Impact of Health Systems on the Implementation of Intermittent Preventive Treatment for Malaria in Pregnancy in Sub-Saharan Africa: A Narrative Synthesis


Abstract
1. Introduction
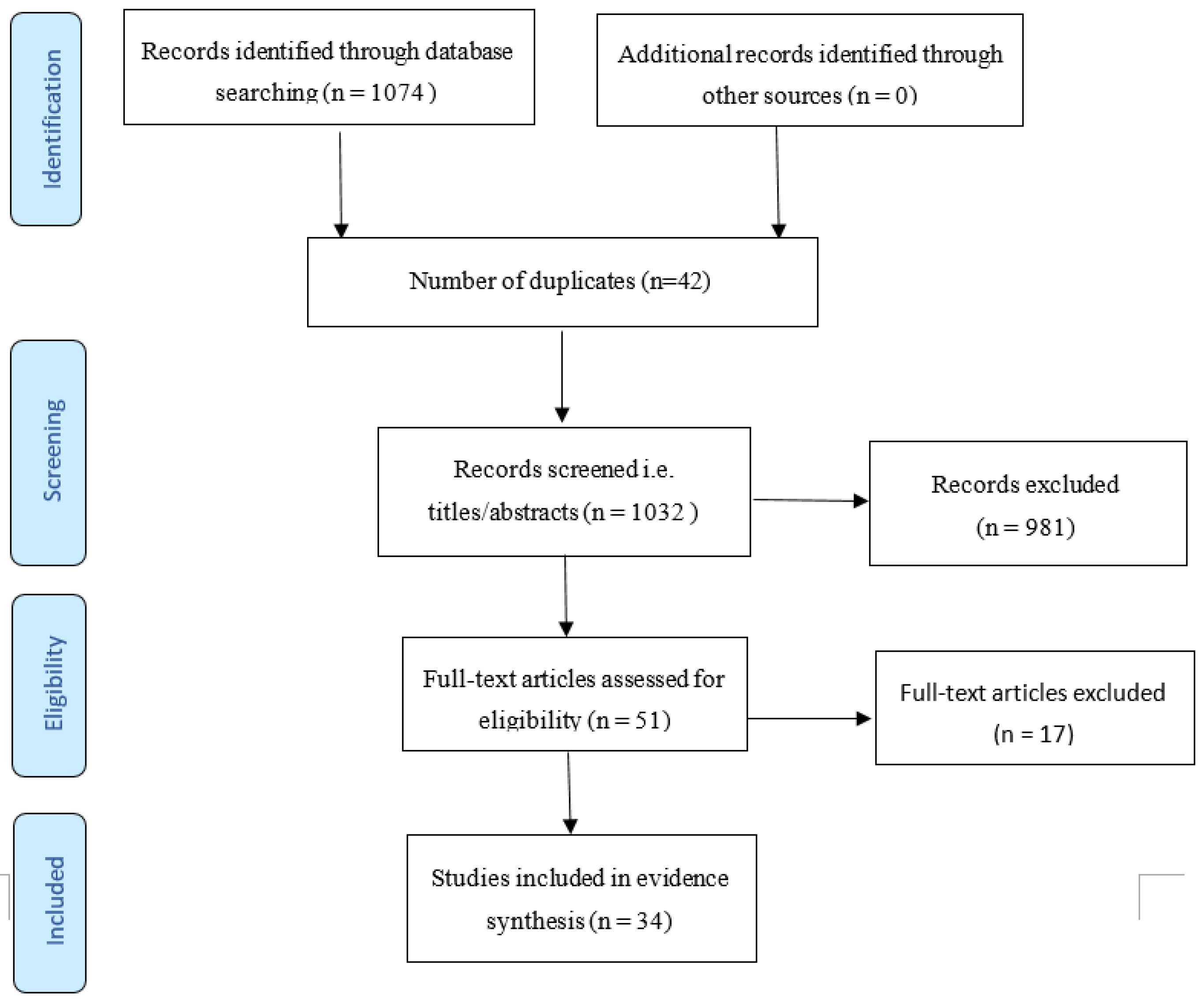
2. Methods
- Keywords: health systems; malaria in pregnancy; intermittent preventive treatment of malaria.
