
Vitamin C Supplementation for the Treatment of COVID-19: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Assessment of Risk of Bias in Included Studies
2.5. Statistical Analysis
3. Results
3.1. Literature Search
3.2. Trials Characteristics and Risk of Bias Assessment
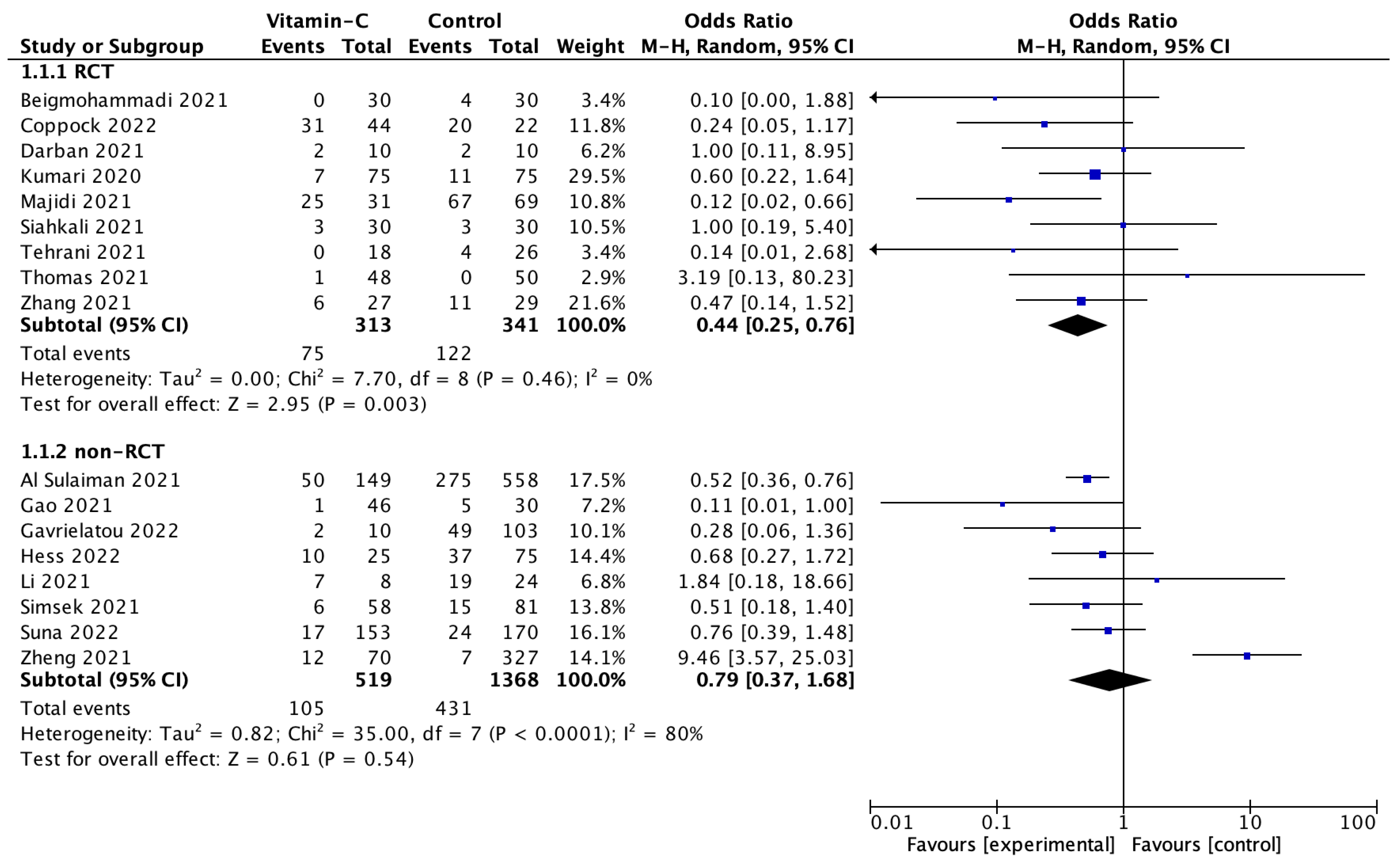
3.3. Data Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muralidar, S.; Ambi, S.V.; Sekaran, S.; Krishnan, U.M. The emergence of COVID-19 as a global pandemic: Understanding the epidemiology, immune response and potential therapeutic targets of SARS-CoV-2. Biochimie 2020, 179, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Korompoki, E.; Fotiou, D.; Migkou, M.; Tzanninis, I.G.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Emerging treatment strategies for COVID-19 infection. Clin. Exp. Med. 2021, 21, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Szarpak, L.; Pruc, M.; Gasecka, A.; Jaguszewski, M.J.; Michalski, T.; Peacock, F.W.; Smereka, J.; Pytkowska, K.; Filipiak, K.J. Should we supplement zinc in COVID-19 patients? Evidence from a meta-analysis. Pol. Arch. Intern. Med. 2021, 131, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Pourkarim, F.; Pourtaghi-Anvarian, S.; Rezaee, H. Molnupiravir: A new candidate for COVID-19 treatment. Pharmacol. Res. Perspect. 2022, 10, e00909. [Google Scholar] [CrossRef]
- Bae, M.; Kim, H. Mini-Review on the Roles of Vitamin C, Vitamin D, and Selenium in the Immune System against COVID-19. Molecules 2020, 25, 5346. [Google Scholar] [CrossRef]
- Shakoor, H.; Feehan, J.; Al Dhaheri, A.S.; Ali, H.I.; Platat, C.; Ismail, L.C.; Apostolopoulos, V.; Stojanovska, L. Immune-boosting role of vitamins D, C, E, zinc, selenium and omega-3 fatty acids: Could they help against COVID-19? Maturitas 2021, 143, 1–9. [Google Scholar] [CrossRef]
- Padayatty, S.J.; Katz, A.; Wang, Y.; Eck, P.; Kwon, O.; Lee, J.H.; Chen, S.; Corpe, C.; Dutta, A.; Dutta, S.K.; et al. Vitamin C as an antioxidant: Evaluation of its role in disease prevention. J. Am. Coll. Nutr. 2003, 22, 18–35. [Google Scholar] [CrossRef]
- Kocot, J.; Luchowska-Kocot, D.; Kiełczykowska, M.; Musik, I.; Kurzepa, J. Does Vitamin C Influence Neurodegenerative Diseases and Psychiatric Disorders? Nutrients 2017, 9, 659. [Google Scholar] [CrossRef]
- Carr, A.; Frei, B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J. 1999, 13, 1007–1024. [Google Scholar] [CrossRef]
- Kaźmierczak-Barańska, J.; Boguszewska, K.; Adamus-Grabicka, A.; Karwowski, B.T. Two Faces of Vitamin C-Antioxidative and Pro-Oxidative Agent. Nutrients 2020, 12, 1501. [Google Scholar] [CrossRef]
- Shilotri, P.; Bhat, K. Effect of mega doses of vitamin C on bactericidal ativity of leukocytes. Am. J. Clin. Nutr. 1977, 30, 1077–1081. [Google Scholar] [CrossRef]
