
Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department

 , ,
, , 
Abstract
1. Introduction
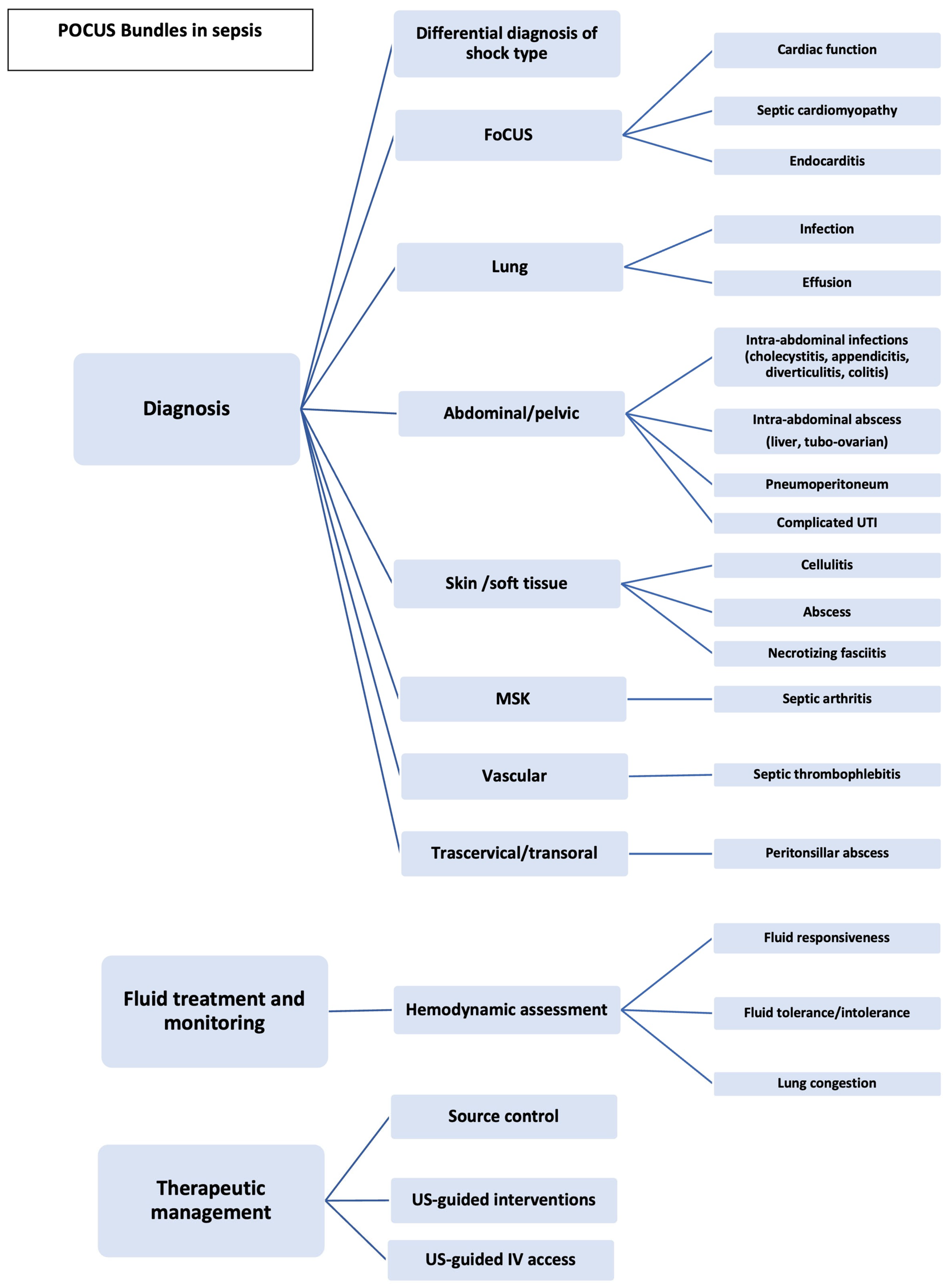
2. POCUS as a Multimodal Tool
3. POCUS as a Tool for Diagnosis
4. POCUS as a Tool for Fluid Treatment and Monitoring
5. POCUS as a Tool for Therapeutic Management
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Park, S. Sepsis: Early Recognition and Optimized Treatment. Tuberc. Respir. Dis. 2019, 82, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Whitson, M.R.; Mayo, P.H. Ultrasonography in the emergency department. Crit. Care 2016, 20, 227. [Google Scholar] [CrossRef]
- Tullo, G.; Candelli, M.; Gasparrini, I.; Micci, S.; Franceschi, F. Ultrasound in Sepsis and Septic Shock-From Diagnosis to Treatment. J. Clin. Med. 2023, 12, 1185. [Google Scholar] [CrossRef]
- Verras, C.; Ventoulis, I.; Bezati, S.; Matsiras, D.; Parissis, J.; Polyzogopoulou, E. Point of Care Ultrasonography for the Septic Patient in the Emergency Department: A Literature Review. J. Clin. Med. 2023, 12, 1105. [Google Scholar] [CrossRef]
- Keikha, M.; Salehi-Marzijarani, M.; Soldoozi Nejat, R.; Sheikh Motahar Vahedi, H.; Mirrezaie, S.M. Diagnostic Accuracy of Rapid Ultrasound in Shock (RUSH) Exam; A Systematic Review and Meta-analysis. Bull. Emerg. Trauma 2018, 6, 271–278. [Google Scholar] [CrossRef]
- Bekgoz, B.; Kilicaslan, I.; Bildik, F.; Keles, A.; Demircan, A.; Hakoglu, O.; Coskun, G.; Demir, H.A. BLUE protocol ultrasonography in Emergency Department patients presenting with acute dyspnea. Am. J. Emerg. Med. 2019, 37, 2020–2027. [Google Scholar] [CrossRef]
- Lichtenstein, D.A.; Meziere, G.A. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: The BLUE protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef]
- Neskovic, A.N.; Edvardsen, T.; Galderisi, M.; Garbi, M.; Gullace, G.; Jurcut, R.; Dalen, H.; Hagendorff, A.; Lancellotti, P.; European Association of Cardiovascular Imaging Document Reviewers; et al. Focus cardiac ultrasound: The European Association of Cardiovascular Imaging viewpoint. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 956–960. [Google Scholar] [CrossRef]
- Ohman, J.; Harjola, V.P.; Karjalainen, P.; Lassus, J. Focused echocardiography and lung ultrasound protocol for guiding treatment in acute heart failure. ESC Heart Fail. 2018, 5, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Hayhurst, C.; Lebus, C.; Atkinson, P.R.; Kendall, R.; Madan, R.; Talbot, J.; Ross, P.; Lewis, D. An evaluation of echo in life support (ELS): Is it feasible? What does it add? Emerg. Med. J. 2011, 28, 119–121. [Google Scholar] [CrossRef]
- Atkinson, P.R.; Milne, J.; Diegelmann, L.; Lamprecht, H.; Stander, M.; Lussier, D.; Pham, C.; Henneberry, R.; Fraser, J.M.; Howlett, M.K.; et al. Does Point-of-Care Ultrasonography Improve Clinical Outcomes in Emergency Department Patients With Undifferentiated Hypotension? An International Randomized Controlled Trial From the SHoC-ED Investigators. Ann. Emerg. Med. 2018, 72, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Stickles, S.P.; Carpenter, C.R.; Gekle, R.; Kraus, C.K.; Scoville, C.; Theodoro, D.; Tran, V.H.; Ubinas, G.; Raio, C. The diagnostic accuracy of a point-of-care ultrasound protocol for shock etiology: A systematic review and meta-analysis. CJEM 2019, 21, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Bagheri-Hariri, S.; Yekesadat, M.; Farahmand, S.; Arbab, M.; Sedaghat, M.; Shahlafar, N.; Takzare, A.; Seyedhossieni-Davarani, S.; Nejati, A. The impact of using RUSH protocol for diagnosing the type of unknown shock in the emergency department. Emerg. Radiol. 2015, 22, 517–520. [Google Scholar] [CrossRef]
