
Association of Coffee and Tea Intake with Bone Mineral Density and Hip Fracture: A Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Statistical Analyses
2.5.1. BMD Group
2.5.2. Hip Fracture Group
3. Results
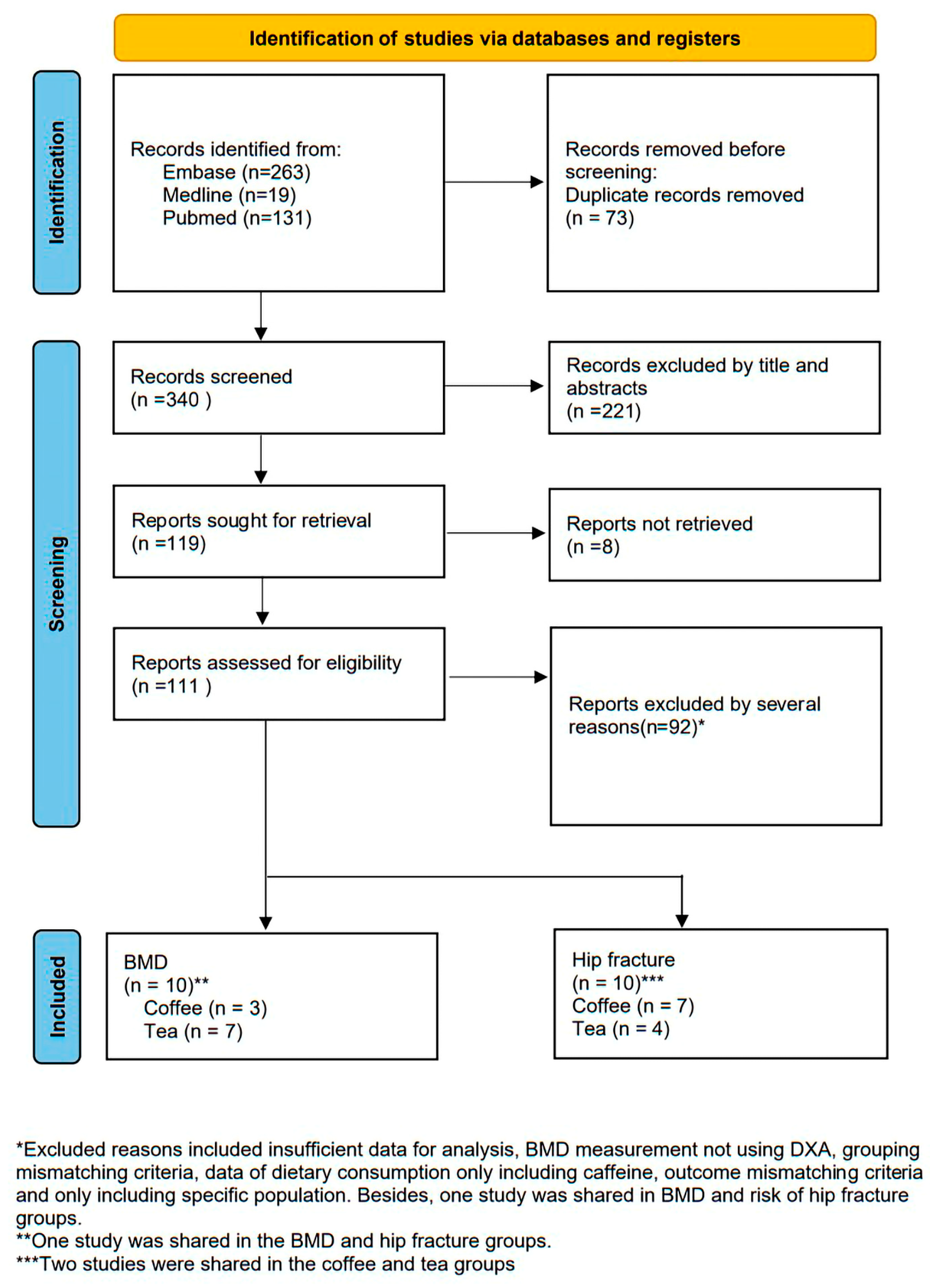
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment Results
3.4. Meta-Analysis Results
3.4.1. Results Pertaining to BMD
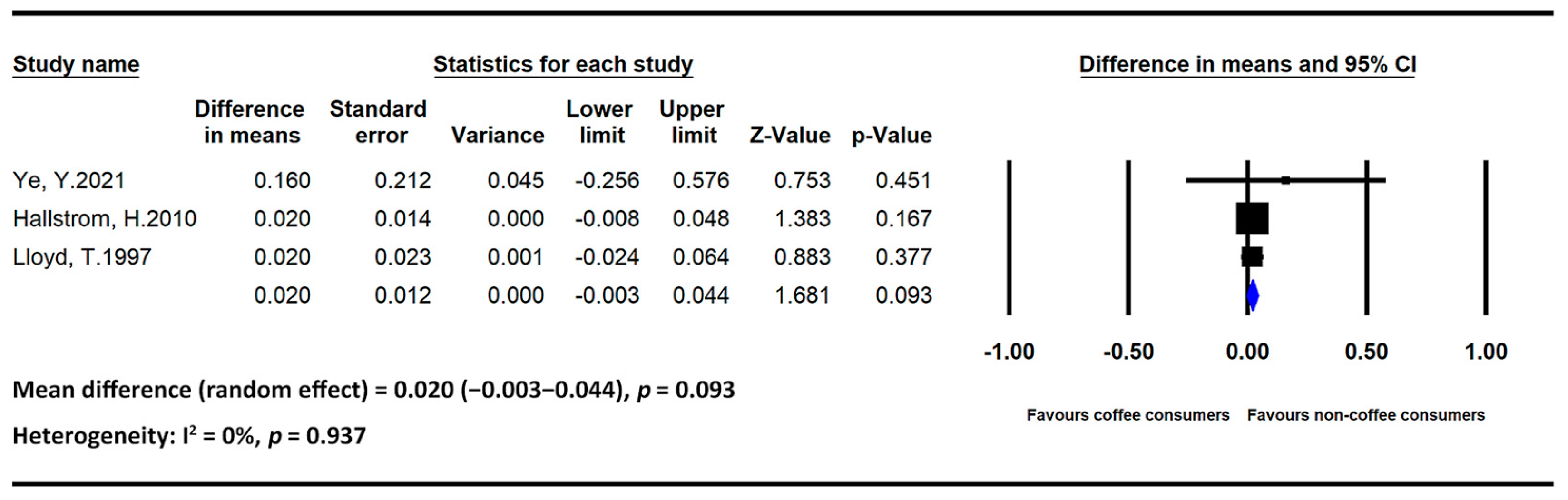
- Coffee
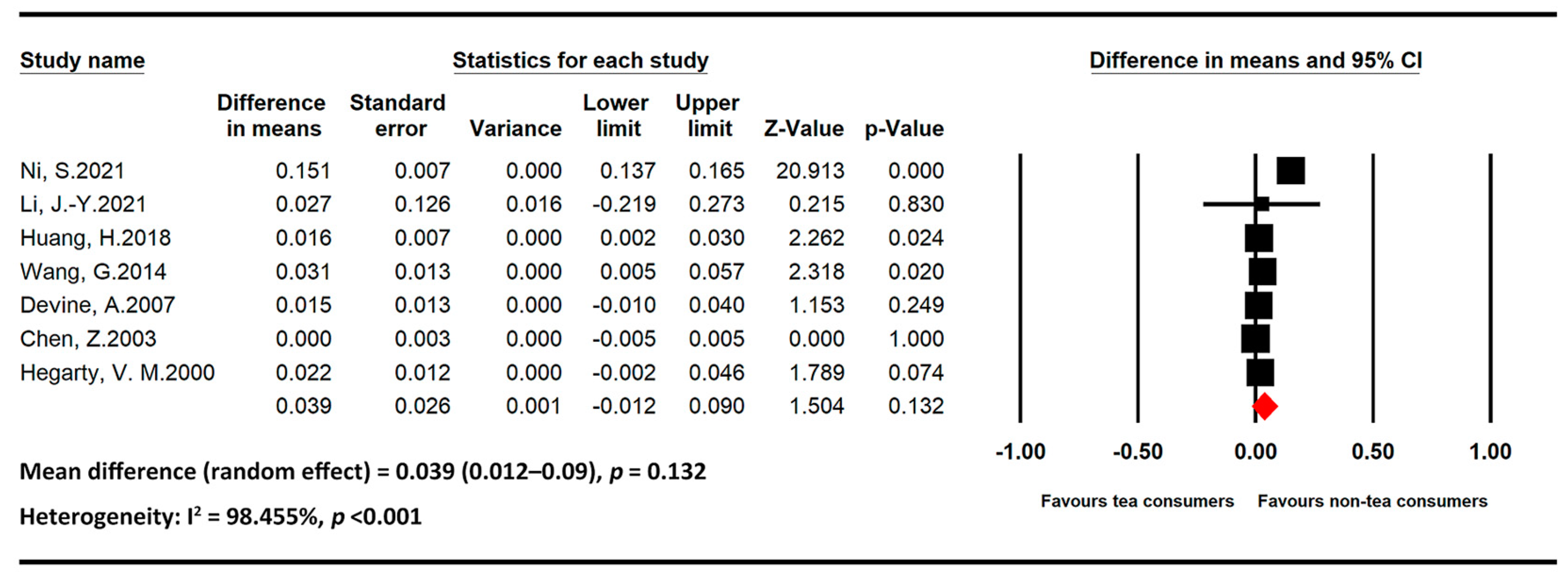
- Tea
3.4.2. Results Pertaining to Hip Fracture
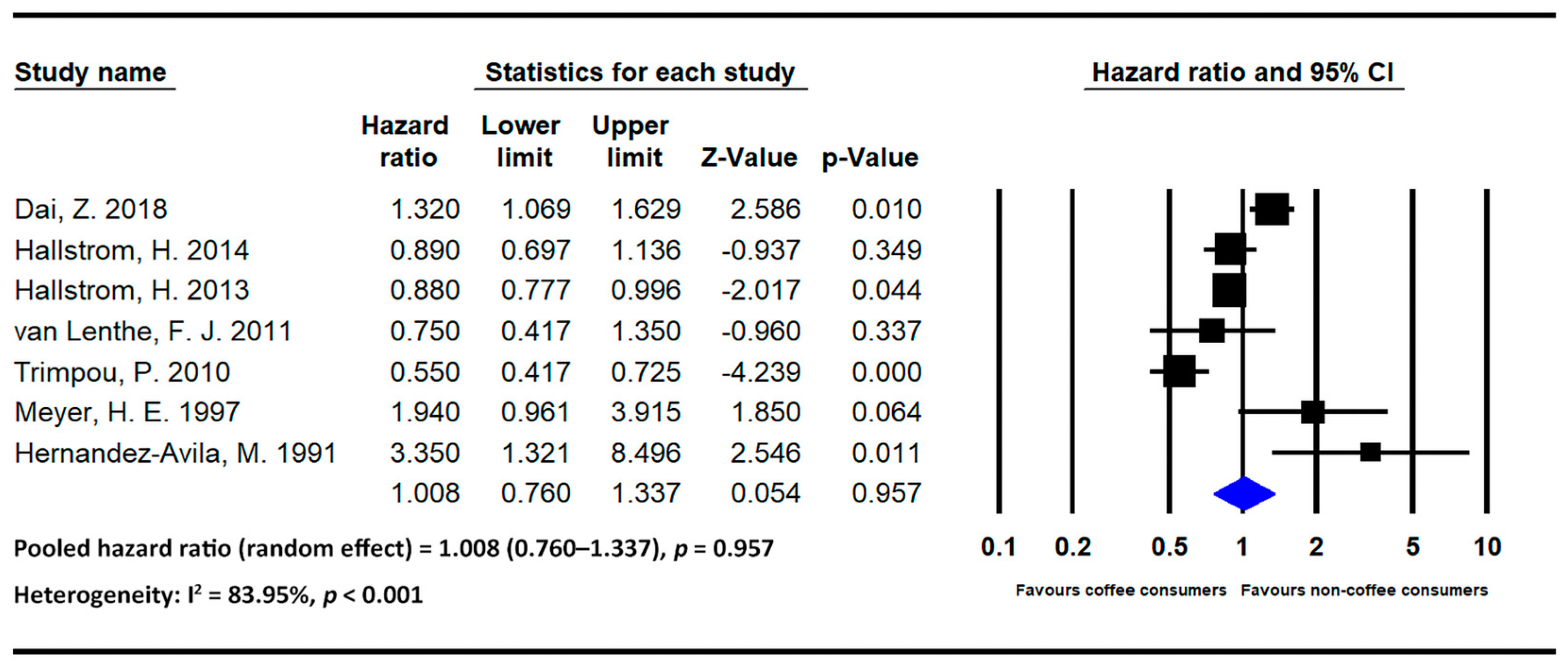
- Coffee
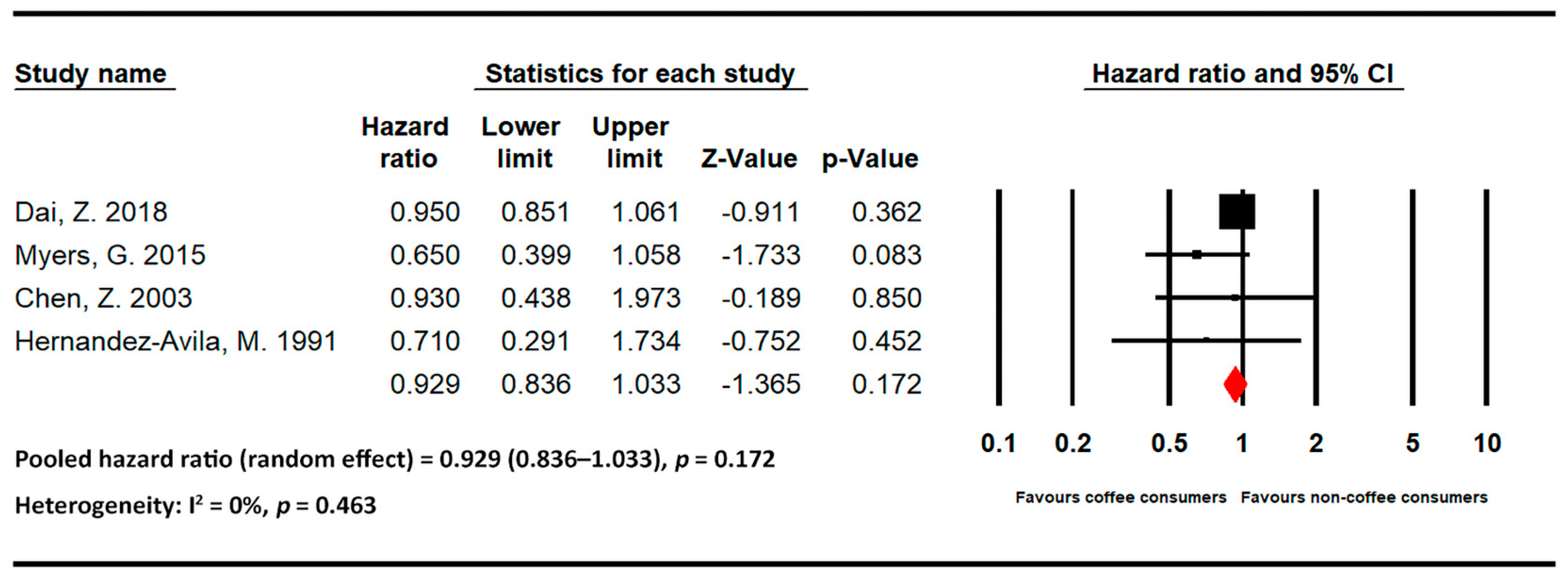
- Tea
3.5. Sensitivity Analysis
3.6. Publication Bias
3.6.1. Results Pertaining to BMD
3.6.2. Results Pertaining to Hip Fracture
4. Discussion
4.1. Effects of Coffee on Bone Health
4.2. Effects of Tea on Bone Health
4.3. Strengths
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trajanoska, K.; Schoufour, J.D.; de Jonge, E.A.L.; Kieboom, B.C.T.; Mulder, M.; Stricker, B.H.; Voortman, T.; Uitterlinden, A.G.; Oei, E.H.G.; Arfan Ikram, M.; et al. Fracture Incidence and Secular Trends between 1989 and 2013 in a Population Based Cohort: The Rotterdam Study. Bone 2018, 114, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.V.; Center, J.R.; Eisman, J.A. Osteoporosis in Elderly Men and Women: Effects of Dietary Calcium, Physical Activity, and Body Mass Index. J. Bone Miner. Res. 2000, 15, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, S.; Poon, S.; Robbins, J.; Bui, M.; Wang, X.; De Groot, L.; Van Loan, M.; Zadeh, A.G.; Nguyen, T.; Seeman, E. Effect of Dietary Sources of Calcium and Protein on Hip Fractures and Falls in Older Adults in Residential Care: Cluster Randomised Controlled Trial. BMJ 2021, 375, n2364. [Google Scholar] [CrossRef]