- Inclusion criteria:
- Studies that describe the health system and investigate malaria in pregnancy
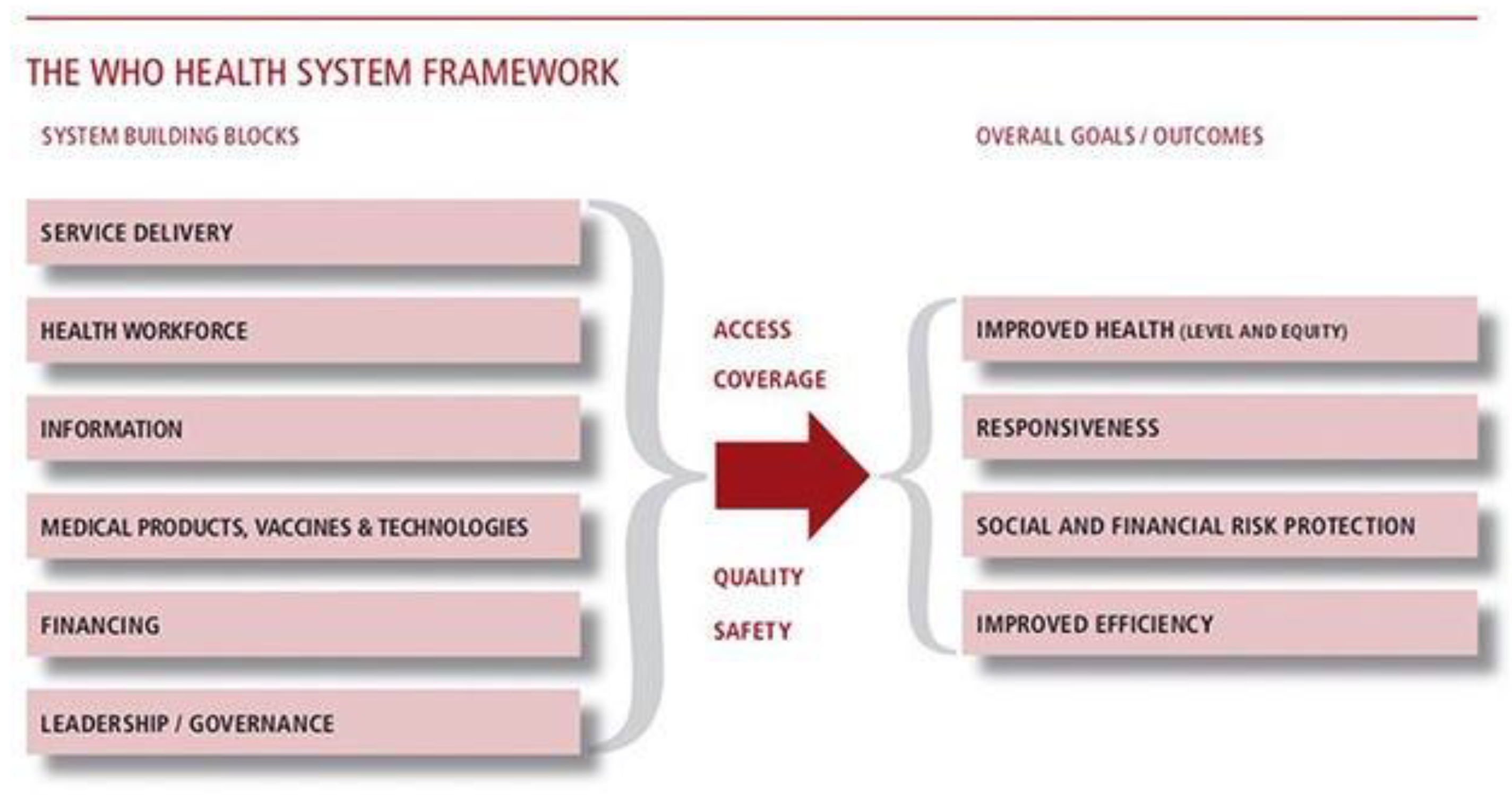
- Studies that investigate the effect of the six pillars of the health system and IPTp
- Studies investigating the outcomes of malaria in pregnancy within the health system
- Studies published in English language between 2010 and 2020
- Exclusion criteria:
- Studies outside the date range
- Studies on malaria that do not address malaria in pregnancy
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Desai, M.; Ter Kuile, F.O.; Nosten, F.; McGready, R.; Asamoa, K.; Brabin, B.; Newman, R.D. Epidemiology and burden of malaria in pregnancy. Lancet Infect. Dis. 2007, 7, 93–104. [Google Scholar] [CrossRef]
- Fried, M.; Duffy, P.E. Malaria during pregnancy. Cold Spring Harb. Perspect. Med. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Malaria Policy Advisory Committee Meeting. 2012. WHO Evidence Review Group: Intermittent Preventive Treatment of malaria in pregnancy (IPTp) with Sulfadoxine‐Pyrimethamine (SP). Available online: https://www.who.int/malaria/mpac/sep2012/iptp_sp_erg_meeting_report_july2012.pdf?ua=1 (accessed on 14 January 2020).
