A Systematic Review of the Effects of Exercise on Hormones in Women with Polycystic Ovary Syndrome


Abstract
1. Introduction
1.1. Polycystic Ovary Syndrome
1.2. Rationale for Systematic Review
1.2.1. Hormones Dysregulated in PCOS
1.2.2. Role of Physical Activity in Managing PCOS Symptoms
1.3. Objectives of Review
2. Materials and Methods
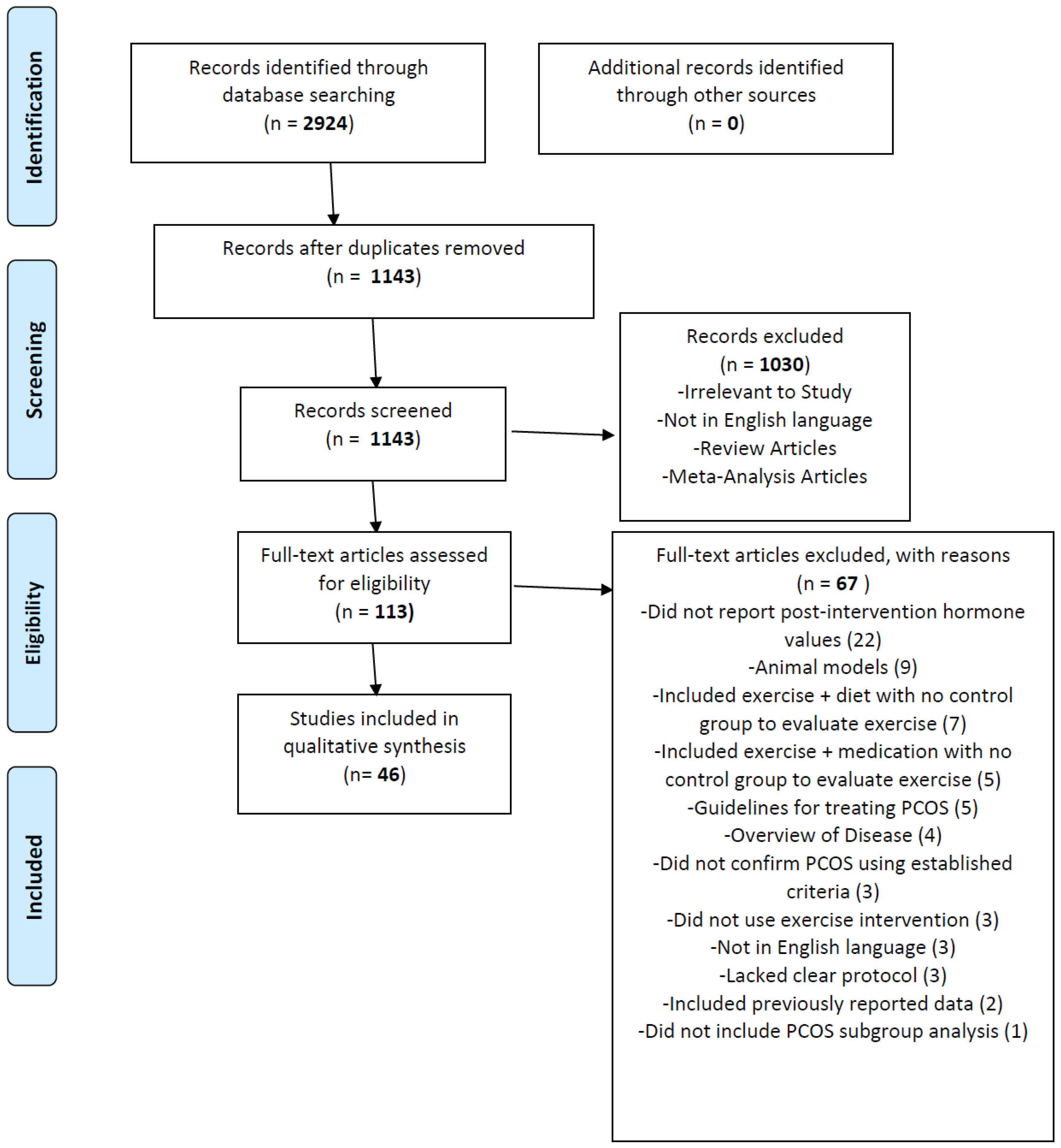
2.1. Literature Search
2.2. Eligibility Criteria, Article Screening, and Exclusion Criteria
2.3. Classification of Articles and Qualitative Synthesis
2.4. Data Collection
2.5. Risk of Bias
3. Results
3.1. Aerobic Exercise

{kind=link}
| Study | Participants | Exercise Intervention | Hormonal Changes | Unchanged |
|---|---|---|---|---|
| RCT, aerobic ex or no ex [84,85] | 90, 124 PCOS (~half/group); mean 22 y; BMI mean 29; Rotterdam criteria | 3-month structured ex. training or non-ex. CG; 3 d/wk; 30 min cycling at 60–70% VO2max; supervised by medical personnel; continuous electrocardio monitoring | ↓FI, AUCin | FSH, LH, PRL E2, P, 17-OHP, T, FAI, A4, DHEA-S SHBG |
| RCT, aerobic ex and detraining [86] | 64 PCOS (32/group); BMI mean 29; Rotterdam criteria | 24-week structured ex. training or 12-week ex. training plus 12-week detraining; 3 d/wk; 30–40 min cycling at 60–70% VO2max; supervised by medical personnel; continuous electrocardio monitoring | ↓FI, AUCins (24 wk ex.) | FSH, LH, PRL E2, P, 17-OHP, T, FAI, A4, DHEA-S SHBG |
| RCT with aerobic ex. [87] Trials NCT02105428 and NCT01477164 | 25 PCOS with OB, IR; Rotterdam criteria | 12-week aerobic exercise or sedentary control; 5 d/wk; 60 min cycling at 65% VO2max | ↑GIR ↑IS ↓C-peptide | E2, P FI, HOMA-IR |
| RCT w/3 arms (ex, OC, or vitamins) [88] Trial NCT00593294 | 150 PCOS (50/group); 18–40 y; BMI 18–30; NIH criteria | 6-month aerobic ex; 3 d/wk for 45 min at 60–70% VO2max; cycling; supervised by medical personnel; HRM | ↓FI, HOMA-IR (ex) ↑GIR (ex) | FSH, LH, TSH, PRL E2, P, 17-OHP, T, A4, FAI, SHBG DHEA-S |
| RCT w/2 parallel arms, ex or no ex [89] | 27 PCOS, sedentary; 18–34 y; BMI 25–39.9; Rotterdam criteria | 16-week progressive aerobic exercise; 3 d/wk for 50 min; indoor track using HRM to regulate walk/jog pace; supervised | N/A (hormones) | FI, HOMA-IR |
| RCT w/3 parallel arms [90,91,92,93] Trial ISRCTN10416750 | 69 PCOS (~23/group); 18–39 y, BMI 18–39.9, sedentary; Rotterdam criteria | 16-week CAT, IAT, or CG; 3 d/wk; treadmill; HRM for intensity, personal trainer for compliance | ↓TT (CAT, IAT groups) ↓FAI (IAT group) | A4, E2 LH, FSH SHBG |
| RCT, ex vs no ex [96] | 20 PCOS; 18–50 y; median BMI 37.9 ex. group; Rotterdam criteria | 16–24-week aerobic ex. individualized program, adapted from STRRIDE study, 14 kcal/kg/wk to determine duration w/recheck half-way; supervised and HRM for compliance | AUCins trended lower | FI, HOMA-IR, 2 h Ins, IS |
| RCT w/3 parallel arms (electroacupuncture, ex, untreated) [97,98,99] Trial NCT00484705 | 20 PCOS (5 ex group); BMI 26.8 ± 4.8; Rotterdam criteria 74 PCOS (30 ex group, 2012, 2015 study) | 16-week aerobic ex. at self-selected pace; at least 3 d/wk; 30–45 min at faster than normal walking pace; weekly phone call to advise how to increase ex. | N/A Note: Low n (5) in 2009 study | LH, FSH, TT, fT, FAI, DHEA-S SHBG, T4, TSH, IGF-1 FI, HOMA-IR APN (2012 study) AMH (2015 study) |
| RCT w/3 parallel arms (electroacupuncture, ex, untreated) [100] Trial NCT00484705 | 74 PCOS (30 ex. group); 30.2 ± 4.7 y; BMI 27.7 ± 6.4; Rotterdam criteria | 16-week aerobic ex., self-selected pace; at least 3 d/wk; at least 30 min at faster than normal walking pace; weekly call to advise increase of ex.; 16-wk follow-up (32 wk) | ↓fT, DHEA-S (16, 32 wk) ↓E1-S, E2 (16 wk) | T, DHT, DHEA LH, FSH, SHBG |
| Non-randomized, aerobic ex vs diet [101] Trial NCT00473538 | 40 PCOS (20 ex. group), self-selected group; 26.8 ± 5.1 y; BMI 33.1 ± 1.3; Rotterdam criteria | 24-week structured ex. training; 30–40 min cycling at 60–70% VO2max 3 d/wk; supervised by medical personnel; continuous electrocardio monitoring | ↓T, FAI (ov., 12, 24 wk) ↓FI, HOMA-IR (ov., 12, 24 wk) ↑glucose:ins (ov., 12, 24 wk) ↑SHBG (ov., 12, 24 wk) | FSH, LH, TSH, PRL E2, P, A4, DHEA-S |
| Prospective, case-control [102] Trial ISRCTN84763265 | 7 PCOS, 8 non-PCOS; BMI > 25 NIH criteria | 12-week intensified endurance ex training program; 3 d/wk; 1 h; treadmill, alternating intensity (moderate and high) | ↑GIR (both groups) ↓AMH (PCOS) | T, FAI, SHBG |
| Prospective, intensified aerobic ex., case-control [103] Trial ISRCTN84763265 | 20 PCOS, 14 non-PCOS; 20-40 y, BMI > 27; NIH criteria | 12-week intensified aerobic ex.; 3 h/wk; treadmill; supervised by ex. physiologist | ↑GIR ↓HOMA-IR, FI | T, FAI, SHBG |
