
Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study

 ,
,  , , ,
, , ,  ,
,  , , ,
, , ,  , , , , , , , ,
, , , , , , , ,  , ,
, ,  , , , , ,
, , , , ,  , ,
, , 
 and
and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment
- I.
- Circumstances of the lockdown (eight items).
- II.
- Effects of the lockdown on eating symptoms (thirteen items): it evaluates symptomatology of AN, BN, BED and OSFED, according with the DSM-5. Comorbidity with other psychiatric disorders or diabetes is assessed.
- III.
- Reaction to the lockdown (34 items): it evaluates the effects of the confinement on eating behaviors, attitudes and habits, anxious-depressive symptoms, emotion dysregulation, and other symptomatology associated with substance use disorders and behavioral addictions.
- IV.
- The evaluation of remote interventions (thirteen items) assesses acceptance, general satisfaction, and motivation for virtual interventions.
2.3. Additional Assessment
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
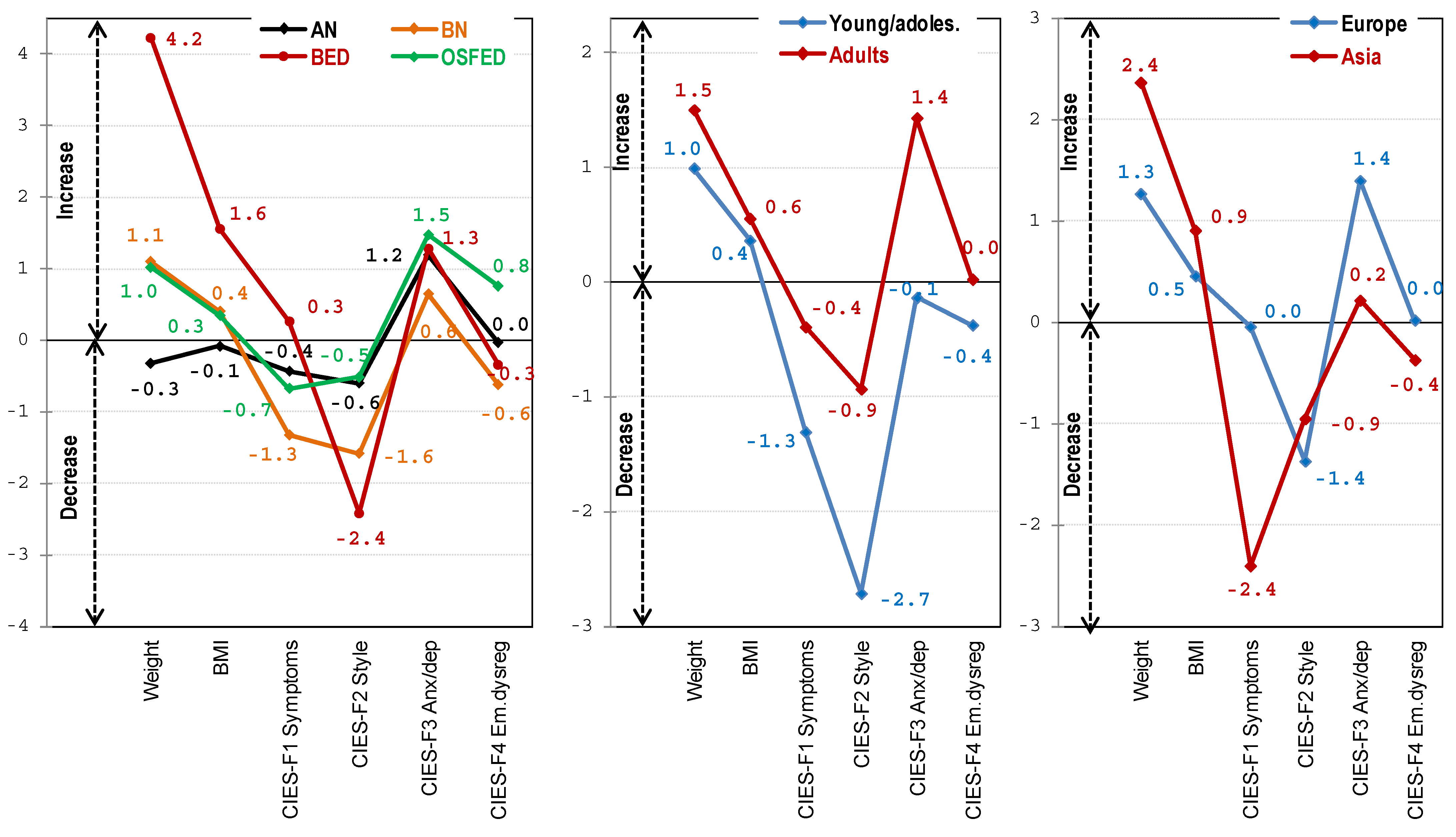
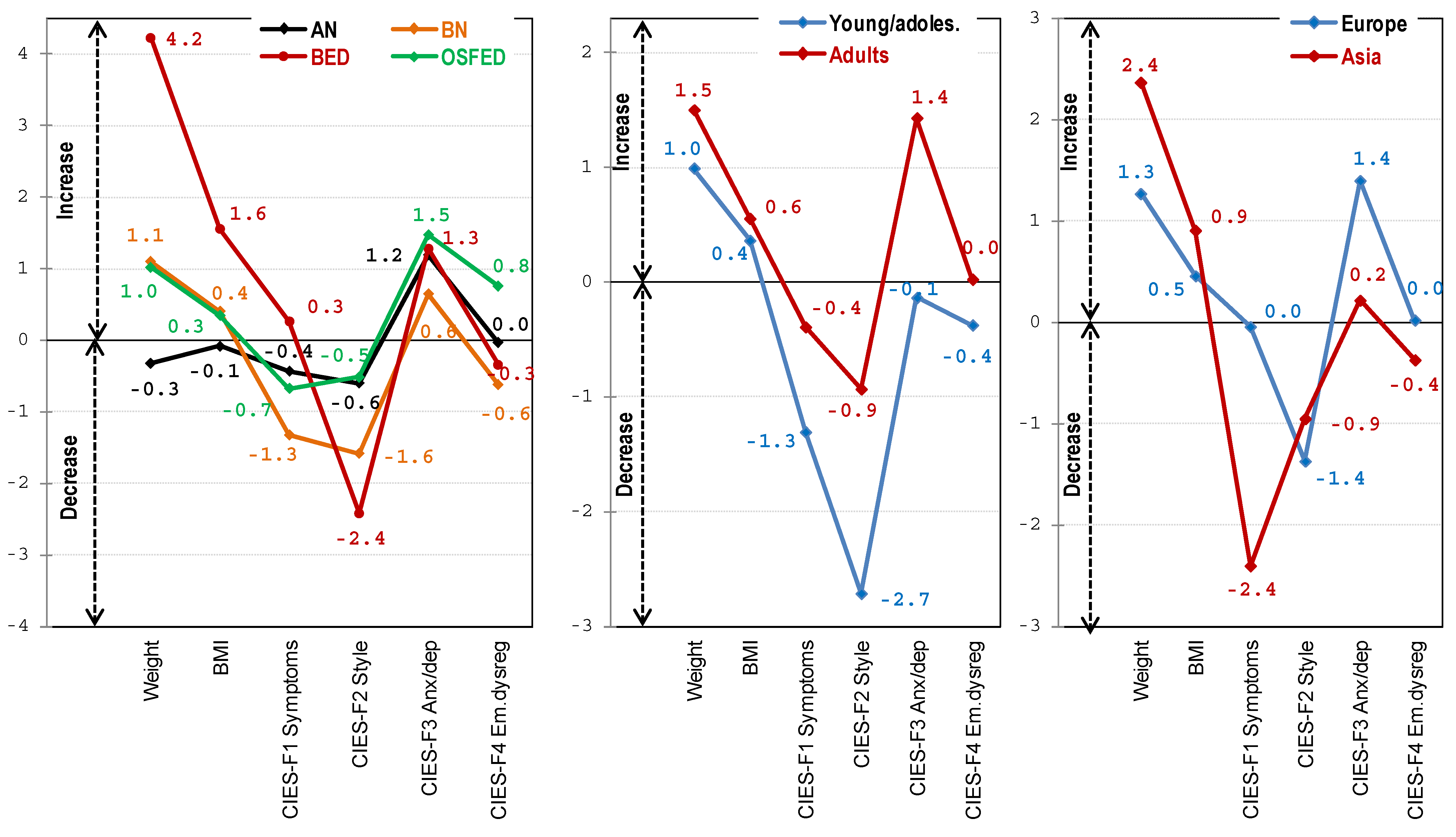
3.2. Comparison between Diagnostic Subtypes of Changes Pre to Post Lockdown
3.3. Comparison between the Groups of Age for the Changes during the Lockdown
3.4. Comparison between Continents for the Changes during the Lockdown
4. Discussion
4.1. ED Subtypes and Changes during Lockdown
4.2. Age Differences Regarding Changes during Lockdown
4.3. Influence of Continental Provenance on the Changes during Lockdown
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodgers, R.F.; Lombardo, C.; Cerolini, S.; Franko, D.L.; Omori, M.; Fuller-Tyszkiewicz, M.; Linardon, J.; Courtet, P.; Guillaume, S. The impact of the COVID-19 pandemic on eating disorder risk and symptoms. Int. J. Eat. Disord. 2020, 53, 1166–1170. [Google Scholar] [CrossRef] [PubMed]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreaks in the general population: Practical considerations for the COVID-19 pandemic. Singap. Med. J. 2020, 61, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- De Girolamo, G.; Cerveri, G.; Clerici, M.; Monzani, E.; Spinogatti, F.; Starace, F.; Tura, G.; Vita, A. Mental Health in the Coronavirus Disease 2019 Emergency—The Italian Response. JAMA Psychiatry 2020, 77, 974–976. [Google Scholar] [CrossRef] [PubMed]
