Objective and Subjective Evaluation of Saccadic Eye Movements in Healthy Children and Children with Neurodevelopmental Disorders: A Pilot Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
- Control group (CG): included 15 healthy children aged 7 to 12 years old. The inclusion criteria for this group were emmetropic ametropic (corrected with spectacles) or emmetropic children achieving a corrected distance visual acuity (CDVA) of 0.00 logMAR (20/20 Snellen) or better. Exclusion criteria were any ocular or systemic disease active at the time of examination as well as any previous ocular surgery. This group was examined by the neuropediatrician to rule out the presence of any neurodevelopmental disorder.
- Group of children diagnosed with a neurodevelopmental disorder (NDDG): included 17 children aged 6 to 10 years. Specifically, there were 7 children with dyslexia (41.1%), 6 (35.3%) with developmental coordination disorder (DCD) and 4 (23.5%) with attention deficit disorder (ADHD). A speech therapist, a psychologist and a pediatrician evaluated all of these children and made a diagnosis of NDD according to the DSM-5 criteria [15]. According to previous scientific studies, oculomotor abnormalities are expected to be present in these children [10,11,12,13,14]. No comorbidity of neurodevelopmental disorders was present in any case. The selection of these disorders was based on the type of patients attending our clinic, these disorders being the most commonly explored. Likewise, the evaluation of oculomotricity is more feasible in these children compared to other NDDs, most of them being cooperative patients.
2.2. Examination Protocol
- Ability. Can the individual take the assigned test?
- Accuracy. What is the quality of execution?
- The level of head movement the patient uses to perform the task. Is head movement spontaneous when doing the task?