| Prospective, case-control, aerobic ex [104] Trial ISRCTN84763265 | 8 PCOS, 8 non-PCOS from subset of earlier study; Rotterdam criteria | 12-week individualized, progressive aerobic ex on motorized treadmill; 3 d/wk for 1h; alternate mod. or high intensity; supervised | ↓FI ↑GIR (both) | HOMA-IR T, FAI, SHBG |
| Prospective, case-control [105] Trial ISRCTN84763265 | 16 PCOS, 13 non-PCOS; BMI > 27; NIH criteria | 12-week supervised aerobic ex; treadmill, alternating intensity (moderate and vigorous); 3 d/wk; 1 h; HRM | ↓FI ↑GIR | SHBG, T, FAI |
| Prospective, aerobic ex, case-control [106] Trial ISRCTN84763265 | 9 PCOS, 7 non-PCOS; BMI > 25, inactive; post-study, categorized as responders (lost ≥ 5% body fat) or nonresponders; Rotterdam criteria | 12-week supervised aerobic exercise; 3 d/wk, 45–60 min; treadmill, alternating moderate (20–60 min walk/jog at 75–80% HRmax) or high (6–8 5 min intervals at 95–100% HR, 2 min rest) intensity; HRM for intensity; compliance monitored by HRM, session sign-ins & duration | ↑GIR/FFM (PCOS nonresponders), positively correlated with FBG | GIR, HOMA-IR, FI |
| Single-arm, aerobic ex [107] | 8 HA PCOS; 25 ± 1 y; BMI 32 ± 1.6; controls for baseline comparison only; NIH criteria | 16-week supervised and individualized aerobic exercise; 5 d/wk; treadmill at 55% VO2max; HRM for ExEE | ↑GDR ↑ANP pD2 (−log[EC50]) | TT, FAI, SHBG FI ANP |
| Prospective, individualized aerobic ex., case-control [108] Trial NCT01150539 | 8 PCOS, 7 non-PCOS; BMI ≥ 25; NIH criteria | 16-week individualized aerobic ex. program; 5 d/wk; treadmill at 55% VO2max; supervised | Improved IS (↑glucose, FFA uptake) 34% ↑ glucose uptake | Ins, TT, FAI SHBG |
| Prospective, aerobic ex., case-control [109] Trial NCT01150539 | 8 PCOS, 8 non-PCOS; Rotterdam criteria | 16-week supervised aerobic ex; 5 d/wk; treadmill at 55% VO2max | ↓Leptin/HMW APN ↑GDR Trend: ↓leptin, ↑DHEA-S | APN, HMW APN T, FAI, SHBG HOMA-IR |
| Prospective, case-control or self-selected ex or no ex [110,111] | 11 PCOS, 6 non-PCOS; 29 ± 7 y; BMI 34 ± 5; Rotterdam criteria 17 PCOS, self-selected to ex (10) or no ex (7) group; mean 28 y; mean BMI 33; Rotterdam criteria | 16-week supervised moderate-intensity aerobic ex on treadmill; 3 d/wk for 30 min at 30% HRR progressing up to 5 d/wk for 45 min at 60% HRR | N/A (hormones) Note: Low n (6–7) | FSH, LH P, E2, T, FAI, SHBG FI, HOMA-IR |
| Prospective, aerobic ex, case-control [112] | 12 PCOS, 10 non-PCOS; Rotterdam criteria | 8-week supervised aerobic exercise; 3 d/wk for 1 h; treadmill at 60% VO2max | ↓GDR Decreased lipid-induced IR | TT, FAI, SHBG FI |
| Prospective, case-control, aerobic ex [113] Trial ISRCTN42448814 | 12 PCOS 10 non-PCOS; mean 28.3 y (PCOS); mean BMI 29.4 (PCOS); Rotterdam criteria | 8-week supervised aerobic ex; 3 d/wk for 1h; treadmill at 60% VO2max | N/A (hormones) | HOMA-IR |
| Single-arm, aerobic ex [114] | 21 PCOS (12 compliant, 9 non); 30.6 ± 6.6 y; BMI 35.5 ± 7.6 NIH criteria | 6-month self-selected brisk walking; at least 3 d/wk; 20–60 min; frequency and duration targets increased fortnightly; self-reported diary submitted monthly | N/A (hormones) | Ins FAI T4 |
3.2. High Intensity Interval Training and Combination Exercise Interventions
3.3. Progressive Resistance Training or Strength Training
3.4. Yoga
3.5. Single Bout Exercise
4. Discussion
4.1. Impact of Exercise on Hormones Related to PCOS Pathology
4.1.1. Sex Hormones
4.1.2. Insulin
4.1.3. LH and FSH
4.1.4. Adipokines
4.1.5. AMH
4.2. Physical Activity Habits in Adolescents and Women with PCOS
4.3. Limitations and Need for Additional Studies
5. Conclusions
5.1. Recommendations for Guidelines
- All patients should be asked about current physical activity type(s), frequency, duration, and intensity. Adolescents and obese patients in particular should be asked about barriers to physical activity and counseled appropriately;
- Vigorous aerobic activity at least three days per week for 30 min or more is recommended. A heart rate monitor or VO2max guided intensity levels (≥60% VO2max) are advisable to obtain insulin-related benefits;
- Combination exercise that includes PRT or ST three days per week on non-consecutive days may provide additional benefits with respect to androgen levels;
- Yoga may be a desirable activity to include as a regular physical exercise, although further studies are warranted to confirm its benefits with respect to androgens and insulin responsiveness.