- Schantz-Dunn, J.; Nour, N.M. Malaria and pregnancy: A global health perspective. Rev. Obstet. Gynecol. 2009, 2, 186–192. [Google Scholar] [PubMed]
- World Health Organization. World Health Statistics 2019: Monitoring Health for the Sdgs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Parise, M.; Nahlen, B.; Menendez, C.; Steketee, R. The burden of malaria in pregnancy in malaria-endemic areas. Am. J. Trop. Med. Hyg. 2017, 64, 28–35. [Google Scholar] [CrossRef]
- Tiono, A.B.; Ouedraogo, A.; Bougouma, E.C.; Diarra, A.; Konaté, A.T.; Nébié, I.; Sirima, S.B. Placental malaria and low birth weight in pregnant women living in a rural area of Burkina Faso following the use of three preventive treatment regimens. Malar. J. 2009, 8, 224. [Google Scholar] [CrossRef]
- O’Neill, P.M.; Bray, P.G.; Hawley, S.R.; Ward, S.A.; Kevin Park, B. 4-Aminoquinolines—Past, present, and future: A chemical perspective. Pharmacol. Ther. 1998, 77, 29–58. [Google Scholar] [CrossRef]
- Pickard, A.L.; Wongsrichanalai, C.; Purfield, A.; Kamwendo, D.; Emery, K.; Zalewski, C.; Meshnick, S.R. Resistance to antimalarials in Southeast Asia and genetic polymorphisms in pfmdr1. Antimicrob. Agents Chemother. 2003, 47, 2418–2423. [Google Scholar] [CrossRef]
- Vangapandu, S.; Jain, M.; Kaur, K.; Patil, P.; Patel, S.R.; Jain, R. Recent advances in antimalarial drug development. Med. Res. Rev. 2007, 27, 65–107. [Google Scholar] [CrossRef]
- Gonçalves, L.A.; Cravo, P.; Ferreira, M.U. Emerging Plasmodium vivax resistance to chloroquine in South America: An overview. Mem. Inst. Oswaldo Cruz 2014, 109, 534–539. [Google Scholar] [CrossRef]
- Chico, R.M.; Chandramohan, D. Intermittent preventive treatment of malaria in pregnancy: At the crossroads of public health policy. Trop. Med. Int. Health. 2011, 16, 774–785. [Google Scholar] [CrossRef]
- Menéndez, C.; D’Alessandro, U.; ter Kuile, F.O. Reducing the burden of malaria in pregnancy by preventive strategies. Lancet Infect. Dis. 2007, 7, 126–135. [Google Scholar] [CrossRef]
- Muanda, F.T.; Chaabane, S.; Boukhris, T.; Santos, F.; Sheehy, O.; Perreault, S.; Bérard, A. Antimalarial drugs for preventing malaria during pregnancy and the risk of low birth weight: A systematic review and meta-analysis of randomized and quasi-randomized trials. BMC Med. 2015, 13, 193. [Google Scholar] [CrossRef] [PubMed]
- Van Eijk, A.M.; Hill, J.; Alegana, V.A.; Kirui, V.; Gething, P.W.; ter Kuile, F.O.; Snow, R.W. Coverage of malaria protection in pregnant women in sub-Saharan Africa: A synthesis and analysis of national survey data. Lancet Infect. Dis. 2011, 11, 190–207. [Google Scholar] [CrossRef]
- Feng, G.; Simpson, J.A.; Chaluluka, E.; Molyneux, M.E.; Rogerson, S.J. Decreasing burden of malaria in pregnancy in malawian women and its relationship to use of intermittent preventive therapy or bed nets. PLoS ONE 2010, 5, e12012. [Google Scholar] [CrossRef]
- Schultz, L.J.; Steketee, R.W.; Macheso, A.; Kazembe, P.; Chitsulo, L.; Wirima, J.J. The efficacy of antimalarial regimens containing sulfadoxine-pyrimethamine and/or chloroquine in preventing peripheral and placental Plasmodium falciparum infection among pregnant women in Malawi. Am. J. Trop. Med. Hyg. 1994, 51, 515–522. [Google Scholar] [CrossRef]
- World Health Organisation. 2013. WHO Policy Brief for the Implementation of Intermittent Preventive Treatment of Malaria in Pregnancy Using Sulfadoxine-Pyrimethamine (IPTp-SP). Available online: https://www.who.int/malaria/publications/atoz/iptp-sp-updated-policy-brief-24jan2014.pdf?ua=1 (accessed on 28 March 2020).