- The level of body movement used.
2.3. Statistical Analysis
3. Results
3.1. General Clinical Data
3.2. Oculomotor Analysis
3.3. Correlation between Subjective and Objective Oculomotor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dodge, R. Five types of eye movement in the horizontal meridian plane of the field of regard. Am. J. Physiol. Content 1903, 8, 307–329. [Google Scholar] [CrossRef]
- Keller, E.L.; Missal, M. Shared brainstem pathways for saccades and smooth-pursuit eye movements. Ann. N. Acad. Sci. 2003, 1004, 29–39. [Google Scholar] [CrossRef]
- Balser, N.; Lorey, B.; Pilgramm, S.; Naumann, T.; Kindermann, S.; Stark, R.; Zentgraf, K.; Williams, A.M.; Munzert, J. The influence of expertise on brain activation of the action observation network during anticipation of tennis and volleyball serves. Front. Hum. Neurosci. 2014, 8, 568. [Google Scholar] [CrossRef]
- Doettl, S.M.; McCaslin, D.L. Oculomotor assessment in children. Semin. Hear. 2018, 39, 275–287. [Google Scholar]
- Anderson, T.J.; MacAskill, M.R. Eye movements in patients with neurodegenerative disorders. Nat. Rev. Neurol. 2013, 9, 74–85. [Google Scholar] [CrossRef]
- Seassau, M.; Bucci, M.P. Reading and visual search: A developmental study in normal children. PLoS ONE 2013, 8, e70261. [Google Scholar]
- Land, M.F. Eye movements and the control of actions in everyday life. Prog. Retin. Eye Res. 2006, 25, 296–324. [Google Scholar] [CrossRef]
- Apicella, F.; Costanzo, V.; Purpura, G. Are early visual behavior impairments involved in the onset of autism spectrum disorders? Insights for early diagnosis and intervention. Eur. J. Pediatr. 2020, 179, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Gil-Casas, A.; Piñero, D.P.; Molina-Martin, A. Binocular, accommodative and oculomotor alterations in multiple sclerosis: A review. Semin. Ophthalmol. 2020, 35, 103–115. [Google Scholar] [CrossRef]