5.2. Overall Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| A4 | Androstenedione |
| AMH | Anti-Mullerian hormone |
| ANP | Atrial natriuretic peptice |
| APN | Adiponectin |
| AUC | Area under the curve |
| Anov | Anovulatory |
| BMI | Body mass index |
| bpm | Beats per minute |
| CAT | Continuous aerobic training |
| cd | Cycle days |
| CG | Control group |
| d | Days |
| DHEA-S | Dehydroepiandrosterone sulfate |
| E1-S | Estrone sulfate |
| E2 | Estradiol |
| Ex | Exercise |
| ExEE | Exercise energy expenditure |
| FAI | Free androgen index |
| FBG | Fasting blood glucose |
| FFM | Fat free mass |
| FI | Fasting insulin |
| FSH | Follicle stimulating hormone |
| fT | Free testosterone |
| GDR | Glucose disposal rate |
| GIR | Glucose infusion rate |
| HIIT | High intensity interval training |
| HMW | High molecular weight |
| HOMA-IR | Homeostatic model assessment of insulin resistance |
| HR | Heart rate |
| HRM | Heart rate monitor |
| HRR | Heart rate reserve |
| IAT | Intermittent aerobic training |
| II | Intensity interval |
| Ins | Insulin |
| IR | Insulin resistance |
| IS | Insulin sensitivity |
| LH | Luteinizing hormone |
| Met | Metformin |
| MICT | Medium intensity continuous training |
| Mo | Month (s) |
| N/A | Not applicable |
| NW | Normoweight |
| OB | Overweight or obese |
| OC | Oral contraceptive |
| OGTT | Oral glucose tolerance test |
| Ov | Ovulatory |
| PA | Physical activity |
| PRL | Prolactin |
| PRT | Progressive resistance training |
| RCT | Randomized controlled trial |
| Reps | Repetitions |
| RM | Repetition maximum |
| SHBG | Sex hormone binding globulin |
| ST | Strength training |
| T | Testosterone |
| T4 | Thyroxine |
| TSH | Thyroid stimulating hormone |
| TT | Total testosterone |
| Wk | Week (s) |
| Wt | Weight |
| Y | Year (s) |
References
- Franks, S. Polycystic ovary syndrome. N. Engl. J. Med. 1995, 333, 853–861. [Google Scholar] [CrossRef] [PubMed]
- March, W.A.; Moore, V.M.; Willson, K.J.; Phillips, D.I.; Norman, R.; Davies, M. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum. Reprod. 2009, 25, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Welt, C.K.; Carmina, E. Clinical review: Lifecycle of polycystic ovary syndrome (PCOS): From in utero to menopause. J. Clin. Endocrinol. Metab. 2013, 98, 4629–4638. [Google Scholar] [CrossRef] [PubMed]
- Zawadski, J.K.; Dunaif, A. Diagnostic Criteria for Polycystic Ovary Syndrome: Towards a Rational Approach; Blackwell Scientific Publications: Boston, MA, USA, 1992. [Google Scholar]
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Carmina, E.; Dewailly, D.; Diamanti-Kandarakis, E.; Escobar-Morreale, H.F.; Futterweit, W.; Janssen, O.E.; Legro, R.S.; Norman, R.; Taylor, A.E.; et al. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: The complete task force report. Fertil. Steril. 2009, 91, 456–488. [Google Scholar] [CrossRef]
- Lujan, M.E.; Chizen, N.R.; Pierson, R.A. Diagnostic Criteria for Polycystic Ovary Syndrome: Pitfalls and Controversies. J. Obstet. Gynaecol. Can. 2008, 30, 671–679. [Google Scholar] [CrossRef]
- Raj, S.G.; Thompson, I.E.; Berger, M.J.; Talert, L.M.; Taymor, M.L. Diagnostic value of androgen measurements in polycystic ovary syndrome. Obstet. Gynecol. 1978, 52, 169–171. [Google Scholar]
- Teede, H.J.; Deeks, A.A.; Moran, L.J. Polycystic ovary syndrome: A complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010, 8, 41. [Google Scholar] [CrossRef]
- Cussons, A.J.; Watts, G.F.; Burke, V.; Shaw, J.E.; Zimmet, P.Z.; Stuckey, B.G.A. Cardiometabolic risk in polycystic ovary syndrome: A comparison of different approaches to defining the metabolic syndrome. Hum. Reprod. 2008, 23, 2352–2358. [Google Scholar] [CrossRef]
- Cinar, N.; Kizilarslanoglu, M.C.; Harmanci, A.; Aksoy, D.Y.; Bozdag, G.; Demir, B.; Yıldız, B.O. Depression, anxiety and cardiometabolic risk in polycystic ovary syndrome. Hum. Reprod. 2011, 26, 3339–3345. [Google Scholar] [CrossRef]
- Stuckey, B.; Opie, N.; Cussons, A.J.; Watts, G.F.; Burke, V. Clustering of metabolic and cardiovascular risk factors in the polycystic ovary syndrome: A principal component analysis. Metabolism 2014, 63, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Norman, R.; Teede, H.J. Metabolic risk in PCOS: Phenotype and adiposity impact. Trends Endocrinol. Metab. 2015, 26, 136–143. [Google Scholar] [CrossRef]
- Talbott, E.O.; Guzick, D.S.; Sutton-Tyrrell, K.; McHugh-Pemu, K.P.; Zborowski, J.V.; Remsberg, K.E.; Kuller, L.H. Evidence for association between polycystic ovary syndrome and premature carotid atherosclerosis in middle-aged women. Arter. Thromb. Vasc. Boil. 2000, 20, 2414–2421. [Google Scholar] [CrossRef] [PubMed]
- Boulman, N.; Levy, Y.; Leiba, R.; Shachar, S.; Linn, R.; Zinder, O.; Blumenfeld, Z. Increased C-Reactive Protein Levels in the Polycystic Ovary Syndrome: A Marker of Cardiovascular Disease. J. Clin. Endocrinol. Metab. 2004, 89, 2160–2165. [Google Scholar] [CrossRef] [PubMed]
- Tarkun, I.; Arslan, B.Ç.; Canturk, Z.; Turemen, E.; Şahin, T.; Duman, C. Endothelial Dysfunction in Young Women with Polycystic Ovary Syndrome: Relationship with Insulin Resistance and Low-Grade Chronic Inflammation. J. Clin. Endocrinol. Metab. 2004, 89, 5592–5596. [Google Scholar] [CrossRef]
- Vryonidou, A.; Papatheodorou, A.; Tavridou, A.; Terzi, T.; Loi, V.; Vatalas, I.-A.; Batakis, N.; Phenekos, C.; Dionyssiou-Asteriou, A. Association of Hyperandrogenemic and Metabolic Phenotype with Carotid Intima-Media Thickness in Young Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 2740–2746. [Google Scholar] [CrossRef]
- Teede, H.J.; Hutchison, S.; Zoungas, S.; Meyer, C. Insulin resistance, the metabolic syndrome, diabetes, and cardiovascular disease risk in women with PCOS. Endocrine 2006, 30, 45–54. [Google Scholar] [CrossRef]
- Ramezani-Binabaj, M.; Motalebi, M.; Karimi-Sari, H.; Rezaee-Zavareh, M.S.; Alavian, S.M. Are women with polycystic ovarian syndrome at a high risk of non-alcoholic Fatty liver disease; a meta-analysis. Hepat. Mon. 2014, 14, 23235. [Google Scholar] [CrossRef]
- Weiner, C.L.; Primeau, M.; Ehrmann, D.A. Androgens and mood dysfunction in women: Comparison of women with polycystic ovarian syndrome to healthy controls. Psychosom. Med. 2004, 66, 356–362. [Google Scholar]
- Månsson, M.; Holte, J.; Landin-Wilhelmsen, K.; Dahlgren, E.; Johansson, A.G.; Landen, M. Women with polycystic ovary syndrome are often depressed or anxious—A case control study. Psychoneuroendocrinology 2008, 33, 1132–1138. [Google Scholar] [CrossRef]
- Benson, S.; Hahn, S.; Tan, S.; Mann, K.; Janssen, O.; Schedlowski, M.; Elsenbruch, S. Prevalence and implications of anxiety in polycystic ovary syndrome: Results of an internet-based survey in Germany. Hum. Reprod. 2009, 24, 1446–1451. [Google Scholar] [CrossRef] [PubMed]
- Laggari, V.; Diareme, S.; Christogiorgos, S.; Deligeoroglou, E.; Christopoulos, P.; Tsiantis, J.; Creatsas, G. Anxiety and depression in adolescents with polycystic ovary syndrome and Mayer-Rokitansky-Küster-Hauser syndrome. J. Psychosom. Obstet. Gynecol. 2009, 30, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Deeks, A.A.; Gibson-Helm, M.E.; Teede, H.J. Anxiety and depression in polycystic ovary syndrome: A comprehensive investigation. Fertil. Steril. 2010, 93, 2421–2423. [Google Scholar] [CrossRef] [PubMed]
- Farrell, K.; Antoni, M.H. Insulin resistance, obesity, inflammation, and depression in polycystic ovary syndrome: Biobehavioral mechanisms and interventions. Fertil. Steril. 2010, 94, 1565–1574. [Google Scholar] [CrossRef]