- Lips, P. Vitamin D Deficiency and Secondary Hyperparathyroidism in the Elderly: Consequences for Bone Loss and Fractures and Therapeutic Implications. Endocr. Rev. 2001, 22, 477–501. [Google Scholar] [CrossRef]
- Yuan, S.; Michaëlsson, K.; Wan, Z.; Larsson, S.C. Associations of Smoking and Alcohol and Coffee Intake with Fracture and Bone Mineral Density: A Mendelian Randomization Study. Calcif. Tissue Int. 2019, 105, 582–588. [Google Scholar] [CrossRef]
- Sheng, J.; Qu, X.; Zhang, X.; Zhai, Z.; Li, H.; Liu, X.; Li, H.; Liu, G.; Zhu, Z.; Hao, Y.; et al. Coffee, Tea, and the Risk of Hip Fracture: A Meta-Analysis. Osteoporos. Int. 2014, 25, 141–150. [Google Scholar] [CrossRef]
- Xu, F.; Liu, P.; Pekar, J.J.; Lu, H. Does Acute Caffeine Ingestion Alter Brain Metabolism in Young Adults? Neuroimage 2015, 110, 39–47. [Google Scholar] [CrossRef]
- Cappelletti, S.; Daria, P.; Sani, G.; Aromatario, M. Caffeine: Cognitive and Physical Performance Enhancer or Psychoactive Drug? Curr. Neuropharmacol. 2015, 13, 71–88. [Google Scholar] [CrossRef]
- Hernández-Avila, M.; Stampfer, M.J.; Ravnikar, V.A.; Willett, W.C.; Schiff, I.; Francis, M.; Longscope, C.; McKinlay, S.M. Caffeine and Other Predictors of Bone Density among Pre- and Perimenopausal Women. Epidemiology 1993, 4, 128–134. [Google Scholar] [CrossRef]