- Bilbao, C.; Piñero, D.P. Distribution of visual and oculomotor alterations in a clinical population of children with and without neurodevelopmental disorders. Brain Sci. 2021, 11, 351. [Google Scholar] [CrossRef] [PubMed]
- Bilbao, C.; Piñero, D.P. Clinical characterization of oculomotricity in children with and without specific learning disorders. Brain Sci. 2020, 10, 836. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.P.; Brémond-Gignac, D.; Kapoula, Z. Poor binocular coordination of saccades in dyslexic children. Graefe’s Arch. Clin. Exp. Ophthalmol. 2008, 246, 417–428. [Google Scholar] [CrossRef]
- Mahone, E.M.; Mostofsky, S.H.; Lasker, A.G.; Zee, D.; Denckla, M.B. Oculomotor anomalies in attention-deficit/hyperactivity disorder: Evidence for deficits in response preparation and inhibition. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 749–756. [Google Scholar] [CrossRef]
- Sumner, E.; Hutton, S.B.; Juhn, G.; Hill, E.L. Oculomotor atypicalities developmental coordination disorder. Dev. Sci. 2018, 21, e12501. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Maples, W.C.; Atchley, J.; Ficklin, T. Northeastern State University College of Optometry’s oculomotor norms. J. Behav. Optom. 1992, 3, 143–150. [Google Scholar]
- Maples, W.C.; Ficklin, T.W. Interrater and test-retest reliability of pursuits and saccades. J. Am. Optom. Assoc. 1988, 59, 549–552. [Google Scholar] [PubMed]
- Bilbao, C.; Piñero, D.P. Diagnosis of oculomotor anomalies in children with learning disorders. Clin. Exp. Optom. 2020, 103, 597–609. [Google Scholar] [CrossRef]
- Loe, I.M.; Feldman, H.M.; Yasui, E.; Luna, B. Oculomotor performance identifies underlying cognitive deficits in attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 431–440. [Google Scholar] [CrossRef]