- Ghane, M.R.; Gharib, M.; Ebrahimi, A.; Saeedi, M.; Akbari-Kamrani, M.; Rezaee, M.; Rasouli, H. Accuracy of early rapid ultrasound in shock (RUSH) examination performed by emergency physician for diagnosis of shock etiology in critically ill patients. J. Emerg. Trauma Shock 2015, 8, 5–10. [Google Scholar] [CrossRef]
- Javali, R.H.; Loganathan, A.; Srinivasarangan, M.; Patil, A.; Siddappa, G.B.; Satyanarayana, N.; Bheemanna, A.S.; Jagadeesh, S.; Betkerur, S. Reliability of Emergency Department Diagnosis in Identifying the Etiology of Nontraumatic Undifferentiated Hypotension. Indian J. Crit. Care Med. 2020, 24, 313–320. [Google Scholar] [CrossRef]
- Berg, I.; Walpot, K.; Lamprecht, H.; Valois, M.; Lanctot, J.F.; Srour, N.; van den Brand, C. A Systemic Review on the Diagnostic Accuracy of Point-of-Care Ultrasound in Patients With Undifferentiated Shock in the Emergency Department. Cureus 2022, 14, e23188. [Google Scholar] [CrossRef]
- Ramadan, A.; Abdallah, T.; Abdelsalam, H.; Mokhtar, A.; Razek, A.A. Accuracy of echocardiography and ultrasound protocol to identify shock etiology in emergency department. BMC Emerg. Med. 2022, 22, 117. [Google Scholar] [CrossRef]
- Lanspa, M.J.; Cirulis, M.M.; Wiley, B.M.; Olsen, T.D.; Wilson, E.L.; Beesley, S.J.; Brown, S.M.; Hirshberg, E.L.; Grissom, C.K. Right Ventricular Dysfunction in Early Sepsis and Septic Shock. Chest 2021, 159, 1055–1063. [Google Scholar] [CrossRef]
- Tucker, R.V.; Williams, K.; Theyyunni, N.; Fung, C.M. Sepsis-Induced Cardiomyopathy Detected With Focused Cardiac Ultrasound in the Emergency Department. J. Emerg. Med. 2022, 63, e91–e99. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.C.; Liu, M.; Hu, J.; Zeng, X.; Zhou, A.Y.; Chen, L. Diagnosis of infective endocarditis using echocardiography. Medicine 2019, 98, e17141. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, D.A.; Wiley, B.M. Integrated Multiorgan Bedside Ultrasound for the Diagnosis and Management of Sepsis and Septic Shock. Semin. Respir. Crit. Care Med. 2021, 42, 641–649. [Google Scholar] [CrossRef]
- La Via, L.; Astuto, M.; Dezio, V.; Muscara, L.; Palella, S.; Zawadka, M.; Vignon, P.; Sanfilippo, F. Agreement between subcostal and transhepatic longitudinal imaging of the inferior vena cava for the evaluation of fluid responsiveness: A systematic review. J. Crit. Care 2022, 71, 154108. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; McSparron, J.I.; Kien, D.T.; Stone, D.J.; Roberts, D.H.; Schwartzstein, R.M.; Vieillard-Baron, A.; Celi, L.A. Transthoracic echocardiography and mortality in sepsis: Analysis of the MIMIC-III database. Intensive Care Med. 2018, 44, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Via, G.P.; Price, S.; Storti, E. Echocardiography in the sepsis syndromes. Crit. Ultrasound J. 2011, 3, 71–85. [Google Scholar] [CrossRef]
- Gu, X.; Zhou, F.; Wang, Y.; Fan, G.; Cao, B. Respiratory viral sepsis: Epidemiology, pathophysiology, diagnosis and treatment. Eur. Respir. Rev. 2020, 29, 157–169. [Google Scholar] [CrossRef]
