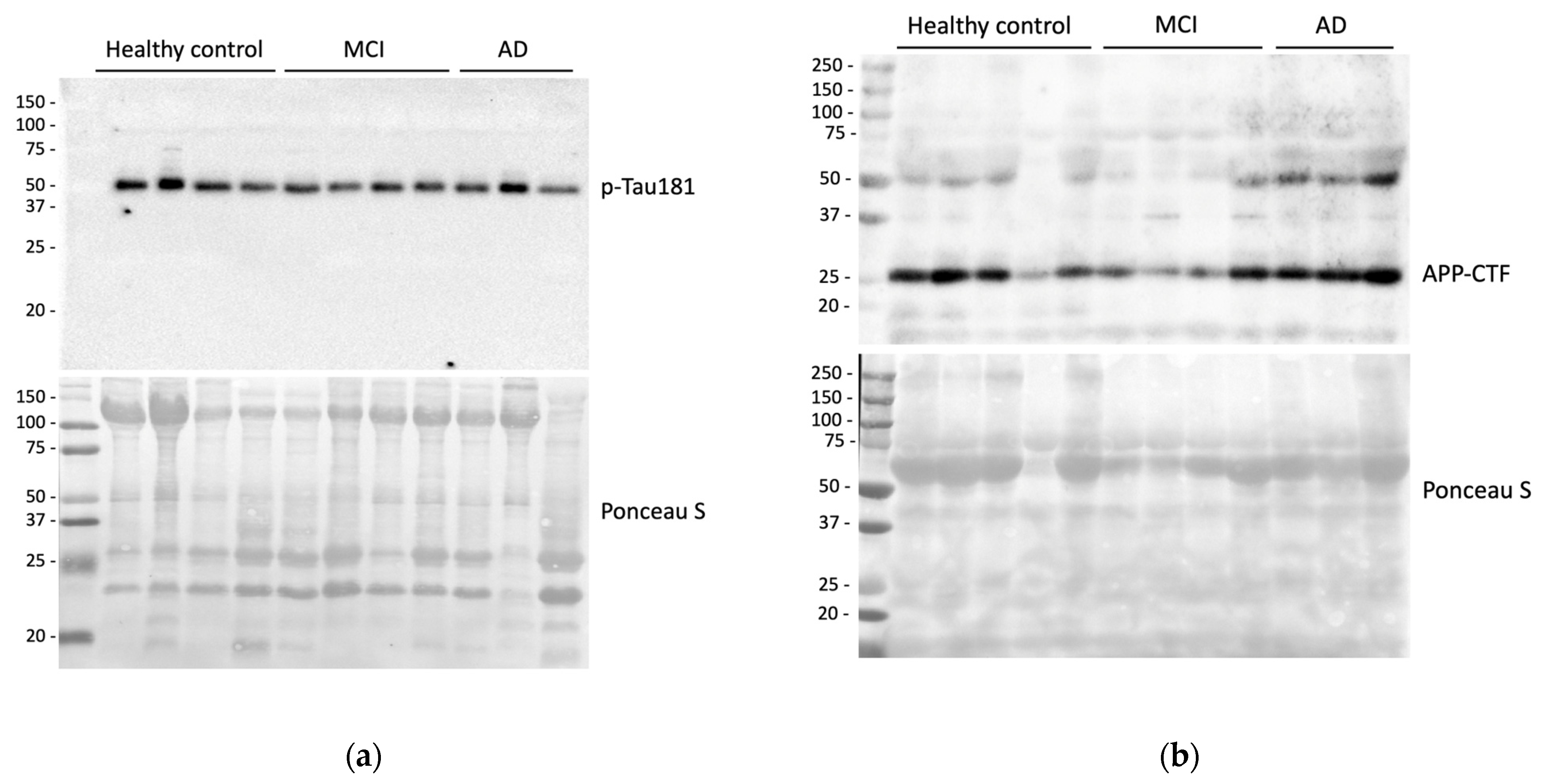
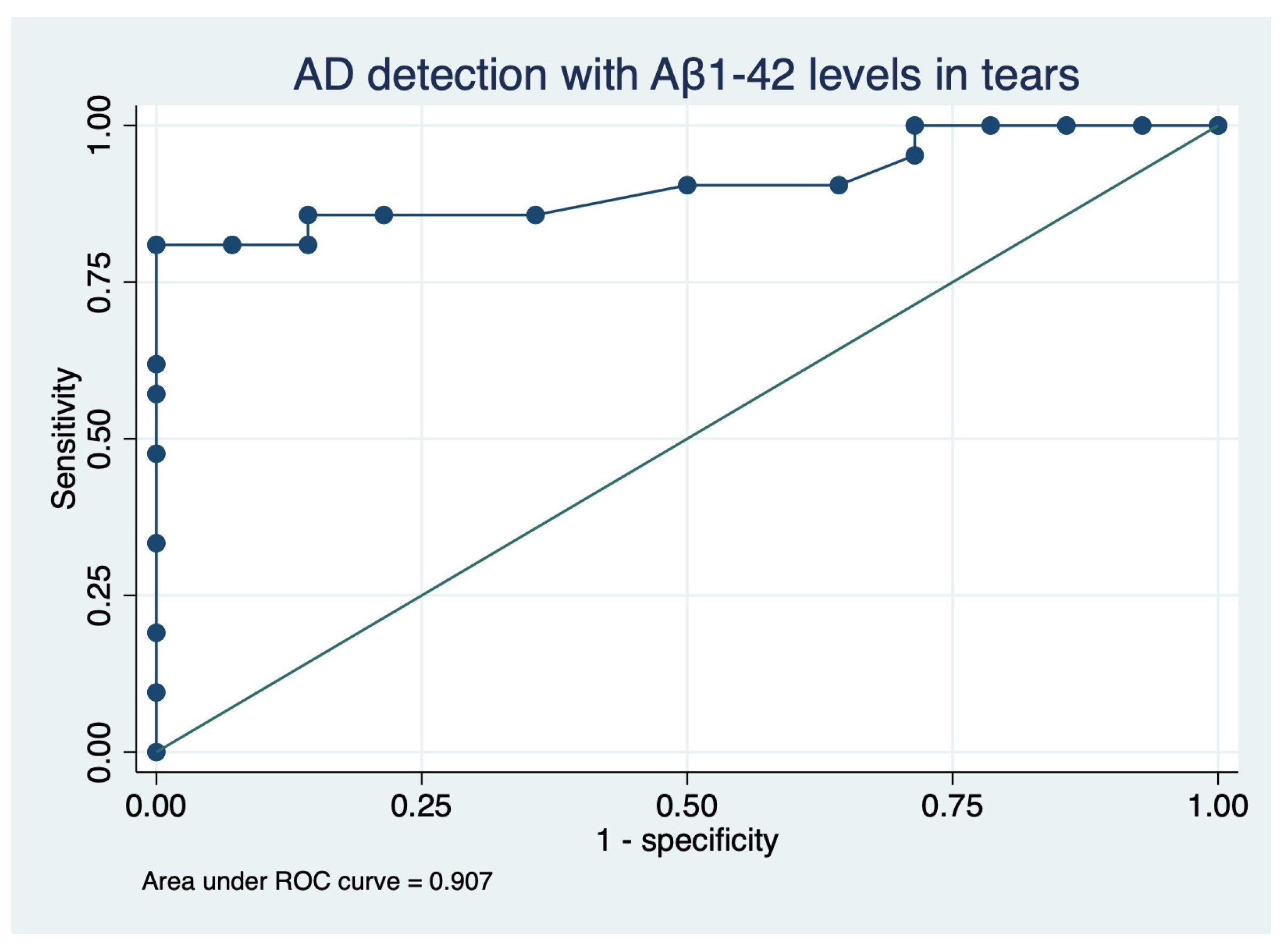
2.1. Tear Sample Analysis of Alzheimer’s Biomarkers
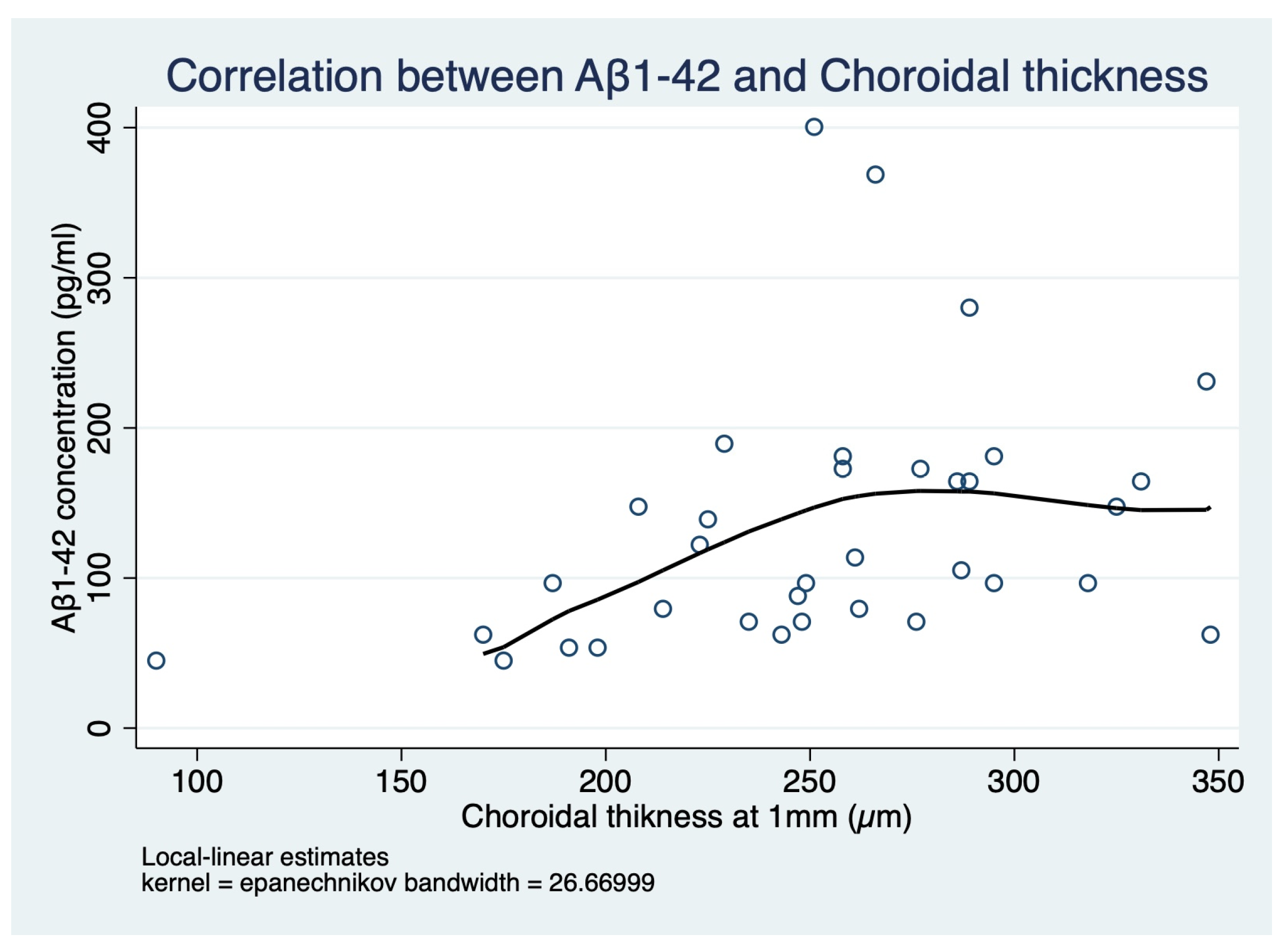
2.2. Neurological and Ophthalmological Correlations
3. Discussion
4. Materials and Methods
4.1. Ophthalmological Evaluation
4.2. Tear Sample Collection and Evaluation
4.3. Sample Size Calculation
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guzman-Martinez, L.; Maccioni, R.B.; Farías, G.A.; Fuentes, P.; Navarrete, L.P. Biomarkers for Alzheimer’s Disease. Curr. Alzheimer Res. 2019, 16, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, E.; Topouzis, F.; Tegos, T.; Tsolaki, M. The Contribution of Ocular Biomarkers in the Differential Diagnosis of Alzheimer’s Disease versus Other Types of Dementia and Future Prospects. J. Alzheimer’s Dis. 2021, 80, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Gharbiya, M.; Trebbastoni, A.; Parisi, F.; Manganiello, S.; Cruciani, F.; D’Antonio, F.; de Vico, U.; Imbriano, L.; Campanelli, A.; de Lena, C. Choroidal Thinning as a New Finding in Alzheimer’s Disease: Evidence from Enhanced Depth Imaging Spectral Domain Optical Coherence Tomography. J. Alzheimer’s Dis. 2014, 40, 907–917. [Google Scholar] [CrossRef]
- Elahi, F.M.; Ashimatey, S.B.; Bennett, D.J.; Walters, S.M.; La Joie, R.; Jiang, X.; Wolf, A.; Cobigo, Y.; Staffaroni, A.M.; Rosen, H.J.; et al. Retinal Imaging Demonstrates Reduced Capillary Density in Clinically Unimpaired APOE Ε4 Gene Carriers. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2021, 13, e12181. [Google Scholar] [CrossRef]
- Tadokoro, K.; Yamashita, T.; Kimura, S.; Nomura, E.; Ohta, Y.; Omote, Y.; Takemoto, M.; Hishikawa, N.; Morihara, R.; Morizane, Y.; et al. Retinal Amyloid Imaging for Screening Alzheimer’s Disease. J. Alzheimer’s Dis. 2021, 83, 927–934. [Google Scholar] [CrossRef]
