

Systematic Review of In Vitro Studies on Distortion Generated by Intraoral Scanning Systems for Oral Rehabilitations with More Than Three Implants


Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Analysis Protocol
2.1.1. Generating the PICO Question
2.1.2. Search Methods
2.1.3. Establishing Inclusion and Exclusion Criteria
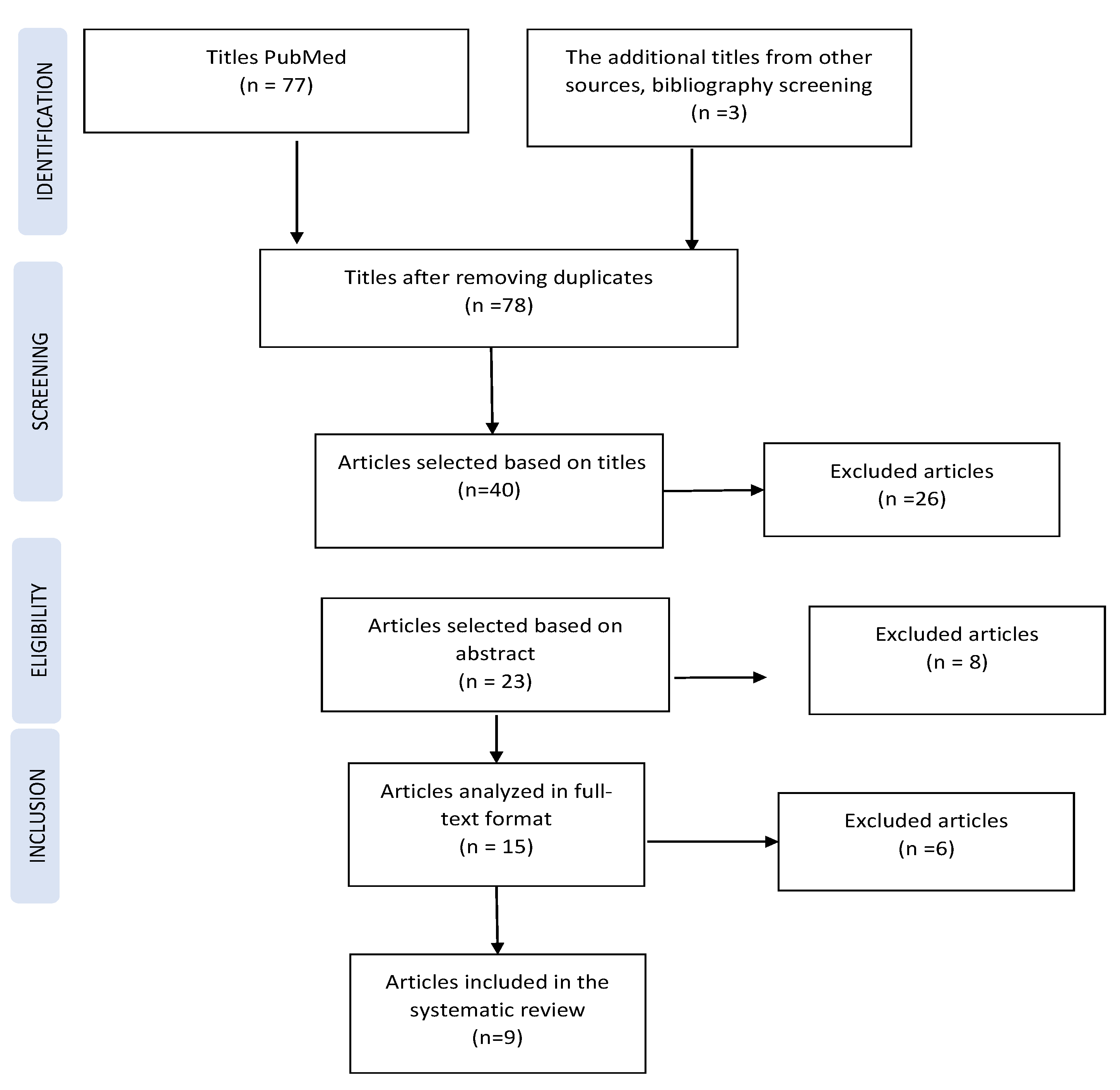
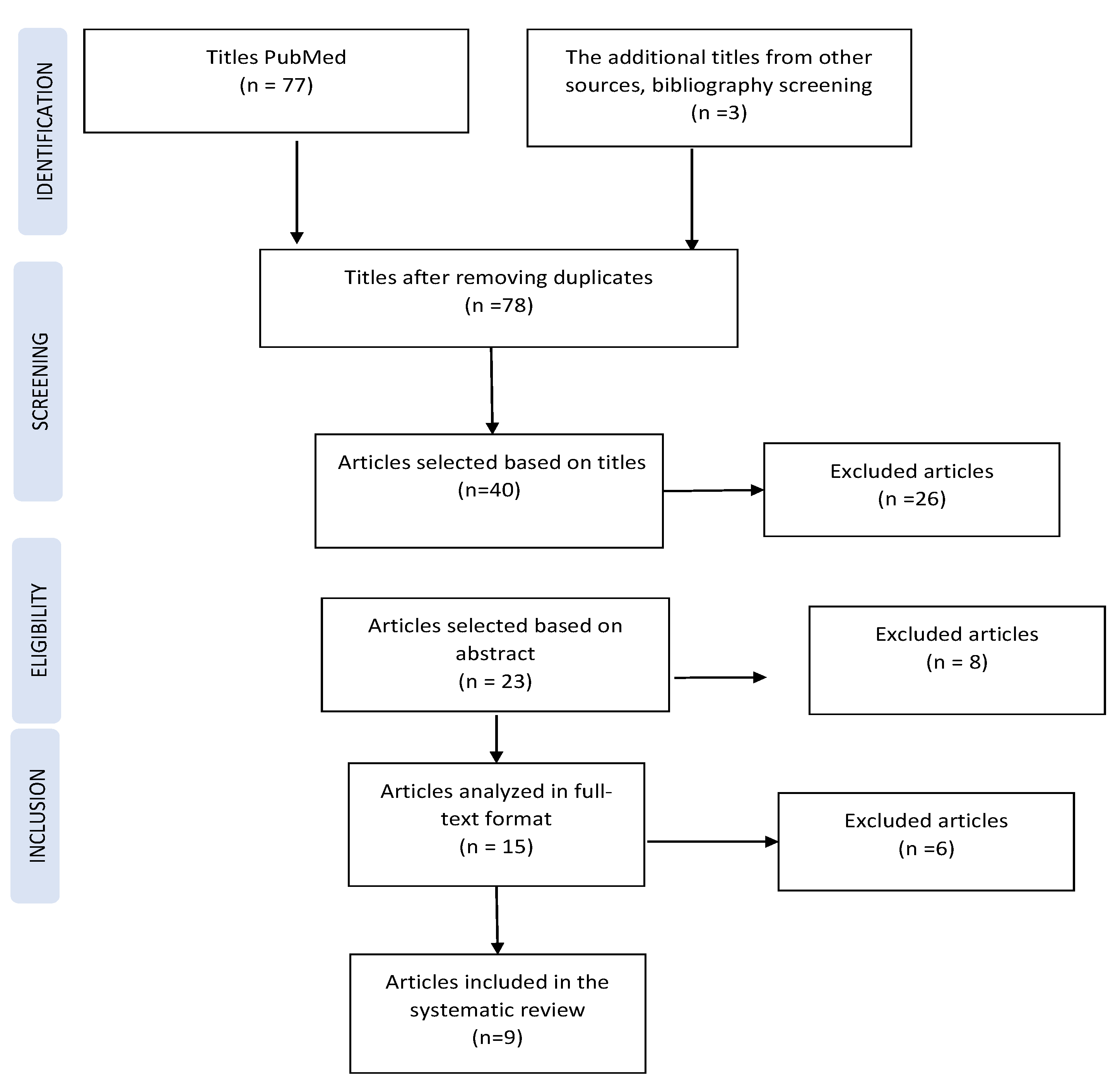
2.1.4. Selecting Studies for the Systematic Analysis
2.1.5. Qualitative Analysis
3. Results
3.1. Systematic Review
3.1.1. The Impact of the Registration Technique/Scanning System on Scanning Error (Table 1)

{kind=link}
| Study (Reference) | Scanning Technology | Conventional Impression Material and Technique | Statistically Significant Differences |
|---|---|---|---|
| 1.Rech-Ortega [25] | True Definition | Polyether—direct technique | Yes/No depending on the recorded distance |
| 2. Moura [31] | Dental Wings 3 Series | Synthetic elastomer—direct and indirect technique | No |
| 3. Kim K.R. [24] | Trios 3Shape | Silicone addition—direct technique | Yes |
| 4. Bohner L. [32] | inEos Blue | Silicone addition | Yes—cusp No—occlusal fossae |
| 5. Alikhasi M. [33] | Trios 3Shape | Silicone addition—direct and indirect technique | No |
| 6. Papaspyridakos P. [34] | Trios 3Shape | Polyether—technique with bonded and sectioned transfer copings, and bonded and unsectioned copings | No |
| 7. Mizumoto R.M. [27] | Trios 3Shape
| - | Yes |
| 8. Vandeweghe S. [26] | Lava COS 3M True Definition Cerec Omnicam 3Shape Trios | - | Yes |
| 9. Flugge T. [28] | iTero Trios 3Shape 3M True Definition | - | Yes |
- Accuracy: 3Shape (28 µm) > True Def (35 µm) > Cerec (61 µm) > Lava (112 µm);
- Precision: True Def (30 µm) > 3Shape (33 µm) > Cerec (59 µm) > Lava (66 µm).