- Sultan, S.R. Association Between Lung Ultrasound Patterns and Pneumonia. Ultrasound Q. 2022, 38, 246–249. [Google Scholar] [CrossRef]
- Shah, A.; Oliva, C.; Stem, C.; Cummings, E.Q. Application of dynamic air bronchograms on lung ultrasound to diagnose pneumonia in undifferentiated respiratory distress. Respir. Med. Case Rep. 2022, 39, 101706. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Mathis, G.; Cui, X.W.; Ignee, A.; Hocke, M.; Hirche, T.O. Ultrasound of the pleurae and lungs. Ultrasound Med. Biol. 2015, 41, 351–365. [Google Scholar] [CrossRef]
- Chavez, M.A.; Shams, N.; Ellington, L.E.; Naithani, N.; Gilman, R.H.; Steinhoff, M.C.; Santosham, M.; Black, R.E.; Price, C.; Gross, M.; et al. Lung ultrasound for the diagnosis of pneumonia in adults: A systematic review and meta-analysis. Respir. Res. 2014, 15, 50. [Google Scholar] [CrossRef]
- Yousefifard, M.; Baikpour, M.; Ghelichkhani, P.; Asady, H.; Shahsavari Nia, K.; Moghadas Jafari, A.; Hosseini, M.; Safari, S. Screening Performance Characteristic of Ultrasonography and Radiography in Detection of Pleural Effusion; a Meta-Analysis. Emergency 2016, 4, 1–10. [Google Scholar] [PubMed]
- Hecker, A.; Reichert, M.; Reuss, C.J.; Schmoch, T.; Riedel, J.G.; Schneck, E.; Padberg, W.; Weigand, M.A.; Hecker, M. Intra-abdominal sepsis: New definitions and current clinical standards. Langenbecks Arch. Surg. 2019, 404, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.; Brown, M.; McLaughlin, K.; Atkinson, P.; Thompson, J.; Powelson, S.; Clark, S.; Lang, E. Emergency physician-performed ultrasound to diagnose cholelithiasis: A systematic review. Acad. Emerg. Med. 2011, 18, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Summers, S.M.; Menchine, M.D.; Fox, J.C.; Wang, R. The Absence of Gallstones on Point-of-Care Ultrasound Rules Out Acute Cholecystitis. J. Emerg. Med. 2015, 49, 475–480. [Google Scholar] [CrossRef]
- Benabbas, R.; Hanna, M.; Shah, J.; Sinert, R. Diagnostic Accuracy of History, Physical Examination, Laboratory Tests, and Point-of-care Ultrasound for Pediatric Acute Appendicitis in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2017, 24, 523–551. [Google Scholar] [CrossRef]
- Wong, C.; Teitge, B.; Ross, M.; Young, P.; Robertson, H.L.; Lang, E. The Accuracy and Prognostic Value of Point-of-care Ultrasound for Nephrolithiasis in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2018, 25, 684–698. [Google Scholar] [CrossRef]
- Nazerian, P.; Morello, F.; Prota, A.; Betti, L.; Lupia, E.; Apruzzese, L.; Oddi, M.; Grosso, F.; Grifoni, S.; Pivetta, E.; et al. Diagnostic accuracy of physician’s gestalt in suspected COVID-19: Prospective bicentric study. Acad. Emerg. Med. 2021, 28, 404–411. [Google Scholar] [CrossRef]
- Kameda, T.; Taniguchi, N. Overview of point-of-care abdominal ultrasound in emergency and critical care. J. Intensive Care 2016, 4, 53. [Google Scholar] [CrossRef]
- Khor, M.; Cutten, J.; Lim, J.; Weerakkody, Y. Sonographic detection of pneumoperitoneum. BJR Case Rep. 2017, 3, 20160146. [Google Scholar] [CrossRef]
- Edell, S.L.; Gefter, W.B. Ultrasonic differentiation of types of ascitic fluid. AJR Am. J. Roentgenol. 1979, 133, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Von Kuenssberg Jehle, D.; Stiller, G.; Wagner, D. Sensitivity in detecting free intraperitoneal fluid with the pelvic views of the FAST exam. Am. J. Emerg. Med. 2003, 21, 476–478. [Google Scholar] [CrossRef] [PubMed]
