Combination of Suicide and Cytokine Gene Therapies as Surgery Adjuvant for Canine Mammary Carcinoma


Abstract
1. Introduction
2. Materials and Methods
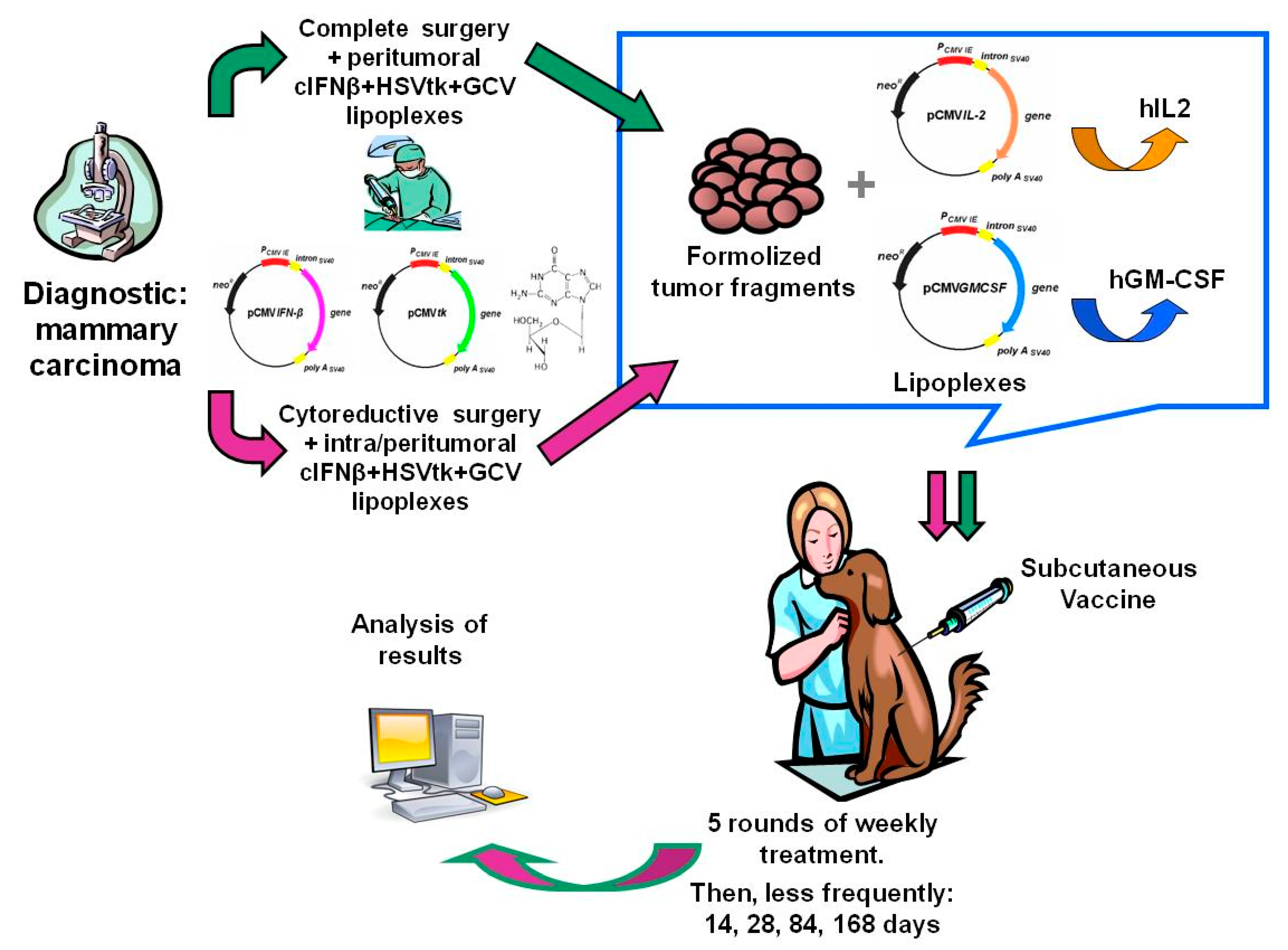
2.1. Plasmids
2.2. Liposomes Preparation and Local Lipoplexes Injection
2.3. Tumor Vaccines Preparation
2.4. Patients
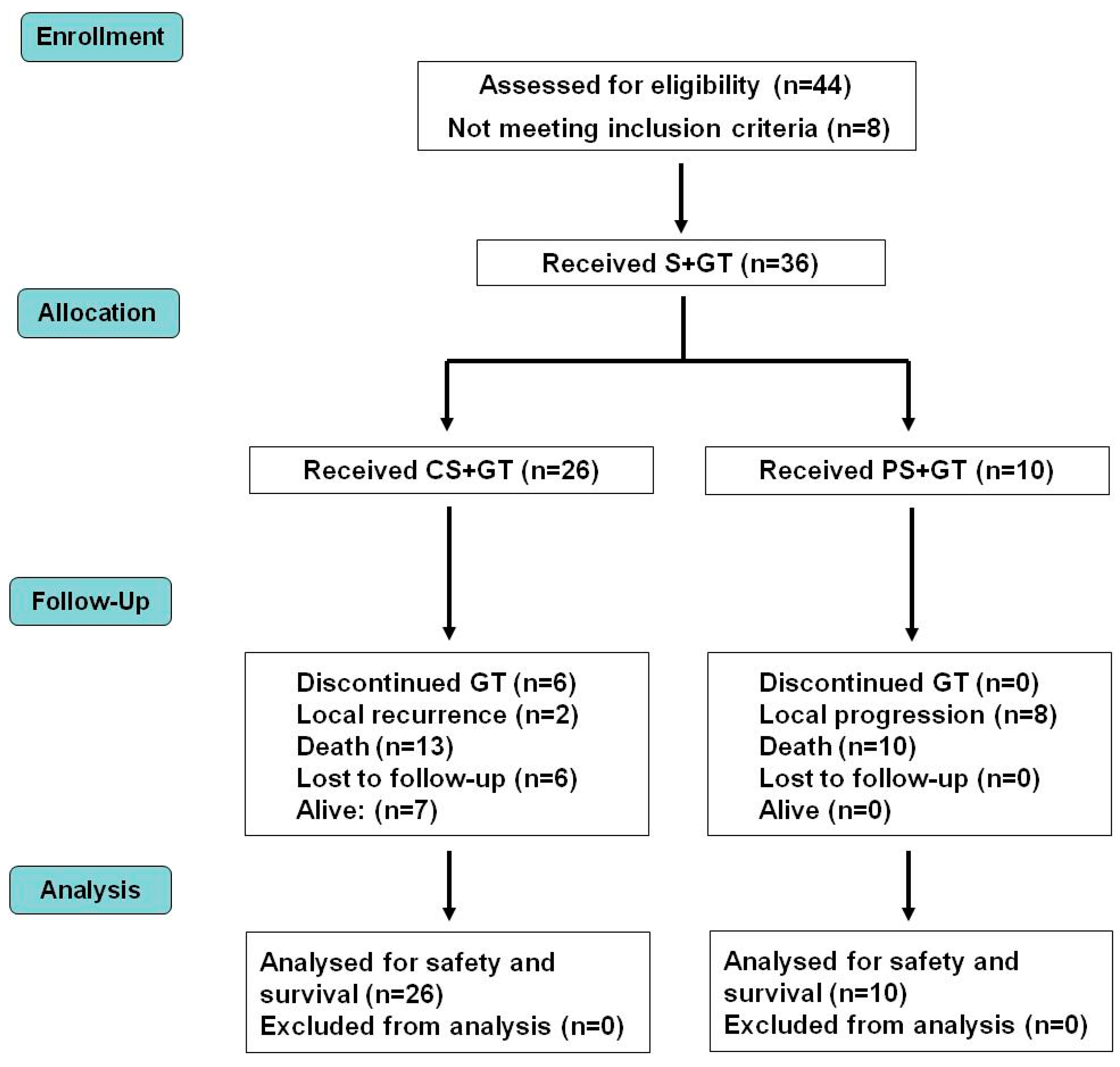
2.5. Study Design and Treatment
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sleeckx, N.; de Rooster, H.; VeldhuisKroeze, E.J.; Van Ginneken, C.; Van Brantegem, L. Canine mammary tumours, an overview. Reprod. Domest. Anim. 2011, 46, 1112–1131. [Google Scholar] [CrossRef] [PubMed]
- Goldschmidt, M.; Peña, L.; Rasotto, R.; Zappulli, V. Classification and grading of canine mammary tumors. Vet. Pathol. 2011, 48, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Pinho, S.S.; Carvalho, S.; Cabral, J.; Reis, C.A.; Gärtner, F. Canine tumors: A spontaneous animal model of human carcinogenesis. Transl. Res. 2012, 159, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, F.; Peña, L.; Ibisch, C.; Loussouarn, D.; Gama, A.; Rieder, N.; Belousov, A.; Campone, M.; Abadie, J. Canine invasive mammary carcinomas as models of human breast cancer. Part 1: Natural history and prognostic factors. Breast Cancer Res. Treat. 2018, 167, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Abadie, J.; Nguyen, F.; Loussouarn, D.; Peña, L.; Gama, A.; Rieder, N.; Belousov, A.; Bemelmans, I.; Jaillardon, L.; Ibisch, C.; Campone, M. Canine invasive mammary carcinomas as models of human breast cancer. Part 2: Immunophenotypes and prognostic significance. Breast Cancer Res. Treat. 2018, 167, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Matos, A.J.; Santos, A.A. Advances in the understanding of the clinically relevant genetic pathways and molecular aspects of canine mammary tumours: Part 1. Proliferation, apoptosis and DNA repair. Vet. J. 2015, 205, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.A.; Matos, A.J. Advances in the understanding of the clinically relevant genetic pathways and molecular aspects of canine mammary tumours. Part 2: Invasion, angiogenesis, metastasis and therapy. Vet. J. 2015, 205, 144–153. [Google Scholar] [CrossRef] [PubMed]