3.1.2. The Impact of Interimplant Distance on Scanning Error (Table 2)
| Study | Implant Number | Scanning Technology | Interimplantar Distance (mm) | Statistically Significant Differences | |
|---|---|---|---|---|---|
| 1. Rech-Ortega [25] | 6 | True Definition | 1–2/5–6: ~11 2–3/–5: ~14 3–4: ~10 | 1–4/3–6: ~32 | yes |
| 1–6: ~40 | |||||
| 2. Kim K.R. [24] | 6 | Trios 3Shape | - | yes | |
| 3. Flugge T. [28] | 5 | Trios 3Shape True Definition iTero | 35–36: 6.6 33–35/45–47:11 33–36: 18 | 35–45: 40 36–47: 50 | yes |
3.1.3. The Impact of Implant Angulation on Scanning Error (Table 3)
| Study (Reference) | Number of Implants | Implants’ Characteristics | Statistically Significant Differences | ||
|---|---|---|---|---|---|
| Position | Angulation | Direction | |||
| 1. Moura R.V. [32] | 6 | 17 23 | 15° | Mesial Distal | No |
| 15, 12, 25, 27 | 0° | - | |||
| 2. Alikhasi M. [34] | 4 | 13, 23 | 0° | - | No (digital) Yes (conventional) |
| 15, 25 | 45° | Distal | |||
| 3. Papaspyridakos P. [35] | 5 | 45, 35 | 15° | Distal | No |
| 43, 33, 41–31 | 0° | ||||
3.1.4. The Impact of the Scan Body Type on Scanning Error
3.2. Statistical Analysis in the Studies
3.3. Evaluation of Study Design from a Qualitative Perspective (Table 4 and Table 5)
| Study (Reference) | Does the Study Address a Clearly Formulated Question? | Does the Study Use Methods That Are Described in Detail and Valid to Answer the Issued Question? | Do the Valid Results Generated Lead to the Conclusions Presented in a Justified Manner? |
|---|---|---|---|
| 1. Rech-Ortega C. [25] | vague | superficial | yes |
| 2. Moura R.V. [32] | yes | yes | yes |
| 3. Kim K.R. [24] | yes | yes | yes |
| 4. Bohner L. [33] | yes | superficial | yes |
| 5. Alikhasi M. [34] | yes | yes | yes |
| 6. Papaspyridakos P. [35] | yes | yes | yes |
| 7. Mizumoto R.M. [27] | yes | yes | yes |
| 8. Vandeweghe S. [26] | vague | superficial | yes |
| 9. Flugge T. [28] | No | superficial | yes |
| Study (Reference) | Is the Adopted Strategy in Accordance with the Recommendations of the Scanning Equipment Manufacturer? | Have Any Modifications Been Made to the Standard Strategy Recommended by the Manufacturer? If So, Was the Manufacturer Consulted Regarding the Modifications Made? | Did the Strategy Generate Scan Gaps that Required a Rescan? |
|---|---|---|---|
| 1. Rech-Ortega [25] | Is not described | Does not mention | Does not mention |
| 2. Moura R.V. [32] | Extraoral scanning | Does not apply | Does not mention |
| 3. Kim K.R. [24] | Yes | Without modifications | Does not mention |
| 4. Bohner L. [33] | Extraoral scanning | Does not apply | Does not mention |
| 5. Alikhasi M. [34] | No | Does not mention | Does not mention |
| 6. Papaspyridakos P. [35] | Yes | Without modifications | Does not mention |
| 7.Mizumoto R.M. [27] | Yes | Without modifications | Does not mention |
| 8.Vandeweghe S. [26] | Is not described | Does not mention | Does not mention |
| 9. Flugge T. [28] | Yes | Without modifications | Does not mention |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef]
- Wiranto, M.G.; Engelbrecht, W.P.; Nolthenius, H.E.T.; van der Meer, W.J.; Ren, Y. Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 140–147. [Google Scholar] [CrossRef]