- De França, N.A.G.; Camargo, M.B.R.; Lazaretti-Castro, M.; Peters, B.S.E.; Martini, L.A. Dietary Patterns and Bone Mineral Density in Brazilian Postmenopausal Women with Osteoporosis: A Cross-Sectional Study. Eur. J. Clin. Nutr. 2016, 70, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Pettinger, M.B.; Ritenbaugh, C.; LaCroix, A.Z.; Robbins, J.; Caans, B.J.; Barad, D.H.; Hakim, I.A. Habitual Tea Consumption and Risk of Osteoporosis: A Prospective Study in the Women’s Health Initiative Observational Cohort. Am. J. Epidemiol. 2003, 158, 772–781. [Google Scholar] [CrossRef]
- Hansen, S.A.; Folsom, A.R.; Kushi, L.H.; Sellers, T.A. Association of Fractures with Caffeine and Alcohol in Postmenopausal Women: The Iowa Women’s Health Study. Public. Health Nutr. 2000, 3, 253–261. [Google Scholar] [CrossRef]
- Jokinen, H.; Pulkkinen, P.; Korpelainen, J.; Heikkinen, J.; Keinänen-Kiukaanniemi, S.; Jämsä, T.; Korpelainen, R. Risk Factors for Cervical and Trochanteric Hip Fractures in Elderly Women: A Population-Based 10-Year Follow-up Study. Calcif. Tissue Int. 2010, 87, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.E.; Pedersen, J.I.; Løken, E.B.; Tverdal, A. Dietary Factors and the Incidence of Hip Fracture in Middle-Aged Norwegians. A Prospective Study. Am. J. Epidemiol. 1997, 145, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Hallström Wolk A Glynn K Michaëlsson, H.A. Coffee, Tea and Caffeine Consumption in Relation to Osteoporotic Fracture Risk in a Cohort of Swedish Women. Osteoporos. Int. 2006, 17, 1055–1064. [Google Scholar] [CrossRef]