- Ozamiz-Etxebarria, N.; Dosil-Santamaria, M.; Picaza-Gorrochategui, M.; Idoiaga-Mondragon, N. Stress, Anxiety, and Depression Levels in the Initial Stage of the COVID-19 Outbreak in a Population Sample in the Northern Spain. Cad. Saúde Pública 2020, 36, e00054020. [Google Scholar] [CrossRef]
- Todisco, P.; Donini, L. Eating disorders and obesity (ED&O) in the COVID-19 storm. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 747–750. [Google Scholar] [CrossRef]
- Branley-Bell, D.; Talbot, C.V. Exploring the impact of the COVID-19 pandemic and UK lockdown on individuals with experience of eating disorders. J. Eat. Disord. 2020, 8, 44. [Google Scholar] [CrossRef]
- Nisticò, V.; Bertelli, S.; Tedesco, R.; Anselmetti, S.; Priori, A.; Gambini, O.; Demartini, B. The psychological impact of COVID-19-related lockdown measures among a sample of Italian patients with eating disorders: A preliminary longitudinal study. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 2771–2777. [Google Scholar] [CrossRef]
- Castellini, G.; Cassioli, E.; Rossi, E.; Innocenti, M.; Gironi, V.; Sanfilippo, G.; Felciai, F.; Monteleone, A.M.; Ricca, V. The impact of COVID-19 epidemic on eating disorders: A longitudinal observation of pre versus post psychopathological features in a sample of patients with eating disorders and a group of healthy controls. Int. J. Eat. Disord. 2020, 53, 1855–1862. [Google Scholar] [CrossRef]
- Msc, J.D.T.; Watson, H.J.; Thornton, L.M.; Borg, S.; Ma, R.E.F.; Ba, C.M.M.; Bs, L.E.H.; van Furth, E.; Peat, C.M.; Bulik, C.M. Early impact of COVID-19 on individuals with self-reported eating disorders: A survey of ~1000 individuals in the United States and the Netherlands. Int. J. Eat. Disord. 2020, 53, 1780–1790. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Casas, M.; Claes, L.; Bryan, D.C.; Favaro, A.; Granero, R.; Gudiol, C.; Jiménez-Murcia, S.; Karwautz, A.; Le Grange, D.; et al. COVID-19 and implications for eating disorders. Eur. Eat. Disord. Rev. 2020, 28, 239–245. [Google Scholar] [CrossRef]
