
Proteoglycan Combined with Hyaluronic Acid and Hydrolyzed Collagen Restores the Skin Barrier in Mild Atopic Dermatitis and Dry, Eczema-Prone Skin: A Pilot Study

 , , , and
, , , and 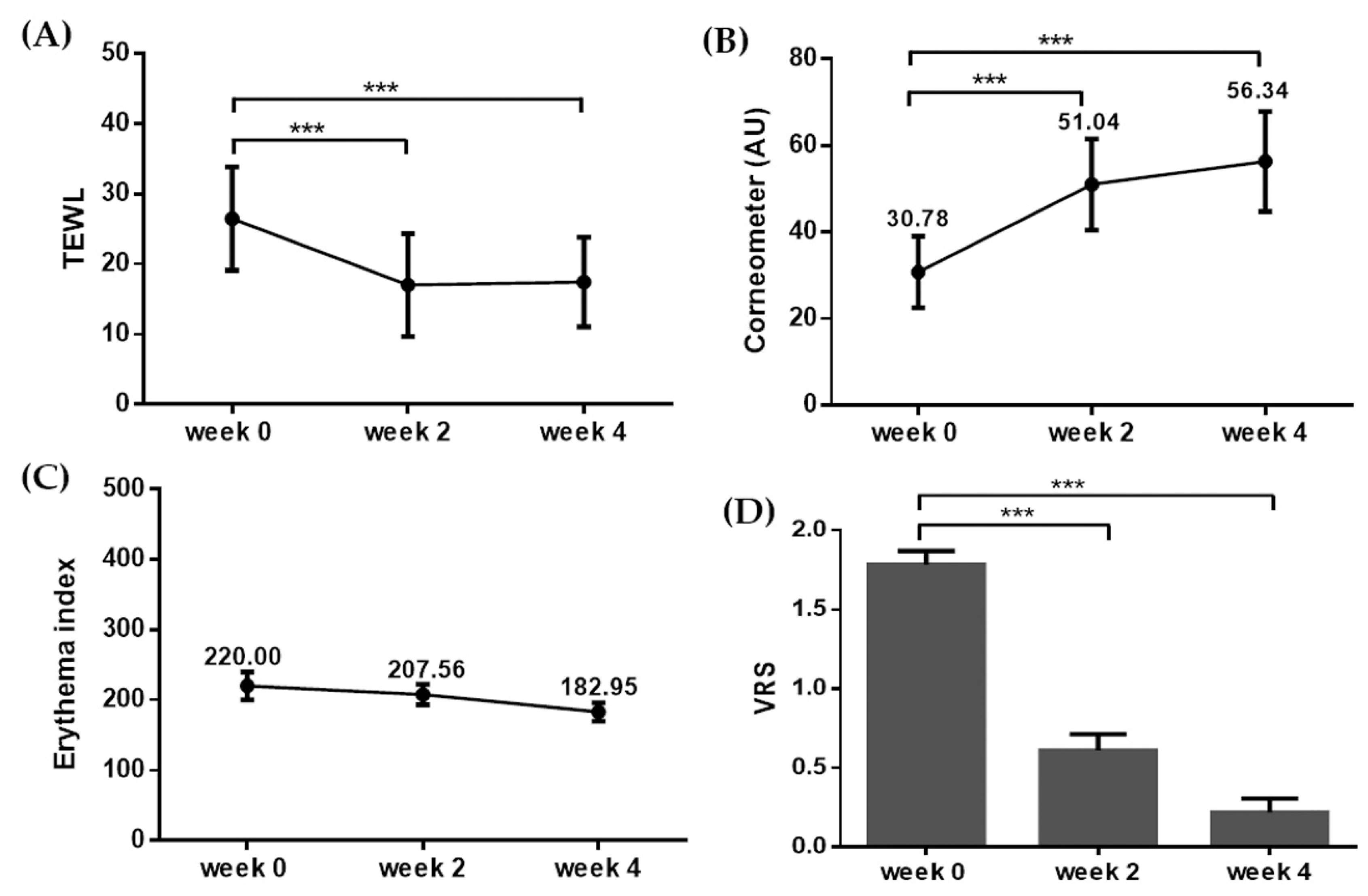{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
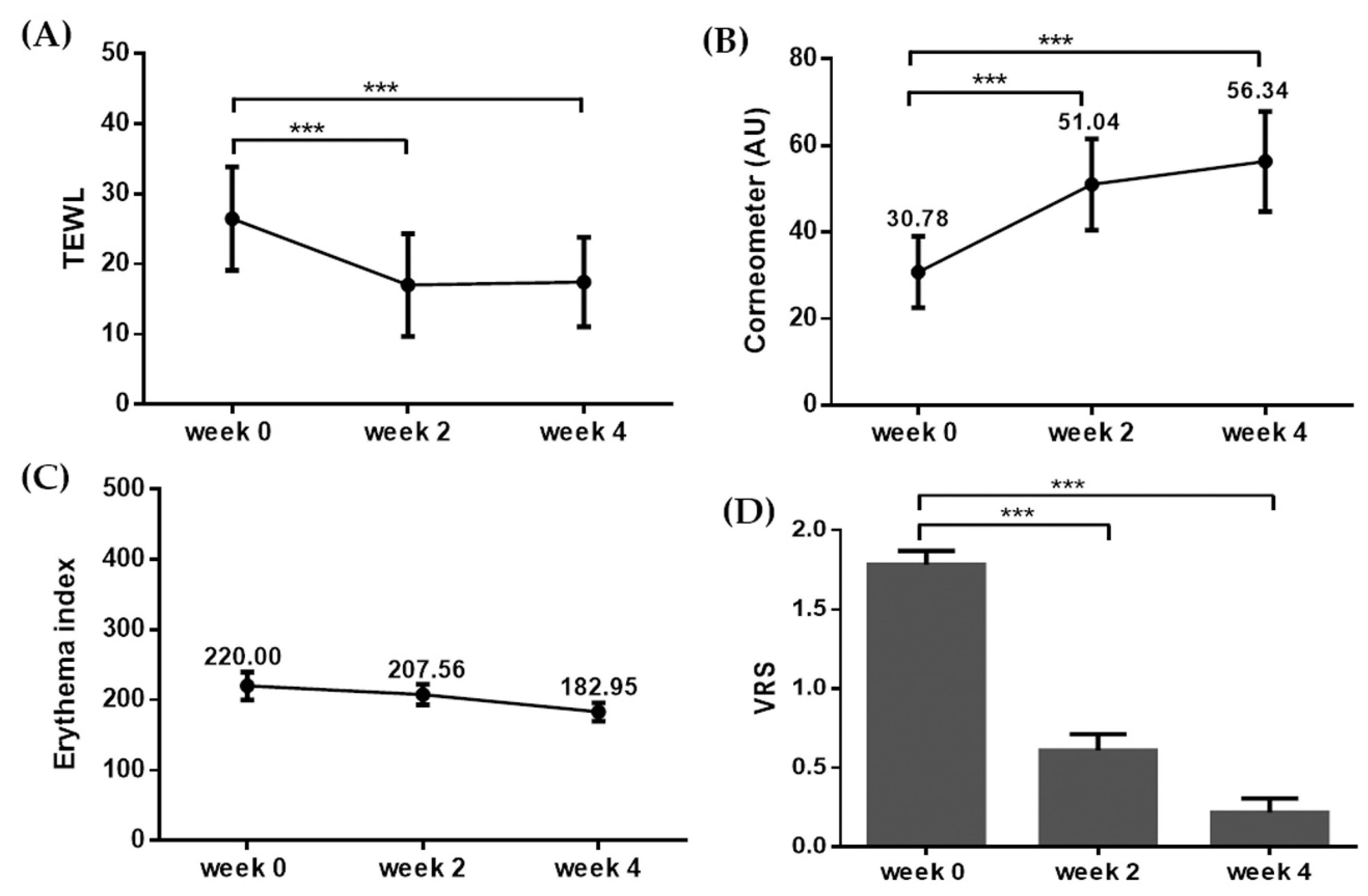
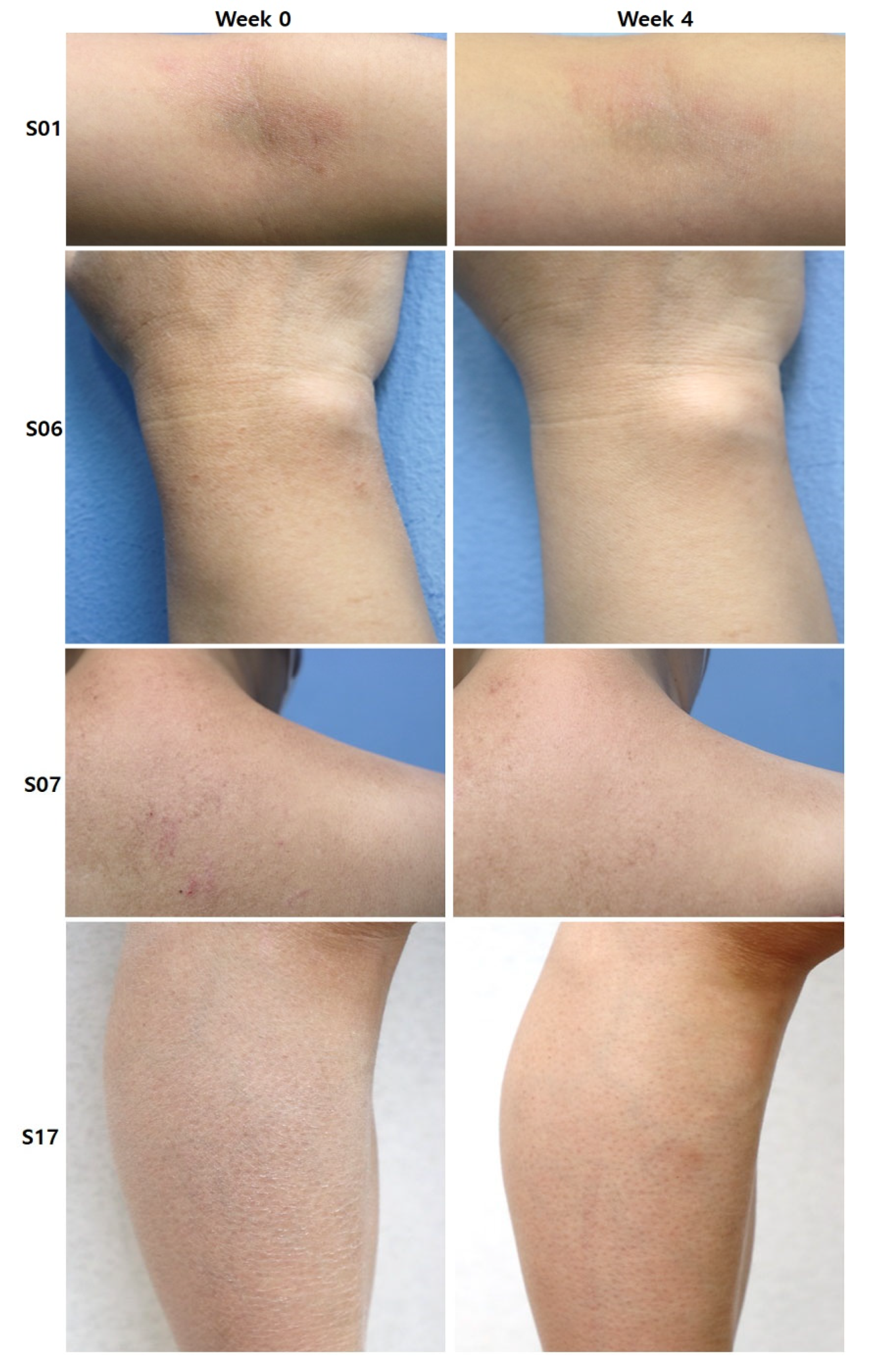
2.2. Clinical Efficacy of a Topical Proteoglycan Product Combined with HA and Collagen
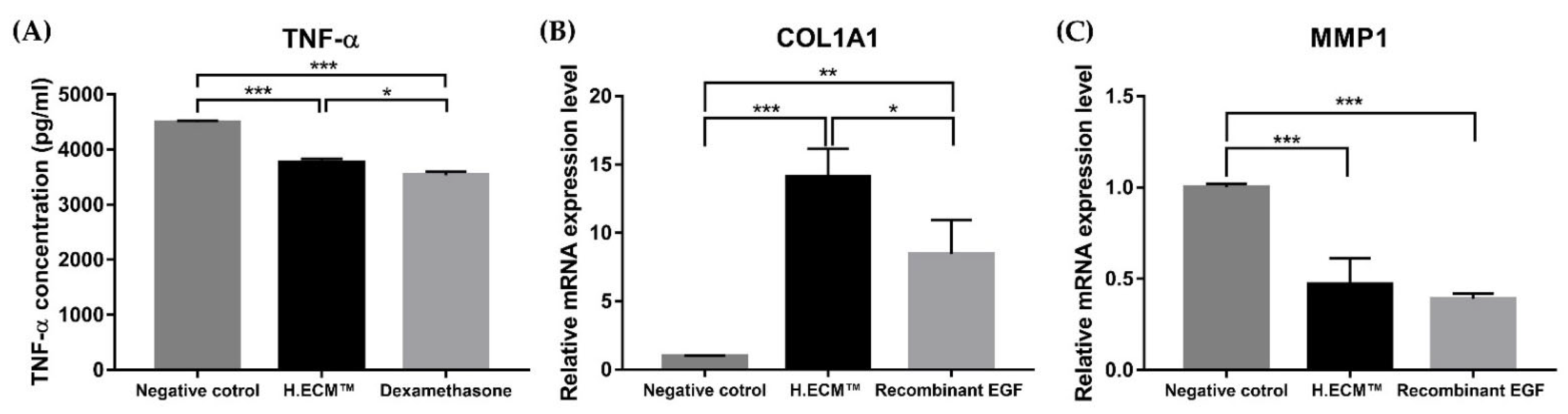
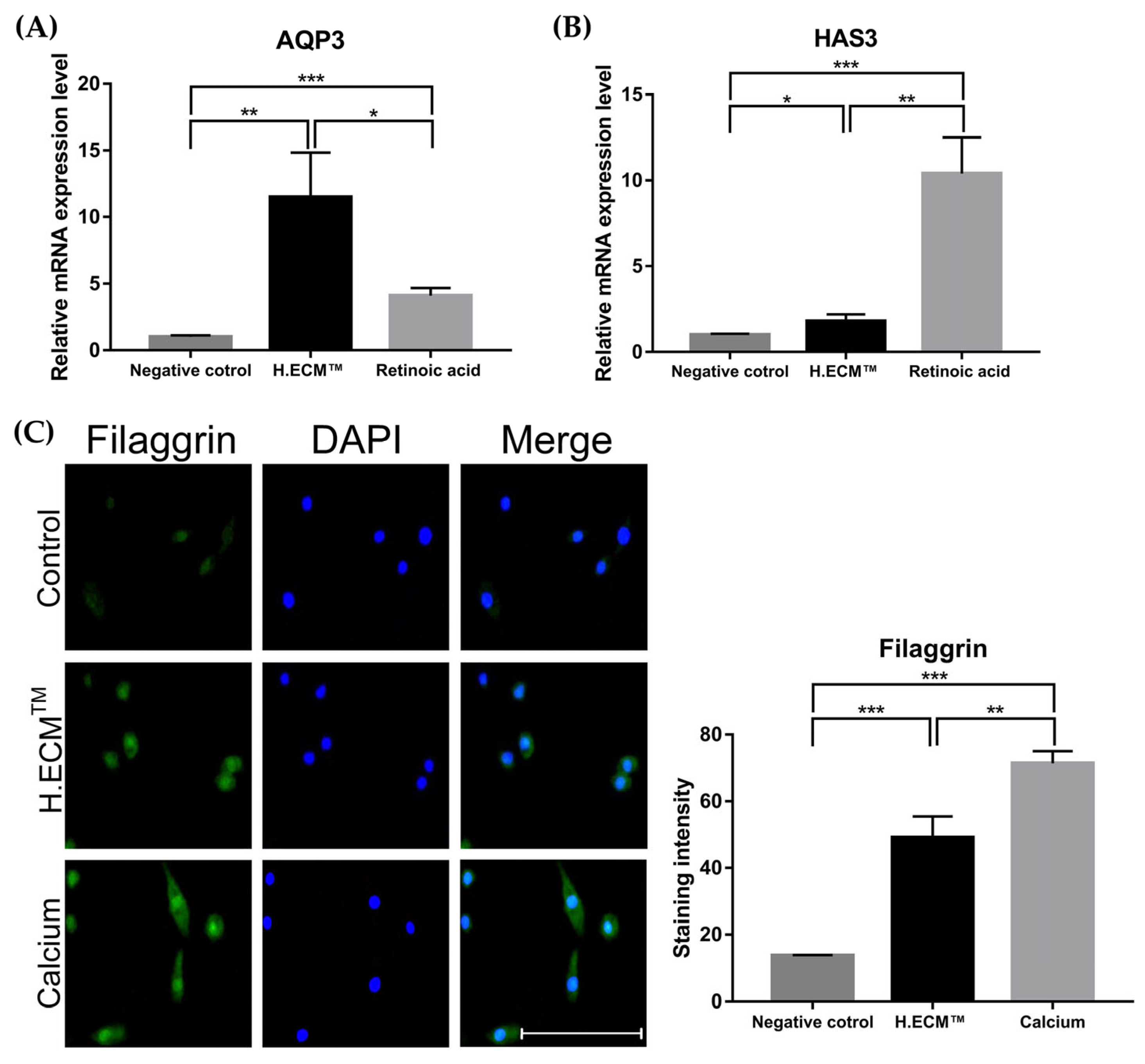
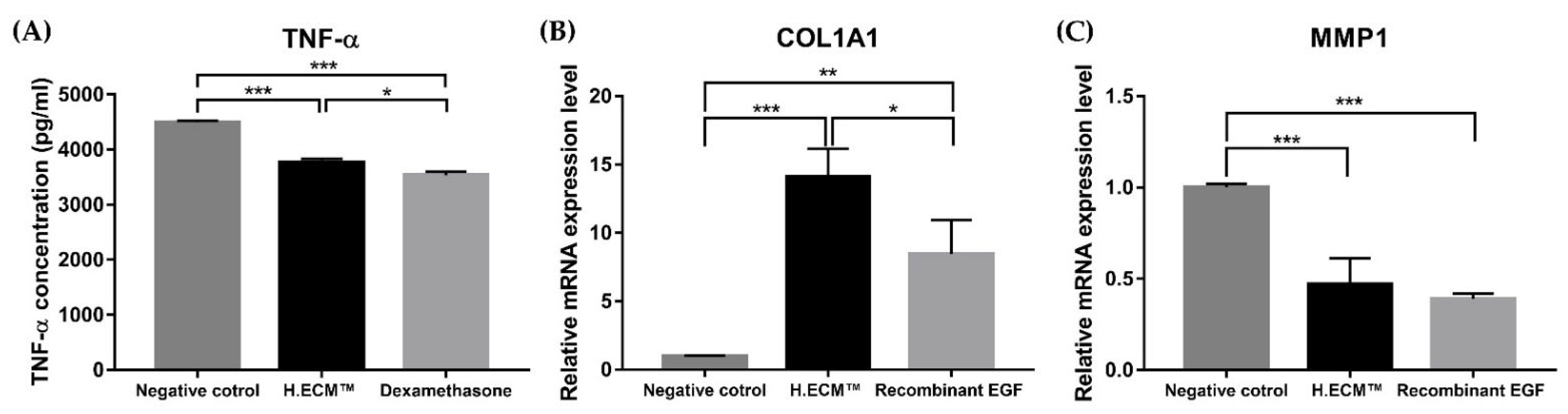
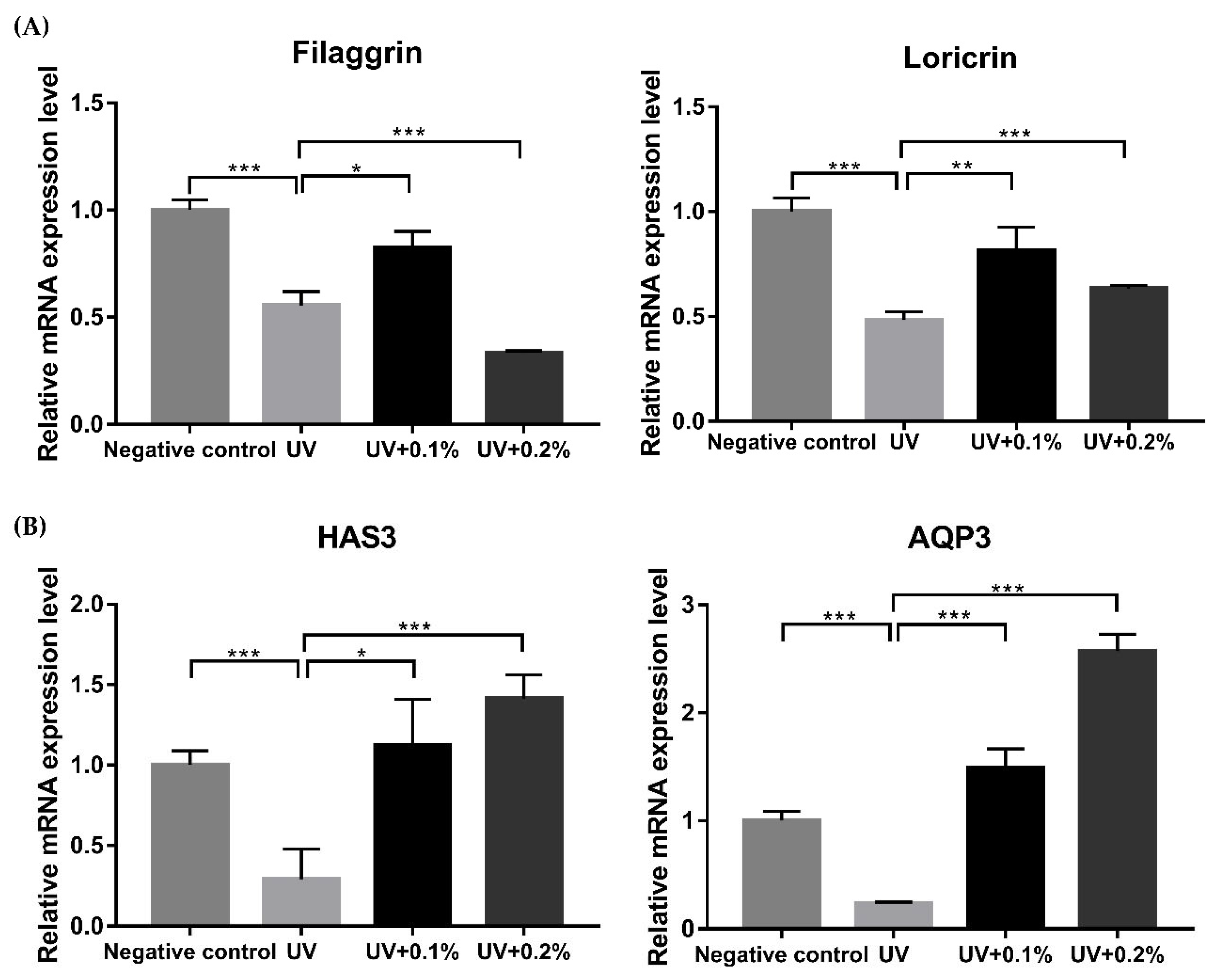
2.3. In Vitro Evaluation of H.ECMTM Liposome and Its Efficacy on Skin Barrier Function and Wrinkles
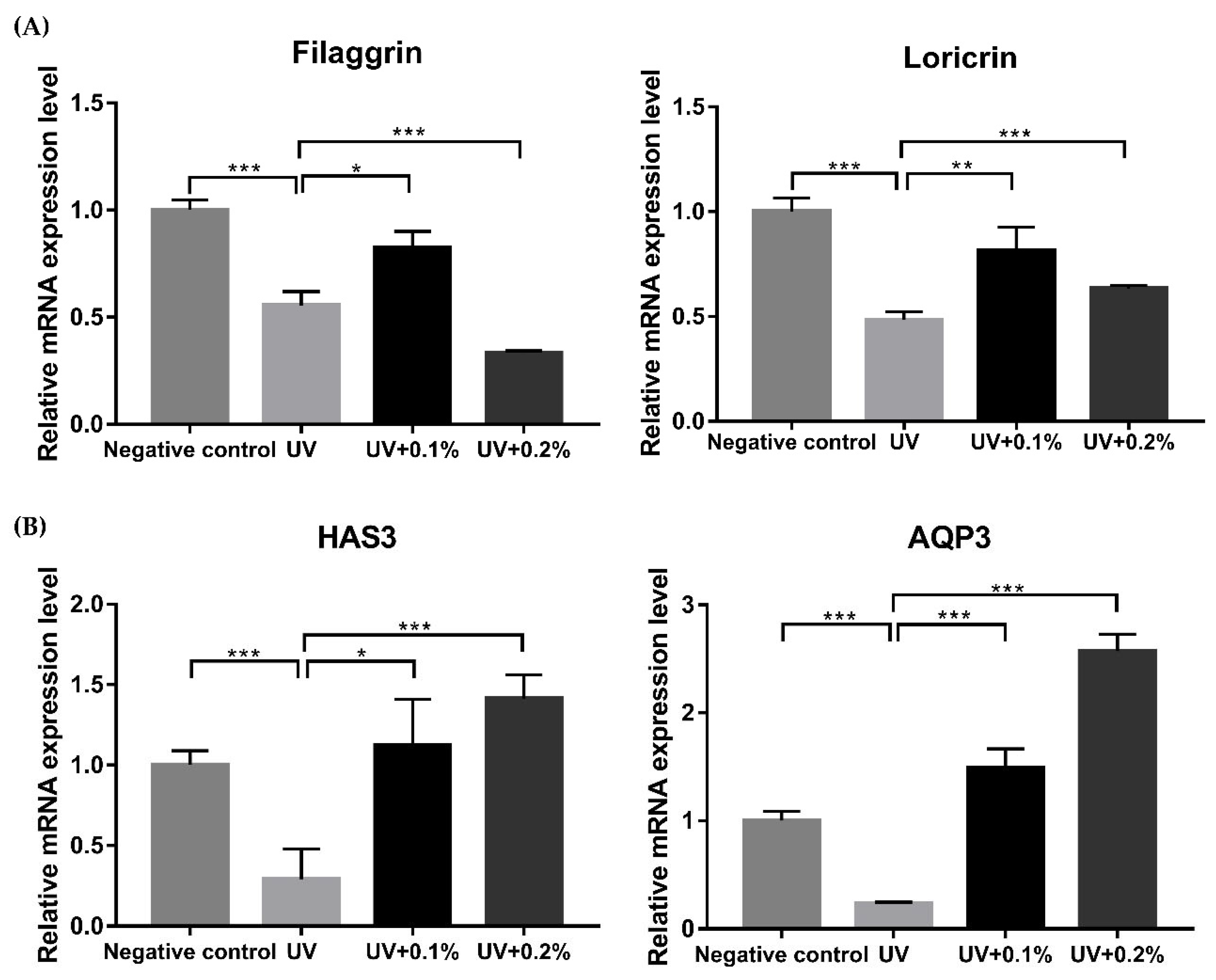
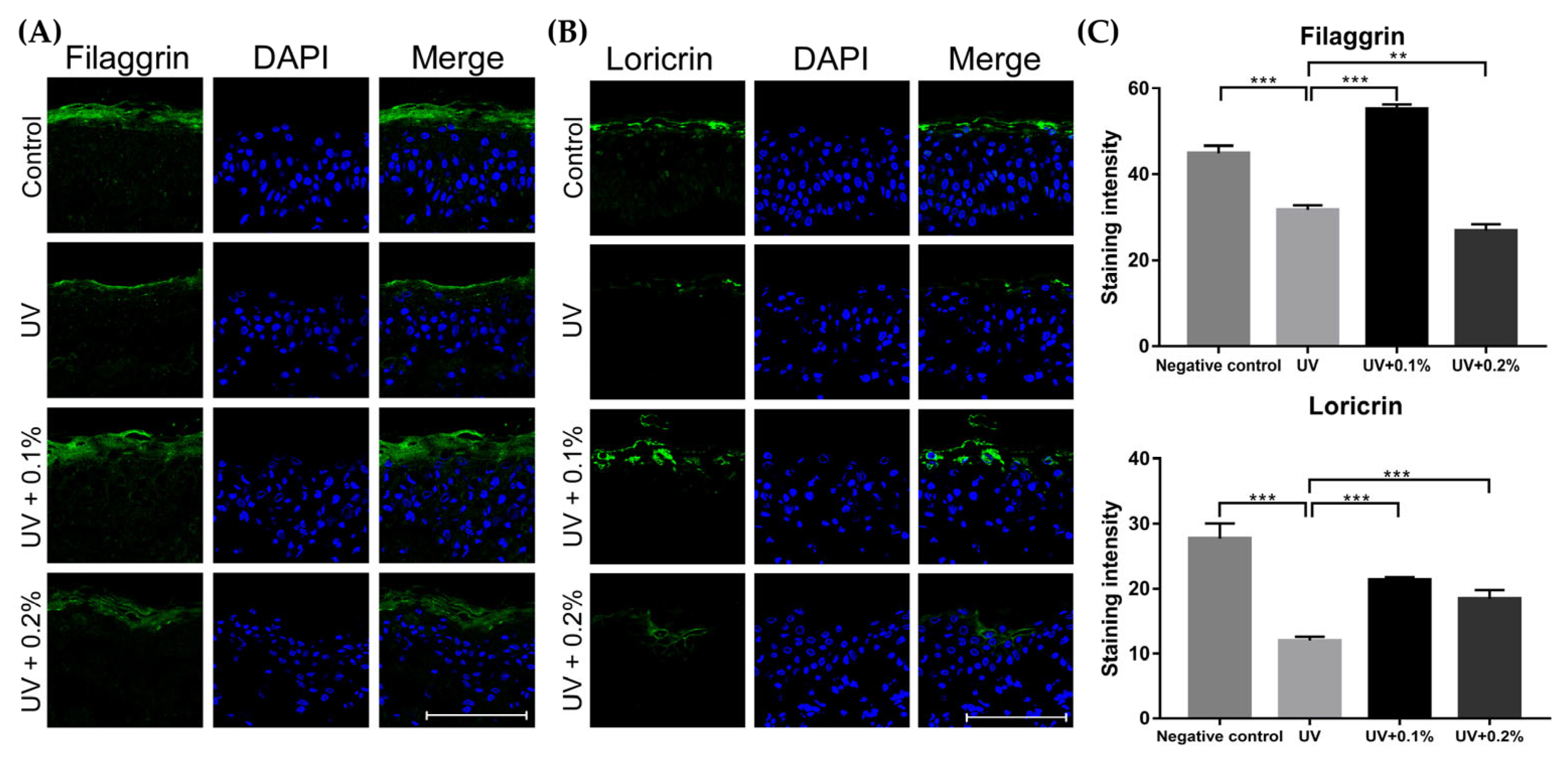
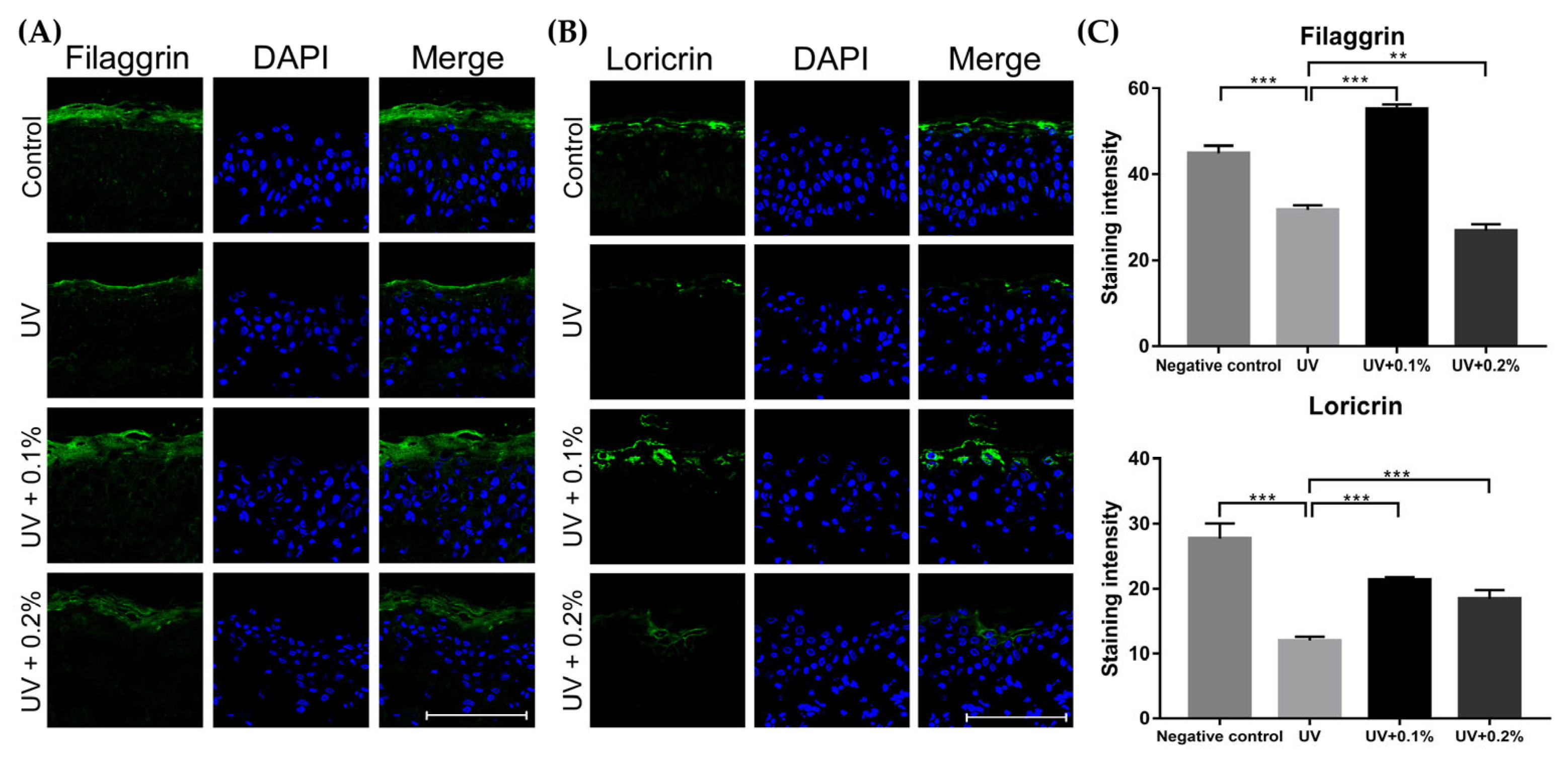
2.4. Ex Vivo Study on the Effect of H.ECMTM Liposomes on Skin Barrier Function and Hydration
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Application of an H.ECMTM Liposome-Containing Emollient Containing Proteoglycan Combined with Hyaluronic Acid and Collagen
4.3. Assessments for Clinical Efficacy
4.4. Cell Culture
4.5. Cell Cytotoxicity Measurement
4.6. Enzyme-Linked Immunosorbent Assay
4.7. Tissue Culture
4.8. Quantitative Reverse Transcription PCR