- Jedel, E.; Waern, M.; Gustafson, D.; Landén, M.; Eriksson, E.; Holm, G.; Nilsson, L.; Lind, A.K.; Janson, P.O.; Stener-Victorin, E. Anxiety and depression symptoms in women with polycystic ovary syndrome compared with controls matched for body mass index. Hum. Reprod. 2009, 25, 450–456. [Google Scholar] [CrossRef]
- Rassi, A.; Veras, A.B.; dos Reis, M.; Pastore, D.L.; Bruno, L.M.; Bruno, R.V.; de Ávila, M.A.; Nardi, A.E. Prevalence of psychiatric disorders in patients with polycystic ovary syndrome. Compr. Psychiatry 2010, 51, 599–602. [Google Scholar] [CrossRef]
- Barry, J.A.; Hardiman, P.J.; Saxby, B.K.; Kuczmierczyk, A. Testosterone and mood dysfunction in women with polycystic ovarian syndrome compared to subfertile controls. J. Psychosom. Obstet. Gynecol. 2011, 32, 104–111. [Google Scholar] [CrossRef]
- Deeks, A.A.; Gibson-Helm, M.E.; Paul, E.; Teede, H.J. Is having polycystic ovary syndrome a predictor of poor psychological function including anxiety and depression? Hum. Reprod. 2011, 26, 1399–1407. [Google Scholar] [CrossRef]
- Livadas, S.; Chaskou, S.; Kandaraki, A.A.; Skourletos, G.; Economou, F.; Christou, M.; Boutzios, G.; Karachalios, A.; Zerva, A.; Xyrafis, X.; et al. Anxiety is associated with hormonal and metabolic profile in women with polycystic ovarian syndrome. Clin. Endocrinol. 2011, 75, 698–703. [Google Scholar] [CrossRef]
- Dokras, A. Mood and anxiety disorders in women with PCOS. Steroids 2012, 77, 338–341. [Google Scholar] [CrossRef]
- Krępuła, K.; Bidzińska-Speichert, B.; Lenarcik, A.; Tworowska-Bardzińska, U. Psychiatric disorders related to polycystic ovary syndrome. Endokrynol. Polska 2012, 63, 488–491. [Google Scholar]
- Açmaz, G.; Albayrak, E.; Acmaz, B.; Başer, M.; Soyak, M.; Zararsız, G.; IpekMüderris, I. Level of anxiety, depression, self-esteem, social anxiety, and quality of life among the women with polycystic ovary syndrome. Sci. World J. 2013, 2013, 851815–851817. [Google Scholar] [CrossRef]
- Mahajan, D.K. Steroidogenesis in Human Polycystic Ovary. Endocrinol. Metab. Clin. N. Am. 1988, 17, 751–769. [Google Scholar] [CrossRef]
- Barnes, R.B. The pathogenesis of polycystic ovary syndrome: Lessons from ovarian stimulation studies. J. Endocrinol. Investig. 1998, 21, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, R.L.; Makris, A.; Randall, R.W.; Daniels, G.; Kistner, R.W.; Ryan, K.J. Insulin stimulates androgen accumulation in incubations of ovarian stroma obtained from women with hyperandrogenism. J. Clin. Endocrinol. Metab. 1986, 62, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, R.L.; Smith, S.; Ryan, K.J. The role of hyperinsulinemia in the pathogenesis of ovarian hyperandrogenism. Fertil. Steril. 1988, 50, 197–212. [Google Scholar]
- Nestler, J.E. Insulin regulation of human ovarian androgens. Hum. Reprod. 1997, 12 (Suppl. 1), 53–62. [Google Scholar] [CrossRef]
- Nestler, J. Role of Hyperinsulinemia in the Pathogenesis of the Polycystic Ovary Syndrome, and Its Clinical Implications. Semin. Reprod. Med. 1997, 15, 111–122. [Google Scholar] [CrossRef]
- Dunaif, A.; Xia, J.; Book, C.B.; Schenker, E.; Tang, Z. Excessive insulin receptor serine phosphorylation in cultured fibroblasts and in skeletal muscle. A potential mechanism for insulin resistance in the polycystic ovary syndrome. J. Clin. Investig. 1995, 96, 801–810. [Google Scholar] [CrossRef]
- Dunaif, A.; Segal, K.R.; Shelley, D.R.; Green, G.; Dobrjansky, A.; Licholai, T. Evidence for distinctive and intrinsic defects in insulin action in polycystic ovary syndrome. Diabetes 1992, 41, 1257–1266. [Google Scholar] [CrossRef]
- Ciaraldi, T.P.; el-Roeiy, A.; Madar, Z.; Reichart, D.; Olefsky, J.M.; Yen, S.S. Cellular mechanisms of insulin resistance in polycystic ovarian syndrome. J. Clin. Endocrinol. Metab. 1992, 75, 577–583. [Google Scholar] [PubMed]
- Corbould, A.; Zhao, H.; Mirzoeva, S.; Aird, F.; Dunaif, A. Enhanced mitogenic signaling in skeletal muscle of women with polycystic ovary syndrome. Diabetes 2006, 55, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Book, C.B.; Dunaif, A. Selective insulin resistance in the polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 1999, 84, 3110–3116. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Kouli, C.R.; Bergiele, A.T.; Filandra, F.A.; Tsianateli, T.C.; Spina, G.G.; Zapanti, E.D.; Bartzis, M.I. A survey of the polycystic ovary syndrome in the Greek island of Lesbos: Hormonal and metabolic profile. J. Clin. Endocrinol. Metab. 1999, 84, 4006–4011. [Google Scholar] [CrossRef] [PubMed]
- Grulet, H.; Hecart, A.C.; Delemer, B.; Gross, A.; Sulmont, V.; Leutenegger, M.; Caron, J. Roles of LH and insulin resistance in lean and obese polycystic ovary syndrome. Clin. Endocrinol. 1993, 38, 621–626. [Google Scholar] [CrossRef]
- Dunaif, A. Insulin resistance and the polycystic ovary syndrome: Mechanism and implications for pathogenesis. Endocr. Rev. 1997, 18, 774–800. [Google Scholar]
- Corbould, A.; Kim, Y.B.; Youngren, J.F.; Pender, C.; Kahn, B.B.; Lee, A.; Dunaif, A. Insulin resistance in the skeletal muscle of women with PCOS involves intrinsic and acquired defects in insulin signaling. Am. J. Physiol. Metab. 2005, 288, E1047–E1054. [Google Scholar] [CrossRef]
- Mario, F.M.; do Amarante, F.; Toscani, M.K.; Spritzer, P.M. Lean muscle mass in classic or ovulatory PCOS: Association with central obesity and insulin resistance. Exp. Clin. Endocrinol. Diabetes 2012, 120, 511–516. [Google Scholar] [CrossRef]
- Farshchi, H.; Rane, A.; Love, A.; Kennedy, R.L. Diet and nutrition in polycystic ovary syndrome (PCOS): Pointers for nutritional management. J. Obstet. Gynaecol. 2007, 27, 762–773. [Google Scholar] [CrossRef]
- Teede, H.J.; Hutchison, S.K.; Zoungas, S. The management of insulin resistance in polycystic ovary syndrome. Trends Endocrinol. Metab. 2007, 18, 273–279. [Google Scholar] [CrossRef]
- Moran, L.J.; Pasquali, R.; Teede, H.J.; Hoeger, K.M.; Norman, R.J. Treatment of obesity in polycystic ovary syndrome: A position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil. Steril. 2009, 92, 1966–1982. [Google Scholar] [CrossRef] [PubMed]
- Artini, P.G.; Di Berardino, O.M.; Simi, G.; Papini, F.; Ruggiero, M.; Monteleone, P.; Cela, V. Best methods for identification and treatment of PCOS. Minerva Ginecol. 2010, 62, 33–48. [Google Scholar] [PubMed]
- Costello, M.; Ledger, W. Evidence-Based Lifestyle and Pharmacological Management of Infertility in Women with Polycystic Ovary Syndrome. Womens Health 2012, 8, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Bates, G.W.; Legro, R.S. Longterm management of Polycystic Ovarian Syndrome (PCOS). Mol. Cell. Endocrinol. 2012, 373, 91–97. [Google Scholar] [CrossRef]
- Carmina, E. Obesity, Adipokines and Metabolic Syndrome in Polycystic Ovary Syndrome. Front. Horm. Res. 2012, 40, 40–50. [Google Scholar]
- Mirza, S.S.; Shafique, K.; Shaikh, A.R.; Khan, N.A.; Anwar Qureshi, M. Association between circulating adiponectin levels and polycystic ovarian syndrome. J. Ovarian Res. 2014, 7, 18. [Google Scholar] [CrossRef]
- Sarray, S.; Madan, S.; Saleh, L.R.; Mahmoud, N.; Almawi, W.Y. Validity of adiponectin-to-leptin and adiponectin-to-resistin ratios as predictors of polycystic ovary syndrome. Fertil. Steril. 2015, 104, 460–466. [Google Scholar] [CrossRef]
- Behboudi-Gandevani, S.; Ramezani Tehrani, F.; Bidhendi Yarandi, R.; Noroozzadeh, M.; Hedayati, M.; Azizi, F. The association between polycystic ovary syndrome, obesity, and the serum concentration of adipokines. J. Endocrinol. Investig. 2017, 40, 859–866. [Google Scholar] [CrossRef]
- Holte, J.; Bergh, T.; Gennarelli, G.; Wide, L. The independent effects of polycystic ovary syndrome and obesity on serum concentrations of gonadotrophins and sex steroids in premenopausal women. Clin. Endocrinol. 1994, 41, 473–481. [Google Scholar] [CrossRef]