- Grünheid, T.; McCarthy, S.D.; Larson, B.E. Clinical use of a direct chairside oral scanner: An assessment of accuracy, time, and patient acceptance. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 673–682. [Google Scholar] [CrossRef]
- Driscoll, C.D. Clinical Applications of Digital Dental Technology; Wiley: Hoboken, NJ, USA, 2015; ISBN 9781118655795. [Google Scholar] [CrossRef]
- Mehl, A.; Ender, A.; Mörmann, W.; Attin, T. Accuracy testing of a new intraoral 3D camera. Int. J. Comput. Dent. 2009, 12, 11–28. [Google Scholar] [CrossRef]
- Rudolph, H.; Salmen, H.; Moldan, M.; Kuhn, K.; Sichwardt, V.; Wöstmann, B.; Luthardt, R.G. Accuracy of intraoral and extraoral digital data acquisition for dental restorations. J. Appl. Oral Sci. 2016, 24, 85–94. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.-C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.A.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406.e1. [Google Scholar] [CrossRef]
- Joda, T.; Braegger, U. Time-Efficiency Analysis Comparing Digital and Conventional Workflows for Implant Crowns: A Prospective Clinical Crossover Trial. Int. J. Oral Maxillofac. Implant. 2015, 30, 1047–1053. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Investig. 2016, 20, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Suh, K.-J.; Lee, K.-M. Validity of intraoral scans compared with plaster models: An in-vivo comparison of dental measurements and 3D surface analysis. PLoS ONE 2016, 11, e0157713. [Google Scholar] [CrossRef] [PubMed]
- Muallah, J.; Wesemann, C.; Nowak, R.; Robben, J.; Mah, J.; Pospiech, P.; Bumann, A. Accuracy of full-arch scans using intraoral and extraoral scanners: An in vitro study using a new method of evaluation Genauigkeit von Ganzkieferscans mit intraoralen und extraoralen Scannern: Eine In-vitro-Untersuchung. Int. J. Comput. Dent. 2017, 20, 151–164. [Google Scholar] [PubMed]
- Wesemann, C.; Muallah, J.; Mah, J.; Bumann, A. Accuracy and efficiency of full-arch digitalization and 3D printing: A comparison between desktop model scanners, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017, 48, 41–50. [Google Scholar] [CrossRef]
- Seelbach, P.; Brueckel, C.; Wöstmann, B. Accuracy of digital and conventional impression techniques and workflow. Clin. Oral Investig. 2013, 17, 1759–1764. [Google Scholar] [CrossRef]
- Güth, J.-F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Investig. 2013, 17, 1201–1208. [Google Scholar] [CrossRef]
- Su, T.-S.; Sun, J. Comparison of repeatability between intraoral digital scanner and extraoral digital scanner: An in-vitro study. J. Prosthodont. Res. 2015, 59, 236–242. [Google Scholar] [CrossRef]
- Rhee, Y.-K.; Huh, Y.-H.; Cho, L.-R.; Park, C.-J. Comparison of intraoral scanning and conventional impression techniques using 3-dimensional superimposition. J. Adv. Prosthodont. 2015, 7, 460–467. [Google Scholar] [CrossRef]
- ISO 5725-1; Accuracy (Trueness and Precision) of Measurement Methods and Results–Part 1: General Principles and Definitions. 1998. Available online: https://www.iso.org/obp/ui/#iso:std:iso:5725:-1:ed-1:v1:en (accessed on 23 March 2021).