- Håkansson, A.; Fernández-Aranda, F.; Menchón, J.M.; Potenza, M.N.; Jiménez-Murcia, S. Gambling During the COVID-19 Crisis – A Cause for Concern. J. Addict. Med. 2020, 14, e10–e12. [Google Scholar] [CrossRef]
- King, D.L.; Delfabbro, P.H.; Billieux, J.; Potenza, M.N. Problematic online gaming and the COVID-19 pandemic. J. Behav. Addict. 2020, 9, 184–186. [Google Scholar] [CrossRef]
- Phillipou, A.; Meyer, D.; Neill, E.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Rossell, S.L. Eating and exercise behaviors in eating disorders and the general population during the COVID -19 pandemic in Australia: Initial results from the COLLATE project. Int. J. Eat. Disord. 2020, 53, 1158–1165. [Google Scholar] [CrossRef]
- Christensen, K.A.; Forbush, K.T.; Richson, B.N.; Thomeczek, M.L.; Perko, V.L.; Bjorlie, K.; Christian, K.; Ayres, J.; Wildes, J.E.; Chana, S.M. Food insecurity associated with elevated eating disorder symptoms, impairment, and eating disorder diagnoses in an American University student sample before and during the beginning of the COVID-19 pandemic. Int. J. Eat. Disord. 2021, 54, 1213–1223. [Google Scholar] [CrossRef]
- Touyz, S.; Lacey, H.; Hay, P. Eating disorders in the time of COVID-19. J. Eat. Disord. 2020, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Weissman, R.S.; Bauer, S.; Thomas, J.J. Access to evidence-based care for eating disorders during the COVID-19 crisis. Int. J. Eat. Disord. 2020, 53, 639–646. [Google Scholar] [CrossRef]
- Baenas, I.; Caravaca-Sanz, E.; Granero, R.; Sánchez, I.; Riesco, N.; Testa, G.; Vintró-Alcaraz, C.; Treasure, J.; Jiménez-Murcia, S.; Fernández-Aranda, F. COVID -19 and eating disorders during confinement: Analysis of factors associated with resilience and aggravation of symptoms. Eur. Eat. Disord. Rev. 2020, 28, 855–863. [Google Scholar] [CrossRef]
- Machado, P.P.P.; Pinto-Bastos, A.; Ramos, R.; Rodrigues, T.F.; Louro, E.; Gonçalves, S.; Brandão, I.; Vaz, A. Impact of COVID-19 lockdown measures on a cohort of eating disorders patients. J. Eat. Disord. 2020, 8, 57. [Google Scholar] [CrossRef] [PubMed]
