The Reduction in Gastric Atrophy after Helicobacter pylori Eradication Is Reduced by Treatment with Inhibitors of Gastric Acid Secretion

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
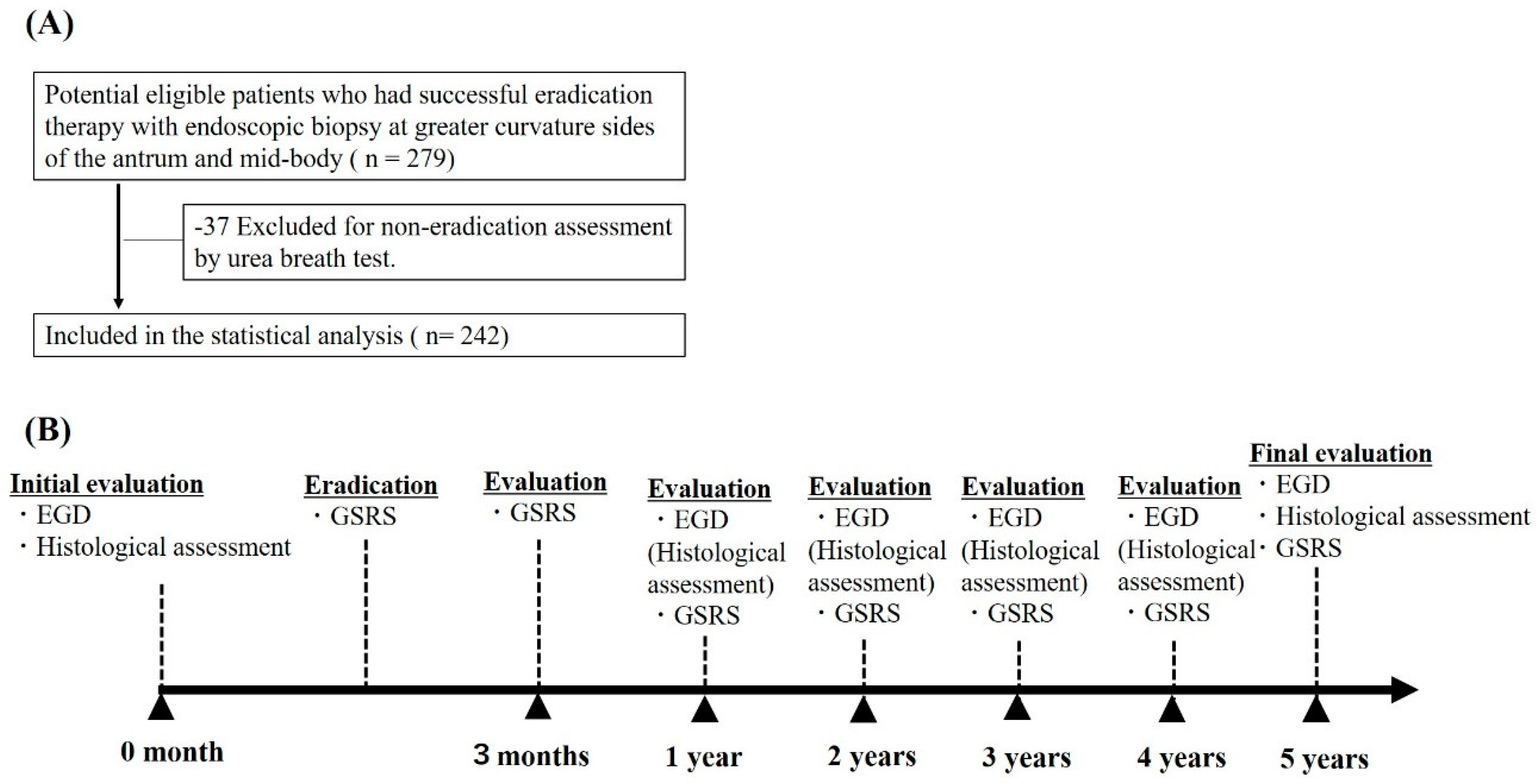
2.1. Patients
2.2. Changes in the Updated Sydney System Scores and Association with Drug Use
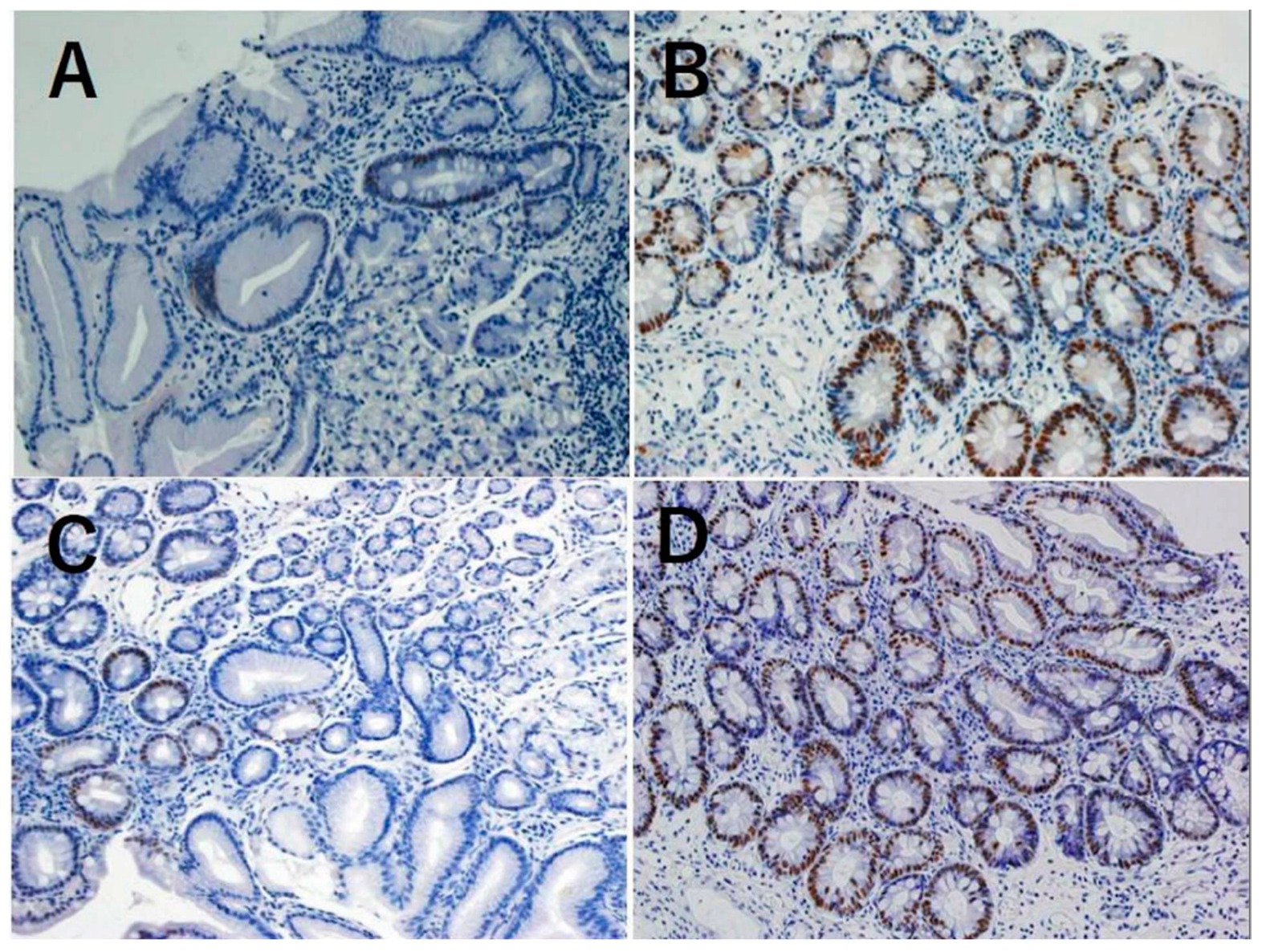
2.3. Association between Caudal Related Homeobox Gene (CDX)1 and CDX2 Expression and Changes in Metaplasia and Atrophy Scores
3. Discussion
4. Methods
4.1. Study Design and Setting
4.2. Participants
4.3. Eradication Treatment and Assessment
4.4. Upper Gastrointestinal Endoscopy and Histological Examination
4.5. Outcomes and Variables
4.6. Immunohistochemical Stain Analyses of CDX1 and CDX2 Expression
4.7. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| H. pylori | Helicobacter pylori |
| PPIs | proton pump inhibitors |
| H2RAs | H2 receptor antagonists |
References
- Shichijo, S.; Hirata, Y.; Niikura, R.; Hayakawa, Y.; Yamada, A.; Ushiku, T.; Fukayama, M.; Koike, K. Histologic intestinal metaplasia and endoscopic atrophy are predictors of gastric cancer development after helicobacter pylori eradication. Gastrointest. Endosc. 2016, 84, 618–624. [Google Scholar] [CrossRef]
- Murakami, K.; Kodama, M.; Nakagawa, Y.; Mizukami, K.; Okimoto, T.; Fujioka, T. Long-term monitoring of gastric atrophy and intestinal metaplasia after helicobacter pylori eradication. Clin. J. Gastroenterol. 2012, 5, 247–250. [Google Scholar] [CrossRef]
- Kodama, M.; Murakami, K.; Okimoto, T.; Abe, T.; Nakagawa, Y.; Mizukami, K.; Uchida, M.; Inoue, K.; Fujioka, T. Helicobacter pylori eradication improves gastric atrophy and intestinal metaplasia in long-term observation. Digestion 2012, 85, 126–130. [Google Scholar] [CrossRef]
- Toyokawa, T.; Suwaki, K.; Miyake, Y.; Nakatsu, M.; Ando, M. Eradication of helicobacter pylori infection improved gastric mucosal atrophy and prevented progression of intestinal metaplasia, especially in the elderly population: A long-term prospective cohort study. J. Gastroenterol. Hepatol. 2010, 25, 544–547. [Google Scholar] [CrossRef]
- Rocco, A.; Suriani, R.; Cardesi, E.; Venturini, I.; Mazzucco, D.; Nardone, G. Gastric atrophy and intestinal metaplasia changes 8 years after helicobacter pylori eradication. A blind, randomised study. Minerva Gastroenterol. Dietol. 2002, 48, 175–178. [Google Scholar] [PubMed]