- Cheung, C.Y.; Mok, V.; Foster, P.J.; Trucco, E.; Chen, C.; Wong, T.Y. Retinal Imaging in Alzheimer’s Disease. J. Neurol. Neurosurg. Psychiatry 2021, 92, 983–994. [Google Scholar] [CrossRef]
- Król-Grzymała, A.; Sienkiewicz-Szłapka, E.; Fiedorowicz, E.; Rozmus, D.; Cieślińska, A.; Grzybowski, A. Tear Biomarkers in Alzheimer’s and Parkinson’s Diseases, and Multiple Sclerosis: Implications for Diagnosis (Systematic Review). Int. J. Mol. Sci. 2022, 23, 10123. [Google Scholar] [CrossRef]
- Gijs, M.; Ramakers, I.H.G.B.; Visser, P.J.; Verhey, F.R.J.; van de Waarenburg, M.P.H.; Schalkwijk, C.G.; Nuijts, R.M.M.A.; Webers, C.A.B. Association of Tear Fluid Amyloid and Tau Levels with Disease Severity and Neurodegeneration. Sci. Rep. 2021, 11, 22675. [Google Scholar] [CrossRef]
- García-Ayllón, M.S.; Lopez-Font, I.; Boix, C.P.; Fortea, J.; Sánchez-Valle, R.; Lleó, A.; Molinuevo, J.L.; Zetterberg, H.; Blennow, K.; Sáez-Valero, J. C-Terminal Fragments of the Amyloid Precursor Protein in Cerebrospinal Fluid as Potential Biomarkers for Alzheimer Disease. Sci. Rep. 2017, 7, 2477. [Google Scholar] [CrossRef]
- Romaus-Sanjurjo, D.; Regueiro, U.; López-López, M.; Vázquez-Vázquez, L.; Ouro, A.; Lema, I.; Sobrino, T. Alzheimer’s Disease Seen through the Eye: Ocular Alterations and Neurodegeneration. Int. J. Mol. Sci. 2022, 23, 2486. [Google Scholar] [CrossRef]
- Kalló, G.; Emri, M.; Varga, Z.; Ujhelyi, B.; Tozsér, J.; Csutak, A.; Csosz, É. Changes in the Chemical Barrier Composition of Tears in Alzheimer’s Disease Reveal Potential Tear Diagnostic Biomarkers. PLoS ONE 2016, 11, e0158000. [Google Scholar] [CrossRef] [PubMed]