- Vuillier, L.; May, L.; Greville-Harris, M.; Surman, R.; Moseley, R.L. The impact of the COVID-19 pandemic on individuals with eating disorders: The role of emotion regulation and exploration of online treatment experiences. J. Eat. Disord. 2021, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, A.M.; Cascino, G.; Marciello, F.; Abbate-Daga, G.; Baiano, M.; Balestrieri, M.; Barone, E.; Bertelli, S.; Carpiniello, B.; Castellini, G.; et al. Risk and resilience factors for specific and general psychopathology worsening in people with Eating Disorders during COVID-19 pandemic: A retrospective Italian multicentre study. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 2443–2452. [Google Scholar] [CrossRef]
- Schlegl, S.; Maier, J.; Meule, A.; Voderholzer, U. Eating disorders in times of the COVID-19 pandemic—Results from an online survey of patients with anorexia nervosa. Int. J. Eat. Disord. 2020, 53, 1791–1800. [Google Scholar] [CrossRef] [PubMed]
- Schlegl, S.; Meule, A.; Favreau, M.; Voderholzer, U. Bulimia nervosa in times of the COVID -19 pandemic—Results from an online survey of former inpatients. Eur. Eat. Disord. Rev. 2020, 28, 847–854. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Munguía, L.; Mestre-Bach, G.; Steward, T.; Etxandi, M.; Baenas, I.; Granero, R.; Sánchez, I.; Ortega, E.; Andreu, A.; et al. COVID Isolation Eating Scale (CIES): Analysis of the impact of confinement in eating disorders and obesity—A collaborative international study. Eur Eat Disord Rev. 2020, 28, 871–883. [Google Scholar] [CrossRef] [PubMed]
- Hamamura, T.; Heine, S.J.; Paulhus, D.L. Cultural differences in response styles: The role of dialectical thinking. Pers. Individ. Differ. 2008, 44, 932–942. [Google Scholar] [CrossRef]
- English, T.; Chen, S. Culture and self-concept stability: Consistency across and within contexts among Asian Americans and European Americans. J. Pers. Soc. Psychol. 2007, 93, 478–490. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV); American Psychiatric Association: Arlington, TX, USA, 2015. [Google Scholar]
- Stata-Corp Stata Statistical Software: Release 17; Statacorp: College Station, TX, USA, 2021.