- Liugan, M.; Carr, A. Vitamin C and neutrophil function: Findings from randomized controlled trials. Nutrients 2019, 11, 2102. [Google Scholar] [CrossRef]
- Ferrón-Celma, I.; Mansilla, A.; Hassan, L.; Garcia-Navarro, A.; Comino, A.M.; Bueno, P.; Ferrón, J.A. Effect of vitamin C administration on neutrophil apoptosis in septic patients after abdominal surgery. J. Surg. Res. 2009, 153, 224–230. [Google Scholar] [CrossRef]
- Manning, J.; Mitchell, B.; Appadurai, D.A.; Shakya, A.; Pierce, L.J.; Wang, H.; Nganga, V.; Swanson, P.C.; May, J.M.; Tantin, D.; et al. Vitamin C promotes maturation of T-cells. Antioxid. Redox Signal. 2013, 19, 2054–2067. [Google Scholar] [CrossRef]
- Moores, J. Vitamin C: A wound healing perspective. Br. J. Community Nurs. 2013, 18, S8–S11. [Google Scholar] [CrossRef]
- Teafatiller, T.; Agrawal, S.; De Robles, G.; Rahmatpanah, F.; Subramanian, V.S.; Agrawal, A. Vitamin C Enhances Antiviral Functions of Lung Epithelial Cells. Biomolecules 2021, 11, 1148. [Google Scholar] [CrossRef]
- Miranda-Massari, J.R.; Toro, A.P.; Loh, D.; Rodriguez, J.R.; Borges, R.M.; Marcial-Vega, V.; Olalde, J.; Berdiel, M.J.; Riordan, N.H.; Martinez, J.M.; et al. The Effects of Vitamin C on the Multiple Pathophysiological Stages of COVID-19. Life 2021, 11, 1341. [Google Scholar] [CrossRef]
- Cerullo, G.; Negro, M.; Parimbelli, M.; Pecoraro, M.; Perna, S.; Liguori, G.; Rondanelli, M.; Cena, H.; D’Antona, G. The Long History of Vitamin C: From Prevention of the Common Cold to Potential Aid in the Treatment of COVID-19. Front. Immunol. 2020, 11, 574029. [Google Scholar] [CrossRef]
- Fashner, J.; Ericson, K.; Werner, S. Treatment of the common cold in children and adults. Am. Fam. Physician 2012, 86, 153–159. [Google Scholar]
- Carr, A.C.; Rowe, S. Factors Affecting Vitamin C Status and Prevalence of Deficiency: A Global Health Perspective. Nutrients 2020, 12, 1963. [Google Scholar] [CrossRef]
- Brant, E.; Angus, D. Is high-dose vitamin C beneficial for patients with sepsis? JAMA 2019, 322, 1257. [Google Scholar] [CrossRef] [PubMed]
- Padayatty, S.J.; Sun, H.; Wang, Y.; Riordan, H.D.; Hewitt, S.M.; Katz, A.; Wesley, R.A.; Levine, M. Vitamin C pharmacokinetics: Implications for oral and intravenous use. Ann. Intern. Med. 2004, 140, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Colunga Biancatelli, R.M.L.; Berrill, M.; Catravas, J.D.; Marik, P.E. Quercetin and Vitamin C: An Experimental, Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19). Front. Immunol. 2020, 11, 1451. [Google Scholar] [CrossRef] [PubMed]
- Milani, G.P.; Macchi, M.; Guz-Mark, A. Vitamin C in the Treatment of COVID-19. Nutrients 2021, 13, 1172. [Google Scholar] [CrossRef] [PubMed]