- Kenny, A.; Jiménez-Mateos, E.M.; Zea-Sevilla, M.A.; Rábano, A.; Gili-Manzanaro, P.; Prehn, J.H.M.; Henshall, D.C.; Ávila, J.; Engel, T.; Hernández, F. Proteins and MicroRNAs Are Differentially Expressed in Tear Fluid from Patients with Alzheimer’s Disease. Sci. Rep. 2019, 9, 15437. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.R.; Chuang, H.C.; Tripathi, A.; Wang, Y.L.; Ko, M.L.; Chuang, C.C.; Chen, J.C. High-Sensitivity and Trace-Amount Specimen Electrochemical Sensors for Exploring the Levels of β-Amyloid in Human Blood and Tears. Anal. Chem. 2021, 93, 8099–8106. [Google Scholar] [CrossRef] [PubMed]
- Lambiase, A.; Micera, A.; Sacchetti, M.; Cortes, M.; Mantelli, F.; Bonini, S. Alterations of Tear Neuromediators in Dry Eye Disease. JAMA Ophthalmol. 2011, 129, 981–986. [Google Scholar] [CrossRef]
- Mohamed Lafirdeen, A.S.; Cognat, E.; Sabia, S.; Hourregue, C.; Lilamand, M.; Dugravot, A.; Bouaziz-Amar, E.; Laplanche, J.L.; Hugon, J.; Singh-Manoux, A.; et al. Biomarker Profiles of Alzheimer’s Disease and Dynamic of the Association between Cerebrospinal Fluid Levels of β-Amyloid Peptide and Tau. PLoS ONE 2019, 14, e0217026. [Google Scholar] [CrossRef]
- Hampel, H.; Teipel, S.J.; Fuchsberger, T.; Andreasen, N.; Wiltfang, J.; Otto, M.; Shen, Y.; Dodel, R.; Du, Y.; Farlow, M.; et al. Value of CSF Beta-Amyloid1-42 and Tau as Predictors of Alzheimer’s Disease in Patients with Mild Cognitive Impairment. Mol. Psychiatry 2004, 9, 705–710. [Google Scholar] [CrossRef]
- Lim, H.J.; Park, J.E.; Kim, B.C.; Choi, S.M.; Song, M.K.; Cho, S.H.; Seo, H.J.; Kim, J.; Song, H.C.; Choi, K.Y.; et al. Comparison of Two Analytical Platforms in Cerebrospinal Fluid Biomarkers for the Classification of Alzheimer’s Disease Spectrum with Amyloid PET Imaging. J. Alzheimer’s Dis. 2020, 75, 949–958. [Google Scholar] [CrossRef]