- Molina, R.; Redondo, B.; Vera, J.; García, J.A.; Muñoz-Hoyos, A.; Jiménez, R. Children with attention-deficit/hyperactivity disorder show an altered eye movement pattern during reading. Optom. Vis. Sci. 2020, 97, 265–274. [Google Scholar] [CrossRef]
- Ayton, L.N.; Abel, L.A.; Fricke, T.R.; McBrien, N.A. Developmental eye movement test: What is it really measuring? Optom. Vis. Sci. 2009, 86, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.; Redman-Bentley, D.; Remick-Waltman, K.; Armstrong, D.C. Differences in oculomotor function between children with sensory processing disorder and typical development. Optom. Vis. Sci. 2019, 96, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Tiadi, A.; Seassau, M.; Gérard, C.; Bucci, P. Differences between dyslexic and non-dyslexic children in the performance of phonological visual-auditory recognition tasks: An eye-tracking study. PLoS ONE 2016, 11, e0159190. [Google Scholar] [CrossRef]
- Bucci, M.P.; Mélithe, D.; Ajrezo, L.; Bui-Quoc, E.; Gérard, C.L. The influence of oculomotor tasks on postural control in dyslexic children. Front. Hum. Neurosci. 2014, 8, 981. [Google Scholar] [CrossRef] [PubMed]
- Hakvoort Schwerdtfeger, R.M.; Alahyane, N.; Brien, D.C.; Coe, B.C.; Stroman, P.W.; Munoz, D.P. Preparatory neural networks are impaired in adults with attention-deficit/hyperactivity disorder during the antisaccade task. Neuroimage Clin. 2012, 2, 63–78. [Google Scholar] [CrossRef]
- Jainta, S.; Kapoula, Z. Dyslexic children are confronted with unstable binocular fixation while reading. PLoS ONE 2011, 6, e18694. [Google Scholar] [CrossRef]
- Vagge, A.; Cavanna, M.; Traverso, C.E.; Iester, M. Evaluation of ocular movements in patients with dyslexia. Ann. Dyslexia 2015, 65, 24–32. [Google Scholar] [CrossRef]
- Kraljević, J.K.; Palmović, M. Spatial and temporal measurements of eye movement in children with dyslexia. Coll. Antropol. 2011, 35, 191–198. [Google Scholar]