- Vollbracht, C.; Kraft, K. Feasibility of Vitamin C in the Treatment of Post Viral Fatigue with Focus on Long COVID, Based on a Systematic Review of IV Vitamin C on Fatigue. Nutrients 2021, 13, 1154. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Al Sulaiman, K.; Aljuhani, O.; Saleh, K.B.; Badreldin, H.A.; Al Harthi, A.; Alenazi, M.; Alharbi, A.; Algarni, R.; Al Harbi, S.; Alhammad, A.M.; et al. Ascorbic acid as an adjunctive therapy in critically ill patients with COVID-19: A propensity score matched study. Sci. Rep. 2021, 11, 17648. [Google Scholar] [CrossRef]
- Beigmohammadi, M.T.; Bitarafan, S.; Hoseindokht, A.; Abdollahi, A.; Amoozadeh, L.; Soltani, D. The effect of supplementation with vitamins A, B, C, D, and E on disease severity and inflammatory responses in patients with COVID-19: A randomized clinical trial. Trials 2021, 22, 802. [Google Scholar] [CrossRef]
- Coppock, D.; Violet, P.C.; Vasquez, G.; Belden, K.; Foster, M.; Mullin, B.; Magee, D.; Mikell, I.; Shah, L.; Powers, V.; et al. Pharmacologic Ascorbic Acid as Early Therapy for Hospitalized Patients with COVID-19: A Randomized Clinical Trial. Life 2022, 12, 453. [Google Scholar] [CrossRef]
- Darban, M.; Malek, F.; Memarian, M.; Gohari, A.; Kiani, A.; Emadi, A.; Lavvaf, S.; Bagheri, B. Efficacy of High Dose Vitamin C, Melatonin and Zinc in Iranian Patients with Acute Respiratory Syndrome due to Coronavirus Infection: A Pilot Randomized Trial. J. Cell. Mol. Anesth. 2021, 6, 164–167. [Google Scholar]
- Gao, D.; Xu, M.; Wang, G.; Lv, J.; Ma, X.; Guo, Y.; Zhang, D.; Yang, H.; Jiang, W.; Deng, F.; et al. The efficiency and safety of high-dose vitamin C in patients with COVID-19: A retrospective cohort study. Aging 2021, 13, 7020–7034. [Google Scholar] [CrossRef]
- Gavrielatou, E.; Xourgia, E.; Xixi, N.A.; Mantelou, A.G.; Ischaki, E.; Kanavou, A.; Zervakis, D.; Routsi, C.; Kotanidou, A.; Siempos, I.I. Effect of Vitamin C on Clinical Outcomes of Critically Ill Patients with COVID-19: An Observational Study and Subsequent Meta-Analysis. Front. Med. 2022, 9, 814587. [Google Scholar] [CrossRef]
- Hakamifard, A.; Soltani, R.; Maghsoudi, A.; Rismanbaf, A.; Aalinezhad, M.; Tarrahi, M.J.; Mashayekhbakhsh, S.; Dolatshahi, K. The effect of vitamin E and vitamin C in patients with COVID-19 pneumonia; a randomized controlled clinical trial. Immunopathol. Persa. 2022, 8, e08. [Google Scholar]
- Hess, A.L.; Halalau, A.; Dokter, J.J.; Paydawy, T.S.; Karabon, P.; Bastani, A.; Baker, R.E.; Balla, A.K.; Galens, S.A. High-dose intravenous vitamin C decreases rates of mechanical ventilation and cardiac arrest in severe COVID-19. Intern. Emerg. Med. 2022, 17, 1759–1768. [Google Scholar] [CrossRef]
- Kumari, P.; Dembra, S.; Dembra, P.; Bhawna, F.; Gul, A.; Ali, B.; Sohail, H.; Kumar, B.; Memon, M.H.; Rizwan, A. The Role of Vitamin C as Adjuvant Therapy in COVID-19. Cureus 2020, 12, e11779. [Google Scholar] [CrossRef]