- Fukase, K.; Kato, M.; Kikuchi, S.; Inoue, K.; Uemura, N.; Okamoto, S.; Terao, S.; Amagai, K.; Hayashi, S.; Asaka, M.; et al. Effect of eradication of helicobacter pylori on incidence of metachronous gastric carcinoma after endoscopic resection of early gastric cancer: An open-label, randomised controlled trial. Lancet 2008, 372, 392–397. [Google Scholar] [CrossRef]
- Kong, Y.J.; Yi, H.G.; Dai, J.C.; Wei, M.X. Histological changes of gastric mucosa after helicobacter pylori eradication: A systematic review and meta-analysis. World J. Gastroenterol. 2014, 20, 5903–5911. [Google Scholar] [CrossRef]
- Testoni, P.A.; Masci, E.; Marchi, R.; Guslandi, M.; Ronchi, G.; Tittobello, A. Gastric cancer in chronic atrophic gastritis. associated gastric ulcer adds no further risk. J. Clin. Gastroenterol. 1987, 9, 298–302. [Google Scholar] [CrossRef]
- Uemura, N.; Okamoto, S.; Yamamoto, S.; Matsumura, N.; Yamaguchi, S.; Yamakido, M.; Taniyama, K.; Sasaki, N.; Schlemper, R.J. Helicobacter pylori infection and the development of gastric cancer. N. Engl. J. Med. 2001, 345, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Waldum, H.L.; Fossmark, R. Types of gastric carcinomas. Int. J. Mol. Sci. 2018, 19, 4109. [Google Scholar] [CrossRef] [PubMed]
- Waldum, H.L.; Hauso, O.; Sordal, O.F.; Fossmark, R. Gastrin may mediate the carcinogenic effect of helicobacter pylori infection of the stomach. Dig. Dis. Sci. 2015, 60, 1522–1527. [Google Scholar] [CrossRef]
- Cheung, K.S.; Chan, E.W.; Wong, A.Y.S.; Chen, L.; Wong, I.C.K.; Leung, W.K. Long-term proton pump inhibitors and risk of gastric cancer development after treatment for helicobacter pylori: A population-based study. Gut 2018, 67, 28–35. [Google Scholar] [CrossRef]
- Niikura, R.; Hayakawa, Y.; Hirata, Y.; Yamada, A.; Fujishiro, M.; Koike, K. Long-term proton pump inhibitor use is a risk factor of gastric cancer after treatment for helicobacter pylori: A retrospective cohort analysis. Gut 2018, 67, 1908–1910. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, H.; Hayakawa, Y.; Koike, K. Metaplasia in the stomach-precursor of gastric cancer? Int. J. Mol. Sci. 2017, 18, 2063. [Google Scholar] [CrossRef] [PubMed]