4.9. Immunofluorescence Staining
4.10. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ooi, K. Onset mechanism and pharmaceutical management of dry skin. Biol. Pharm. Bull. 2021, 44, 1037–1043. [Google Scholar] [CrossRef]
- Danby, S.G.; Andrew, P.V.; Brown, K.; Chittock, J.; Kay, L.J.; Cork, M.J. An investigation of the skin barrier restoring effects of a cream and lotion containing ceramides in a multi-vesicular emulsion in people with dry, eczema-prone, skin: The restore study phase 1. Dermatol. Ther. 2020, 10, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Chung, B.Y.; Kim, H.O.; Kang, S.Y.; Jung, M.J.; Kim, S.W.; Yoo, K.S.; Shin, K.O.; Jeong, S.K.; Park, C.W. Increased 1-deoxysphingolipids and skin barrier dysfunction in the skin of x-ray or ultraviolet b irradiation and atopic dermatitis lesion could be prevented by moisturizer with physiological lipid mixture. Ann. Dermatol. 2020, 32, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Holleran, W.M.; Uchida, Y.; Halkier-Sorensen, L.; Haratake, A.; Hara, M.; Epstein, J.H.; Elias, P.M. Structural and biochemical basis for the uvb-induced alterations in epidermal barrier function. Photodermatol. Photoimmunol. Photomed. 1997, 13, 117–128. [Google Scholar] [CrossRef]