- Marshall, J.C.; Eagleson, C.A. NEUROENDOCRINE ASPECTS OF POLYCYSTIC OVARY SYNDROME. Endocrinol. Metab. Clin. N. Am. 1999, 28, 295–324. [Google Scholar] [CrossRef]
- Li, H.; He, Y.L.; Li, R.; Wong, C.; Sy, B.; Lam, C.W.; Lam, K.; Peng, H.M.; Mu, S.; Schooling, M.; et al. Age-specific reference ranges of serum anti-müllerian hormone in healthy women and its application in diagnosis of polycystic ovary syndrome: A population study. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.L.; Field, H.P.; Calder, N.; Picton, H.M.; Balen, A.H.; Barth, J.H. Anti-Müllerian hormone reflects the severity of polycystic ovary syndrome. Clin. Endocrinol. 2016, 86, 395–400. [Google Scholar] [CrossRef]
- Lie Fong, S.; Laven, J.S.E.; Duhamel, A.; Dewailly, D. Polycystic ovarian morphology and the diagnosis of polycystic ovary syndrome: Redefining threshold levels for follicle count and serum anti-Müllerian hormone using cluster analysis. Hum. Reprod. 2017, 32, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, T.; Munkhzaya, M.; Iwasa, T.; Tungalagsuvd, A.; Yano, K.; Mayila, Y.; Yanagihara, R.; Tokui, T.; Kato, T.; Kuwahara, A.; et al. Relationship between serum anti-Mullerian hormone and clinical parameters in polycystic ovary syndrome. Endocr. J. 2017, 64, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Sathyapalan, T.; Al-Qaissi, A.; Kilpatrick, E.S.; Dargham, S.R.; Atkin, S.L. Anti-Müllerian hormone measurement for the diagnosis of polycystic ovary syndrome. Clin. Endocrinol. 2018, 88, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Batarfi, A.A.; Bajouh, O.S.; Bakhashab, S. Serum Anti-Müllerian Hormone in the Diagnosis of Polycystic Ovary Syndrome in Association with Clinical Symptoms. Diagnostics 2019, 9, 136. [Google Scholar] [CrossRef] [PubMed]
- Karkanaki, A.; Piouka, A.; Katsikis, I.; Farmakiotis, D.; Macut, D.; Panidis, D. Adiponectin levels reflect the different phenotypes of polycystic ovary syndrome: Study in normal weight, normoinsulinemic patients. Fertil. Steril. 2009, 92, 2078–2081. [Google Scholar] [CrossRef]
- Niafar, M.; Nader, N.D. Adiponectin as serum biomarker of insulin resistance in patients with polycystic ovarian syndrome. Gynecol. Endocrinol. 2015, 31, 1–4. [Google Scholar] [CrossRef]
- Chan, T.F.; Chen, Y.L.; Chen, H.H.; Lee, C.H.; Jong, S.B.; Tsai, E.M. Increased plasma visfatin concentrations in women with polycystic ovary syndrome. Fertil. Steril. 2007, 88, 401–405. [Google Scholar] [CrossRef]
- Kowalska, I.; Straczkowski, M.; Nikolajuk, A.; Adamska, A.; Karczewska-Kupczewska, M.; Otziomek, E.; Wolczynski, S.; Gorska, M. Serum visfatin in relation to insulin resistance and markers of hyperandrogenism in lean and obese women with polycystic ovary syndrome. Hum. Reprod. 2007, 22, 1824–1829. [Google Scholar] [CrossRef]
- Panidis, D.; Farmakiotis, D.; Rousso, D.; Katsikis, I.; Delkos, D.; Piouka, A.; Gerou, S.; Diamanti-Kandarakis, E. Plasma visfatin levels in normal weight women with polycystic ovary syndrome. Eur. J. Intern. Med. 2008, 19, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Gen, R.; Akbay, E.; Muslu, N.; Sezer, K.; Cayan, F. Plasma visfatin level in lean women with PCOS: Relation to proinflammatory markers and insulin resistance. Gynecol. Endocrinol. 2009, 25, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Dıkmen, E.; Tarkun, I.; Cantürk, Z.; Cetınarslan, B. Plasma visfatin level in women with polycystic ovary syndrome. Gynecol. Endocrinol. 2010, 27, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Farshchian, F.; Ramezani Tehrani, F.; Amirrasouli, H.; Rahimi Pour, H.; Hedayati, M.; Kazerouni, F.; Soltani, A. Visfatin and resistin serum levels in normal-weight and obese women with polycystic ovary syndrome. Int. J. Endocrinol. Metab. 2014, 12, 15503. [Google Scholar] [CrossRef]
- Lewandowski, K.C.; Szosland, K.; O’Callaghan, C.; Tan, B.K.; Randeva, H.S.; Lewinski, A. Adiponectin and resistin serum levels in women with polycystic ovary syndrome during oral glucose tolerance test: A significant reciprocal correlation between adiponectin and resistin independent of insulin resistance indices. Mol. Genet. Metab. 2005, 85, 61–69. [Google Scholar] [CrossRef]
- Seow, K.M.; Juan, C.C.; Wu, L.Y.; Hsu, Y.P.; Yang, W.M.; Tsai, Y.L.; Hwang, J.L.; Ho, L.T. Serum and adipocyte resistin in polycystic ovary syndrome with insulin resistance. Hum. Reprod. 2004, 19, 48–53. [Google Scholar] [CrossRef]
- Munir, I.; Yen, H.W.; Baruth, T.; Tarkowski, R.; Azziz, R.; Magoffin, D.A.; Jakimiuk, A.J. Resistin stimulation of 17alpha-hydroxylase activity in ovarian theca cells in vitro: Relevance to polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 4852–4857. [Google Scholar] [CrossRef]
- Zheng, S.-H.; Du, D.-F.; Li, X.-L. Leptin Levels in Women With Polycystic Ovary Syndrome: A Systematic Review and a Meta-Analysis. Reprod. Sci. 2016, 24, 656–670. [Google Scholar] [CrossRef]
- Mantzoros, C.S.; Dunaif, A.; Flier, J.S. Leptin concentrations in the polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 1997, 82, 1687–1691. [Google Scholar] [CrossRef]
- Baldani, D.P.; Skrgatic, L.; Kasum, M.; Zlopasa, G.; Kralik Oguic, S.; Herman, M. Altered leptin, adiponectin, resistin and ghrelin secretion may represent an intrinsic polycystic ovary syndrome abnormality. Gynecol. Endocrinol. 2019, 35, 401–405. [Google Scholar] [CrossRef]
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Consensus on women’s health aspects of polycystic ovary syndrome (PCOS). Hum. Reprod. 2012, 27, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Hoeger, K. Exercise Therapy in Polycystic Ovary Syndrome. Semin. Reprod. Med. 2008, 26, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Vigorito, C.; Giallauria, F.; Palomba, S.; Cascella, T.; Manguso, F.; Lucci, R.; De Lorenzo, A.; Tafuri, D.; Lombardi, G.; Colao, A.; et al. Beneficial effects of a three-month structured exercise training program on cardiopulmonary functional capacity in young women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2007, 92, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Giallauria, F.; Palomba, S.; Maresca, L.; Vuolo, L.; Tafuri, D.; Lombardi, G.; Colao, A.; Vigorito, C.; Francesco, O. Exercise training improves autonomic function and inflammatory pattern in women with polycystic ovary syndrome (PCOS). Clin. Endocrinol. 2008, 69, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Orio, F.; Giallauria, F.; Palomba, S.; Manguso, F.; Orio, M.; Tafuri, D.; Lombardi, G.; Carmina, E.; Colao, A.; Vigorito, C. Metabolic and cardiopulmonary effects of detraining after a structured exercise training programme in young PCOS women. Clin. Endocrinol. 2008, 68, 976–981. [Google Scholar] [CrossRef]
- Konopka, A.R.; Asante, A.; Lanza, I.R.; Robinson, M.M.; Johnson, M.L.; Dalla Man, C.; Cobelli, C.; Amols, M.H.; Irving, B.A.; Nair, K.S. Defects in mitochondrial efficiency and H2O2 emissions in obese women are restored to a lean phenotype with aerobic exercise training. Diabetes 2015, 64, 2104–2115. [Google Scholar] [CrossRef]
- Orio, F.; Muscogiuri, G.; Giallauria, F.; Savastano, S.; Bottiglieri, P.; Tafuri, D.; Predotti, P.; Colarieti, G.; Colao, A.; Palomba, S. Oral contraceptives versus physical exercise on cardiovascular and metabolic risk factors in women with polycystic ovary syndrome: A randomized controlled trial. Clin. Endocrinol. 2016, 85, 764–771. [Google Scholar] [CrossRef]