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Kelley, K.; Preacher, K.J. On effect size. Psychol. Methods 2012, 17, 137–152. [Google Scholar] [CrossRef]
- Finner, H.; Roters, M. On the false discovery rate and expecte type I errors. J. Am. Stat. Assoc. 2001, 88, 920–923. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Sánchez, E.; Lecube, A.; Bellido, D.; Monereo, S.; Malagón, M.M.; Tinahones, J.F. Leading Factors for Weight Gain during COVID-19 Lockdown in a Spanish Population: A Cross-Sectional Study. Nutrients 2021, 13, 894. [Google Scholar] [CrossRef]
- Bhutani, S.; Cooper, J.A. COVID-19–Related Home Confinement in Adults: Weight Gain Risks and Opportunities. Obesity 2020, 28, 1576–1577. [Google Scholar] [CrossRef]
- Stevenson, J.L.; Krishnan, S.; A Stoner, M.; Goktas, Z.; A Cooper, J. Effects of exercise during the holiday season on changes in body weight, body composition and blood pressure. Eur. J. Clin. Nutr. 2013, 67, 944–949. [Google Scholar] [CrossRef] [Green Version]
- Agüera, Z.; Lozano-Madrid, M.; Mallorquí-Bagué, N.; Jiménez-Murcia, S.; Menchón, J.M.; Fernández-Aranda, F. A review of binge eating disorder and obesity. Neuropsychiatrie 2021, 35, 57–67. [Google Scholar] [CrossRef]
- Villarejo, C.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Peñas-Lledó, E.; Granero, R.; Penelo, E.; Tinahones, F.J.; Sancho, C.; Vilarrasa, N.; Montserrat-Gil de Bernabé, M.; et al. Lifetime Obesity in Patients with Eating Disorders: Increasing Prevalence, Clinical and Personality Correlates. Eur. Eat. Disord. Rev. 2012, 20, 250–254. [Google Scholar] [CrossRef] [Green Version]
- Monteleone, A.M.; Marciello, F.; Cascino, G.; Abbate-Daga, G.; Anselmetti, S.; Baiano, M.; Balestrieri, M.; Barone, E.; Bertelli, S.; Carpiniello, B.; et al. The impact of COVID-19 lockdown and of the following “re-opening” period on specific and general psychopathology in people with Eating Disorders: The emergent role of internalizing symptoms. J. Affect. Disord. 2021, 285, 77–83. [Google Scholar] [CrossRef]
- Agüera, Z.; Riesco, N.; Valenciano-Mendoza, E.; Granero, R.; Sánchez, I.; Andreu, A.; Jiménez-Murcia, S.; Fernández-Aranda, F. Illness perception in patients with eating disorders: Clinical, personality, and food addiction correlates. Eat. Weight. Disord.—Stud. Anorex. Bulim. Obes. 2021, 26, 2287–2300. [Google Scholar] [CrossRef]
- Bryan, D.C.; Macdonald, P.; Ambwani, S.; Cardi, V.; Rowlands, K.; Willmott, D.; Treasure, J. Exploring the ways in which COVID-19 and lockdown has affected the lives of adult patients with anorexia nervosa and their carers. Eur. Eat. Disord. Rev. 2020, 28, 826–835. [Google Scholar] [CrossRef]
- Claes, L.; Boekaerts, E.; Verschueren, M.; Boukaert, W.; Luyckx, K. Identity statuses in prebariatric patients with obesity: Associations with eating disorder symptoms, psychological complaints, and coping behaviour? Eur. Eat. Disord. Rev. 2019, 27, 410–420. [Google Scholar] [CrossRef]
- Riesco, N.; Agüera, Z.; Granero, R.; Jiménez-Murcia, S.; Menchón, J.M.; Fernández-Aranda, F. Other Specified Feeding or Eating Disorders (OSFED): Clinical heterogeneity and cognitive-behavioral therapy outcome. Eur. Psychiatry 2018, 54, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, M.; Xian, Y.; Lv, X.; He, J.; Ren, Y. Changes in Body Weight, Physical Activity, and Lifestyle During the Semi-lockdown Period After the Outbreak of COVID-19 in China: An Online Survey. Disaster Med. Public Heal. Prep. 2021, 15, e23–e28. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Pre | Post | |||||