- Stine, C.D.; Arterburn, M.R.; Stern, N.S. Vision and sports: A review of the literature. J. Am. Optom. Assoc. 1982, 53, 627–633. [Google Scholar]
- Aksum, K.M.; Magnaguagno, L.; Bjørndal, C.T.; Jordet, G. What do football players look at? An eye-tracking analysis of the visual fixations of players in 11v11 elite football match play. Front. Psychol. 2020, 11, 562995. [Google Scholar] [CrossRef] [PubMed]
- Hitzeman, S.A.; Beckerman, S.A. What the literature says about sports vision. Optom. Clin. 1993, 3, 145–169. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Performance Area | Evaluation Procedure | Scoring System |
|---|---|---|
| Ability | Patient’s ability of performing 5 cycles of change of fixation between the two stimuli presented | 1 point: 1 cycle or no ability 2 points: 2 cycles 3 points: 3 cycles 4 points: 4 cycles 5 points: 5 cycles |
| Accuracy | Patient’s ability of performing 5 cycles of change of fixation without correcting refixations | 1 point: significant hyper- or hypometric movements 2 points: large to moderate hyper- or hypometric movements 3 points: slight hyper or hypometric movements but constant 4 points: slight hyper or hypometric movements but intermittent 5 points: no correcting refixations |
| Head/body movement associated | Patient’s ability of performing 5 cycles of change of fixation without head or body movements | 1 point: 1 cycle or no ability 2 points: 2 cycles 3 points: 3 cycles 4 points: 4 cycles 5 points: 5 cycles |
| Mean (SD) Median (Range) | CG (15 Children) | NDDG (17 Children) | p-Value |
|---|---|---|---|
| Age (years) | 9.3 (1.6) 10.0 (7.0 to 12.0) | 8.2 (1.4) 8.0 (6.0 to 10.0) | 0.069 |
| Sphere RE (D) | 0.40 (1.30) 0.00 (0.00 to 5.00) | 0.03 (0.12) 0.00 (0.00 to 0.50) | 0.710 |
| Cylinder RE (D) | −0.25 (0.78) 0.00 (−3.00 to 0.00) | −0.01 (0.06) 0.00 (−0.25 to 0.00) | 0.710 |