- Spence, A.D.; Cardwell, C.R.; McMenamin, U.C.; Hicks, B.M.; Johnston, B.T.; Murray, L.J.; Coleman, H.G. Adenocarcinoma risk in gastric atrophy and intestinal metaplasia: A systematic review. BMC Gastroenterol. 2017, 17, 157. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. the updated sydney system. international workshop on the histopathology of gastritis, houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef] [PubMed]
- Shichijo, S.; Hirata, Y.; Sakitani, K.; Yamamoto, S.; Serizawa, T.; Niikura, R.; Watabe, H.; Yoshida, S.; Yamada, A.; Yamaji, Y. Distribution of intestinal metaplasia as a predictor of gastric cancer development. J. Gastroenterol. Hepatol. 2015, 30, 1260–1264. [Google Scholar] [CrossRef] [PubMed]
- Svedlund, J.; Sjodin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef]
- Choi, I.J.; Kook, M.C.; Kim, Y.I.; Cho, S.J.; Lee, J.Y.; Kim, C.G.; Park, B.; Nam, B.H. Helicobacter pylori therapy for the prevention of metachronous gastric cancer. N. Engl. J. Med. 2018, 378, 1085–1095. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Kim, N.; Baek, S.M.; Lee, H.S.; Lee, J.; Hwang, Y.J.; Yoon, H.; Shin, C.M.; Park, Y.S.; Kim, J.W. The prevalence of histologic atrophy and intestinal metaplasia in the corpus has decreased over 15 years in females in the korean population. Helicobacter 2019. [Google Scholar] [CrossRef]
- Hwang, Y.J.; Kim, N.; Lee, H.S.; Lee, J.B.; Choi, Y.J.; Yoon, H.; Shin, C.M.; Park, Y.S.; Lee, D.H. Reversibility of atrophic gastritis and intestinal metaplasia after helicobacter pylori eradication—A prospective study for up to 10 years. Aliment. Pharmacol. Ther. 2018, 47, 380–390. [Google Scholar] [CrossRef]
- Rokkas, T.; Pistiolas, D.; Sechopoulos, P.; Robotis, I.; Margantinis, G. The long-term impact of helicobacter pylori eradication on gastric histology: A systematic review and meta-analysis. Helicobacter 2007, 12 (Suppl. 2), 32–38. [Google Scholar] [CrossRef]
- Wang, J.; Xu, L.; Shi, R.; Huang, X.; Li, S.W.; Huang, Z.; Zhang, G. Gastric atrophy and intestinal metaplasia before and after helicobacter pylori eradication: A meta-analysis. Digestion 2011, 83, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Kong, P.; Wu, R.; Liu, X.; Liu, J.; Chen, S.; Ye, M.; Yang, C.; Song, Z.; He, W.; Yin, C. The effects of anti-inflammatory drug treatment in gastric cancer prevention: An update of a meta-analysis. J. Cancer 2016, 7, 2247–2257. [Google Scholar] [CrossRef] [PubMed]
- Mutoh, H.; Sakurai, S.; Satoh, K.; Osawa, H.; Hakamata, Y.; Takeuchi, T.; Sugano, K. Cdx1 induced intestinal metaplasia in the transgenic mouse stomach: Comparative study with Cdx2 transgenic mice. Gut 2004, 53, 1416–1423. [Google Scholar] [CrossRef] [PubMed]