- Paajanen, H.; Lahti, P.; Nordback, I. Sensitivity of transabdominal ultrasonography in detection of intraperitoneal fluid in humans. Eur. Radiol. 1999, 9, 1423–1425. [Google Scholar] [CrossRef] [PubMed]
- Cardona-Castro, W.; Zuluaga-Gomez, M.; Gonzalez-Arroyave, D.; Ardila, C.M. Accuracy of point-of-care ultrasonography in the diagnosis of necrotizing fasciitis: A case report. Biomed. Rep. 2022, 17, 98. [Google Scholar] [CrossRef]
- Subramaniam, S.; Bober, J.; Chao, J.; Zehtabchi, S. Point-of-care Ultrasound for Diagnosis of Abscess in Skin and Soft Tissue Infections. Acad. Emerg. Med. 2016, 23, 1298–1306. [Google Scholar] [CrossRef]
- Marks, A.; Patel, D.; Sundaram, T.; Johnson, J.; Gottlieb, M. Ultrasound for the diagnosis of necrotizing fasciitis: A systematic review of the literature. Am. J. Emerg. Med. 2023, 65, 31–35. [Google Scholar] [CrossRef]
- Adhikari, S.; Blaivas, M. Sonography first for subcutaneous abscess and cellulitis evaluation. J. Ultrasound Med. 2012, 31, 1509–1512. [Google Scholar] [CrossRef]
- Mnif, J.; Khannous, M.; Keskes, H.; Louati, N.; Damak, J.; Kechaou, M.S. Ultrasonography in the diagnostic approach of septic arthritis. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1997, 83, 148–155. [Google Scholar]
- Kotlarsky, P.; Shavit, I.; Kassis, I.; Eidelman, M. Treatment of septic hip in a pediatric ED: A retrospective case series analysis. Am. J. Emerg. Med. 2016, 34, 602–605. [Google Scholar] [CrossRef]
- Long, B.; Koyfman, A.; Gottlieb, M. Evaluation and Management of Septic Arthritis and its Mimics in the Emergency Department. West J. Emerg. Med. 2019, 20, 331–341. [Google Scholar] [CrossRef]
- Perez, J.; Sorensen, S.; Rosselli, M. Utilisation of musculoskeletal ultrasonography for the evaluation of septic arthritis in a patient presenting to the emergency department with fever during the era of COVID-19. BMJ Case Rep. 2021, 14, e242370. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.; Anjum, F.; dela Cruz, J. Deep Venous Thrombosis Ultrasound Evaluation; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Yeh, Y.T.; Tsai, S.E.; Chen, Y.C.; Yang, S.F.; Yeh, H.W.; Wang, B.Y.; Yeh, L.T.; Shih, N.C.; Wang, Y.H.; Chen, Y.Y.; et al. Deep Venous Thrombosis and Risk of Consequent Sepsis Event: A Retrospective Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 7879. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S. Point-of-care ultrasound diagnosis of peripheral vein septic thrombophlebitis in the emergency department. J. Emerg. Med. 2013, 44, 183–184. [Google Scholar] [CrossRef] [PubMed]
- Froehlich, M.H.; Huang, Z.; Reilly, B.K. Utilization of ultrasound for diagnostic evaluation and management of peritonsillar abscesses. Curr. Opin. Otolaryngol. Head Neck Surg. 2017, 25, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Bryczkowski, C.; Haussner, W.; Rometti, M.; Wei, G.; Morrison, D.; Geria, R.; McCoy, J.V. Impact of Bedside Ultrasound on Emergency Department Length of Stay and Admission in Patients With a Suspected Peritonsillar Abscess. Cureus 2022, 14, e32207. [Google Scholar] [CrossRef]
- Izumo, M.; Akashi, Y.J. Role of echocardiography for takotsubo cardiomyopathy: Clinical and prognostic implications. Cardiovasc. Diagn. Ther. 2018, 8, 90–100. [Google Scholar] [CrossRef]