- LutfulKabir, F.M.; Alvarez, C.E.; Bird, R.C. Canine Mammary Carcinomas: A Comparative Analysis of Altered Gene Expression. Vet. Sci. 2015, 3. [Google Scholar] [CrossRef]
- Glikin, G.C.; Finocchiaro, L.M. Clinical trials of immunogene therapy for spontaneous tumors in companion animals. Sci. World J. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, L.M.; Glikin, G.C. Recent clinical trials of cancer immunogene therapy in companion animals. World J. Exp. Med. 2017, 7, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Cemazar, M.; Sersa, G.; Pavlin, D.; Tozon, N. Intramuscular IL-12 electrogene therapy for treatment of spontaneous canine tumors. In Targets in Gene Therapy; You, Y., Ed.; InTech: Rijeka, Croatia, 2011; pp. 299–320. ISBN 978-953-307-540-2. [Google Scholar]
- Cicchelero, L.; Denies, S.; Haers, H.; Vanderperren, K.; Stock, E.; Van Brantegem, L.; de Rooster, H.; Sanders, N.N. Intratumoural interleukin 12 gene therapy stimulates the immune system and decreases angiogenesis in dogs with spontaneous cancer. Vet. Comp. Oncol. 2017, 15, 1187–1205. [Google Scholar] [CrossRef] [PubMed]
- Gabai, V.; Venanzi, F.M.; Bagashova, E.; Rud, O.; Mariotti, F.; Vullo, C.; Catone, G.; Sherman, M.Y.; Concetti, A.; Chursov, A.; et al. Pilot study of p62 DNA vaccine in dogs with mammary tumors. Oncotarget 2014, 5, 12803–12810. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, L.M.; Fondello, C.; Gil-Cardeza, M.L.; Rossi, Ú.; Villaverde, M.S.; Riveros, M.D.; Glikin, G.C. Cytokine-Enhanced Vaccine and Interferon-β plus Suicide Gene Therapy as Surgery Adjuvant Treatments for Spontaneous Canine Melanoma. Hum. Gene Ther. 2015, 26, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, L.M.; Villaverde, M.S.; Gil-Cardeza, M.L.; Riveros, M.D.; Glikin, G.C. Cytokine-enhanced vaccine and interferon-β plus suicide gene as combined therapy for spontaneous canine sarcomas. Res. Vet. Sci. 2011, 91, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, L.M.E.; Spector, A.; Rossi, U.A.; Gil-Cardeza, M.L.; Suarez, J.L.; Riveros, M.D.; Villaverde, M.S.; Glikin, G.C. The