- Abe, T.; Mayuzumi, J. The change and recovery of human skin barrier functions after ultraviolet light irradiation. Chem. Pharm. Bull. 1979, 27, 458–462. [Google Scholar] [CrossRef] [Green Version]
- Iozzo, R.V.; Schaefer, L. Proteoglycan form and function: A comprehensive nomenclature of proteoglycans. Matrix Biol. 2015, 42, 11–55. [Google Scholar] [CrossRef] [PubMed]
- Sashinami, H.; Takagaki, K.; Nakane, A. Salmon cartilage proteoglycan modulates cytokine responses to escherichia coli in mouse macrophages. Biochem. Biophys. Res. Commun. 2006, 351, 1005–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirose, S.; Narita, K.; Asano, K.; Nakane, A. Salmon cartilage proteoglycan promotes the healing process of staphylococcus aureus-infected wound. Heliyon 2018, 4, e00587. [Google Scholar] [CrossRef]
- Hardingham, T.E.; Fosang, A.J. Proteoglycans: Many forms and many functions. FASEB J. 1992, 6, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Miyanaga, M.; Uchiyama, T.; Motoyama, A.; Ochiai, N.; Ueda, O.; Ogo, M. Oral supplementation of collagen peptides improves skin hydration by increasing the natural moisturizing factor content in the stratum corneum: A randomized, double-blind, placebo-controlled clinical trial. Skin Pharmacol. Physiol. 