- Soni, N.J.; Franco, R.; Velez, M.I.; Schnobrich, D.; Dancel, R.; Restrepo, M.I.; Mayo, P.H. Ultrasound in the diagnosis and management of pleural effusions. J. Hosp. Med. 2015, 10, 811–816. [Google Scholar] [CrossRef]
- Borzellino, G.; Massimiliano Motton, A.P.; Minniti, F.; Montemezzi, S.; Tomezzoli, A.; Genna, M. Sonographic diagnosis of acute cholecystitis in patients with symptomatic gallstones. J. Clin. Ultrasound 2016, 44, 152–158. [Google Scholar] [CrossRef]
- Chan, L.; Shin, L.K.; Pai, R.K.; Jeffrey, R.B. Pathologic continuum of acute appendicitis: Sonographic findings and clinical management implications. Ultrasound Q. 2011, 27, 71–79. [Google Scholar] [CrossRef]
- Cohen, A.; Li, T.; Stankard, B.; Nelson, M. A Prospective Evaluation of Point-of-Care Ultrasonographic Diagnosis of Diverticulitis in the Emergency Department. Ann. Emerg. Med. 2020, 76, 757–766. [Google Scholar] [CrossRef]
- Worlicek, H.; Lutz, H.; Heyder, N.; Matek, W. Ultrasound findings in Crohn’s disease and ulcerative colitis: A prospective study. J. Clin. Ultrasound 1987, 15, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Watanabe, G.; Hashimoto, M.; Udagawa, H.; Okuda, C.; Takeuchi, K. Sonographic features of intra-abdominal abscess caused by spilled stones during laparoscopic cholecystectomy. J. Med. Ultrason. 2003, 30, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Bacci, M.; Kushwaha, R.; Cabrera, G.; Kalivoda, E.J. Point-of-Care Ultrasound Diagnosis of Pneumoperitoneum in the Emergency Department. Cureus 2020, 12, e8503. [Google Scholar] [CrossRef] [PubMed]
- Edell, S.L.; Bonavita, J.A. The sonographic appearance of acute pyelonephritis. Radiology 1979, 132, 683–685. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, K.; Kibbee, N.; Stubbs, A. Ultrasound for the Evaluation of Skin and Soft Tissue Infections. Mo. Med. 2015, 112, 202–205. [Google Scholar]
- Al Nakshabandi, N.; Joharji, E.; El-Haddad, H. Radiology in Rheumatology. In Skills in Rheumatology; Almoallim, H., Cheikh, M., Eds.; Springer: Singapore, 2021; pp. 105–123. [Google Scholar] [CrossRef]
- Secko, M.; Sivitz, A. Think ultrasound first for peritonsillar swelling. Am. J. Emerg. Med. 2015, 33, 569–572. [Google Scholar] [CrossRef]
- Long, B.; Koyfman, A. Clinical Mimics: An Emergency Medicine-Focused Review of Sepsis Mimics. J. Emerg. Med. 2017, 52, 34–42. [Google Scholar] [CrossRef]
- Soans, S.T.P. Sepsis Mimics. Pediatr. Inf. Dis. 2019, 1, 145–147. [Google Scholar] [CrossRef]
- Rola, P.; Miralles-Aguiar, F.; Argaiz, E.; Beaubien-Souligny, W.; Haycock, K.; Karimov, T.; Dinh, V.A.; Spiegel, R. Clinical applications of the venous excess ultrasound (VExUS) score: Conceptual review and case series. Ultrasound J. 2021, 13, 32. [Google Scholar] [CrossRef]
- Bentzer, P.; Griesdale, D.E.; Boyd, J.; MacLean, K.; Sirounis, D.; Ayas, N.T. Will This Hemodynamically Unstable Patient Respond to a Bolus of Intravenous Fluids? JAMA 2016, 316, 1298–1309. [Google Scholar] [CrossRef]