- Briand, V.; Cottrell, G.; Massougbodji, A.; Cot, M. Intermittent preventive treatment for the prevention of malaria during pregnancy in high transmission areas. Malar. J. 2007, 6, 160. [Google Scholar] [CrossRef]
- Diala, C.C.; Pennas, T.; Marin, C.; Belay, K.A. Perceptions of intermittent preventive treatment of malaria in pregnancy (IPTp) and barriers to adherence in Nasarawa and Cross River States in Nigeria. Malar. J. 2013, 12, 342. [Google Scholar] [CrossRef]
- Iliyasu, Z.; Gajida, A.U.; Galadanci, H.S.; Abubakar, I.S.; Baba, A.S.; Jibo, A.M.; Aliyu, M.H. Adherence to intermittent preventive treatment for malaria in pregnancy in urban Kano, northern Nigeria. Pathog. Glob. Health 2012, 106, 323–329. [Google Scholar] [CrossRef]
- Mbonye, A.K.; Bygbjerg, I.C.; Magnussen, P. Intermittent preventive treatment of malaria in pregnancy: A new delivery system and its effect on maternal health and pregnancy outcomes in Uganda. Bull. World Health Organ. 2008, 86, 93–100. [Google Scholar] [CrossRef]
- Onoka, C.A.; Onwujekwe, O.E.; Hanson, K.; Uzochukwu, B.S. Sub-optimal delivery of intermittent preventive treatment for malaria in pregnancy in Nigeria: Influence of provider factors. Malar. J. 2012, 11, 317. [Google Scholar] [CrossRef]
- Onyebuchi, A.K.; Lawani, L.O.; Iyoke, C.A.; Onoh, C.R.; Okeke, N.E. Adherence to intermittent preventive treatment for malaria with sulphadoxine-pyrimethamine and outcome of pregnancy among parturients in South East Nigeria. Patient Prefer. Adherence 2014, 8, 447–452. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Toure, O.A.; Kone, P.L.; Coulibaly, M.A.A.; Ako, B.A.A.; Gbessi, E.A.; Coulibaly, B.; Koffi, D.; Beourou, S.; Soumahoro, A.; Bassinka, I.; et al. Coverage and efficacy of intermittent preventive treatment with sulphadoxine pyrimethamine against malaria in pregnancy in Côte d’Ivoire five years after its implementation. Parasites Vectors 2014, 7, 495. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. World Malaria Report 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- WHO. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action. 2007. Available online: https://www.who.int/healthsystems/strategy/everybodys_business.pdf (accessed on 14 April 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analysis: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Henry, M.; Florey, L.; Youll, S.; Gutman, J.R. An analysis of country adoption and implementation of the 2012 WHO recommendations for intermittent preventive treatment for pregnant women in sub-Saharan Africa. Malar. J. 2018, 17, 364. [Google Scholar] [CrossRef] [PubMed]
- Popay, J.; Roberts, H.; Sowden, A.; Rodgers, M.; Petticrew, M.; Arai, L.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. Prod. ESRC Method. Progr. 2006, 1, b92. [Google Scholar] [CrossRef]
- Buh, A.; Kota, K.; Bishwajit, G.; Yaya, S. Prevalence and associated factors of taking intermittent preventive treatment in pregnancy in Sierra Leone. Trop. Med. Infect. Dis. 2019, 4, 32. [Google Scholar] [CrossRef]
- Rassi, C.; Graham, K.; Mufubenga, P.; King, R.; Meier, J.; Gudoi, S.S. Assessing supply-side barriers to uptake of intermittent preventive treatment for malaria in pregnancy: A qualitative study and document and record review in two regions of Uganda. Malar. J. 2016, 15, 341. [Google Scholar] [CrossRef]
- Okello, G.; Gerrets, R.; Zakayo, S.; Molyneux, S.; Jones, C. “Every day they keep adding new tools but they don’t take any away”: Producing indicators for intermittent preventive treatment for malaria in pregnancy (IPTp) from routine data in Kenya. PLoS ONE 2018, 13, e0189699. [Google Scholar] [CrossRef]
- Ayanore, M.A.; Amuna, N.; Aviisah, M.; Awolu, A.; Kipo-Sunyehzi, D.D.; Mogre, V.; Gyapong, M. Towards resilient health systems in sub-saharan africa: A systematic review of the english language literature on health workforce, surveillance, and health governance issues for health systems strengthening. Ann. Glob. Health 2019, 85, 113. [Google Scholar] [CrossRef]
- Konje, E.T.; Magoma, M.T.N.; Hatfield, J.; Kuhn, S.; Sauve, R.S.; Dewey, D. Missed opportunities in antenatal care for improving the health of pregnant women and newborns in Geita district, Northwest Tanzania. BMC Pregnancy Childbirth 2018, 18, 394. [Google Scholar] [CrossRef]
- Maheu-Giroux, M.; Castro, M.C. Factors affecting providers’ delivery of intermittent preventive treatment for malaria in pregnancy: A five-country analysis of national service provision assessment surveys. Malar. J. 2014, 13, 440. [Google Scholar] [CrossRef] [PubMed]
- Azizi, S.C. Uptake of intermittent preventive treatment for malaria during pregnancy with Sulphadoxine-Pyrimethamine in Malawi after adoption of updated World Health Organization policy: An analysis of demographic and health survey 2015–2016. BMC Public Health 2020, 20, 335. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.; Kayentao, K.; Bruce, J.; Diawara, S.I.; Abathina, A.; Haiballa, A.A.; Hill, J. Prevention of Malaria in Pregnancy with Intermittent Preventive Treatment and Insecticide Treated Nets in Mali: A Quantitative Health Systems Effectiveness Analysis. PLoS ONE 2013, 8, e67520. [Google Scholar] [CrossRef]
- Van De Pas, R.; Kolie, D.; Delamou, A.; Van Damme, W. Health workforce development and retention in Guinea: A policy analysis post-Ebola. Hum. Resour. Health 2019, 17, 1–12. [Google Scholar] [CrossRef]