- Kodama, M.; Murakami, K.; Okimoto, T.; Sato, R.; Uchida, M.; Abe, T.; Shiota, S.; Nakagawa, Y.; Mizukami, K.; Fujioka, T. Ten-year prospective follow-up of histological changes at five points on the gastric mucosa as recommended by the updated sydney system after helicobacter pylori eradication. J. Gastroenterol. 2012, 47, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Mera, R.M.; Bravo, L.E.; Camargo, M.C.; Bravo, J.C.; Delgado, A.G.; Romero-Gallo, J.; Yepez, M.C.; Realpe, J.L.; Schneider, B.G.; Morgan, D.R. Dynamics of helicobacter pylori infection as a determinant of progression of gastric precancerous lesions: 16-year follow-up of an eradication trial. Gut 2018, 67, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Annibale, B.; Di Giulio, E.; Caruana, P.; Lahner, E.; Capurso, G.; Bordi, C.; Delle Fave, G. The long-term effects of cure of helicobacter pylori infection on patients with atrophic body gastritis. Aliment. Pharmacol. Ther. 2002, 16, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Zhao, C.M.; Dockray, G.J.; Varro, A.; Van Hoek, A.; Sinclair, N.F.; Wang, T.C.; Koh, T.J. Glycine-extended gastrin synergizes with gastrin 17 to stimulate acid secretion in gastrin-deficient mice. Gastroenterology 2000, 119, 756–765. [Google Scholar] [CrossRef]
- Takaishi, S.; Cui, G.; Frederick, D.M.; Carlson, J.E.; Houghton, J.; Varro, A.; Dockray, G.J.; Ge, Z.; Whary, M.T.; Rogers, A.B. Synergistic inhibitory effects of gastrin and histamine receptor antagonists on helicobacter-induced gastric cancer. Gastroenterology 2005, 128, 1965–1983. [Google Scholar] [CrossRef]
- Hagiwara, T.; Mukaisho, K.; Nakayama, T.; Sugihara, H.; Hattori, T. Long-term proton pump inhibitor administration worsens atrophic corpus gastritis and promotes adenocarcinoma development in mongolian gerbils infected with helicobacter pylori. Gut 2011, 60, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, E.J.; Uyterlinde, A.M.; Pena, A.S.; Hazenberg, H.J.; Bloemena, E.; Lindeman, J.; Klinkenberg-Knol, E.C.; Meuwissen, S.G. Increase of helicobacter pylori-associated corpus gastritis during acid suppressive therapy: Implications for long-term safety. Am. J. Gastroenterol. 1995, 90, 1401–1406. [Google Scholar] [PubMed]