- Kattan, E.; Castro, R.; Miralles-Aguiar, F.; Hernandez, G.; Rola, P. The emerging concept of fluid tolerance: A position paper. J. Crit. Care 2022, 71, 154070. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Wang, X.T.; Long, Y.; Liu, D.W. Monitoring Changes in Hepatic Venous Velocities Flow after a Fluid Challenge Can Identify Shock Patients Who Lack Fluid Responsiveness. Chin. Med. J. 2017, 130, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- Kenny, J.S. Assessing Fluid Intolerance with Doppler Ultrasonography: A Physiological Framework. Med. Sci. 2022, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Girardis, M.; Martin-Loeches, I. Source control in the management of sepsis and septic shock. Intensive Care Med. 2022, 48, 1799–1802. [Google Scholar] [CrossRef]
- Brogi, E.; Gargani, L.; Bignami, E.; Barbariol, F.; Marra, A.; Forfori, F.; Vetrugno, L. Thoracic ultrasound for pleural effusion in the intensive care unit: A narrative review from diagnosis to treatment. Crit. Care 2017, 21, 325. [Google Scholar] [CrossRef]
- Nelson, M.; Stankard, B.; Greco, J.; Okumura, Y. Point of Care Ultrasound Diagnosis of Empyema. J. Emerg. Med. 2016, 51, 140–143. [Google Scholar] [CrossRef]
- Cantey, E.P.; Walter, J.M.; Corbridge, T.; Barsuk, J.H. Complications of thoracentesis: Incidence, risk factors, and strategies for prevention. Curr. Opin. Pulm. Med. 2016, 22, 378–385. [Google Scholar] [CrossRef]
- Mercaldi, C.J.; Lanes, S.F. Ultrasound guidance decreases complications and improves the cost of care among patients undergoing thoracentesis and paracentesis. Chest 2013, 143, 532–538. [Google Scholar] [CrossRef]
- Cho, J.; Jensen, T.P.; Reierson, K.; Mathews, B.K.; Bhagra, A.; Franco-Sadud, R.; Grikis, L.; Mader, M.; Dancel, R.; Lucas, B.P.; et al. Recommendations on the Use of Ultrasound Guidance for Adult Abdominal Paracentesis: A Position Statement of the Society of Hospital Medicine. J. Hosp. Med. 2019, 14, E7–E15. [Google Scholar] [CrossRef]
- Sola, E.; Sole, C.; Gines, P. Management of uninfected and infected ascites in cirrhosis. Liver Int. 2016, 36 (Suppl. S1), 109–115. [Google Scholar] [CrossRef]
- Navuluri, R.; Hoyer, M.; Osman, M.; Fergus, J. Emergent Treatment of Acute Cholangitis and Acute Cholecystitis. Semin. Intervent. Radiol. 2020, 37, 14–23. [Google Scholar] [CrossRef]
- Yarmohammadi, H.; Covey, A.M. Percutaneous biliary interventions and complications in malignant bile duct obstruction. Chin. Clin. Oncol. 2016, 5, 68. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Saito, Y.; Ogura, H.; Yaguchi, Y.; Shimizu, T.; Hasegawa, Y. Ultrasound-Guided Needle Aspiration of Peritonsillar Abscesses: Utility of Transoral Pharyngeal Ultrasonography. Diagnostics 2019, 9, 141. [Google Scholar] [CrossRef]
- Efesoy, O.; Saylam, B.; Bozlu, M.; Cayan, S.; Akbay, E. The results of ultrasound-guided percutaneous nephrostomy tube placement for obstructive uropathy: A single-centre 10-year experience. Turk. J. Urol. 2018, 44, 329–334. [Google Scholar] [CrossRef]
- Uppot, R.N. Emergent nephrostomy tube placement for acute urinary obstruction. Tech. Vasc. Interv. Radiol. 2009, 12, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Puebla, D.L.; Farrow, R.A. Ultrasound Guided Arthrocentesis; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Shah, K.H.; McGillicuddy, D.; Spear, J.; Edlow, J.A. Predicting difficult and traumatic lumbar punctures. Am. J. Emerg. Med. 2007, 25, 608–611. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Huang, J.; Liu, J.C. Efficacy of ultrasound guidance for lumbar punctures: A systematic review and meta-analysis of randomised controlled trials. Postgrad. Med. J. 2021, 97, 40–47. [Google Scholar] [CrossRef]