- Grimmer, T.; Riemenschneider, M.; Förstl, H.; Henriksen, G.; Klunk, W.E.; Mathis, C.A.; Shiga, T.; Wester, H.J.; Kurz, A.; Drzezga, A. Beta Amyloid in Alzheimer’s Disease: Increased Deposition in Brain Is Reflected in Reduced Concentration in Cerebrospinal Fluid. Biol. Psychiatry 2009, 65, 927–934. [Google Scholar] [CrossRef]
- Calais, G.; Forzy, G.; Crinquette, C.; MacKowiak, A.; de Seze, J.; Blanc, F.; Lebrun, C.; Heinzlef, O.; Clavelou, P.; Moreau, T.; et al. Tear Analysis in Clinically Isolated Syndrome as New Multiple Sclerosis Criterion. Mult. Scler. J. 2009, 16, 87–92. [Google Scholar] [CrossRef]
- Serafini, B.; Rosicarelli, B.; Magliozzi, R.; Stigliano, E.; Aloisi, F. Detection of Ectopic B-Cell Follicles with Germinal Centers in the Meninges of Patients with Secondary Progressive Multiple Sclerosis. Brain Pathol. 2004, 14, 164–174. [Google Scholar] [CrossRef]
- Van Setten, G.B.; Nilsson, L.; Hahne, S.; Johnston, J.A.; Kvanta, A.; Gandy, S.E.; Näslund, J.; Nordstedt, C. Beta-Amyloid Protein Protein Precursor Expression in Lacrimal Glands and Tear Fluid. Investig. Ophthalmol. Vis. Sci. 1996, 37, 2585–2593. [Google Scholar]
- Selkoe, D.J. Cell Biology of the Amyloid Beta-Protein Precursor and the Mechanism of Alzheimer’s Disease. Annu. Rev. Cell Biol. 1994, 10, 373–403. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Li, R.; Lyu, J.H.; Chen, J.H.; Wang, W.; Gao, M.L.; Li, W.J.; De, J.; Mu, H.Y.; Pan, W.G.; et al. Relationship Between Alzheimer’s Disease and Retinal Choroidal Thickness: A Cross-Sectional Study. J. Alzheimer’s Dis. 2021, 80, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, R.; Huang, S.C.; Bernasconi, M.P.; Falautano, M.; Comi, G.; Magnani, G.; Leocani, L. Neuro-Retina Might Reflect Alzheimer’s Disease Stage. J. Alzheimer’s Dis. 2020, 77, 1455–1468. [Google Scholar] [CrossRef] [PubMed]