- Li, M.; Ching, T.H.; Hipple, C.; Lopez, R.; Sahibzada, A.; Rahman, H. Use of Intravenous Vitamin C in Critically Ill Patients with COVID-19 Infection. J. Pharm. Pract. 2021, 20, 8971900211015052. [Google Scholar] [CrossRef]
- Majidi, N.; Rabbani, F.; Gholami, S.; Gholamalizadeh, M.; BourBour, F.; Rastgoo, S.; Hajipour, A.; Shadnoosh, M.; Akbari, M.E.; Bahar, B.; et al. The Effect of Vitamin C on Pathological Parameters and Survival Duration of Critically Ill Coronavirus Disease 2019 Patients: A Randomized Clinical Trial. Front. Immunol. 2021, 12, 717816. [Google Scholar] [CrossRef]
- Siahkali, J.M.S.; Zarezade, B.; Koolaji, S.; Seyed Alinaghi, S.; Zendehdel, A.; Tabarestani, M.; Sekhavati Moghadam, E.; Abbasian, L.; Dehghan Manshadi, S.A.; Salehi, M.; et al. Safety and effectiveness of high-dose vitamin C in patients with COVID-19: A randomized open-label clinical trial. Eur. J. Med. Res. 2021, 26, 20. [Google Scholar]
- Simsek, F.; Senkal, S.; Yazici, E.; Yonca, H.; Tahmaz, I.; Kara, U.; Sir, E.; Eksert, S.; Ince, M.E.; Ozdemirkan, I.; et al. Effects of high dose vitamin C administration in COVID-19 patients. Ann. Med. Res. 2021, 28, 1699–1703. [Google Scholar] [CrossRef]
- Suna, K.; Melahat, U.Ş.; Murat, Y.; Figen, Ö.E.; Ayperi, Ö. Effect of high-dose intravenous vitamin C on prognosis in patients with SARS-CoV-2 pneumonia. Med. Clin. 2022, 158, 356–360. [Google Scholar] [CrossRef]
- Tehrani, S.; Yadegarynia, D.; Abrishami, A.; Moradi, H.; Gharaei, B.; Rauofi, M.; Maghsoudi Nejad, F.; Sali, S.; Khabiri, N.; Abolghasemi, S. An investigation into the Effects of Intravenous Vitamin C on Pulmonary CT Findings and Clinical Outcomes of Patients with COVID 19 Pneumonia A Randomized Clinical Trial. Urol. J. 2021, 21, 6863. [Google Scholar]
- Thomas, S.; Patel, D.; Bittel, B.; Wolski, K.; Wang, Q.; Kumar, A.; Il’Giovine, Z.J.; Mehra, R.; McWilliams, C.; Nissen, S.E.; et al. Effect of High-Dose Zinc and Ascorbic Acid Supplementation vs Usual Care on Symptom Length and Reduction Among Ambulatory Patients with SARS-CoV-2 Infection: The COVID A to Z Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e210369. [Google Scholar] [CrossRef]
- Zhang, J.; Rao, X.; Li, Y.; Zhu, Y.; Liu, F.; Guo, G.; Luo, G.; Meng, Z.; De Backer, D.; Xiang, H.; et al. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann. Intensive Care 2021, 11, 5. [Google Scholar] [CrossRef]
- Zhao, B.; Liu, M.; Liu, P.; Peng, Y.; Huang, J.; Li, M.; Wang, Y.; Xu, L.; Sun, S.; Qi, X.; et al. High Dose Intravenous Vitamin C for Preventing The Disease Aggravation of Moderate COVID-19 Pneumonia. A Retrospective Propensity Matched Before-After Study. Front. Pharmacol. 2021, 12, 638556. [Google Scholar] [CrossRef]