- Soni, N.J.; Franco-Sadud, R.; Kobaidze, K.; Schnobrich, D.; Salame, G.; Lenchus, J.; Kalidindi, V.; Mader, M.J.; Haro, E.K.; Dancel, R.; et al. Recommendations on the Use of Ultrasound Guidance for Adult Lumbar Puncture: A Position Statement of the Society of Hospital Medicine. J. Hosp. Med. 2019, 14, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Berlanga-Macias, C.; Diez-Fernandez, A.; Martinez-Hortelano, J.A.; Sequi-Dominguez, I.; Saz-Lara, A.; Pozuelo-Carrascosa, D.; Martinez-Vizcaino, V. Ultrasound-guided versus traditional method for peripheral venous access: An umbrella review. BMC Nurs. 2022, 21, 307. [Google Scholar] [CrossRef]
- Young, J.B.; Gondek, S.P.; Kahn, S.A.; May, A.K. Challenging IV Access in the Patient with Septic Shock. In Complications in Acute Care Surgery: The Management of Difficult Clinical Scenarios; Diaz, J.J., Efron, D.T., Eds.; Springer International Publishing: Cham, Germany, 2017; pp. 1–13. [Google Scholar] [CrossRef]
- Blanco, P. Ultrasound-guided peripheral venous cannulation in critically ill patients: A practical guideline. Ultrasound J. 2019, 11, 27. [Google Scholar] [CrossRef]
- Hafeez, S.B.; Ahmed, A.; Akhtar, A.; Ishtiaq, W.; Javed, N.U.S.; Abbas, K.; Khan, M.; Zafar, H.; Jawed, A. Catheter-Related Bloodstream Infection With Femoral Central Access Versus Internal Jugular Access in Patients Admitting to Medical Intensive Care Unit. Cureus 2022, 14, e29416. [Google Scholar] [CrossRef]
- Ishizuka, M.; Nagata, H.; Takagi, K.; Kubota, K. Femoral venous catheterization is a major risk factor for central venous catheter-related bloodstream infection. J. Invest. Surg. 2009, 22, 16–21. [Google Scholar] [CrossRef]
- Ishizuka, M.; Nagata, H.; Takagi, K.; Kubota, K. Right internal jugular vein is recommended for central venous catheterization. J. Invest. Surg. 2010, 23, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Zawadka, M.; La Via, L.; Wong, A.; Olusanya, O.; Muscara, L.; Continella, C.; Andruszkiewicz, P.; Sanfilippo, F. Real-Time Ultrasound Guidance as Compared With Landmark Technique for Subclavian Central Venous Cannulation: A Systematic Review and Meta-Analysis With Trial Sequential Analysis. Crit. Care Med. 2023, 51, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Sundaram, T.; Holladay, D.; Nakitende, D. Ultrasound-Guided Peripheral Intravenous Line Placement: A Narrative Review of Evidence-based Best Practices. West J. Emerg. Med. 2017, 18, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Duran-Gehring, P.E.; Guirgis, F.W.; McKee, K.C.; Goggans, S.; Tran, H.; Kalynych, C.J.; Wears, R.L. The bubble study: Ultrasound confirmation of central venous catheter placement. Am. J. Emerg. Med. 2015, 33, 315–319. [Google Scholar] [CrossRef]
- Mosier, J.M.; Stolz, U.; Milligan, R.; Roy-Chaudhury, A.; Lutrick, K.; Hypes, C.D.; Billheimer, D.; Cairns, C.B. Impact of Point-of-Care Ultrasound in the Emergency Department on Care Processes and Outcomes in Critically Ill Nontraumatic Patients. Crit. Care Explor. 2019, 1, e0019. [Google Scholar] [CrossRef]
- Levitov, A.; Marik, P.E. Echocardiographic assessment of preload responsiveness in critically ill patients. Cardiol. Res. Pract. 2012, 2012, 819696. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Diagnosis | US Findings |