- López-de-Eguileta, A.; Lage, C.; López-García, S.; Pozueta, A.; García-Martínez, M.; Kazimierczak, M.; Bravo, M.; de Arcocha-Torres, M.; Banzo, I.; Jimenez-Bonilla, J.; et al. Ganglion Cell Layer Thinning in Prodromal Alzheimer’s Disease Defined by Amyloid PET. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Albert, M.S.; Knopman, D.S.; McKhann, G.M.; Sperling, R.A.; Carrillo, M.C.; Thies, B.; Phelps, C.H. Introduction to the Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimer’s Dement. 2011, 7, 257–262. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The Diagnosis of Dementia Due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef]
- Gharbiya, M.; Albanese, G.M.; Plateroti, A.M.; Marcelli, M.; Marenco, M.; Lambiase, A. Macular Ganglion Cell Layer Thickness after Macula-Off Rhegmatogenous Retinal Detachment Repair: Scleral Buckling versus Pars Plana Vitrectomy. J. Clin. Med. 2020, 9, 1411. [Google Scholar] [CrossRef]
- Albanese, G.M.; Visioli, G.; Iannetti, L.; Giovannetti, F.; Armentano, M.; Romano, E.; Macario, F.; Fino, P.; Gharbiya, M. Does Choroidal Thickness Predict Persistent Subretinal Fluid after Rhegmatogenous Retinal Detachment Repair? A Retrospective Study with Fellow Eye Comparison. Acta Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Armstrong, R.A.; Armstrong, R. Statistical Guidelines for the Analysis of Data Obtained from One or Both Eyes. Ophthalmic Physiol. Opt. 2013, 33, 7–14. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Total | MCI and AD | CG | p-Value |
|---|---|---|---|---|
| n 35 | n 21 | n 14 | ||
| Sex (female), n (%) | 20 (57.1%) | 11 (53.4%) | 9 (64.3%) | 0.728 ‡ |
| Age, mean ± SD | 71.7 ± 6.9 | 72.9 ± 7.3 | 69.9 ± 6.1 | 0.212 * |
| MMSE score, mean ± SD | 25.9 ± 3.7 | 23.7 ± 3.2 | 29.1 ± 1.0 | <0.001† |