- Zheng, S.; Chen, Q.; Jiang, H.; Guo, C.; Luo, J.; Li, S.; Wang, H.; Li, H.; Zheng, X.; Weng, Z. No significant benefit of moderate-dose vitamin C on severe COVID-19 cases. Open Med. 2021, 16, 1403–1414. [Google Scholar] [CrossRef]
- Lamontagne, F.; Masse, M.H.; Menard, J.; Sprague, S.; Pinto, R.; Heyland, D.K.; Cook, D.J.; Battista, M.C.; Day, A.G.; Guyatt, G.H.; et al. Intravenous Vitamin C in Adults with Sepsis in the Intensive Care Unit. N. Engl. J. Med. 2022, 386, 2387–2398. [Google Scholar] [CrossRef] [PubMed]
- Pedrosa, L.F.C.; Barros, A.N.A.B.; Leite-Lais, L. Nutritional risk of vitamin D, vitamin C, zinc, and selenium deficiency on risk and clinical outcomes of COVID-19: A narrative review. Clin. Nutr. ESPEN 2022, 47, 9–27. [Google Scholar] [CrossRef] [PubMed]
- Shahbaz, U.; Fatima, N.; Basharat, S.; Bibi, A.; Yu, X.; Hussain, M.I.; Nasrullah, M. Role of vitamin C in preventing of COVID-19 infection, progression and severity. AIMS Microbiol. 2022, 8, 108–124. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.; Gennari-Felipe, M.; Dias, B.B.; Hatanaka, E. Melatonin, Zinc, and Vitamin C: Potential Adjuvant Treatment for COVID-19 Patients. Front. Nutr. 2022, 8, 821824. [Google Scholar] [CrossRef]
- Vollbracht, C.; Kraft, K. Oxidative Stress and Hyper-Inflammation as Major Drivers of Severe COVID-19 and Long COVID: Implications for the Benefit of High-Dose Intravenous Vitamin C. Front. Pharmacol. 2022, 13, 899198. [Google Scholar] [CrossRef]
- Gröber, U.; Holick, M.F. The coronavirus disease (COVID-19)—A supportive approach with selected micronutrients. Int. J. Vitam. Nutr. Res. 2022, 92, 13–34. [Google Scholar] [CrossRef]
- Ao, G.; Li, J.; Yuan, Y.; Wang, Y.; Nasr, B.; Bao, M.; Gao, M.; Qi, X. Intravenous vitamin C use and risk of severity and mortality in COVID-19: A systematic review and meta-analysis. Nutr. Clin. Pract. 2022, 37, 274–281. [Google Scholar] [CrossRef]
- Migliorini, F.; Vaishya, R.; Eschweiler, J.; Oliva, F.; Hildebrand, F.; Maffulli, N. Vitamins C and D and COVID-19 Susceptibility, Severity and Progression: An Evidence Based Systematic Review. Medicina 2022, 58, 941. [Google Scholar] [CrossRef]
- Rawat, D.; Roy, A.; Maitra, S.; Gulati, A.; Khanna, P.; Baidya, D.K. Vitamin C and COVID-19 treatment: A systematic review and meta-analysis of randomized controlled trials. Diabetes Metab. Syndr. 2021, 15, 102324. [Google Scholar] [CrossRef]
- Hemilä, H.; de Man, A.M.E. Vitamin C and COVID-19. Front. Med. 2021, 7, 559811. [Google Scholar] [CrossRef]
- Bhowmik, K.K.; Barek, M.A.; Aziz, M.A.; Islam, M.S. Impact of high-dose vitamin C on the mortality, severity, and duration of hospital stay in COVID-19 patients: A meta-analysis. Health Sci. Rep. 2022, 5, e762. [Google Scholar] [CrossRef]