- Kuipers, E.J.; Lundell, L.; Klinkenberg-Knol, E.C.; Havu, N.; Festen, H.P.; Liedman, B.; Lamers, C.B.; Jansen, J.B.; Dalenback, J.; Snel, P. Atrophic gastritis and helicobacter pylori infection in patients with reflux esophagitis treated with omeprazole or fundoplication. N. Engl. J. Med. 1996, 334, 1018–1022. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | No. of Patients (%) | p Value | ||
|---|---|---|---|---|
| PPI Use (n = 110) | H2RA Use (n = 33) | Non-Acid Suppressant Use (n = 99) | ||
| Age category (years) | ||||
| <50 | 4 (3.63) | 5 (15.15) | 6 (6.06) | 0.564 |
| 50–60 | 12 (10.91) | 4 (12.13) | 19 (19.19) | |
| 60–70 | 37 (33.64) | 11 (33.33) | 37 (37.37) | |
| 70–80 | 46 (41.82) | 13 (39.39) | 35 (35.35) | |
| ≥80 | 11 (10.00) | 0 | 2 (2.02) | |
| Sex | ||||
| Female | 49 (44.55) | 20 (60.61) | 44 (44.44) | 0.202 |
| Male | 61 (55.45) | 13 (39.39) | 55 (55.56) | |
| NSAID use | 51 (46.36) | 17 (51.52) | 24 (24.24) | <0.001 |
| Sydney System Factor Score | ||||
| Atrophy antrum | 1.221 ± 0.778 | 1.160 ± 0.898 | 0.986 ± 0.778 | 0.254 |
| corpus | 0.755 ± 0.860 | 0.429 ± 0.898 | 0.613 ± 0.751 | 0.140 |
| Metaplasia antrum | 0.633 ± 0.889 | 0.515 ± 0.667 | 0.443 ± 0.667 | 0.411 |
| corpus | 0.284 ± 0.708 | 0.156 ± 0.448 | 0.122 ± 0.503 | 0.116 |
| Mononuclear cell antrum | 1.211 ± 0.639 | 1.303 ± 0.684 | 1.243 ± 0.648 | 0.713 |
| corpus | 1.211 ± 0.759 | 1.273 ± 0.674 | 1.102 ± 0.681 | 0.428 |
| Neutrophil antrum | 0.352 ± 0.646 | 0.455 ± 0.833 | 0.427 ± 0.778 | 0.925 |
| corpus | 0.444 ± 0.777 | 0.424 ± 0.708 | 0.433 ± 0.776 | 0.947 |
| H. pylori antrum | 0.389 ± 0.783 | 0.273 ± 0.626 | 0.333 ± 0.660 | 0.769 |
| corpus | 0.333 ± 0.641 | 0.424 ± 0.969 | 0.443 ± 0.841 | 0.826 |
| Sydney System Factor | PPI Use (n = 110) | H2RA Use (n = 33) | Non-Acid Suppressant Use (n = 99) | p Value |
|---|---|---|---|---|
| Score Coefficient (Point), Per Year (95% CI) | ||||
| Atrophy antrum | −0.004 (−0.028 to 0.020) | −0.011 (−0.060 to 0.039) | −0.036 (−0.059 to −0.012) | 0.042 |
| corpus | −0.023 (−0.045 to −0.0002) | −0.021 (−0.050 to 0.009) | −0.030 (−0.052 to −0.007) | 0.020 |
| Metaplasia antrum | 0.014 (−0.009 to 0.036) | −0.031 (−0.069 to 0.007) | −0.007 (−0.030 to 0.015) | 0.271 |
| corpus | −0.003 (−0.020 to 0.013) | −0.007 (−0.033 to 0.019) | 0.001 (−0.012 to 0.015) | 0.077 |
| Mononuclear cell antrum | −0.050 (−0.064 to −0.035) | −0.050 (−0.080 to −0.020) | −0.055 (−0.071 to −0.039) | 0.815 |