- van Geel, A.C.M.; Geusens, P.P.; Nagtzaam, I.F.; Schreurs, C.M.J.R.; van der Voort, D.J.M.; Rinkens, P.E.L.M.; Kester, A.D.M.; Dinant, G.J. Timing and Risk Factors for Clinical Fractures among Postmenopausal Women: A 5-Year Prospective Study. BMC Med. 2006, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Hallström, H.; Byberg, L.; Glynn, A.; Lemming, E.W.; Wolk, A.; Michaëlsson, K. Long-Term Coffee Consumption in Relation to Fracture Risk and Bone Mineral Density in Women. Am. J. Epidemiol. 2013, 178, 898–909. [Google Scholar] [CrossRef]
- Chau, Y.P.; Au, P.C.M.; Li, G.H.Y.; Sing, C.W.; Cheng, V.K.F.; Tan, K.C.B.; Kung, A.W.C.; Cheung, C.L. Serum Metabolome of Coffee Consumption and Its Association with Bone Mineral Density: The Hong Kong Osteoporosis Study. J. Clin. Endocrinol. Metab. 2020, 105, e619–e627. [Google Scholar] [CrossRef]
- Trimpou, P.; Odén, A.; Simonsson, T.; Wilhelmsen, L.; Landin-Wilhelmsen, K. High Serum Total Cholesterol Is a Long-Term Cause of Osteoporotic Fracture. Osteoporos. Int. 2011, 22, 1615–1620. [Google Scholar] [CrossRef]
- Trimpou, P.; Landin-Wilhelmsen, K.; Odén, A.; Rosengren, A.; Wilhelmsen, L. Male Risk Factors for Hip Fracture-a 30-Year Follow-up Study in 7495 Men. Osteoporos. Int. 2010, 21, 409–416. [Google Scholar] [CrossRef]
- van Lenthe, F.J.; Avendano, M.; van Beeck, E.F.; Mackenbach, J.P. Childhood and Adulthood Socioeconomic Position and the Hospital-Based Incidence of Hip Fractures after 13 Years of Follow-up: The Role of Health Behaviours. J. Epidemiol. Community Health (1978) 2011, 65, 980–985. [Google Scholar] [CrossRef]