- Corrao, S.; Mallaci Bocchio, R.; Lo Monaco, M.; Natoli, G.; Cavezzi, A.; Troiani, E.; Argano, C. Does Evidence Exist to Blunt Inflammatory Response by Nutraceutical Supplementation during COVID-19 Pandemic? An Overview of Systematic Reviews of Vitamin D, Vitamin C, Melatonin, and Zinc. Nutrients 2021, 13, 1261. [Google Scholar] [CrossRef]
- Rs, N.; Reddy, M.V.N.J.; Batra, S.; Srivastava, S.K.; Syal, K. Vitamin C and its therapeutic potential in the management of COVID19. Clin. Nutr. ESPEN 2022, 50, 8–14. [Google Scholar] [CrossRef]
- Firouzi, S.; Pahlavani, N.; Navashenaq, J.G.; Clayton, Z.S.; Beigmohammadi, M.T.; Malekahmadi, M. The effect of Vitamin C and Zn supplementation on the immune system and clinical outcomes in COVID-19 patients. Clin. Nutr. Open Sci. 2022, 44, 144–154. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Design | Rout of Vitamin C Administration | Group with Vitamin C supplementation | Group without Vitamin C Supplementation | ||||
|---|---|---|---|---|---|---|---|---|---|
| No. of Patients | Age | Sex, Male | No. of Patients | Age | Sex, Male | ||||
| Al Sulaiman et al., 2021 [32] | Saudi Arabia | Retrospective study | P.O. | 158 | 60.5 ± 15.09 | 124 (79.0) | 581 | 60.7 ± 14.75 | 407 (70.1) |
| Beigmohammadi et al., 2021 [33] | Iran | RCT | P.O. | 30 | 51.00 ± 17.25 | 15 (50.0%) | 30 | 53.0 ± 7.00 | 16 (53.3%) |
| Coppock et al., 2022 [34] | USA | RCT | I.V. | 44 | 60 ± 17 | 22 (50.0%) | 22 | 61 ± 11 | 11 (50.0%) |
| Darban et al., 2021 [35] | Iran | RCT | I.V. | 10 | NS | NS | 10 | NS | NS |
| Gao et al., 2021 [36] | China | Retrospective study | I.V. | 46 | 62.75 ± 4.25 | 21 (45.7%) | 30 | 57.5 ± 4.5 | 14 (46.7%) |
| Gavrielatou et al., 2022 [37] | Greece | Retrospective study | I.V. | 10 | 68.5 ± 4.9 | 7 | 103 | 67.5 ± 3.7 | 78 |
| Hakamifard et al., 2022 [38] | Iran | RCT | P.O. | 38 | 35.68 | 24 (63.2%) | 34 | 37.41 | 22 (64.7%) |
| Hess et al., 2022 [39] | USA | Retrospective study | I.V. | 25 | 58.3 ± 14.2 | 13 (52.0%) | 75 | 71.2 ± 13.0 | 42 (56.0%) |
| Kumari et al., 2020 [40] | Pakistan | RCT | I.V. | 75 | 52 ± 11 | NS | 75 | 53 ± 12 | NS |
| Li et al., 2021 [41] | USA | Retrospective study | I.V. | 8 | 64.1 + 8.3 | 3 | 24 | 64.9 + 11.8 | 9 |
| Majidi et al., 2021 [42] | Iran | RCT | P.O. | 31 | 59.42 ± 15.07 | 19 | 69 | 63.82 ± 14.58 | 41 |
| Siahkali et al., 2021 [43] | Iran | RCT | I.V. | 30 | 57.53 ± 18.27 | 15 | 30 | 61 ± 15.9 | 15 |
| Simsek et al., 2021 [44] | Turkey | Retrospective study | I.V. | 58 | 56.53 ± 18.77 | 27 | 81 | 62.20 ± 15.72 | 52 |
| Suna et al., 2022 [45] | Turkey | Retrospective study | I.V. | 153 | 60.16 ± 13.65 | 102 | 170 | 64.27 ± 14.49 | 102 |
| Tehrani et al., 2021 [46] | Iran | RCT | I.V. | 18 | 58 ± 19 | 8 | 26 | 61 ± 17 | 18 |
| Thomas et al., 2021 [47] | USA | RCT | P.O. | 48 | 45.6 ± 15.0 | 15 | 50 | 42.0 ± 14.6 | 19 |
| Zhang et al., 2021 [48] | China | RCT | I.V. | 27 | 66.3 ± 11.2 | 15 (55.6%) | 29 | 67.0 ± 14.3 | 22 (75.9%) |