potential of suicide plus immune gene therapy for treating osteosarcoma: The experience on canine veterinary patients. In Sarcoma: Symptoms, Causes and Treatments; Butler, E.J., Ed.; Nova Science Publishers: New York, NY, USA, 2012; pp. 107–122. ISBN 978-1-62100-362-5. [Google Scholar]
- Finocchiaro, L.M.; Glikin, G.C. Cytokine-enhanced vaccine and suicide gene therapy as surgery adjuvant treatments for spontaneous canine melanoma: 9 years of follow-up. Cancer Gene Ther. 2012, 19, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Thamm, D.H.; Kurzman, I.D.; Clark, M.A.; Ehrhart, E.J., 3rd; Kraft, S.L.; Gustafson, D.L.; Vail, D.M. Preclinical investigation of PEGylated tumor necrosis factor alpha in dogs with spontaneous tumors: Phase I evaluation. Clin. Cancer Res. 2010, 16, 1498–1508. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [PubMed]
- Veterinary Co-operative Oncology Group (VCOG). Veterinary Co-Operative Oncology Group—Common Terminology Criteria for Adverse Events (VCOG-CTCAE) following chemotherapy or biological antineoplastic therapy in dogs and cats v1.0. Vet. Comp. Oncol. 2004, 2, 195–213. [Google Scholar] [CrossRef] [PubMed]
- Szczubiał, M.; Łopuszynski, W. Prognostic value of regional lymph node status in canine mammary carcinomas. Vet. Comp. Oncol. 2011, 9, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Betz, D.; Schoenrock, D.; Mischke, R.; Baumgärtner, W.; Nolte, I. Postoperative treatment outcome in canine mammary tumors. Multivariate analysis of the prognostic value of pre- and postoperatively available information. Tierarztl Prax Ausg K Kleintiere Heimtiere 2012, 40, 235–242. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| # | Breed | Initial Age (Years) | Stage | Surgery Type | Local Relapse | Cause of Death | Survival (Days) |
|---|---|---|---|---|---|---|---|
| 1 | Schnauzer | 9 | II | Complete | No | Alive | >306 |
| 2 | Cocker spaniel | 10 | II | Complete | No | Alive | >491 |
| 3 | Bichon frisé | 12 | II | Complete | No | Alive | >1498 |
| 4 | Mixed breed | 14 | II | Complete | Yes | Unrelated | 358 |