- Costa, E.C.; DE Sá, J.C.F.; Stepto, N.K.; Costa, I.B.B.; Farias-Junior, L.F.; Moreira, S.D.N.T.; Soares, E.M.M.; Lemos, T.M.A.M.; Browne, R.A.V.; Azevedo, G.D. Aerobic Training Improves Quality of Life in Women with Polycystic Ovary Syndrome. Med. Sci. Sports Exerc. 2018, 50, 1357–1366. [Google Scholar] [CrossRef]
- Lopes, I.P.; Ribeiro, V.B.; Reis, R.M.; Silva, R.C.; Dutra de Souza, H.C.; Kogure, G.S.; Ferriani, R.A.; Silva Lara, L.A.D. Comparison of the Effect of Intermittent and Continuous Aerobic Physical Training on Sexual Function of Women With Polycystic Ovary Syndrome: Randomized Controlled Trial. J. Sex. Med. 2018, 15, 1609–1619. [Google Scholar] [CrossRef]
- Ribeiro, V.B.; Lopes, I.P.; Dos Reis, R.M.; Silva, R.C.; Mendes, M.C.; Melo, A.S.; de Souza, H.C.D.; Ferriani, R.A.; Kogure, G.S.; Lara, L.A.D.S. Continuous versus intermittent aerobic exercise in the improvement of quality of life for women with polycystic ovary syndrome: A randomized controlled trial. J. Health Psychol. 2019. [Google Scholar] [CrossRef]
- Ribeiro, V.B.; Kogure, G.S.; Lopes, I.P.; Silva, R.C.; Pedroso, D.C.C.; de Melo, A.S.; de Souza, H.C.D.; Ferriani, R.A.; Miranda Furtado, C.L.; Dos Reis, R.M. Effects of continuous and intermittent aerobic physical training on hormonal and metabolic profile, and body composition in women with polycystic ovary syndrome: A randomized controlled trial. Clin. Endocrinol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kogure, G.S.; Lopes, I.P.; Ribeiro, V.B.; Mendes, M.C.; Kodato, S.; Furtado, C.L.M.; Silva de Sá, M.F.; Ferriani, R.A.; Lara, L.A.D.S.; Reis, R.M.D. The effects of aerobic physical exercises on body image among women with polycystic ovary syndrome. J. Affect. Disord. 2020, 262, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Slentz, C.A.; Aiken, L.B.; Houmard, J.A.; Bales, C.W.; Johnson, J.L.; Tanner, C.J.; Duscha, B.D.; Kraus, W.E. Inactivity, exercise, and visceral fat. STRRIDE: A randomized, controlled study of exercise intensity and amount. J. Appl. Physiol. 2005, 99, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Slentz, C.A.; Bateman, L.A.; Willis, L.H.; Shields, A.T.; Tanner, C.J.; Piner, L.W.; Hawk, V.H.; Muehlbauer, M.J.; Samsa, G.P.; Nelson, R.C.; et al. Effects of aerobic vs. resistance training on visceral and liver fat stores, liver enzymes, and insulin resistance by HOMA in overweight adults from STRRIDE AT/RT. Am. J. Physiol. Metab. 2011, 301, E1033–E1039. [Google Scholar] [CrossRef]
- Brown, A.J.; Setji, T.L.; Sanders, L.L.; Lowry, K.P.; Otvos, J.D.; Kraus, W.E.; Svetkey, P.L. Effects of exercise on lipoprotein particles in women with polycystic ovary syndrome. Med. Sci. Sports Exerc. 2009, 41, 497–504. [Google Scholar] [CrossRef]
- Stener-Victorin, E.; Jedel, E.; Janson, P.O.; Sverrisdottir, Y.B. Low-frequency electroacupuncture and physical exercise decrease high muscle sympathetic nerve activity in polycystic ovary syndrome. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 297, R387–R395. [Google Scholar] [CrossRef]
- Stener-Victorin, E.; Baghaei, F.; Holm, G.; Janson, P.O.; Olivecrona, G.; Lönn, M.; Mannerås-Holm, L. Effects of acupuncture and exercise on insulin sensitivity, adipose tissue characteristics, and markers of coagulation and fibrinolysis in women with polycystic ovary syndrome: Secondary analyses of a randomized controlled trial. Fertil. Steril. 2012, 97, 501–508. [Google Scholar] [CrossRef]
- Leonhardt, H.; Hellström, M.; Gull, B.; Lind, A.K.; Nilsson, L.; Janson, P.O.; Stener-Victorin, E. Serum anti-Müllerian hormone and ovarian morphology assessed by magnetic resonance imaging in response to acupuncture and exercise in women with polycystic ovary syndrome: Secondary analyses of a randomized controlled trial. Acta Obstet. Gynecol. Scand. 2015, 94, 279–287. [Google Scholar] [CrossRef]
- Jedel, E.; Labrie, F.; Odén, A.; Holm, G.; Nilsson, L.; Janson, P.O.; Lind, A.K.; Ohlsson, C.; Stener-Victorin, E. Impact of electro-acupuncture and physical exercise on hyperandrogenism and oligo/amenorrhea in women with polycystic ovary syndrome: A randomized controlled trial. Am. J. Physiol. Metab. 2011, 300, E37–E45. [Google Scholar] [CrossRef]
- Palomba, S.; Giallauria, F.; Falbo, A.; Russo, T.; Oppedisano, R.; Tolino, A.; Colao, A.; Vigorito, C.; Zullo, F.; Orio, F. Structured exercise training programme versus hypocaloric hyperproteic diet in obese polycystic ovary syndrome patients with anovulatory infertility: A 24-week pilot study. Hum. Reprod. 2008, 23, 642–650. [Google Scholar] [CrossRef]
- Moran, L.J.; Harrison, C.L.; Hutchison, S.K.; Stepto, N.K.; Strauss, B.J.; Teede, H.J. Exercise decreases anti-müllerian hormone in anovulatory overweight women with polycystic ovary syndrome: A pilot study. Horm. Metab. Res. 2011, 43, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, S.K.; Stepto, N.K.; Harrison, C.L.; Moran, L.J.; Strauss, B.J.; Teede, H.J. Effects of exercise on insulin resistance and body composition in overweight and obese women with and without polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2011, 96, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Stepto, N.K.; Hiam, D.; Gibson-Helm, M.; Cassar, S.; Harrison, C.L.; Hutchison, S.K.; Joham, A.E.; Canny, B.J.; Moreno-Asso, A.; Strauss, B.J.; et al. Exercise and insulin resistance in PCOS: Muscle insulin signalling and fibrosis. Endocr. Connect. 2020, 9, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, S.K.; Teede, H.J.; Rachoń, D.; Harrison, C.L.; Strauss, B.J.; Stepto, N.K. Effect of exercise training on insulin sensitivity, mitochondria and computed tomography muscle attenuation in overweight women with and without polycystic ovary syndrome. Diabetologia 2012, 55, 1424–1434. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Teede, H.J.; Rachoń, D.; Harrison, C.L.; Strauss, B.J.; Stepto, N.K. Exploring factors related to changes in body composition, insulin sensitivity and aerobic capacity in response to a 12-week exercise intervention in overweight and obese women with and without polycystic ovary syndrome. PLoS ONE 2017, 12, e0182412. [Google Scholar] [CrossRef]
- Moro, C.; Pasarica, M.; Elkind-Hirsch, K.; Redman, L.M. Aerobic exercise training improves atrial natriuretic peptide and catecholamine-mediated lipolysis in obese women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2009, 94, 2579–2586. [Google Scholar] [CrossRef]
- Redman, L.M.; Elkind-Hirsch, K.; Ravussin, E. Aerobic exercise in women with polycystic ovary syndrome improves ovarian morphology independent of changes in body composition. Fertil. Steril. 2011, 95, 2696–2699. [Google Scholar] [CrossRef]
- Covington, J.D.; Tam, C.S.; Pasarica, M.; Redman, L.M. Higher circulating leukocytes in women with PCOS is reversed by aerobic exercise. Biochimie 2014, 124, 27–33. [Google Scholar] [CrossRef]
- Sprung, V.S.; Cuthbertson, D.J.; Pugh, C.J.; Aziz, N.; Kemp, G.J.; Daousi, C.; Green, D.J.; Cable, N.T.; Jones, H. Exercise training in polycystic ovarian syndrome enhances flow-mediated dilation in the absence of changes in fatness. Med. Sci. Sports Exerc. 2013, 45, 2234–2242. [Google Scholar] [CrossRef]
- Sprung, V.S.; Cuthbertson, D.J.; Pugh, C.J.; Daousi, C.; Atkinson, G.; Aziz, N.F.; Kemp, G.J.; Green, D.J.; Cable, N.T.; Jones, H. Nitric oxide-mediated cutaneous microvascular function is impaired in polycystic ovary sydrome but can be improved by exercise training. J. Physiol. 2013, 591, 1475–1487. [Google Scholar] [CrossRef]
- Aye, M.M.; Butler, A.E.; Kilpatrick, E.S.; Kirk, R.; Vince, R.; Rigby, A.S.; Sandeman, D.; Atkin, S.L. Dynamic Change in Insulin Resistance Induced by Free Fatty Acids Is Unchanged Though Insulin Sensitivity Improves Following Endurance Exercise in PCOS. Front. Endocrinol. 2018, 9, 592. [Google Scholar] [CrossRef] [PubMed]