| ADAS-cog score, mean ± SD | 18.0 ± 13.7 | 28.2 ± 6.4 | 2.6 ± 2.2 | <0.001† |
| Systemic hypertension, n (%) | 17 (48.6%) | 8 (38.1%) | 9 (64.3%) | 0.176 ‡ |
| Dyslipidemia, n (%) | 15 (42.9%) | 9 (42.9%) | 6 (42.9%) | 1.000 ‡ |
| Ischemic heart disease, n (%) | 3 (8.6%) | 1 (4.8%) | 2 (14.3%) | 0.551 ‡ |
| Heart arrhythmia, n (%) | 1 (2.9%) | 1 (4.8%) | 0 (0.0%) | 1.000 ‡ |
| Dysthyroidism, n (%) | 5 (14.3%) | 1 (4.8%) | 4 (28.6%) | 0.134 ‡ |
| COPD, n (%) | 3 (8.6%) | 1 (4.8%) | 2 (14.3%) | 0.551 ‡ |
| Digestive Diseases, n (%) | 4 (11.4%) | 3 (14.3%) | 1 (7.1%) | 0.635 ‡ |
| Baseline Characteristics | MCI | AD | MCI vs. AD | MCI vs. CG | AD vs. CG | Overall § |
|---|---|---|---|---|---|---|
| n 11 | n 10 | p-Value | p-Value | p-Value | p-Value | |
| Sex (female), n (%) | 5 (45.5%) | 6 (0.6%) | 0.670 | 0.435 | 1.000 | 0.688 ‡ |
| Age, mean ± SD | 75.3 ± 6.8 | 70.2 ± 7.1 | 0.202 | 0.122 | 0.991 | 0.108 † |
| MMSE score, mean ± SD | 25.8 ± 1.7 | 21.3 ± 2.7 | 0.029 | <0.001 | <0.001 | <0.001 * |
| ADAS-cog score, mean ± SD | 25.5 ± 6.0 | 31.2 ± 5.6 | 0.347 | <0.001 | <0.001 | <0.001 * |
| Ophthalmological Data | Total | MCI and AD | CG | p-Value |
|---|---|---|---|---|
| n 35 | n 21 | n 14 | ||
| Lens status (phakic), n (%) | 29 (82.9%) | 18 (85.8%) | 11 (78.6%) | 0.664 ‡ |
| SEQ, mean ± SD | −0.70 ± 1.79 | −0.95 ± 1.64 | −0.32 ± 2.00 | 0.319 * |
| 1 mm foveal thickness, mean ± SD | 272.8 ± 25.0 | 268.5 ± 25.4 | 279.1 ± 23.8 | 0.223 * |
| 1 mm CT, mean ± SD | 252.9 ± 54.3 | 237.2 ± 58.2 | 276.4 ± 38.9 | 0.035 * |
| 1 mm foveal NFL, mean ± SD | 12.7 ± 2.4 | 12.3 ± 2.3 | 13.4 ± 2.3 | 0.163 * |
| 1 mm foveal GCL-IPL, mean ± SD | 33.9 ± 8.6 | 32.9 ± 8.4 | 35.4 ± 8.8 | 0.405 * |
| Peripapillary RNFL (total), mean ± SD | 92.8 ± 14.0 | 92.1 ± 8.8 | 93.9 ± 19.7 | 0.702 ‡ |