| Zhao et al., 2021 [49] | China | Retrospective study | I.V. | 55 | 37.5 ± 4.0 | 33 | 55 | 37.25 ± 3.75 | 35 |
| Zheng et al., 2021 [50] | China | Retrospective study | I.V. | 73 | 67.5 ± 2.0 | 38 (51.1%) | 323 | 67.5 ± 2.0 | 207 |
| Adverse Event Type | No of Studies | Events/Participants | Events | Heterogeneity between Trials | p-Value for Differences across Groups | |||
|---|---|---|---|---|---|---|---|---|
| Vitamin C Supplementation | Standard Treatment | OR | 95%CI | p-Value | I2 Statistic | |||
| Acute kidney injury | 3 | 67/241 (27.8%) | 306/680 (45.0%) | 0.56 | 0.40 to 0.78 | 0.34 | 7% | <0.001 |
| Liver injury | 2 | 26/183 (14.2%) | 76/597 (12.7%) | 0.83 | 0.49 to 1.41 | 0.72 | 0% | 0.49 |
| Respiratory failure required MV | 3 | 50/185 (27.0%) | 62/260 (23.8%) | 1.22 | 0.78 to 1.89 | 0.29 | 18% | 0.38 |
| Coagulation disorders | 2 | 18/181 (9.9%) | 71/594 (12.0%) | 0.80 | 0.25 to 2.49 | 0.09 | 65% | 0.15 |
| Acute cardiac injury | 1 | 7/27 (25.9%) | 13/29 (44.8%) | 0.43 | 0.14 to 1.33 | NA | NA | 0.14 |
| Vitamin C Daily Dose | No of Studies | Events/Participants | Events | Heterogeneity between Trials | p-Value for Differences across Groups | |||
|---|---|---|---|---|---|---|---|---|
| Vitamin C Supplementation | Standard Treatment | OR | 95%CI | p-Value | I2 Statistic | |||
| ≤1 g/day | 4 | 108/234 (46.2%) | 411/752 (54.7%) | 0.45 | 0.32 to 0.64 | 0.28 | 22% | <0.001 |
| >1 g/day ≤10 g/day | 9 | 38/418 (9.1%) | 72/445 (16.2%) | 0.62 | 0.40 to 0.96 | 0.48 | 0.48 | 0.03 |
| >10 g/day | 4 | 34/180 (18.9%) | 70/512 (13.7%) | 1.13 | 0.27 to 4.73 | <0.001 | 88% | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olczak-Pruc, M.; Swieczkowski, D.; Ladny, J.R.; Pruc, M.; Juarez-Vela, R.; Rafique, Z.; Peacock, F.W.; Szarpak, L. Vitamin C Supplementation for the Treatment of COVID-19: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4217. https://doi.org/10.3390/nu14194217
Olczak-Pruc M, Swieczkowski D, Ladny JR, Pruc M, Juarez-Vela R, Rafique Z, Peacock FW, Szarpak L. Vitamin C Supplementation for the Treatment of COVID-19: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(19):4217. https://doi.org/10.3390/nu14194217
Chicago/Turabian StyleOlczak-Pruc, Monika, Damian Swieczkowski, Jerzy R. Ladny, Michal Pruc, Raul Juarez-Vela, Zubaid Rafique, Frank W. Peacock, and Lukasz Szarpak. 2022. "Vitamin C Supplementation for the Treatment of COVID-19: A Systematic Review and Meta-Analysis" Nutrients 14, no. 19: 4217. https://doi.org/10.3390/nu14194217
APA StyleOlczak-Pruc, M., Swieczkowski, D., Ladny, J. R., Pruc, M., Juarez-Vela, R., Rafique, Z., Peacock, F. W., & Szarpak, L. (2022). Vitamin C Supplementation for the Treatment of COVID-19: A Systematic Review and Meta-Analysis. Nutrients, 14(19), 4217. https://doi.org/10.3390/nu14194217