- Halama, A.; Aye, M.M.; Dargham, S.R.; Kulinski, M.; Suhre, K.; Atkin, S.L. Metabolomics of Dynamic Changes in Insulin Resistance Before and After Exercise in PCOS. Front. Endocrinol. 2019, 10, 116. [Google Scholar] [CrossRef] [PubMed]
- Randeva, H.S.; Lewandowski, K.C.; Drzewoski, J.; Brooke-Wavell, K.; O’Callaghan, C.; Czupryniak, L.; Hillhouse, E.W.; Prelevic, G.M. Exercise decreases plasma total homocysteine in overweight young women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2002, 87, 4496–4501. [Google Scholar] [CrossRef] [PubMed]
- Joham, A.E.; Teede, H.J.; Hutchison, S.K.; Stepto, N.K.; Harrison, C.L.; Strauss, B.J.; Paul, E.; Watt, M.J. Pigment epithelium-derived factor, insulin sensitivity, and adiposity in polycystic ovary syndrome: Impact of exercise training. Obesity 2012, 20, 2390–2396. [Google Scholar] [CrossRef] [PubMed]
- Almenning, I.; Rieber-Mohn, A.; Lundgren, K.M.; Shetelig Løvvik, T.; Garnæs, K.K.; Moholdt, T. Effects of High Intensity Interval Training and Strength Training on Metabolic, Cardiovascular and Hormonal Outcomes in Women with Polycystic Ovary Syndrome: A Pilot Study. PLoS ONE 2015, 10, e0138793. [Google Scholar] [CrossRef] [PubMed]
- Aktaş, H.; Uzun, Y.E.; Kutlu, O.; Pençe, H.H.; Özçelik, F.; Çil, E.; Irak, L.; Altun, Ö.; Özcan, M.; Özsoy, N.; et al. The effects of high intensity-interval training on vaspin, adiponectin and leptin levels in women with polycystic ovary syndrome. Arch. Physiol. Biochem. 2019, 1–6. [Google Scholar] [CrossRef]
- Samadi, Z.; Bambaeichi, E.; Valiani, M.; Shahshahan, Z. Evaluation of Changes in Levels of Hyperandrogenism, Hirsutism and Menstrual Regulation After a Period of Aquatic High Intensity Interval Training in Women with Polycystic Ovary Syndrome. Int. J. Prev. Med. 2019, 10, 187. [Google Scholar]
- Bruner, B.; Chad, K.; Chizen, D. Effects of exercise and nutritional counseling in women with polycystic ovary syndrome. Appl. Physiol. Nutr. Metab. 2006, 31, 384–391. [Google Scholar] [CrossRef]
- Thomson, R.L.; Buckley, J.D.; Noakes, M.; Clifton, P.M.; Norman, R.J.; Brinkworth, G.D. The effect of a hypocaloric diet with and without exercise training on body composition, cardiometabolic risk profile, and reproductive function in overweight and obese women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2008, 93, 3373–3380. [Google Scholar] [CrossRef]
- Nybacka, Å.; Carlström, K.; Fabri, F.; Hellström, P.M.; Hirschberg, A.L. Serum antimüllerian hormone in response to dietary management and/or physical exercise in overweight/obese women with polycystic ovary syndrome: Secondary analysis of a randomized controlled trial. Fertil. Steril. 2013, 100, 1096–1102. [Google Scholar] [CrossRef]
- Nybacka, Å.; Hellström, P.M.; Hirschberg, A.L. Increased fibre and reduced trans fatty acid intake are primary predictors of metabolic improvement in overweight polycystic ovary syndrome-Substudy of randomized trial between diet, exercise and diet plus exercise for weight control. Clin. Endocrinol. 2017, 87, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Turan, V.; Mutlu, E.K.; Solmaz, U.; Ekin, A.; Tosun, O.; Tosun, G.; Mat, E.; Gezer, C.; Malkoc, M. Benefits of short-term structured exercise in non-overweight women with polycystic ovary syndrome: A prospective randomized controlled study. J. Phys. Ther. Sci. 2015, 27, 2293–2297. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, N.; Pasrija, S.; Jain, S. Randomised controlled trial to study the efficacy of exercise with and without metformin on women with polycystic ovary syndrome. Eur. J. Obstet. Gynecol. Reprod. Boil. 2019, 234, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Legro, R.S. Obesity and PCOS: Implications for diagnosis and treatment. Semin. Reprod. Med. 2012, 30, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Furtado, C.L.; Ramos, F.K.; Kogure, G.S.; Santana-Lemos, B.A.; Ferriani, R.A.; Calado, R.T.; Dos Reis, R.M. A Nonrandomized Trial of Progressive Resistance Training Intervention in Women With Polycystic Ovary Syndrome and Its Implications in Telomere Content. Reprod. Sci. 2015, 23, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Kogure, G.S.; Silva, R.C.; Miranda-Furtado, C.L.; Ribeiro, V.B.; Pedroso, D.C.C.; Melo, A.S.; Ferriani, R.A.; Reis, R.M.D. Hyperandrogenism Enhances Muscle Strength After Progressive Resistance Training, Independent of Body Composition, in Women With Polycystic Ovary Syndrome. J. Strength Cond. Res. 2018, 32, 2642–2651. [Google Scholar] [CrossRef]
- Kogure, G.S.; Miranda-Furtado, C.L.; Pedroso, D.C.C.; Ribeiro, V.B.; Eiras, M.C.; Silva, R.C.; Caetano, L.C.; Ferriani, R.A.; Calado, R.T.; Dos Reis, R.M. Effects of Progressive Resistance Training on Obesity Indices in Polycystic Ovary Syndrome and the Relationship With Telomere Length. J. Phys. Act. Health 2019, 16, 601–607. [Google Scholar] [CrossRef]
- Ramos, F.K.; Lara, L.A.; Kogure, G.S.; Silva, R.C.; Ferriani, R.A.; Silva de Sá, M.F.; Reis, R.M. Quality of Life in Women with Polycystic Ovary Syndrome after a Program of Resistance Exercise Training. Rev. Bras. Ginecol. Obstet. 2016, 38, 340–347. [Google Scholar] [CrossRef]
- Nidhi, R.; Padmalatha, V.; Nagarathna, R.; Ram, A. Effect of a yoga program on glucose metabolism and blood lipid levels in adolescent girls with polycystic ovary syndrome. Int. J. Gynaecol. Obstet. 2012, 118, 37–41. [Google Scholar] [CrossRef]
- Patel, V.; Menezes, H.; Menezes, C.; Bouwer, S.; Bostick-Smith, C.A.; Speelman, D.L. Regular Mindful Yoga Practice as a Method to Improve Androgen Levels in Women With Polycystic Ovary Syndrome: A Randomized, Controlled Trial. J. Am. Osteopath. Assoc. 2020, 120, 323–335. [Google Scholar] [CrossRef]
- Dantas, W.S.; Marcondes, J.A.; Shinjo, S.K.; Perandini, L.A.; Zambelli, V.O.; Neves, W.D.; Barcellos, C.R.; Rocha, M.P.; Dos Reis Vieira Yance, V.; Pereira, R.T.; et al. GLUT4 translocation is not impaired after acute exercise in skeletal muscle of women with obesity and polycystic ovary syndrome. Obesity 2015, 23, 2207–2215. [Google Scholar] [CrossRef] [PubMed]
- Giallauria, F.; Palomba, S.; Manguso, F.; Vitelli, A.; Maresca, L.; Tafuri, D.; Lombardi, G.; Colao, A.; Vigorito, C.; Orio, F. Abnormal heart rate recovery after maximal cardiopulmonary exercise stress testing in young overweight women with polycystic ovary syndrome. Clin. Endocrinol. 2008, 68, 88–93. [Google Scholar] [CrossRef] [PubMed]
- El-Halawaty, S.; Rizk, A.; Kamal, M.; Aboulhassan, M.; Al-Sawah, H.; Noah, O.; Al-Inany, H. Clinical significance of serum concentration of anti-Müllerian hormone in obese women with polycystic ovary syndrome. Reprod. Biomed. Online 2007, 15, 495–499. [Google Scholar] [CrossRef]
- Álvarez-Blasco, F.; Luque-Ramírez, M.; Escobar-Morreale, H.F. Diet composition and physical activity in overweight and obese premenopausal women with or without polycystic ovary syndrome. Gynecol. Endocrinol. 2011, 27, 978–981. [Google Scholar] [CrossRef] [PubMed]
- Mario, F.M.; Graff, S.K.; Spritzer, P.M. Habitual physical activity is associated with improved anthropometric and androgenic profile in PCOS: A cross-sectional study. J. Endocrinol. Investig. 2016, 40, 377–384. [Google Scholar] [CrossRef]
- Moran, L.J.; Brown, W.J.; McNaughton, S.A.; Joham, A.E.; Teede, H.J. Weight management practices associated with PCOS and their relationships with diet and physical activity. Hum. Reprod. 2017, 32, 669–678. [Google Scholar] [CrossRef]