2021, 34, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.H.; Schachter, J.; Sutton, A.B.; Salsberg, J.M.; Li, M.K.; Humphrey, S.D.; Dayeh, N.R. 89% vichy mineralizing water with hyaluronic acid is a well-tolerated adjunct treatment that helps restore skin barrier function in dry skin-related inflammatory dermatoses and post-procedure skin care: A canadian study. J. Cosmet. Dermatol. 2021, 20, 2148–2155. [Google Scholar] [CrossRef]
- Simon, D.; Nobbe, S.; Nageli, M.; Barysch, M.; Kunz, M.; Borelli, S.; Hasan-Ali, O.; Wildi, E.; Gasser, U.E. Short- and long-term effects of two emollients on itching and skin restoration in xerotic eczema. Dermatol. Ther. 2018, 31, e12692. [Google Scholar] [CrossRef]
- Lee, D.H.; Oh, J.H.; Chung, J.H. Glycosaminoglycan and proteoglycan in skin aging. J. Dermatol. Sci. 2016, 83, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Choi, F.D.; Sung, C.T.; Juhasz, M.L.; Mesinkovsk, N.A. Oral collagen supplementation: A systematic review of dermatological applications. J. Drugs Dermatol. 2019, 18, 9–16. [Google Scholar] [PubMed]
- Proksch, E.; Segger, D.; Degwert, J.; Schunck, M.; Zague, V.; Oesser, S. Oral supplementation of specific collagen peptides has beneficial effects on human skin physiology: A double-blind, placebo-controlled study. Skin Pharmacol. Physiol. 2014, 27, 47–55. [Google Scholar] [CrossRef]