|---|---|---|---|---|---|---|
| Anorexia (n = 370) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 48.29 | 9.02 | 48.27 | 8.23 | 0.954 | 0.00 |
| BMI (kg/m2) | 17.92 | 3.06 | 17.94 | 3.00 | 0.862 | 0.01 |
| CIES-F1 ED symptoms | 13.94 | 6.93 | 13.32 | 7.46 | 0.089 | 0.09 |
| CIES-F2 Eating style | 10.96 | 8.75 | 9.98 | 8.71 | 0.005 * | 0.11 |
| CIES-F3 Anxiety-depression | 17.20 | 9.62 | 17.93 | 9.85 | 0.089 | 0.07 |
| CIES-F4 Emotion dysregulation | 8.51 | 5.09 | 8.27 | 5.26 | 0.247 | 0.05 |
| n | % | n | % | p | |h| | |
| Tobacco | 52 | 14.1% | 52 | 14.1% | 1.00 | 0.00 |
| Alcohol | 57 | 15.4% | 38 | 10.3% | 0.001 * | 0.15 |
| Other illegal drugs | 33 | 8.9% | 26 | 7.0% | 0.143 | 0.07 |
| Behavioral addictions | 244 | 65.9% | 242 | 65.4% | 0.875 | 0.01 |
| Bulimia (n = 148) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 61.09 | 14.52 | 62.26 | 13.89 | 0.026 * | 0.08 |
| BMI (kg/m2) | 22.27 | 5.07 | 22.70 | 4.84 | 0.025 * | 0.09 |
| CIES-F1 ED symptoms | 19.78 | 6.82 | 18.39 | 7.16 | 0.048 * | 0.20 |
| CIES-F2 Eating style | 21.96 | 10.15 | 20.28 | 10.79 | 0.073 | 0.16 |
| CIES-F3 Anxiety-depression | 20.36 | 9.02 | 20.84 | 9.61 | 0.467 | 0.05 |
| CIES-F4 Emotion dysregulation | 9.91 | 4.83 | 9.22 | 5.28 | 0.045 * | 0.14 |
| n | % | n | % | p | |h| | |
| Tobacco | 42 | 28.4% | 46 | 31.1% | 0.388 | 0.06 |
| Alcohol | 62 | 41.9% | 45 | 30.4% | <0.001 * | 0.24 |
| Other illegal drugs | 30 | 20.3% | 22 | 14.9% | 0.115 | 0.14 |
| Behavioral addictions | 108 | 73.0% | 106 | 71.6% | 0.839 | 0.03 |
| BED (n = 113) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 95.27 | 33.79 | 99.18 | 31.49 | <0.001 * | 0.12 |
| BMI (kg/m2) | 33.63 | 10.38 | 35.08 | 9.63 | <0.001 * | 0.14 |
| CIES-F1 ED symptoms | 14.10 | 7.26 | 14.57 | 6.72 | 0.449 | 0.07 |
| CIES-F2 Eating style | 20.88 | 11.30 | 18.86 | 11.60 | 0.010 * | 0.18 |
| CIES-F3 Anxiety-depression | 17.66 | 10.37 | 19.45 | 11.37 | 0.004 * | 0.16 |
| CIES-F4 Emotion dysregulation | 8.99 | 5.91 | 8.88 | 5.87 | 0.745 | 0.02 |
| n | % | n | % | p | |d| | |
| Tobacco | 29 | 25.7% | 28 | 24.8% | 1.00 | 0.02 |
| Alcohol | 36 | 31.9% | 31 | 27.4% | 0.405 | 0.10 |
| Other illegal drugs | 18 | 15.9% | 13 | 11.5% | 0.332 | 0.13 |
| Behavioral addictions | 73 | 64.6% | 79 | 69.9% | 0.263 | 0.11 |
| OSFED (n = 198) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 81.68 | 25.86 | 82.25 | 26.29 | 0.280 | 0.02 |
| BMI (kg/m2) | 28.58 | 8.06 | 28.77 | 8.13 | 0.340 | 0.02 |
| CIES-F1 ED symptoms | 13.74 | 5.95 | 13.35 | 5.70 | 0.266 | 0.07 |
| CIES-F2 Eating style | 13.94 | 9.14 | 13.99 | 9.12 | 0.924 | 0.00 |
| CIES-F3 Anxiety-depression | 13.99 | 10.03 | 16.17 | 10.90 | <0.001 * | 0.21 |
| CIES-F4 Emotion dysregulation | 6.73 | 5.08 | 7.80 | 5.86 | <0.001 * | 0.20 |
| n | % | n | % | p | |h| | |
| Tobacco | 58 | 29.3% | 65 | 32.8% | 0.092 | 0.08 |
| Alcohol | 57 | 28.8% | 51 | 25.8% | 0.286 | 0.07 |
| Other illegal drugs | 13 | 6.6% | 16 | 8.1% | 0.629 | 0.06 |