- Greenwood, E.A.; Noel, M.W.; Kao, C.N.; Shinkai, K.; Pasch, L.A.; Cedars, M.I.; Huddleston, H.G. Vigorous exercise is associated with superior metabolic profiles in polycystic ovary syndrome independent of total exercise expenditure. Fertil. Steril. 2016, 105, 486–493. [Google Scholar] [CrossRef]
- Eleftheriadou, M.; Michala, L.; Stefanidis, K.; Iliadis, I.; Lykeridou, A.; Antsaklis, A. Exercise and sedentary habits among adolescents with PCOS. J. Pediatr. Adolesc. Gynecol. 2012, 25, 172–174. [Google Scholar] [CrossRef]
- Barr, S.; Hart, K.; Reeves, S.; Sharp, K.; Jeanes, Y.M. Habitual dietary intake, eating pattern and physical activity of women with polycystic ovary syndrome. Eur. J. Clin. Nutr. 2011, 65, 1126–1132. [Google Scholar] [CrossRef]
- Banting, L.K.; Gibson-Helm, M.; Polman, R.; Teede, H.J.; Stepto, N.K. Physical activity and mental health in women with polycystic ovary syndrome. BMC Womens Health 2014, 14, 51. [Google Scholar] [CrossRef]
- Cramer, H.; Haller, H.; Dobos, G.; Lauche, R. A Systematic Review and Meta-Analysis Estimating the Expected Dropout Rates in Randomized Controlled Trials on Yoga Interventions. Evid. Based Complement. Altern. Med. 2016, 2016, 5859729. [Google Scholar] [CrossRef] [PubMed]

| 1990 National Institutes of Health (NIH) Criteria | Rotterdam Criteria | Androgen Excess Criteria |
|---|---|---|
| Demonstrates both: Clinical and/or biochemical hyperandrogenism Oligo- or anovulation | Demonstrates at least two of three: Clinical and/or biochemical hyperandrogenism Oligo- or anovulation Polycystic ovaries | Demonstrates: Hirsutism and/or hyperandrogenemia Also demonstrates at least one: Oligo- or anovulation Polycystic ovaries |
| Plus: Exclusion of other causes of androgen excess and anovulatory infertility | Plus: Exclusion of other causes of androgen excess and anovulatory infertility | Plus: Exclusion of other causes of androgen excess and anovulatory infertility |
| Study | Participants | Exercise Intervention | Hormonal Changes | Unchanged |
|---|---|---|---|---|
| Prospective, intensified aerobic ex., case-control [115] Trial ISRCTN84763265 | 20 PCOS, 14 non-PCOS; 20–40 y, BMI > 27; NIH criteria | 12-week intensified aerobic ex; 3 h/wk; added 8-week HIIT on treadmill, mod. intensity: 70% VO2max or 75–85% HRmax, HIIT: 6x 5 min intervals 95–100% VO2max or HRmax, 2 min rest, up to 8 reps and rest down to 1 min by 8 wk; HRM | ↑GIR | PEDF |
| RCT w/3 parallel arms (HIIT, ST, no ex) [116] Trial NCT01919281 | 31 PCOS (~10/group); 27.2 ± 5.5 y; BMI 26.7 ± 6; Rotterdam criteria | 10-week HIIT or ST; 3 d/wk; HIIT: 2 d/wk of 4 × 4 min at 90–95% HRmax w/ 3 min mod. II at 70% HRmax, plus 1 d/wk 10× 1 min at max intensity w/1 min rest/low II; walking/running and/or cycling; at least 1 d/wk supervised; HRM; ST: 8 dynamic drills at 75% resistance of 1 RM, 3× 10 reps w/1 min rests | ↓FI, HOMA-IR (HIIT) ↓DHEA-S (HIIT) ↓FAI, AMH (ST) ↑SHBG (ST) | T, APN, Leptin |
| Nonrandomized, HIIT or MICT [117] | 20 PCOS (10/group); mean age 25 y; BMI 21.2–41.6; Rotterdam criteria | 12-week HIIT or MICT program; 3 d/wk for 30 min; HIIT: 2 min run, 2 min walk; MICT: run at mod. tempo, constant speed | ↓FI (HIIT) ↑APN (HIIT) Trended in MICT | Leptin, vaspin |
| RCT w/2 arms (aquatic HIIT+met, met) [118] | 30 PCOS (15/group); 20–35 y; BMI ≥ 30; Rotterdam criteria | 12-week aquatic HIIT; 3 d/wk for 30 min with 4 × 4min intervals, each with 8 rounds of 20 s max II w/10 s rest, and 1 min rest between each 4 min bout; HRM | ↓LH, ↑FSH ↑SHBG ↓fT, TT, FAI, DHEA-S ↓HOMA-IR | N/A (hormones) |
| RCT w/2 arms (diet or diet+ex) [119] | 5 PCOS (diet), 7 PCOS (diet+ex); mean BMI 36.6; Rotterdam criteria | 12-week aerobic and resistance ex; 3 d/wk for 30 min at 70–85% HRmax plus 12 resistance ex of 2 × 10 reps progressing to 3 × 15 reps, increasing wt 5%; total of 90 min sessions; supervised | ↓FI (both groups) | LH:FSH T, FAI, SHBG |
| RCT w/3 parallel arms (diet, diet and aerobic ex., diet and aerobic-resistance ex) [120] | 94 PCOS (~30/group); 29.3 ± 0.7 y; BMI 36.1 ± 0.5; Rotterdam criteria | 20-week walking/jogging program 5 d/wk or walking/jogging 3 d/wk plus PRT 2 d/wk on nonconsecutive days; | ↓FI, HOMA-IR (both ex. groups, 10 wk; all at 20 wk) ↓T (both ex. groups, 10, 20 wk) ↓FAI (all at 10, 20 wk) ↑SHBG (both ex. groups, 10, 20 wk) | N/A (hormones) |
| RCT w/3 arms (diet, ex, diet+ex) [121,122] Trial ISRCTN48342048 | 57 PCOS (19/group); 18–40 y; BMI > 27; Rotterdam criteria | 4-month individualized moderate exercise (aerobic and strength training); moderate to high intensity; 2–3 d/wk; 45–60 min; physiotherapist supervised | N/A (hormones) | LH, FSH T, fT, SHBG AMH FI, HOMA-IR, IGF-1 |
| RCT w/2 arms, ex or no ex [123] | 32 PCOS (16/group); BMI < 25; Rotterdam criteria | 8-week aerobic and resistance ex; 3 d/wk for 50–60 min; treadmill and step, resistance band; supervised by physiotherapist | ↓FI, HOMA-IR | FSH, LH E2, TT, fT |
| RCT w/2 arms (ex or ex+met) [124] | 66 PCOS; 24.4 ± 4.3 y; BMI 26 ± 4; Rotterdam criteria | 6-month marching in place; 3 d/wk for 30 min; monitored by investigator for first 3 months to ensure HR ≥ 120 bpm | N/A (hormones) | T |
| Study | Participants | Exercise Intervention | Hormonal Changes | Unchanged |
|---|---|---|---|---|
| Nonrandomized, case-control [126,127,128] Brazilian Clinical Trials Registry (ReBec: RBR-7p23c3) | 45 PCOS, 52 non-PCOS; 18–37 y; Rotterdam criteria | 4-month PRT; 3 d/wk of PRT for 1h w/microcycles of increasing intensity, decreasing reps (linear periodization) | ↑PRL ↑A4 ↓T, FAI ↓SHBG | FSH, LH E2 FI, HOMA-IR |
| Prospective, case-control, PRT [129] | 43 PCOS, 51 non-PCOS; sedentary; 18–37 y; BMI 18–39.9; Rotterdam criteria | 16-week PRT; 4 microcycles of 4 wk w/linear periodization; 10 ex w/10 reps/ex; supervised | ↓T ↑A4 | N/A (hormones) |
| Study | Participants | Exercise Intervention | Hormonal Changes | Unchanged |
|---|---|---|---|---|
| RCT w/2 arms (yoga, CE) [130] Central Trial Registry of India No.: REFCTRI-2008 000291 | 90 PCOS; 15-18 y; mean BMI 20.8; Rotterdam criteria | 12-week supervised yoga or CE; 90 sessions total of 1 h; yoga: surya namaskara, asanas, pranayama, relaxation, meditation; CE: walking, standing, sitting, supine ex w/no yogic concepts or breathing | ↓FI, HOMA-IR (yoga) ↓LH (yoga) ↓TT (yoga) ↓AMH (yoga, CE) | FSH, PRL |
| RCT w/3 arms (yoga, OMT, no ex) [131] Trial NCT03383484 | 22 PCOS (13 yoga, 9 no ex); 22–43 y; BMI 20–48; Rotterdam criteria | 3-month supervised mindful yoga; 3 d/wk for 1 h; yoga: pranayama, vinyasa flows, restorative asanas, mindfulness, meditation; follow-up 3 mo post-study | ↓fT (yoga, persisted 3 mo) ↓APN DHEA trended lower | DHEA-S, A4FI, HOMA-IR |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shele, G.; Genkil, J.; Speelman, D. A Systematic Review of the Effects of Exercise on Hormones in Women with Polycystic Ovary Syndrome. J. Funct. Morphol. Kinesiol. 2020, 5, 35. https://doi.org/10.3390/jfmk5020035
Shele G, Genkil J, Speelman D. A Systematic Review of the Effects of Exercise on Hormones in Women with Polycystic Ovary Syndrome. Journal of Functional Morphology and Kinesiology. 2020; 5(2):35. https://doi.org/10.3390/jfmk5020035
Chicago/Turabian StyleShele, Grei, Jessica Genkil, and Diana Speelman. 2020. "A Systematic Review of the Effects of Exercise on Hormones in Women with Polycystic Ovary Syndrome" Journal of Functional Morphology and Kinesiology 5, no. 2: 35. https://doi.org/10.3390/jfmk5020035
APA StyleShele, G., Genkil, J., & Speelman, D. (2020). A Systematic Review of the Effects of Exercise on Hormones in Women with Polycystic Ovary Syndrome. Journal of Functional Morphology and Kinesiology, 5(2), 35. https://doi.org/10.3390/jfmk5020035