- Jhawar, N.; Wang, J.V.; Saedi, N. Oral collagen supplementation for skin aging: A fad or the future? J. Cosmet. Dermatol. 2020, 19, 910–912. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.I.; Lee, S.G.; Kim, E.; Jung, I.; Suk, J.; Kim, J.; Lee, J.H. Anti-aging effect of an oral disintegrating collagen film: A prospective, single-arm study. Int. J. Dermatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Garre, A.; Narda, M.; Valderas-Martinez, P.; Piquero, J.; Granger, C. Antiaging effects of a novel facial serum containing l-ascorbic acid, proteoglycans, and proteoglycan-stimulating tripeptide: Ex vivo skin explant studies and in vivo clinical studies in women. Clin. Cosmet. Investig. Dermatol. 2018, 11, 253–263. [Google Scholar] [CrossRef] [Green Version]
- Bukhari, S.N.A.; Roswandi, N.L.; Waqas, M.; Habib, H.; Hussain, F.; Khan, S.; Sohail, M.; Ramli, N.A.; Thu, H.E.; Hussain, Z. Hyaluronic acid, a promising skin rejuvenating biomedicine: A review of recent updates and pre-clinical and clinical investigations on cosmetic and nutricosmetic effects. Int. J. Biol. Macromol. 2018, 120, 1682–1695. [Google Scholar] [CrossRef]