|---|---|
| Septic cardiomyopathy [5] | Reduced EF Ventricular hypokinesis |
| Endocarditis [22] | Amorphous, independent motioned, echogenic masses, associated with cardiac valves Thickened, abnormal valve |
| Takotsubo cardiomyopathy [57] | Impaired contractility of the apex and hypercontractility of LV base |
| Severe RV failure [20] | Dilated RV and right atrium |
| Ischemic cardiomyopathy [26] | RWMAs |
| Pneumonia [28,29,30] | Focal B-lines Lung consolidation or hepatization Dynamic air bronchograms Subpleural abnormalities Irregular and thickened pleura |
| Pleural effusion [58] | Anechoic fluid collection above the diaphragm Spine sign Quad sign Sinusoid sign |
| Empyema [58] | Echogenic pleural effusion ± septations |
| Cholecystitis [59] | Gallbladder wall thickening (>3 mm) and/or oedema Positive sonographic Murphy sign Pericholecystic fluid Gallstones |
| Appendicitis [60] | Dilated (>6 mm), aperistaltic, non-compressible appendix Appendicolith Hyperechoic periappendiceal fat |
| Diverticulitis [61] | Colonic wall thickening >5 mm Fat enhancement Visualized diverticula Air artifacts Tenderness with compression of the probe |
| Colitis [62] | Increased symmetrical wall thickening Submucosal echogenicity |
| Intra-abdominal abscess [63] | Anechoic to hypoechoic cystic collections Internal echoes and debris Irregular margins, ±septations |
| Pneumoperitoneum [64] | Peritoneal stripe enhancement Repeating, horizontal long-path reverberation artifacts that extend into the far field Gas bubbles |
| Pyelonephritis [65] | Abnormal echogenicity of the renal parenchyma Gas bubbles (emphysematous pyelonephritis) Particulate matter in the collecting system |
| Cellulitis [44] | Cobble-stone appearance Increased echogenicity of the subcutaneous tissue |
| Necrotic fasciitis [44] | Fascial and subcutaneous tissue thickening Fascial fluid Subcutaneous air |
| Skin/soft tissue abscess [66] | Irregular hypoechoic fluid collection |
| Septic arthritis [67] | Joint effusion Increased peri-synovial vascularity |
| Septic thrombophlebitis [52] | Venous thrombus Non compressible vein |
| Peritonsillar abscess [68] | Hypoechoic, heterogeneous or complex cystic structure |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polyzogopoulou, E.; Velliou, M.; Verras, C.; Ventoulis, I.; Parissis, J.; Osterwalder, J.; Hoffmann, B. Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department. Medicina 2023, 59, 1180. https://doi.org/10.3390/medicina59061180
Polyzogopoulou E, Velliou M, Verras C, Ventoulis I, Parissis J, Osterwalder J, Hoffmann B. Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department. Medicina. 2023; 59(6):1180. https://doi.org/10.3390/medicina59061180
Chicago/Turabian StylePolyzogopoulou, Effie, Maria Velliou, Christos Verras, Ioannis Ventoulis, John Parissis, Joseph Osterwalder, and Beatrice Hoffmann. 2023. "Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department" Medicina 59, no. 6: 1180. https://doi.org/10.3390/medicina59061180
APA StylePolyzogopoulou, E., Velliou, M., Verras, C., Ventoulis, I., Parissis, J., Osterwalder, J., & Hoffmann, B. (2023). Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department. Medicina, 59(6), 1180. https://doi.org/10.3390/medicina59061180