| Sphere LE (D) | 0.43 (1.32) 0.00 (0.00 to 5.00) | 0.03 (0.12) 0.00 (0.00 to 0.50) | 0.710 |
| Cylinder LE (D) | −0.23 (0.68) 0.00 (−2.50 to 0.00) | 0.00 (0.00) 0.00 (0.00 to 0.00) | 0.526 |
| LogMAR CDVA RE | 0.01 (0.03) 0.00 (0.00 to 0.10) | 0.00 (0.00) 0.00 (0.00 to 0.00) | 0.766 |
| LogMAR CDVA LE | 0.01 (0.03) 0.00 (0.00 to 0.10) | 0.00 (0.00) 0.00 (0.00 to 0.00) | 0.766 |
| Phoria at distance (prism diopters) | −3.07 (3.59) −4.00 (−10.00 to 3.00) | −3.65 (4.14) −2.00 (−10.00 to 0.00) | 0.823 |
| Phoria at near (prism diopters) | −4.13 (5.21) −6.00 (−12.00 to 6.00) | −5.18 (4.95) −6.00 (−12.00 to 0.00) | 0.576 |
| NPC (cm) | 7.07 (5.20) 6.00 (0.00 to 15.00) | 8.12 (5.74) 8.00 (0.00 to 20.00) | 0.628 |
| Mean (SD) Median (Range) | CG (15 Children) | NDDG (17 Children) | p-Value |
|---|---|---|---|
| NSUCO test | |||
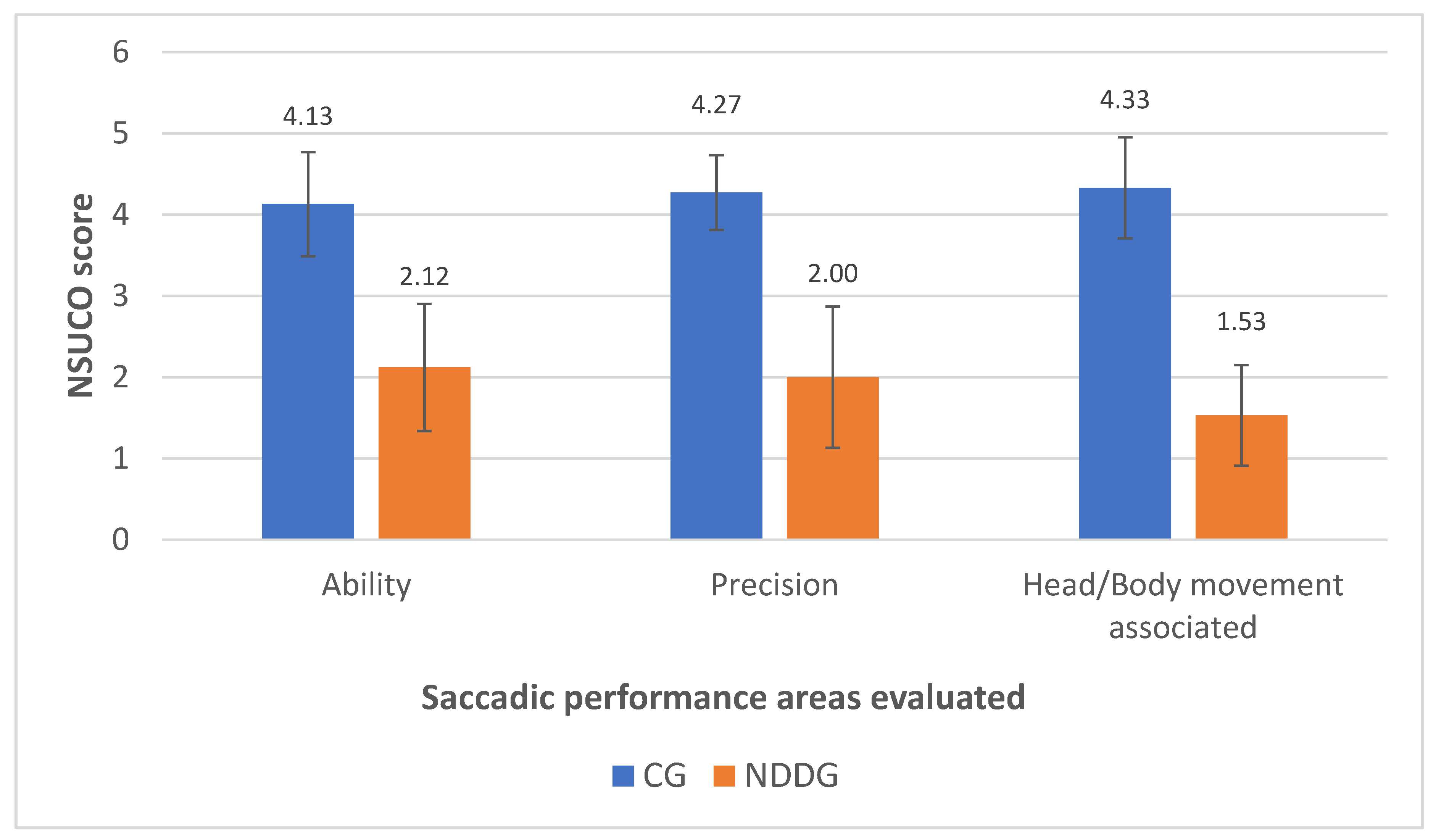
| Saccadic Ability | 4.13 (0.64) 4.00 (3.00 to 5.00) | 2.12 (0.78) 2.00 (1.00 to 3.00) | <0.001 |
| Saccadic Precision | 4.27 (0.46) 4.00 (4.00 to 5.00) | 2.00 (0.87) 2.00 (1.00 to 3.00) | <0.001 |
| Body and head movements associated | 4.33 (0.62) 4.00 (3.00 to 5.00) | 1.53 (0.62) 1.00 (1.00 to 3.00) | <0.001 |
| Eye tracker analysis | |||
| Number of cycles 0.5 s | 18.73 (6.65) 16.00 (13.00 to 37.00) | 17.38 (4.01) 15.00 (14.00 to 25.00) | 0.455 |
| 1 s | 14.07 (1.98) 15.00 (9.00 to 16.00) | 14.36 (1.34) 15.00 (11.00 to 15.00) | 0.910 |
| % of regressions 0.5 s | 31.12 (9.91) 29.00 (15.00 to 51.40) | 32.19 (5.64) 31.05 (23.00 to 40.30) | 0.526 |
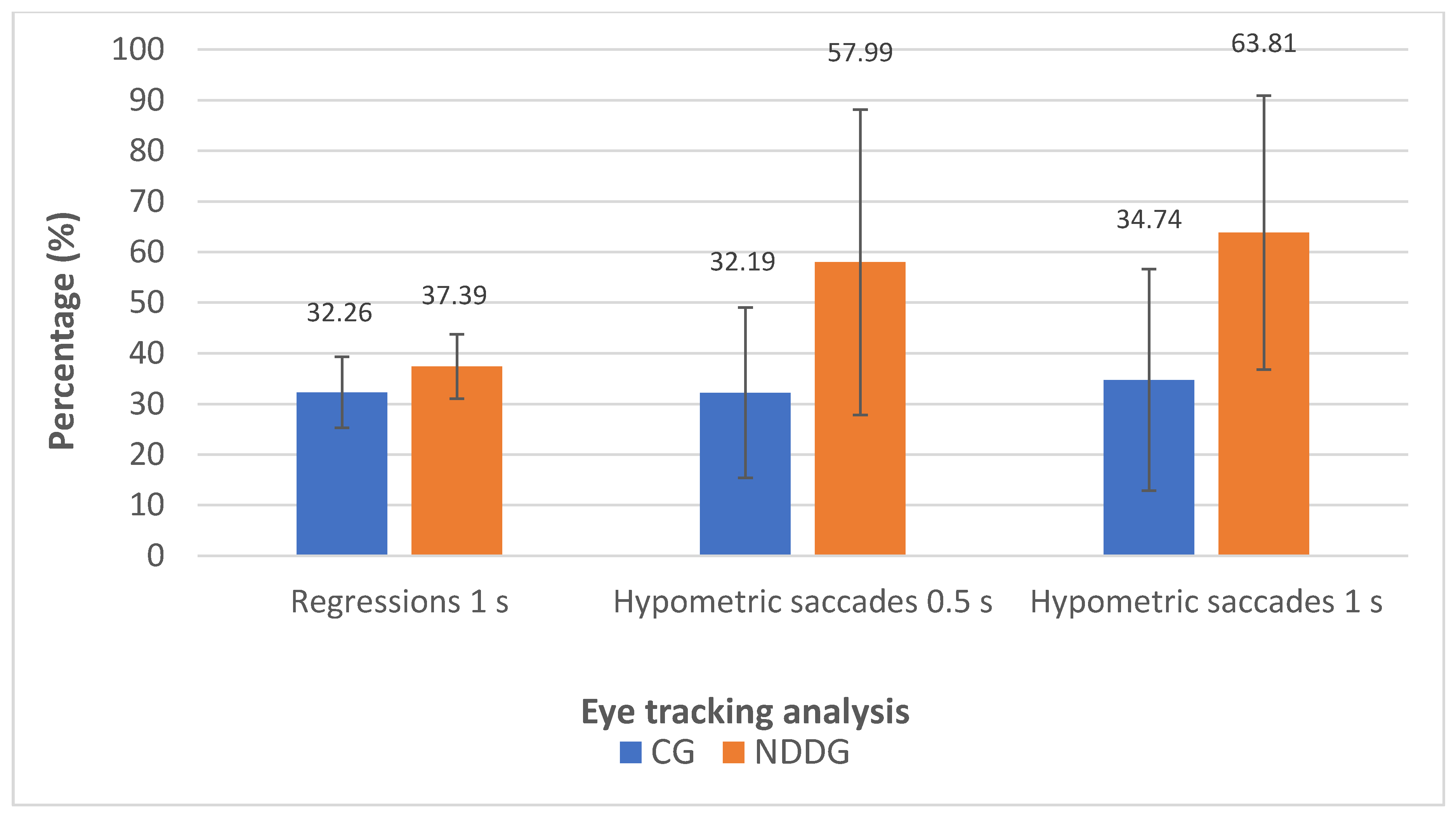
| 1 s | 32.26 (7.00) 31.80 (13.00 to 43.50) | 37.39 (6.38) 37.50 (21.00 to 47.10) | 0.012 |
| Number of completed saccades 0.5 s | 13.80 (5.12) 15.00 (5.00 to 28.00) | 11.25 (4.96) 14.00 (1.00 to 15.00) | 0.089 |
| 1 s | 10.50 (2.85) 11.00 (5.00 to 15.00) | 8.71 (3.27) 8.50 (4.00 to 15.00) | 0.114 |