| Behavioral addictions | 123 | 62.1% | 131 | 66.2% | 0.152 | 0.08 |
| Anorexia (AN) | Bulimia (BN) | BED | OSFED | Significant | |||||
|---|---|---|---|---|---|---|---|---|---|
| n = 370 | n = 148 | n = 113 | n = 198 | Pairwise | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Comparisons | |
| Weight (kg) | −0.32 | 6.66 | 1.10 | 6.32 | 4.22 | 11.58 | 1.02 | 7.43 | BED ≠ (AN = BN = OSFED) |
| BMI (kg/m2) | −0.09 | 2.54 | 0.40 | 2.31 | 1.55 | 4.13 | 0.35 | 2.71 | BED ≠ (AN = BN = OSFED) |
| CIES-F1 ED symptoms | −0.43 | 7.03 | −1.32 | 8.52 | 0.26 | 6.54 | −0.67 | 4.90 | BED ≠ (AN = BN = OSFED) |
| CIES-F2 Eating style | −0.60 | 6.72 | −1.58 | 11.34 | −2.42 | 8.12 | −0.52 | 6.69 | (BED = BN) ≠ (AN = OSFED) |
| CIES-F3 Anxiety-dep. | 1.19 | 8.28 | 0.65 | 8.28 | 1.28 | 6.53 | 1.47 | 7.04 | OSFED ≠ (AN = BN = BED) |
| CIES-F4 Emot.dysreg. | −0.03 | 4.06 | −0.62 | 4.25 | −0.34 | 3.73 | 0.75 | 3.94 | OSFED ≠ (AN = BN = BED) |
| Pre | Post | |||||
|---|---|---|---|---|---|---|
| Age: young/adolescents (n = 172) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 63.49 | 13.52 | 65.44 | 13.51 | 0.073 | 0.14 |
| BMI (kg/m2) | 22.74 | 4.00 | 23.37 | 3.97 | 0.119 | 0.16 |
| CIES-F1 ED symptoms | 14.83 | 6.73 | 13.32 | 7.52 | 0.213 | 0.21 |
| CIES-F2 Eating style | 16.54 | 9.23 | 12.75 | 8.60 | 0.003 * | 0.43 |
| CIES-F3 Anxiety-depression symptoms | 15.96 | 8.89 | 15.46 | 8.83 | 0.701 | 0.06 |
| CIES-F4 Emotion dysregulation | 8.84 | 5.24 | 8.39 | 5.33 | 0.537 | 0.09 |
| n | % | n | % | p | |h| | |
| Tobacco | 14 | 9.6% | 16 | 11.1% | 0.566 | 0.05 |
| Alcohol | 18 | 9.7% | 9 | 3.1% | 0.118 | 0.28 |
| Other illegal drugs | 9 | 6.0% | 8 | 5.8% | 0.945 | 0.01 |
| Behavioral addictions | 125 | 79.7% | 127 | 80.1% | 0.948 | 0.01 |
| Age: adults (n = 657) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 72.18 | 27.82 | 73.62 | 27.96 | <0.001 * | 0.05 |
| BMI (kg/m2) | 25.79 | 9.00 | 26.32 | 9.10 | <0.001 * | 0.06 |
| CIES-F1 ED symptoms | 15.54 | 7.14 | 15.22 | 6.96 | 0.237 | 0.04 |
| CIES-F2 Eating style | 17.17 | 10.60 | 16.32 | 10.52 | 0.008 * | 0.08 |
| CIES-F3 Anxiety-depression symptoms | 17.69 | 10.13 | 19.26 | 10.57 | <0.001 * | 0.15 |
| CIES-F4 Emotion dysregulation | 8.61 | 5.27 | 8.70 | 5.53 | 0.546 | 0.02 |
| n | % | n | % | p | |h| | |
| Tobacco | 167 | 26.2% | 175 | 27.4% | 0.235 | 0.03 |
| Alcohol | 194 | 31.4% | 156 | 25.4% | <0.001 * | 0.13 |
| Other illegal drugs | 85 | 13.9% | 69 | 11.0% | 0.025 * | 0.09 |
| Behavioral addictions | 423 | 65.0% | 431 | 66.6% | 0.272 | 0.03 |
| Young/Adolescents | Adults | |||||
|---|---|---|---|---|---|---|
| n = 172 | n = 657 | |||||
| Mean | SD | Mean | SD | p | |d| | |
| Weight (kg) | 0.99 | 7.16 | 1.50 | 7.86 | 0.480 | 0.07 |
| BMI (kg/m2) | 0.36 | 2.66 | 0.56 | 2.89 | 0.471 | 0.04 |
| CIES-F1 ED symptoms | −1.30 | 7.94 | −0.39 | 6.50 | 0.154 | 0.13 |
| CIES-F2 Eating style | −2.71 | 8.17 | −0.93 | 7.85 | 0.017 * | 0.22 |
| CIES-F3 Anxiety-depression symptoms | −0.13 | 8.55 | 1.43 | 7.52 | 0.030 * | 0.19 |
| CIES-F4 Emotion dysregulation | −0.37 | 4.77 | 0.03 | 3.84 | 0.289 | 0.09 |
| Pre | Post | |||||
|---|---|---|---|---|---|---|
| Europe (n = 676) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 72.99 | 27.78 | 74.20 | 28.24 | 0.001 * | 0.04 |