- Yaya, S.; Uthman, O.A.; Amouzou, A.; Bishwajit, G. Use of intermittent preventive treatment among pregnant women in sub-Saharan Africa: Evidence from malaria indicator surveys. Trop. Med. Infect. Dis. 2018, 3, 18. [Google Scholar] [CrossRef]
- Hill, J.; Hoyt, J.; Achieng, F.; Ouma, P.; Anne, L.; Kariuki, S.; Webster, J. User and Provider Acceptability of Intermittent Screening and Treatment and Intermittent Preventive Treatment with Dihydroartemisinin-Piperaquine to Prevent Malaria in Pregnancy in Western Kenya. PLoS ONE 2016, 11, e0150259. [Google Scholar] [CrossRef] [PubMed]
- Dellicour, S.; Hill, J.; Bruce, J.; Ouma, P.; Marwanga, D.; Otieno, P.; Webster, J. Effectiveness of the delivery of interventions to prevent malaria in pregnancy in Kenya. Malar. J. 2016, 15, 221. [Google Scholar] [CrossRef] [PubMed]
- Mubyazi, G.M.; Magnussen, P.; Byskov, J.; Bloch, P. Feasibility and coverage of implementing intermittent preventive treatment of malaria in pregnant women contacting private or public clinics in Tanzania: Experience-based viewpoints of health managers in Mkuranga and Mufindi districts. BMC Health Serv. Res. 2013, 13, 1. [Google Scholar] [CrossRef]
- Aregbeshola, B.S.; Khan, S.M. Out-of-pocket payments, catastrophic health expenditure and poverty among households in Nigeria 2010. Int. J. Health Policy Manag. 2018, 7, 798–806. [Google Scholar] [CrossRef]
- Awantang, G.N.; Babalola, S.O.; Koenker, H.; Fox, K.A.; Toso, M.; Lewicky, N. Malaria-related ideational factors and other correlates associated with intermittent preventive treatment among pregnant women in Madagascar. Malar. J. 2018, 17, 176. [Google Scholar] [CrossRef]
- Arnaldo, P.; Cambe, M.I.; Magaço, A.; Chicumbe, S.; Rovira-Vallbona, E.; Rosanas-Urgell, A.; Enosse, S.M. Access to and use of preventive intermittent treatment for Malaria during pregnancy: A qualitative study in the Chókwè district, Southern Mozambique. PLoS ONE 2019, 14, e0203740. [Google Scholar] [CrossRef]
- Ameh, S.; Owoaje, E.; Oyo-Ita, A.; Kabiru, C.W.; Akpet, O.E.O.; Etokidem, A.; Ekpenyong, N. Barriers to and determinants of the use of intermittent preventive treatment of malaria in pregnancy in Cross River State, Nigeria: A cross-sectional study. BMC Pregnancy Childbirth 2016, 16, 99. [Google Scholar] [CrossRef] [PubMed]
- Klootwijk, L.; Chirwa, A.E.; Kabaghe, A.N.; Van Vugt, M. Challenges affecting prompt access to adequate uncomplicated malaria case management in children in rural primary health facilities in Chikhwawa Malawi. BMC Health Serv. Res. 2019, 19, 735. [Google Scholar] [CrossRef] [PubMed]
- Oleribe, O.O.; Momoh, J.; Uzochukwu, B.S.C.; Mbofana, F.; Adebiyi, A.; Barbera, T.; Taylor-Robinson, S.D. Identifying key challenges facing healthcare systems in Africa and potential solutions. Int. J. Gen. Med. 2019, 12, 395–403. [Google Scholar] [CrossRef]
- Rassi, C.; Graham, K.; King, R.; Ssekitooleko, J.; Mufubenga, P.; Gudoi, S.S. Assessing demand-side barriers to_uptake of_intermittent preventive treatment for_malaria in_pregnancy: A qualitative study in_two regions of_Uganda. Malar. J. 2016, 15, 530. [Google Scholar] [CrossRef]
- Hill, J.; Dellicour, S.; Bruce, J.; Ouma, P.; Smedley, J.; Otieno, P.; Ombock, M.; Kariuki, S.; Desai, M.; Hamel, M.J.; et al. Effectiveness of Antenatal Clinics to Deliver Intermittent Preventive Treatment and Insecticide Treated Nets for the Control of Malaria in Pregnancy in Kenya. PLoS ONE 2013, 8, e64913. [Google Scholar] [CrossRef] [PubMed]
- Arnaldo, P.; Rovira-Vallbona, E.; Langa, J.S.; Salvador, C.; Guetens, P.; Chiheb, D.; Rosanas-Urgell, A. Uptake of intermittent preventive treatment and pregnancy outcomes: Health facilities and community surveys in Chókwè district, southern Mozambique. Malar. J. 2018, 17. [Google Scholar] [CrossRef]
- Mubyazi, G.M.; Bloch, P. Psychosocial, behavioural and health system barriers to delivery and uptake of intermittent preventive treatment of malaria in pregnancy in Tanzania—Viewpoints of service providers in Mkuranga and Mufindi districts. BMC Health Serv. Res. 2014, 14, 15. [Google Scholar] [CrossRef]
- Okethwangu, D.; Opigo, J.; Atugonza, S.; Kizza, C.T.; Nabatanzi, M.; Biribawa, C.; Ario, A.R. Factors associated with uptake of optimal doses of intermittent preventive treatment for malaria among pregnant women in Uganda: Analysis of data from the Uganda Demographic and Health Survey, 2016. Malar. J. 2019, 18, 250. [Google Scholar] [CrossRef]
- Oppong, F.B.; Gyaase, S.; Zandoh, C.; Nettey, O.E.A.; Amenga-Etego, S.; Anane, E.A.; Asante, K.P. Intermittent preventive treatment of pregnant women in Kintampo area of Ghana with sulphadoxine-pyrimethamine (SP): Trends spanning 2011 and 2015. BMJ Open 2019, 9, e027946. [Google Scholar] [CrossRef]
- Henriksson, D.K.; Fredriksson, M.; Waiswa, P.; Selling, K.; Peterson, S.S. Bottleneck analysis at district level to illustrate gaps within the district health system in Uganda. Glob. Health Action 2017, 10, 1327256. [Google Scholar] [CrossRef]
- Mubyazi, G.M.; Bloch, P.; Byskov, J.; Magnussen, P.; Bygbjerg, I.C.; Hansen, K.S. Supply-related drivers of staff motivation for providing intermittent preventive treatment of malaria during pregnancy in Tanzania: Evidence from two rural districts. Malar. J. 2012, 11, 48. [Google Scholar] [CrossRef]
- Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. NIH National Heart, Lung and Blood Institute. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 17 May 2020).