| % of completed saccades 0.5 s | 75.63 (21.56) 83.33 (33.33 to 100.00) | 66.63 (31.35) 76.14 (6.67 to 100.00) | 0.411 |
| 1 s | 75.06 (19.35) 73.33 (45.45 to 100.00) | 61.69 (24.57) 60.00 (26.67 to 100.00) | 0.178 |
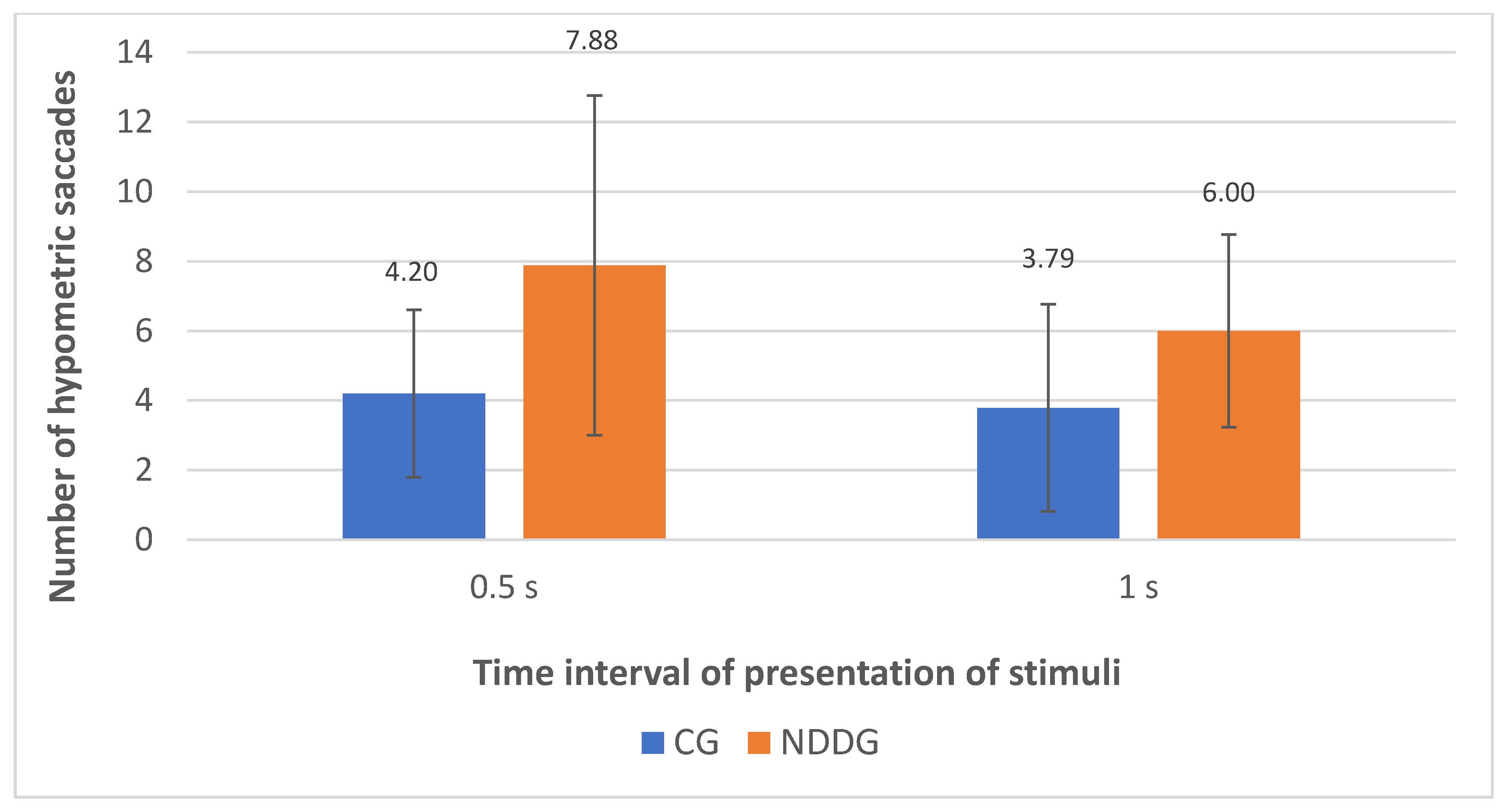
| Number of hypometric saccades 0.5 s | 4.20 (2.40) 3.00 (2.00 to 10.00) | 7.88 (4.88) 7.50 (2.00 to 21.00) | 0.010 |
| 1 s | 3.79 (2.97) 3.00 (0.00 to 10.00) | 6.00 (2.77) 6.50 (1.00 to 10.00) | 0.044 |
| Number of hypermetric saccades 0.5 s | 1.47 (1.46) 1.00 (0.00 to 4.00) | 1.69 (1.78) 1.00 (0.00 to 7.00) | 0.830 |
| 1 s | 0.57 (0.94) 0.00 (0.00 to 3.00) | 1.14 (1.56) 0.50 (0.00 to 5.00) | 0.401 |
| % hypometric saccades/completed 0.5 s | 32.19 (16.81) 26.67 (13.33 to 66.67) | 57.99 (30.18) 60.00 (13.00 to 100.00) | 0.022 |
| 1 s | 34.74 (21.87) 34.85 (0.00 to 71.43) | 63.81 (27.07) 70.00 (7.14 to 100.00) | 0.003 |
| % hypermetric saccades/completed 0.5 s | 10.85 (11.83) 6.67 (0.00 to 40.00) | 19.83 (25.04) 14.36 (0.00 to 100.00) | 0.370 |
| 1 s | 6.19 (10.14) 0.00 (0.00 to 33.33) | 12.18 (14.02) 5.56 (0.00 to 33.33) | 0.376 |
| Relationship | Linear Equation | R2 | p-Value |
|---|---|---|---|
| Percentage regressions 1 s—Ability NSUCO | Y = 40.39 − 1.77 × X | 0.096 | 0.108 |
| Percentage regressions 1 s—Precision NSUCO | Y = 40.63 − 1.81 × X | 0108 | 0.088 |
| Percentage regressions 1 s—Head/body movement associated NSUCO | Y = 39.52 − 1.61 × X | 0.118 | 0.073 |
| Number saccades completed 0.5 s—Ability NSUCO | Y = 8.61 + 1.20 × X | 0.083 | 0.109 |
| Number saccades completed 0.5 s—Precision NSUCO | Y = 9.19 + 1.01 × X | 0.069 | 0.146 |
| Number saccades completed 1 s—Ability NSUCO | Y = 5.92 + 1.17 × X | 0.214 | 0.013 |
| Number saccades completed 1 s—Precision NSUCO | Y = 5.84 + 1.17 × X | 0.230 | 0.010 |
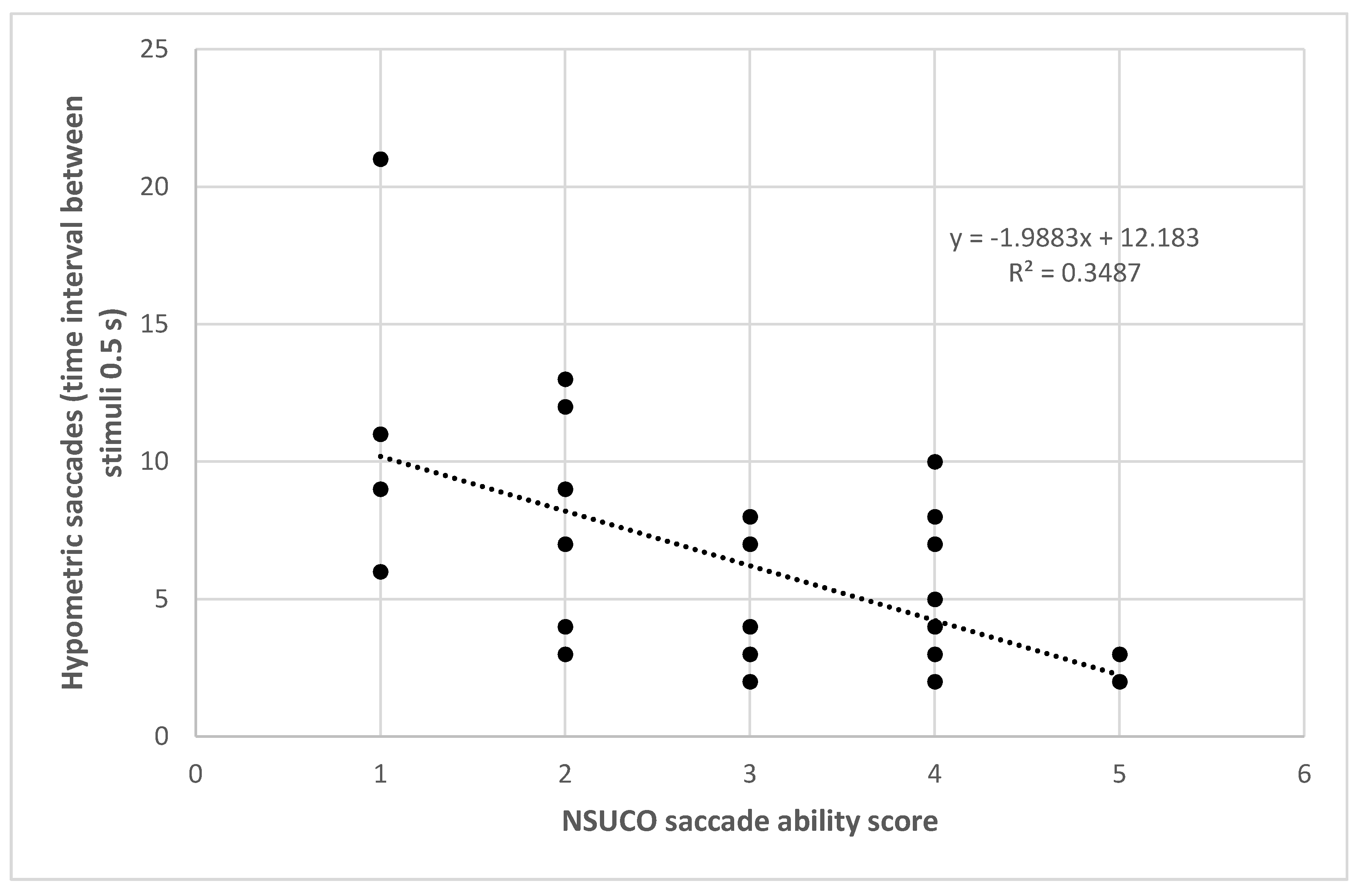
| Number hypometric saccades 0.5 s—Ability NSUCO | Y = 12.18 − 1.99 × X | 0.349 | <0.001 |