- Määttä, M.; Terho, E.; Jokinen, H.; Pulkkinen, P.; Korpelainen, J.; Heikkinen, J.; Keinänen-Kiukaanniemi, S.; Jämsä, T.; Korpelainen, R. Lifestyle Factors and Site-Specific Risk of Hip Fracture in Community Dwelling Older Women--a 13-Year Prospective Population-Based Cohort Study. BMC Musculoskelet. Disord. 2012, 13, 173. [Google Scholar] [CrossRef]
- Hallström, H.; Wolk, A.; Glynn, A.; Michaëlsson, K.; Byberg, L.; Hallström, H.; Wolk, A.; Glynn, A.; Michaëlsson, K.; Byberg, L. Coffee Consumption and Risk of Fracture in the Cohort of Swedish Men (COSM). PLoS ONE 2014, 9, e97770. [Google Scholar] [CrossRef]
- Myers, G.; Prince, R.L.; Kerr, D.A.; Devine, A.; Woodman, R.J.; Lewis, J.R.; Hodgson, J.M. Tea and Flavonoid Intake Predict Osteoporotic Fracture Risk in Elderly Australian Women: A Prospective Study. Am. J. Clin. Nutr. 2015, 102, 958–965. [Google Scholar] [CrossRef]
- Dai, Z.; Jin, A.; Soh, A.Z.; Ang, L.W.; Yuan, J.M.; Koh, W.P. Coffee and Tea Drinking in Relation to Risk of Hip Fracture in the Singapore Chinese Health Study. Bone 2018, 112, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Avila, M.; Colditz, G.A.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Willett, W.C. Caffeine, Moderate Alcohol Intake, and Risk of Fractures of the Hip and Forearm in Middle-Aged Women. Am. J. Clin. Nutr. 1991, 54, 157–163. [Google Scholar] [CrossRef]
- Zeng, X.; Su, Y.; Tan, A.; Zou, L.; Zha, W.; Yi, S.; Lv, Y.; Kwok, T. The Association of Coffee Consumption with the Risk of Osteoporosis and Fractures: A Systematic Review and Meta-Analysis. Osteoporos. Int. 2022, 33, 1871–1893. [Google Scholar] [CrossRef] [PubMed]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 22 May 2022).