| Peripapillary RNFL (superior), mean ± SD | 115.4 ± 22.2 | 113.3 ± 19.6 | 118.4 ± 26.2 | 0.515 * |
| Peripapillary RNFL (nasal), mean ± SD | 71.0 ± 13.9 | 71.5 ± 14.8 | 70.3 ± 12.8 | 0.800 * |
| Peripapillary RNFL (inferior), mean ± SD | 116.1 ± 22.4 | 114.4 ± 17.5 | 118.6 ± 28.8 | 0.599 ‡ |
| Peripapillary RNFL (temporal), mean ± SD | 68.7 ± 16.0 | 68.9 ± 14.5 | 68.4 ± 18.6 | 0.930 * |
| Ophthalmological Data | MCI | AD | MCI vs. AD | MCI vs. CG | AD vs. CG | Overall § |
|---|---|---|---|---|---|---|
| n 11 | n 10 | p-Value | p-Value | p-Value | p-Value | |
| Lens status (phakic), n (%) | 2 (18.2%) | 1 (10%) | 1.000 ‡ | 1.000 ‡ | 0.615 ‡ | 0.861 ‡ |
| SEQ, mean ± SD | −0.67 ± 1.73 | −1.25 ± 1.57 | 0.743 | 0.881 | 0.436 | 0.468 † |
| 1 mm foveal thickness, mean ± SD | 278.1 ± 16.0 | 258.0 ± 30.2 | 0.146 | 0.993 | 0.096 | 0.082 † |
| 1 mm CT, mean ± SD | 246.5 ± 39.3 | 227.0 ± 74.8 | 0.665 | 0.337 | 0.069 | 0.077 † |
| 1 mm foveal NFL, mean ± SD | 13.0 ± 1.4 | 11.5 ± 2.9 | 0.301 | 0.887 | 0.118 | 0.128 † |
| 1 mm foveal GCL-IPL, mean ± SD | 34.2 ± 5.3 | 31.4 ± 11.1 | 0.744 | 0.939 | 0.518 | 0.543 † |
| RNFL (total), mean ± SD | 90.8 ± 7.8 | 93.4 ± 9.9 | 0.716 * | 0.405 * | 1.000 * | 0.537 * |
| RNFL (superior), mean ± SD | 106.6 ± 12.0 | 120.7 ± 24.1 | 0.324 | 0.391 | 0.967 | 0.289 † |
| RNFL (nasal), mean ± SD | 71.9 ± 13.6 | 71.1 ± 16.8 | 0.991 | 0.957 | 0.990 | 0.961 † |
| RNFL (inferior), mean ± SD | 115.3 ± 8.3 | 113.5 ± 24.5 | 0.845 * | 1.000 * | 1.000 * | 0.843 * |
| RNFL (temporal), mean ± SD | 69.8 ± 17.6 | 67.8 ± 11.2 | 0.958 | 0.974 | 0.996 | 0.958 † |
| Baseline Characteristics | p-tau (a.u.) | Aβ42 (pg/mL) | APP-CTF 25 kDa (a.u.) |
|---|---|---|---|
| Total, n 35 | 0.94 ± 0.43 | 133.6 ± 84.3 | 0.94 ± 0.28 |
| MCI, n 11 | 0.83 ± 0.41 | 104.1 ± 50.0 | 0.75 ± 0.18 |