- Juncan, A.M.; Moisa, D.G.; Santini, A.; Morgovan, C.; Rus, L.L.; Vonica-Tincu, A.L.; Loghin, F. Advantages of hyaluronic acid and its combination with other bioactive ingredients in cosmeceuticals. Molecules 2021, 26, 4429. [Google Scholar] [CrossRef]
- Kang, M.C.; Yumnam, S.; Kim, S.Y. Oral intake of collagen peptide attenuates ultraviolet b irradiation-induced skin dehydration in vivo by regulating hyaluronic acid synthesis. Int. J. Mol. Sci. 2018, 19, 3551. [Google Scholar] [CrossRef] [Green Version]
- Asserin, J.; Lati, E.; Shioya, T.; Prawitt, J. The effect of oral collagen peptide supplementation on skin moisture and the dermal collagen network: Evidence from an ex vivo model and randomized, placebo-controlled clinical trials. J. Cosmet. Dermatol. 2015, 14, 291–301. [Google Scholar] [CrossRef] [Green Version]
- Oba, C.; Ohara, H.; Morifuji, M.; Ito, K.; Ichikawa, S.; Kawahata, K.; Koga, J. Collagen hydrolysate intake improves the loss of epidermal barrier function and skin elasticity induced by uvb irradiation in hairless mice. Photodermatol. Photoimmunol. Photomed. 2013, 29, 204–211. [Google Scholar] [CrossRef]
- Hsu, T.F.; Su, Z.R.; Hsieh, Y.H.; Wang, M.F.; Oe, M.; Matsuoka, R.; Masuda, Y. Oral hyaluronan relieves wrinkles and improves dry skin: A 12-week double-blinded, placebo-controlled study. Nutrients 2021, 13, 2220. [Google Scholar] [CrossRef]