- Checklist for Analytical cross Sectional Studies in Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 22 May 2022).
- Mengist, B.; Desta, M.; Tura, A.K.; Habtewold, T.D.; Abajobir, A. Maternal near Miss in Ethiopia: Protective Role of Antenatal Care and Disparity in Socioeconomic Inequities: A Systematic Review and Meta-Analysis. Int. J. Afr. Nurs. Sci. 2021, 15, 100332. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.J.; Ge, J.R.; Chen, J.; Li, J.Y.; Chai, H.; Xie, L.H. Correlation between Hip Geometric Mechanics and Lifestyle Habits in Postmenopausal Women. Chin. J. Tissue Eng. Res. 2021, 25, 4277–4282. [Google Scholar] [CrossRef]
- Hallström, H.; Melhus, H.; Glynn, A.; Lind, L.; Syvänen, A.C.; Michalsson, K. Coffee Consumption and CYP1A2 Genotype in Relation to Bone Mineral Density of the Proximal Femur in Elderly Men and Women: A Cohort Study. Nutr. Metab. (Lond) 2010, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, T.; Rollings, N.; Eggli, D.F.; Kieselhorst, K.; Chinchilli, V.M. Dietary Caffeine Intake and Bone Status of Postmenopausal Women. Am. J. Clin. Nutr. 1997, 65, 1826–1830. [Google Scholar] [CrossRef] [PubMed]
- Ni, S.; Wang, L.; Wang, G.; Lin, J.; Ma, Y.; Zhao, X.; Ru, Y.; Zheng, W.; Zhang, X.; Zhu, S. Drinking Tea before Menopause Is Associated with Higher Bone Mineral Density in Postmenopausal Women. Eur. J. Clin. Nutr. 2021, 75, 1454–1464. [Google Scholar] [CrossRef]
- Li, J.Y.; Ge, J.R.; Chen, J.; Ye, Y.J.; Xie, L.H.; Li, L.; Chai, H. Clinical Study on the Influence of Tea Drinking Habits on Bone Mineral Density and Osteoporosis in Postmenopausal Women in Fuzhou City, China. Prog. Nutr. 2021, 23, e2021033. [Google Scholar] [CrossRef]
- Huang, H.; Han, G.Y.; Jing, L.P.; Chen, Z.Y.; Chen, Y.M.; Xiao, S.M. Tea Consumption Is Associated with Increased Bone Strength in Middle-Aged and Elderly Chinese Women. J. Nutr. Health Aging 2018, 22, 216–221. [Google Scholar] [CrossRef]
- Wang, G.; Liu, L.H.; Zhang, Z.; Zhang, F.; Li, S.; Chen, Y.; Zhao, H. Oolong Tea Drinking Could Help Prevent Bone Loss in Postmenopausal Han Chinese Women. Cell Biochem. Biophys. 2014, 70, 1289–1293. [Google Scholar] [CrossRef]
- Devine, A.; Hodgson, J.M.; Dick, I.M.; Prince, R.L. Tea Drinking Is Associated with Benefits on Bone Density in Older Women. Am. J. Clin. Nutr. 2007, 86, 1243–1247. [Google Scholar] [CrossRef]
- Hegarty, V.M.; May, H.M.; Khaw, K.T. Tea Drinking and Bone Mineral Density in Older Women. Am. J. Clin. Nutr. 2000, 71, 1003–1007. [Google Scholar] [CrossRef]
- Muraki, S.; Yamamoto, S.; Ishibashi, H.; Oka, H.; Yoshimura, N.; Kawaguchi, H.; Nakamura, K. Diet and Lifestyle Associated with Increased Bone Mineral Density: Cross-Sectional Study of Japanese Elderly Women at an Osteoporosis Outpatient Clinic. J. Orthop. Sci. 2007, 12, 317–320. [Google Scholar] [CrossRef]
- Xu, H.; Liu, T.; Hu, L.; Li, J.; Gan, C.; Xu, J.; Chen, F.; Xiang, Z.; Wang, X.; Sheng, J. Effect of Caffeine on Ovariectomy-Induced Osteoporosis in Rats. Biomed. Pharmacother. 2019, 112, 108650. [Google Scholar] [CrossRef] [PubMed]
- Berman, N.K.; Honig, S.; Cronstein, B.N.; Pillinger, M.H. The effects of caffeine on bone mineral density and fracture risk. Osteoporos. Int. 2022, 33, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.H.; Chen, C.; Yang, R.S.; Yen, Y.P.; Yang, Y.T.; Tsai, C. Caffeine Enhances Osteoclast Differentiation from Bone Marrow Hematopoietic Cells and Reduces Bone Mineral Density in Growing Rats. Journal. Orthop. Res. 2011, 29, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Rapuri, P.B.; Gallagher, J.C.; Nawaz, Z. Caffeine Decreases Vitamin D Receptor Protein Expression and 1,25(OH)2D3 Stimulated Alkaline Phosphatase Activity in Human Osteoblast Cells. J. Steroid Biochem. Mol. Biol. 2007, 103, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Dew, T.P.; Day, A.J.; Morgan, M.R.A. Bone Mineral Density, Polyphenols and Caffeine: A Reassessment. Nutr. Res. Rev. 2007, 20, 89–105. [Google Scholar] [CrossRef]