| BMI (kg/m2) | 26.06 | 8.95 | 26.49 | 9.14 | 0.001 * | 0.05 |
| CIES-F1 ED symptoms | 14.94 | 6.61 | 15.09 | 7.06 | 0.587 | 0.02 |
| CIES-F2 Eating style | 16.29 | 9.73 | 15.03 | 9.82 | <0.001 * | 0.13 |
| CIES-F3 Anxiety-depression symptoms | 17.00 | 9.65 | 18.51 | 10.34 | <0.001 * | 0.15 |
| CIES-F4 Emotion dysregulation | 8.54 | 5.13 | 8.58 | 5.46 | 0.805 | 0.01 |
| n | % | n | % | p | |h| | |
| Tobacco | 166 | 28.2% | 173 | 29.3% | 0.306 | 0.02 |
| Alcohol | 172 | 30.8% | 132 | 22.9% | <0.001 * | 0.18 |
| Other illegal drugs | 75 | 14.5% | 58 | 10.2% | 0.003 * | 0.13 |
| Behavioral addictions | 440 | 66.9% | 452 | 68.4% | 0.209 | 0.03 |
| Asia (n=153) | Mean | SD | Mean | SD | p | |d| |
| Weight (kg) | 56.19 | 15.41 | 58.01 | 14.99 | 0.038 * | 0.12 |
| BMI (kg/m2) | 20.79 | 4.95 | 21.51 | 4.91 | 0.030 * | 0.15 |
| CIES-F1 ED symptoms | 17.91 | 8.14 | 15.55 | 7.53 | 0.006 * | 0.30 |
| CIES-F2 Eating style | 19.78 | 12.44 | 18.61 | 12.15 | 0.314 | 0.10 |
| CIES-F3 Anxiety-depression symptoms | 19.02 | 10.74 | 19.13 | 10.59 | 0.899 | 0.01 |
| CIES-F4 Emotion dysregulation | 9.13 | 5.75 | 8.61 | 5.73 | 0.241 | 0.09 |
| n | % | n | % | p | |h| | |
| Tobacco | 15 | 12.0% | 18 | 14.6% | 0.167 | 0.08 |
| Alcohol | 40 | 28.6% | 33 | 25.6% | 0.354 | 0.07 |
| Other illegal drugs | 19 | 13.6% | 19 | 14.4% | 0.736 | 0.02 |
| Behavioral addictions | 108 | 68.0% | 106 | 73.0% | 0.284 | 0.11 |
| Europe | Asia | |||||
|---|---|---|---|---|---|---|
| n = 676 | n = 153 | |||||
| Mean | SD | Mean | SD | p | |d| | |
| Weight (kg) | 1.27 | 7.47 | 2.37 | 8.73 | 0.138 | 0.13 |
| BMI (kg/m2) | 0.46 | 2.73 | 0.91 | 3.28 | 0.100 | 0.15 |
| CIES-F1 ED symptoms | −0.04 | 6.32 | −2.40 | 8.43 | <0.001 * | 0.32 |
| CIES-F2 Eating style | −1.37 | 6.90 | −0.95 | 11.48 | 0.583 | 0.04 |
| CIES-F3 Anxiety-depression symptoms | 1.40 | 7.54 | 0.22 | 8.62 | 0.113 | 0.15 |
| CIES-F4 Emotion dysregulation | 0.02 | 3.94 | −0.37 | 4.47 | 0.309 | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baenas, I.; Etxandi, M.; Munguía, L.; Granero, R.; Mestre-Bach, G.; Sánchez, I.; Ortega, E.; Andreu, A.; Moize, V.L.; Fernández-Real, J.-M.; et al. Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study. Nutrients 2022, 14, 100. https://doi.org/10.3390/nu14010100
Baenas I, Etxandi M, Munguía L, Granero R, Mestre-Bach G, Sánchez I, Ortega E, Andreu A, Moize VL, Fernández-Real J-M, et al. Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study. Nutrients. 2022; 14(1):100. https://doi.org/10.3390/nu14010100
Chicago/Turabian StyleBaenas, Isabel, Mikel Etxandi, Lucero Munguía, Roser Granero, Gemma Mestre-Bach, Isabel Sánchez, Emilio Ortega, Alba Andreu, Violeta L. Moize, Jose-Manuel Fernández-Real, and et al. 2022. "Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study" Nutrients 14, no. 1: 100. https://doi.org/10.3390/nu14010100
APA StyleBaenas, I., Etxandi, M., Munguía, L., Granero, R., Mestre-Bach, G., Sánchez, I., Ortega, E., Andreu, A., Moize, V. L., Fernández-Real, J.-M., Tinahones, F. J., Diéguez, C., Frühbeck, G., Le Grange, D., Tchanturia, K., Karwautz, A., Zeiler, M., Imgart, H., Zanko, A., ... Fernández-Aranda, F. (2022). Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study. Nutrients, 14(1), 100. https://doi.org/10.3390/nu14010100