- Cabral, L.R.B.; Teixeira, L.N.; Gimenez, R.P.; Demasi, A.P.D.; de Brito Junior, R.B.; de Araujo, V.C.; Martinez, E.F. Effect of hyaluronic acid and poly-l-lactic acid dermal fillers on collagen synthesis: An in vitro and in vivo study. Clin. Cosmet. Investig. Dermatol. 2020, 13, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Kalinin, A.; Marekov, L.N.; Steinert, P.M. Assembly of the epidermal cornified cell envelope. J. Cell Sci. 2001, 114, 3069–3070. [Google Scholar] [CrossRef]
- Candi, E.; Schmidt, R.; Melino, G. The cornified envelope: A model of cell death in the skin. Nat. Rev. Mol. Cell Biol. 2005, 6, 328–340. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.E.; Howell, M.D.; Guttman-Yassky, E.; Gilleaudeau, P.M.; Cardinale, I.R.; Boguniewicz, M.; Krueger, J.G.; Leung, D.Y. Tnf-alpha downregulates filaggrin and loricrin through c-jun n-terminal kinase: Role for tnf-alpha antagonists to improve skin barrier. J. Investig. Dermatol. 2011, 131, 1272–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham, H.T.; Exelbert, L.; Segal-Owens, A.C.; Veves, A. A prospective, randomized, controlled double-blind study of a moisturizer for xerosis of the feet in patients with diabetes. Ostomy Wound Manag. 2002, 48, 30–36. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.I.; Lee, S.G.; Kim, J.; Choi, S.; Jung, I.; Lee, J.H. Proteoglycan Combined with Hyaluronic Acid and Hydrolyzed Collagen Restores the Skin Barrier in Mild Atopic Dermatitis and Dry, Eczema-Prone Skin: A Pilot Study. Int. J. Mol. Sci. 2021, 22, 10189. https://doi.org/10.3390/ijms221910189
Lee YI, Lee SG, Kim J, Choi S, Jung I, Lee JH. Proteoglycan Combined with Hyaluronic Acid and Hydrolyzed Collagen Restores the Skin Barrier in Mild Atopic Dermatitis and Dry, Eczema-Prone Skin: A Pilot Study. International Journal of Molecular Sciences. 2021; 22(19):10189. https://doi.org/10.3390/ijms221910189
Chicago/Turabian StyleLee, Young In, Sang Gyu Lee, Jemin Kim, Sooyeon Choi, Inhee Jung, and Ju Hee Lee. 2021. "Proteoglycan Combined with Hyaluronic Acid and Hydrolyzed Collagen Restores the Skin Barrier in Mild Atopic Dermatitis and Dry, Eczema-Prone Skin: A Pilot Study" International Journal of Molecular Sciences 22, no. 19: 10189. https://doi.org/10.3390/ijms221910189
APA StyleLee, Y. I., Lee, S. G., Kim, J., Choi, S., Jung, I., & Lee, J. H. (2021). Proteoglycan Combined with Hyaluronic Acid and Hydrolyzed Collagen Restores the Skin Barrier in Mild Atopic Dermatitis and Dry, Eczema-Prone Skin: A Pilot Study. International Journal of Molecular Sciences, 22(19), 10189. https://doi.org/10.3390/ijms221910189