- Nawrot, P.; Jordan, S.; Eastwood, J.; Rotstein, J.; Hugenholtz, A.; Feeley, M. Effects of Caffeine on Human Health. Food Addit. Contam. 2003, 20, 1–30. [Google Scholar] [CrossRef]
- Tomaszewska, E.; Dobrowolski, P.; Winiarska-Mieczan, A.; Kwiecień, M.; Muszyński, S.; Tomczyk, A. The Effect of Tannic Acid on Bone Mechanical and Geometric Properties, Bone Density, and Trabecular Histomorphometry as Well as the Morphology of Articular and Growth Cartilages in Rats Co-Exposed to Cadmium and Lead Is Dose Dependent. Toxicol. Ind. Health 2017, 33, 855–866. [Google Scholar] [CrossRef]
- Zhang, Z.F.; Yang, J.L.; Jiang, H.C.; Lai, Z.; Wu, F.; Liu, Z.X. Updated Association of Tea Consumption and Bone Mineral Density: A Meta-Analysis. Medicine 2017, 96, e6437. [Google Scholar] [CrossRef]
- Chacko, S.M.; Thambi, P.T.; Kuttan, R.; Nishigaki, I. Beneficial Effects of Green Tea: A Literature Review. Chin. Med. 2010, 5, 13. [Google Scholar] [CrossRef]
- Al-Othman, A.; Al-Musharaf, S.; Al-Daghri, N.M.; Yakout, S.; Alkharfy, K.M.; Al-Saleh, Y.; Al-Attas, O.S.; Alokail, M.S.; Moharram, O.; Sabico, S.; et al. Tea and Coffee Consumption in Relation to Vitamin D and Calcium Levels in Saudi Adolescents. Nutr. J. 2012, 11, 56. [Google Scholar] [CrossRef]
- Massey, L.K.; Whiting, S.J. Caffeine, Urinary Calcium, Calcium Metabolism and Bone. J. Nutr. 1993, 123, 1611–1614. [Google Scholar] [CrossRef]
- Choi, E.M.; Hwang, J.K. Effects of (+)-Catechin on the Function of Osteoblastic Cells. Biol. Pharm. Bull. 2003, 26, 523–526. [Google Scholar] [CrossRef]
- Singh, B.N.; Shankar, S.; Srivastava, R.K. Green Tea Catechin, Epigallocatechin-3-Gallate (EGCG): Mechanisms, Perspectives and Clinical Applications. Biochem. Pharmacol. 2011, 82, 1807. [Google Scholar] [CrossRef]
- Shen, C.L.; Yeh, J.K.; Cao, J.J.; Wang, J.S. Green Tea and Bone Metabolism. Nutr. Res. 2009, 29, 437–456. [Google Scholar] [CrossRef]
- Park, Y.H.; Han, D.W.; Suh, H.; Ryu, G.H.; Hyon, S.H.; Cho, B.K.; Park, J.C. Protective Effects of Green Tea Polyphenol against Reactive Oxygen Species-Induced Oxidative Stress in Cultured Rat Calvarial Osteoblast. Cell Biol. Toxicol. 2003, 19, 325–337. [Google Scholar] [CrossRef]
- Picherit, C.; Coxam, V.; Bennetau-Pelissero, C.; Kati-Coulibaly, S.; Davicco, M.J.; Lebecque, P.; Barlet, J.P. Daidzein Is More Efficient than Genistein in Preventing Ovariectomy-Induced Bone Loss in Rats. J. Nutr. 2000, 130, 1675–1681. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BMD Group | |||||||
|---|---|---|---|---|---|---|---|
| Author, year | Country | Study design | Study population (age in years) | Groups | Number of participants | Bone mineral density mean difference | |
| Coffee | |||||||
| Ye, 2021 [34] | China | Cross-sectional | Postmenopausal women (47–90) | ≥2 cups/day vs. 0 cups/day | 648 | 0.16 | |
| Hallström, 2010 [35] | Sweden | Prospective cohort | Men and women (72) | >4 cups/day vs. 0–2 cups/day | 717 | 0.02 | |
| Lloyd, 1997 [36] | United States | Cross-sectional | Postmenopausal White women (55–70) | ≥5 cups/day vs. 0–2 cups/day | 138 | 0.02 | |
| Tea | |||||||
| Ni, 2021 [37] | China | Cross-sectional | Postmenopausal women (<80) | Drinkers vs. nondrinkers | 1377 | 0.151 | |