| corpus | −0.063 (−0.080 to −0.045) | −0.035 (−0.062 to −0.008) | −0.051 (−0.068 to −0.034) | 0.204 |
| Neutrophil antrum | −0.034 (−0.049 to −0.019) | −0.040 (−0.072 to −0.009) | −0.053 (−0.069 to −0.037) | 0.961 |
| corpus | −0.047 (−0.065 to −0.029) | −0.037 (−0.065 to −0.009) | −0.050 (−0.066 to −0.034) | 0.350 |
| H. pylori antrum | −0.038 (−0.055 to −0.020) | −0.027 (−0.052 to −0.001) | −0.043 (−0.057 to −0.028) | 0.395 |
| corpus | −0.040 (−0.056 to −0.023) | −0.042 (−0.082 to −0.003) | −0.060 (−0.078 to −0.041) | 0.906 |
| Sydney System Factor | PPI Long-term Use (n = 87) | PPI Short-term Use (n = 23) | p Value |
|---|---|---|---|
| Score Coefficient (Point), Per Year (95% CI) | |||
| Atrophy antrum | −0.002 (−0.029 to 0.026) | −0.016 (−0.075 to 0.043) | 0.189 |
| corpus | −0.021 (−0.045 to 0.003) | −0.027 (−0.095 to 0.041) | 0.016 |
| Metaplasia antrum | 0.014 (−0.011 to 0.039) | 0.006 (−0.048 to 0.060) | 0.639 |
| corpus | −0.0001 (−0.017 to 0.017) | −0.040 (−0.092 to 0.012) | 0.177 |
| Mononuclear cell antrum | −0.052 (−0.067 to −0.037) | −0.036 (−0.082 to 0.009) | 0.957 |
| corpus | −0.064 (−0.084 to −0.045) | −0.051 (−0.088 to −0.013) | 0.656 |
| Neutrophil antrum | −0.028 (−0.043 to −0.012) | −0.060 (−0.102 to −0.018) | 0.682 |
| corpus | −0.042 (−0.063 to −0.022) | −0.070 (−0.110 to −0.030) | 0.777 |
| H. pylori antrum | −0.032 (−0.049 to −0.014) | −0.067 (−0.128 to −0.006) | 0.107 |
| corpus | −0.038 (−0.057 to −0.019) | −0.044 (−0.078 to −0.010) | 0.631 |
| Sydney System Factor | H2RA Long-term Use (n = 16) | H2RA Short-term Use (n = 17) | p Value |
|---|---|---|---|
| Score Coefficient (Point), Per Year (95% CI) | |||
| Atrophy antrum | −0.037 (−0.117 to 0.044) | 0.045 (−0.056 to 0.147) | 0.382 |
| corpus | −0.034 (−0.067 to −0.001) | 0.005 (−0.056 to 0.066) | 0.108 |
| Metaplasia antrum | −0.053 (−0.100 to −0.0057) | −0.022 (−0.075 to 0.031) | 0.296 |
| corpus | −0.021 (−0.066 to 0.024) | −0.008 (−0.035 to 0.019) | 0.350 |
| Mononuclear cell antrum | −0.039 (−0.085 to 0.007) | −0.078 (−0.135 to −0.022) | 0.567 |
| corpus | −0.026 (−0.070 to 0.017) | −0.051 (−0.102 to −0.001) | 0.988 |
| Neutrophil antrum | −0.034 (−0.076 to 0.009) | −0.066 (−0.129 to −0.002) | 0.681 |
| corpus | −0.026 (−0.061 to 0.009) | −0.063 (−0.124 to −0.003) | 0.692 |
| H. pylori antrum | −0.023 (−0.057 to 0.010) | −0.065 (−0.144 to 0.015) | 0.443 |