| AD, n 10 | 0.92 ± 0.38 | 74.3 ± 25.0 | 1.17 ± 0.35 |
| CG, n 14 | 1.03 ± 0.49 | 199.2 ± 90.3 | 0.93 ± 0.18 |
| MCI vs. AD, p-value | 0.646 * | 0.298 * | 0.001† |
| MCI vs. CG, p-value | 0.149 * | 0.008 * | 0.168 † |
| AD vs. CG, p-value | 0.661 * | <0.001 * | 0.057 † |
| MCI vs. AD vs. CG, p-value | 0.257 * | <0.001 * | 0.002† |
| MCI + AD vs. CG, p-value | 0.148 § | <0.001§ | 0.847 ‡ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gharbiya, M.; Visioli, G.; Trebbastoni, A.; Albanese, G.M.; Colardo, M.; D’Antonio, F.; Segatto, M.; Lambiase, A. Beta-Amyloid Peptide in Tears: An Early Diagnostic Marker of Alzheimer’s Disease Correlated with Choroidal Thickness. Int. J. Mol. Sci. 2023, 24, 2590. https://doi.org/10.3390/ijms24032590
Gharbiya M, Visioli G, Trebbastoni A, Albanese GM, Colardo M, D’Antonio F, Segatto M, Lambiase A. Beta-Amyloid Peptide in Tears: An Early Diagnostic Marker of Alzheimer’s Disease Correlated with Choroidal Thickness. International Journal of Molecular Sciences. 2023; 24(3):2590. https://doi.org/10.3390/ijms24032590
Chicago/Turabian StyleGharbiya, Magda, Giacomo Visioli, Alessandro Trebbastoni, Giuseppe Maria Albanese, Mayra Colardo, Fabrizia D’Antonio, Marco Segatto, and Alessandro Lambiase. 2023. "Beta-Amyloid Peptide in Tears: An Early Diagnostic Marker of Alzheimer’s Disease Correlated with Choroidal Thickness" International Journal of Molecular Sciences 24, no. 3: 2590. https://doi.org/10.3390/ijms24032590
APA StyleGharbiya, M., Visioli, G., Trebbastoni, A., Albanese, G. M., Colardo, M., D’Antonio, F., Segatto, M., & Lambiase, A. (2023). Beta-Amyloid Peptide in Tears: An Early Diagnostic Marker of Alzheimer’s Disease Correlated with Choroidal Thickness. International Journal of Molecular Sciences, 24(3), 2590. https://doi.org/10.3390/ijms24032590