| Li, 2021 [38] | China | Cross-sectional | Postmenopausal women | Daily drinkers vs. nondrinkers | 947 | 0.027 | |
| Huang, 2018 [39] | China | Prospective cohort | Women (≥40) | ≥7 times/week vs. ≤1 time/week | 1495 | 0.016 | |
| Wang, 2014 [40] | China | Cross-sectional | Postmenopausal women (62.2519 ± 6.2837) | ≥1 cup/day vs. 0 cup/day | 680 | 0.031 | |
| Devine, 2007 [41] | Australia | Cross-sectional | Postmenopausal women (70–85) | ≥5 cups/day vs. 0 cup/day | 1027 | 0.015 | |
| Chen, 2003 [11] | United States | Prospective cohort | Postmenopausal women (50–79) | ≥5 cups/day vs. <1 cup/day | 91,465 | 0.000 | |
| Hegarty, 2000 [42] | United Kingdom | Cross-sectional | Postmenopausal women (65–76) | >6 cups/day vs. 0 cup/day | 1256 | 0.048 | |
| Hip Fracture Group | |||||||
| Author, year | Country | Design | Study population (age in years) | Groups | Number of participants | Number of hip fracture cases | Hazard ratio (95% confidence interval) |
| Coffee | |||||||
| Dai, 2018 [25] | Singapore | Prospective cohort | Men and women (45–74) | ≥4 cups/day vs. <1 cup/week | 63,154 | 2502 | 1.32 (1.07–1.63) |
| Hallström, 2014 [23] | Sweden | Prospective cohort | Men (45–79) | ≥4 cups/day vs. <1 cup/day | 42,978 | 1186 | 0.89 (0.70–1.14) |
| Hallström, 2013 [17] | Sweden | Prospective cohort | Women (not available) | ≥4 cups/day vs. <1 cup/day | 61,433 | 3871 | 0.88 (0.78–1.00) |
| van-Lenthe, 2011 [21] | The Netherlands | Prospective cohort | Women (25–74) | ≥3 cups/day vs. 0 cup/day | 16,578 | 192 | 0.75 (0.42–1.36) |
| Trimpou, 2010 [19] | Sweden | Prospective cohort | Men (46–56) | ≥5 cups/day vs. 0 cup/day | 7495 | 451 | 0.55 (0.42–0.73) |
| Meyer, 1997 [14] | Norway | Prospective cohort | Men and women (35–49) | ≥9 cups/day vs. <1 cup/day | 39,787 | 213 | Women: 1.94 (0.96–3.91) Men: 1.04 (0.37–2.94) |
| Hernandez-Avila, 1991 [28] | United States | Prospective cohort | Women (34–59) | ≥4 cups/day vs. individuals who rarely drank coffee | 84,484 | 65 | 3.35 (1.32–8.49) |
| Tea | |||||||
| Dai, 2018 [25] | Singapore | Prospective cohort | Men and women (45–74) | Daily vs. less frequent than weekly | 63,154 | 2502 | 0.95 (0.85–1.06) |
| Myers, 2015 [24] | Australia | Prospective cohort | Postmenopausal women (>75) | ≥3 cups/day vs. ≤1 cup/day | 1188 | 129 | 0.65 (0.40–1.06) |
| Chen, 2003 [11] | United States | Prospective cohort | Postmenopausal women (50–79) | ≥5 cups/day vs. <1 cup/day | 91,465 | 386 | 0.93 (0.44–1.98) |
| Hernandez-Avila, 1991 [26] | United States | Prospective cohort | Women (34–59) | ≥2 cups/day vs. individuals who rarely drank tea | 84,484 | 65 | 0.71 (0.29–1.73) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-C.; Shen, Y.-M.; Li, S.-B.; Huang, S.-W.; Kuo, Y.-J.; Chen, Y.-P. Association of Coffee and Tea Intake with Bone Mineral Density and Hip Fracture: A Meta-Analysis. Medicina 2023, 59, 1177. https://doi.org/10.3390/medicina59061177
Chen C-C, Shen Y-M, Li S-B, Huang S-W, Kuo Y-J, Chen Y-P. Association of Coffee and Tea Intake with Bone Mineral Density and Hip Fracture: A Meta-Analysis. Medicina. 2023; 59(6):1177. https://doi.org/10.3390/medicina59061177
Chicago/Turabian StyleChen, Chun-Ching, Yu-Ming Shen, Siou-Bi Li, Shu-Wei Huang, Yi-Jie Kuo, and Yu-Pin Chen. 2023. "Association of Coffee and Tea Intake with Bone Mineral Density and Hip Fracture: A Meta-Analysis" Medicina 59, no. 6: 1177. https://doi.org/10.3390/medicina59061177
APA StyleChen, C.-C., Shen, Y.-M., Li, S.-B., Huang, S.-W., Kuo, Y.-J., & Chen, Y.-P. (2023). Association of Coffee and Tea Intake with Bone Mineral Density and Hip Fracture: A Meta-Analysis. Medicina, 59(6), 1177. https://doi.org/10.3390/medicina59061177