- Lorenc, T.; Petticrew, M.; Whitehead, M.; Neary, D.; Clayton, S.; Wright, K.; Thomson, H.; Cummins, S.; Sowden, A.; Renton, A. Crime, Fear of Crime and Mental Health: Synthesis of Theory and Systematic Reviews of Interventions and Qualitative Evidence; NIHR Journals Library: Southampton, UK, 2014; (Public Health Research, No. 2.2.) Appendix 5, Quality assessment for the systematic review of qualitative evidence. Available online: https://www.ncbi.nlm.nih.gov/books/NBK262835/ (accessed on 28 March 2020).
- Hill, J.; Kayentao, K.; Touré, M.; Diarwara, S.; Bruce, J.; Smedley, J.; Webster, J. Effectiveness of antenatal clinics to deliver intermittent preventive treatment and insecticide treated nets for the control of malaria in pregnancy in Mali: A household survey. PLoS ONE 2014, 9, e92102. [Google Scholar] [CrossRef] [PubMed]
- Kibusi, S.M.; Kimunai, E.; Hines, C.S. Predictors for uptake of intermittent preventive treatment of malaria in pregnancy (IPTp) in Tanzania. BMC Public Health. 2015, 15, 540. [Google Scholar] [CrossRef] [PubMed]
- Thiam, S.; Kimotho, V.; Gatonga, P. Why are IPTp coverage targets so elusive in sub-Saharan Africa? A systematic review of health system barriers. Malar. J. 2013, 12, 353. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.C.; Harvey, S.A.; Diarra, H.; Hurley, E.A.; Rao, N.; Diop, S.; Doumbia, S. “There is no free here, you have to_pay”: Actual and_perceived costs as_barriers to_intermittent preventive treatment of_malaria in_pregnancy in_Mali. Malar. J. 2016, 15, 158. [Google Scholar] [CrossRef]
- Mbengue, M.A.S.; Bei, A.K.; Mboup, A.; Ahouidi, A.; Sarr, M.; Mboup, S.; Gaye, O. Factors influencing the use of malaria prevention strategies by women in Senegal: A cross-sectional study. Malar. J. 2017, 16, 470. [Google Scholar] [CrossRef]
- Kibusi, S.M.; Sunguya, B.F.; Kimunai, E.; Hines, C.S. Health insurance is important in improving maternal health service utilization in Tanzania—Analysis of the 2011/2012 Tanzania HIV/AIDS and malaria indicator survey. BMC Health Serv. Res. 2018, 18, 112. [Google Scholar] [CrossRef]
- Orobaton, N.; Austin, A.M.; Abegunde, D.; Ibrahim, M.; Mohammed, Z.; Abdul-Azeez, J.; Beal, K. Scaling-up the use of sulfadoxine-pyrimethamine for the preventive treatment of malaria in pregnancy: Results and lessons on scalability, costs and programme impact from three local government areas in Sokoto State, Nigeria. Malar. J. 2016, 15, 1–24. [Google Scholar] [CrossRef]
- Crawley, J.; Hill, J.; Yartey, J.; Robalo, M.; Serufilira, A.; Ba-Nguz, A.; Roman, E.; Palmer, A.; Asamoa, K.; Steketee, R. From evidence to action? Challenges to policy change and programme delivery for malaria in pregnancy. Lancet Infect. Dis. 2007, 7, 145–155. [Google Scholar] [CrossRef]
- Agarwal, K.; Alonso, P.; Chico, R.M.; Coleman, J.; Dellicour, S.; Hill, J.; Majeres-Lugand, M.; Mangiaterra, V.; Menéndez, C.; Mitchell, K.; et al. Global Call to Action to scale-up coverage of intermittent preventive treatment of malaria in pregnancy: Seminar report. Malar. J. 2015, 14, 206. [Google Scholar] [CrossRef] [PubMed]
- Kirigia, J.M.; Nganda, B.M.; Mwikisa, C.N.; Cardoso, B. Effects of global financial crisis on funding for health development in nineteen countries of the WHO African Region. BMC Int. Health Hum. Rights 2011, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Kates, R.W.; Dasgupta, P. African poverty: A grand challenge for sustainability science. Proc. Natl. Acad. Sci. USA 2007, 104, 16747–16750. [Google Scholar] [CrossRef] [PubMed]
- Dukes, M.N.G. Declaration of Alma-Ata. Lancet 1978, 312, 1256. [Google Scholar] [CrossRef]
- Chabot, J. The Bamako Initiative. Lancet 1988, 332, 1366–1367. [Google Scholar] [CrossRef]
- Donfouet, H.P.; Mahieu, P. Community-based health insurance and social capital: A review. Health Econ. Rev. 2012, 2, 5. [Google Scholar] [CrossRef]
- Mekonen, A.M.; Gebregziabher, M.G.; Teferra, A.S. The effect of community based health insurance on catastrophic health expenditure in Northeast Ethiopia: A cross sectional study. PLoS ONE 2018, 13, e0205972. [Google Scholar] [CrossRef]