- Menditto, A.; Patriarca, M.; Magnusson, B. Understanding the meaning of accuracy, trueness and precision. Accredit. Qual. Assur. 2007, 12, 45–47. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.R.; Seo, K.-Y.; Kim, S. Conventional open-tray impression versus intraoral digital scan for implant-level complete-arch impression. J. Prosthet. Dent. 2019, 122, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Rech-Ortega, C.; Fernandez-Estevan, L.; Sola-Ruiz, M.; Agustin-Panadero, R.; Labaig-Rueda, C. Comparative in vitro study of the accuracy of impression techniques for dental implants: Direct technique with an elastomeric impression material versus intraoral scanner. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e89–e95. [Google Scholar] [CrossRef]
- Vandeweghe, S.; Vervack, V.; Dierens, M.; De Bruyn, H. Accuracy of digital impressions of multiple dental implants: An in vitro study. Clin. Oral Implant. Res. 2017, 28, 648–653. [Google Scholar] [CrossRef]
- Mizumoto, R.M.; Yilmaz, B.; McGlumphy, E.A.J.; Seidt, J.; Johnston, W.M. Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses. J. Prosthet. Dent. 2020, 123, 96–104. [Google Scholar] [CrossRef]
- Flügge, T.V.; Att, W.; Metzger, M.C.; Nelson, K. Precision of Dental Implant Digitization Using Intraoral Scanners. Int. J. Prosthodont. 2016, 29, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.Y.; Yee, S.H.X.; Wong, K.M.; Tan, Y.H.; Tan, K.B.C. Comparison of Three-Dimensional Accuracy of Digital and Conventional Implant Impressions: Effect of Interimplant Distance in an Edentulous Arch. Int. J. Oral Maxillofac. Implant. 2019, 34, 366–380. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Taylor, R. How to read a paper: Papers that go beyond numbers (qualitative research). BMJ 1997, 315, 740–743. [Google Scholar] [CrossRef]
- Moura, R.V.; Kojima, A.N.; Saraceni, C.H.C.; Bassolli, L.; Balducci, I.; Özcan, M.; Mesquita, A.M.M. Evaluation of the Accuracy of Conventional and Digital Impression Techniques for Implant Restorations. J. Prosthodont. 2019, 28, e530–e535. [Google Scholar] [CrossRef]
- Bohner, L.; Hanisch, M.; Canto, G.D.L.; Mukai, E.; Sesma, N.; Neto, P.T. Accuracy of Casts Fabricated by Digital and Conventional Implant Impressions. J. Oral Implant. 2019, 45, 94–99. [Google Scholar] [CrossRef]
- Alikhasi, M.; Siadat, H.; Nasirpour, A.; Hasanzade, M. Three-Dimensional Accuracy of Digital Impression versus Conventional Method: Effect of Implant Angulation and Connection Type. Int. J. Dent. 2018, 2018, 3761750. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Gallucci, G.O.; Chen, C.-J.; Hanssen, S.; Naert, I.; Vandenberghe, B. Digital versus conventional implant impressions for edentulous patients: Accuracy outcomes. Clin. Oral Implant. Res. 2016, 27, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Conrad, H.J.; Pesun, I.J.; DeLong, R.; Hodges, J.S. Accuracy of two impression techniques with angulated implants. J. Prosthet. Dent. 2007, 97, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Andriessen, F.S.; Rijkens, D.R.; van der Meer, W.J.; Wismeijer, D.W. Applicability and accuracy of an intraoral scanner for scanning multiple implants in edentulous mandibles: A pilot study. J. Prosthet. Dent. 2014, 111, 186–194. [Google Scholar] [CrossRef] [PubMed]
- McLean, J.W.; von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oancea, L.; Luca, I.; Radulescu, S.; Macris, A.; Ciocan, T. Systematic Review of In Vitro Studies on Distortion Generated by Intraoral Scanning Systems for Oral Rehabilitations with More Than Three Implants. Prosthesis 2023, 5, 1139-1152. https://doi.org/10.3390/prosthesis5040080
Oancea L, Luca I, Radulescu S, Macris A, Ciocan T. Systematic Review of In Vitro Studies on Distortion Generated by Intraoral Scanning Systems for Oral Rehabilitations with More Than Three Implants. Prosthesis. 2023; 5(4):1139-1152. https://doi.org/10.3390/prosthesis5040080
Chicago/Turabian StyleOancea, Luminita, Ioana Luca, Sergiu Radulescu, Andrei Macris, and Toma Ciocan. 2023. "Systematic Review of In Vitro Studies on Distortion Generated by Intraoral Scanning Systems for Oral Rehabilitations with More Than Three Implants" Prosthesis 5, no. 4: 1139-1152. https://doi.org/10.3390/prosthesis5040080
APA StyleOancea, L., Luca, I., Radulescu, S., Macris, A., & Ciocan, T. (2023). Systematic Review of In Vitro Studies on Distortion Generated by Intraoral Scanning Systems for Oral Rehabilitations with More Than Three Implants. Prosthesis, 5(4), 1139-1152. https://doi.org/10.3390/prosthesis5040080