| corpus | −0.035 (−0.084 to 0.014) | −0.038 (−0.091 to 0.015) | 0.633 |
| Metaplasia Change | CDX1 Expression Rates, Mean ± SD | p Value | |
| Initial assessment | Final assessment | ||
| Improvement | |||
| Antrum (N = 25) | 0.217 ± 0.231 | 0.033 ± 0.091 | <0.001 |
| Corpus (N = 11) | 0.092 ± 0.103 | 0.008 ± 0.022 | 0.019 |
| Exacerbation | |||
| Antrum (N = 21) | 0.059 ± 0.132 | 0.100 ± 0.169 | 0.128 |
| Corpus (N = 6) | 0.002 ± 0.005 | 0.093 ± 0.105 | 0.080 |
| Metaplasia Change | CDX2 Expression Rate, Mean ± SD | p Value | |
| Initial Assessment | Final Assessment | ||
| Improvement | |||
| Antrum (N = 25) | 0.195 ± 0.194 | 0.031 ± 0.059 | <0.001 |
| Corpus (N = 11) | 0.128 ± 0.168 | 0.069 ± 0.211 | 0.401 |
| Exacerbation | |||
| Antrum (N = 21) | 0.060 ± 0.100 | 0.114 ± 0.156 | 0.079 |
| Corpus (N = 6) | 0.003 ± 0.007 | 0.103 ± 0.155 | 0.159 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niikura, R.; Hayakawa, Y.; Hirata, Y.; Ogura, K.; Fujishiro, M.; Yamada, A.; Ushiku, T.; Konishi, M.; Fukayama, M.; Koike, K. The Reduction in Gastric Atrophy after Helicobacter pylori Eradication Is Reduced by Treatment with Inhibitors of Gastric Acid Secretion. Int. J. Mol. Sci. 2019, 20, 1913. https://doi.org/10.3390/ijms20081913
Niikura R, Hayakawa Y, Hirata Y, Ogura K, Fujishiro M, Yamada A, Ushiku T, Konishi M, Fukayama M, Koike K. The Reduction in Gastric Atrophy after Helicobacter pylori Eradication Is Reduced by Treatment with Inhibitors of Gastric Acid Secretion. International Journal of Molecular Sciences. 2019; 20(8):1913. https://doi.org/10.3390/ijms20081913
Chicago/Turabian StyleNiikura, Ryota, Yoku Hayakawa, Yoshihiro Hirata, Keiji Ogura, Mitsuhiro Fujishiro, Atsuo Yamada, Tetsuo Ushiku, Mitsuru Konishi, Masashi Fukayama, and Kazuhiko Koike. 2019. "The Reduction in Gastric Atrophy after Helicobacter pylori Eradication Is Reduced by Treatment with Inhibitors of Gastric Acid Secretion" International Journal of Molecular Sciences 20, no. 8: 1913. https://doi.org/10.3390/ijms20081913
APA StyleNiikura, R., Hayakawa, Y., Hirata, Y., Ogura, K., Fujishiro, M., Yamada, A., Ushiku, T., Konishi, M., Fukayama, M., & Koike, K. (2019). The Reduction in Gastric Atrophy after Helicobacter pylori Eradication Is Reduced by Treatment with Inhibitors of Gastric Acid Secretion. International Journal of Molecular Sciences, 20(8), 1913. https://doi.org/10.3390/ijms20081913