- Hill, J.; Hoyt, J.; Van Eijk, A.M.; D’Mello-Guyett, L.; Ter Kuile, F.O.; Steketee, R.; Smith, H.; Webster, J. Factors Affecting the Delivery, Access, and Use of Interventions to Prevent Malaria in Pregnancy in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. PLoS Med. 2013, 10, e1001488. [Google Scholar] [CrossRef]
- Lund, S.; Nielsen, B.B.; Hemed, M.; Boas, I.M.; Said, A.; Said, K.; Makungu, M.H. Mobile phones improve antenatal care attendance in Zanzibar: A cluster randomized controlled trial. BMC Pregnancy Childbirth 2014, 14, 29. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Year | Country | Setting |
|---|---|---|---|
| Ameh [31] | 2016 | Nigeria | Cross-sectional study of 400 ANC attendees to identify barriers to and determinants of IPTp uptake |
| Arnaldo [32] | 2019 | Mozambique | Qualitative study on access to and use of preventive intermittent treatment for Malaria during pregnancy |
| Arnaldo [33] | 2018 | Mozambique | Community and facility-based surveys of 1141 mothers to assess IPTp-SP coverage and factors associated with low uptake |
| Awantang [34] | 2018 | Madagascar | Cross-sectional household survey of mothers with children under the age of 2 years on factors associated with IPTp uptake |
| Azizi [35] | 2020 | Malawi | Analysis of 2015–16 DHS dataset to assess uptake of IPTp in Malawi after adoption of updated WHO IPTp-SP policy |
| Buh [36] | 2019 | Sierra Leone | Secondary data analysis of the Multiple Indicator Cluster Survey (MICS 5) among reproductive age women |
| Dellicour [37] | 2016 | Kenya | Cross-sectional facility survey on effectiveness of the delivery of interventions to prevent malaria in pregnancy |
| Diala [19] | 2013 | Nigeria | Qualitative study on perceptions of IPTp and barriers to adherence |
| Henriksson [38] | 2017 | Uganda | Secondary data analysis to identify bottlenecks in service delivery within the district health system |
| Henry [28] | 2018 | 17 countries in sub-Saharan Africa | Country analysis of implementation of updated WHO policy |
| Hill [39] | 2013 | Kenya | Secondary analysis of household survey data to evaluate the effectiveness of antenatal clinics to deliver IPTp and ITNs |
| Hill [40] | 2014 | Mali | Secondary analysis of household survey data to evaluate the effectiveness of antenatal clinics to deliver 2 doses of IPTp and ITNs |
| Hill [41] | 2016 | Kenya | Qualitative data on user and provider acceptability within RCT comparing ISTp-DP and IPTp-DP with IPTp-SP |
| Iliyasu [20] | 2012 | Nigeria | Cross-sectional study of 239 ANC attendees on IPT adherence |
| Kibusi [30] | 2015 | Tanzania | Analysis of 2011–2012 HIV and Malaria Indicators Survey of 1616 women to identify factors responsible for IPTp uptake |
| Kibusi [42] | 2018 | Tanzania | Analysis of 2011–2012 HIV and Malaria Indicators Survey to examine the role of health insurance coverage in utilization of maternal health services |
| Klein [43] | 2016 | Mali | Qualitative study of pregnant women, husbands, mothers-in-law and health workers in two rural regions |
| Konje [44] | 2018 | Tanzania | Mixed method population-based study on ANC availability, utilization, challenges and barriers among pregnant women and community health workers in rural areas |
| Maheu-Giroux [45] | 2014 | Kenya, Namibia, Rwanda, Tanzania, Uganda | Secondary data analysis of service provision assessment surveys over a five-year period to explore factors affecting provider’s delivery of IPTp during ANC consultations |
| Mbengue [46] | 2017 | Senegal | Secondary analysis of 4616 women from 2013–2014 Demographic and Health Survey to assess factors associated with optimal IPTp and ITN uptake |
| Mubyazi [47] | 2014 | Tanzania | Mixed method study among ANC providers in two rural districts on psychosocial, behavioural and health system barriers to IPTp delivery and uptake |
| Mubyazi [48] | 2013 | Tanzania | Qualitative study among health managers in public and private clinics on IPTp feasibility, acceptability and challenges |
| Mubyazi [49] | 2012 | Tanzania | Qualitative study on the drivers of motivation and performance among health workers providing IPTp in public and private facilities |
| Okello [50] | 2018 | Kenya | Qualitative study among health workers and sub-country managers |
| Okethwangu [51] | 2019 | Uganda | Secondary data analysis from Uganda Demographic and Health Survey on factors associated with uptake of optimal IPTp doses |