| Number hypometric saccades 0.5 s—Precision NSUCO | Y = 11.09 − 1.63 × X | 0.274 | 0.002 |
| Number hypometric saccades 0.5 s—Head/body movement associated NSUCO | Y = 9.29 − 1.13 × X | 0.173 | 0.018 |
| Percentage hypometric saccades 0.5 s—Ability NSUCO | Y = 84.81 − 12.71 × X | 0.324 | 0.001 |
| Percentage hypometric saccades 0.5 s—Precision NSUCO | Y = 79.15 − 10.86 × X | 0.276 | 0.002 |
| Percentage hypometric saccades 0.5 s—Head/body movement associated NSUCO | Y = 69.61 − 8.34 × X | 0.217 | 0.007 |
| Percentage hypometric saccades 1.0 s—Ability NSUCO | Y = 82.25 − 10.49 × X | 0.211 | 0.014 |
| Percentage hypometric saccades 1.0 s—Precision NSUCO | Y = 86.71 − 11.65 × X | 0.280 | 0.004 |
| Percentage hypometric saccades 1.0 s—Head/body movement associated NSUCO | Y = 74.94 − 8.76 × X | 0.219 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilbao, C.; Piñero, D.P. Objective and Subjective Evaluation of Saccadic Eye Movements in Healthy Children and Children with Neurodevelopmental Disorders: A Pilot Study. Vision 2021, 5, 28. https://doi.org/10.3390/vision5020028
Bilbao C, Piñero DP. Objective and Subjective Evaluation of Saccadic Eye Movements in Healthy Children and Children with Neurodevelopmental Disorders: A Pilot Study. Vision. 2021; 5(2):28. https://doi.org/10.3390/vision5020028
Chicago/Turabian StyleBilbao, Carmen, and David P. Piñero. 2021. "Objective and Subjective Evaluation of Saccadic Eye Movements in Healthy Children and Children with Neurodevelopmental Disorders: A Pilot Study" Vision 5, no. 2: 28. https://doi.org/10.3390/vision5020028
APA StyleBilbao, C., & Piñero, D. P. (2021). Objective and Subjective Evaluation of Saccadic Eye Movements in Healthy Children and Children with Neurodevelopmental Disorders: A Pilot Study. Vision, 5(2), 28. https://doi.org/10.3390/vision5020028