| Onoka [22] | 2012 | Nigeria | Cross-sectional study among healthcare providers |
| Onyebuchi [23] | 2014 | Nigeria | Prospective descriptive study of 516 pregnant women from their ANC booking till delivery |
| Oppong [52] | 2019 | Ghana | 5-year retrospective data analysis of a district within a Health and Demographic Surveillance System area |
| Orobaton [53] | 2016 | Nigeria | Community intervention study on IPTp delivery strategies to assess scalability, costs and program impact |
| Rassi [54] | 2016 | Uganda | Qualitative study of district health officials, health workers, pregnant women and opinion leaders (supply side) |
| Rassi [55] | 2016 | Uganda | Qualitative study of district health officials, health workers, pregnant women and opinion leaders (demand side) |
| Toure [24] | 2014 | Cote D’Ivoire | Cross-sectional survey of 1317 delivered women |
| Yaya [56] | 2018 | Burkina Faso, Ghana, Mali, Malawi, Kenya, Nigeria, Sierra Leone, and Uganda | Cross-sectional data on 18,603 women from Malaria Indicator Surveys |
| Webster [57] | 2013 | Mali | Cross-sectional study of 780 women to evaluate health system effectiveness of ANC for the delivery of a dose of IPTp and an ITN |
| Sub-Saharan Africa Region | Number of Publications |
|---|---|
| East Africa | 19 |
| West Africa | 12 |
| Southern Africa | 0 |
| Trans-regional publications | 3 |
| Total | 34 |
| Health System Pillar | Country | Barrier to IPTp Implementation |
|---|---|---|
| Service delivery | Kenya, Nigeria, Tanzania, Mali, Senegal | Ambiguity of IPTp policy and administration [33,53], poor supervision [47], poor quality of service [35,56], long distance [35], poor health worker adherence to IPTp guidelines including gestational age and DOT [38,42,60], poor provider knowledge of IPTp protocol [20,23,38], long waiting time [35], water shortages [43], SP safety concerns [38,53], informal health center regulations [35], complex guidelines [38], late ANC registration [53,60,61,62], insufficient time for ANC counseling [46] |
| Health workforce | Mozambique, Uganda, Kenya, Tanzania | Human resource shortages [33,35,52,56] understaffing [43,57], poor supervision [57], health worker job dissatisfaction [57] |
| Health information | Kenya | Ambiguity of IPTp data recording and reporting guidelines [33], redundant tools [33] |
| Medical products, vaccines and technologies | Kenya, Nigeria, Tanzania, Namibia, Rwanda, Uganda | Drug stock-out [20,33,35,36,47], absent or inadequate supply of free SP for IPTp to private facilities [43] |
| Healthcare financing | Mali, Tanzania, Ghana, Senegal | Out-of-pocket payment for healthcare [35,38], hidden costs [35], poverty [35,55,62], ambiguity on free and fee-based services at health facility [53,63], delayed government funding for health centers [43] |
| Leadership and governance | Mali, Mozambique | Inconsistent policy implementation [63], conflicting guidelines [53], poor community awareness of IPTp [52] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olaleye, A.O.; Walker, O. Impact of Health Systems on the Implementation of Intermittent Preventive Treatment for Malaria in Pregnancy in Sub-Saharan Africa: A Narrative Synthesis. Trop. Med. Infect. Dis. 2020, 5, 134. https://doi.org/10.3390/tropicalmed5030134
Olaleye AO, Walker O. Impact of Health Systems on the Implementation of Intermittent Preventive Treatment for Malaria in Pregnancy in Sub-Saharan Africa: A Narrative Synthesis. Tropical Medicine and Infectious Disease. 2020; 5(3):134. https://doi.org/10.3390/tropicalmed5030134
Chicago/Turabian StyleOlaleye, Atinuke O., and Oladapo Walker. 2020. "Impact of Health Systems on the Implementation of Intermittent Preventive Treatment for Malaria in Pregnancy in Sub-Saharan Africa: A Narrative Synthesis" Tropical Medicine and Infectious Disease 5, no. 3: 134. https://doi.org/10.3390/tropicalmed5030134
APA StyleOlaleye, A. O., & Walker, O. (2020). Impact of Health Systems on the Implementation of Intermittent Preventive Treatment for Malaria in Pregnancy in Sub-Saharan Africa: A Narrative Synthesis. Tropical Medicine and Infectious Disease, 5(3), 134. https://doi.org/10.3390/tropicalmed5030134