| 5 | Cocker spaniel | 13 | II | Complete | No | Unrelated | 422 |
| 6 | Beagle | 11 | II | Complete | No | Unrelated | 449 |
| 7 | Mixed breed | 13 | II | Complete | No | Unrelated | 496 |
| 8 | Doberman pinscher | 13 | II | Complete | No | Discontinued | >580 |
| 9 | Breton | 13 | II | Complete | No | Unrelated | 788 |
| 10 | Siberian husky | 13 | II | Complete | No | Discontinued | >1163 |
| 11 | Mixed breed | 12 | II | Complete | No | Unrelated | 1033 |
| 12 | Mixed breed | 9 | III | Complete | No | Alive | >273 |
| 13 | Pointer | 11 | III | Complete | No | Alive | >834 |
| 14 | Cocker spaniel | 12 | III | Complete | No | Alive | >935 |
| 15 | Boston terrier | 13 | III | Complete | No | Alive | >991 |
| 16 | Cocker spaniel | 13 | III | Complete | Yes | Related | 211 |
| 17 | Mixed breed | 10 | III | Partial | * Yes | Related * | 241 |
| 18 | German shepherd | 14 | III | Partial | * Yes | Related | 330 |
| 19 | Mixed breed | 11 | III | Partial | * Yes | Related | 352 |
| 20 | Mixed breed | 14 | III | Complete | No | Discontinued | >384 |
| 21 | Brittany | 11 | III | Complete | No | Discontinued | >575 |
| 22 | Mixed breed | 9 | III | Complete | No | Unrelated | 594 |
| 23 | Cocker spaniel | 12 | III | Partial | * Yes | Related | 708 |
| 24 | Cocker spaniel | 12 | III | Complete | No | Discontinued | >775 |
| 25 | Schnauzer | 11 | III | Complete | No | Unrelated | 869 |
| 26 | Rottweiler | 13 | III | Partial | * Yes | Unrelated | 876 |
| 27 | German shepherd | 8 | III | Partial | * Yes | Related | 932 |
| 28 | Mixed breed | 7 | III | Complete | No | Unrelated | 1234 |
| 29 | Cocker spaniel | 10 | III | Complete | No | Discontinued | >1345 |
| 30 | German shepherd | 11 | IV | Complete | No | Related | 99 |
| 31 | Mixed breed | 5 | IV | Complete | No | Related | 117 |
| 32 | German shepherd | 6 | IV | Partial | * Yes | Related * | 127 |
| 33 | Mixed breed | 15 | IV | Partial | * Yes | Related * | 170 |
| 34 | Rottweiler | 13 | IV | Partial | * Yes | Unrelated | 175 |
| 35 | Mixed breed | 11 | IV | Complete | No | Related * | 183 |
| 36 | German shepherd | 12 | IV | Partial | * Yes | Related * | 205 |
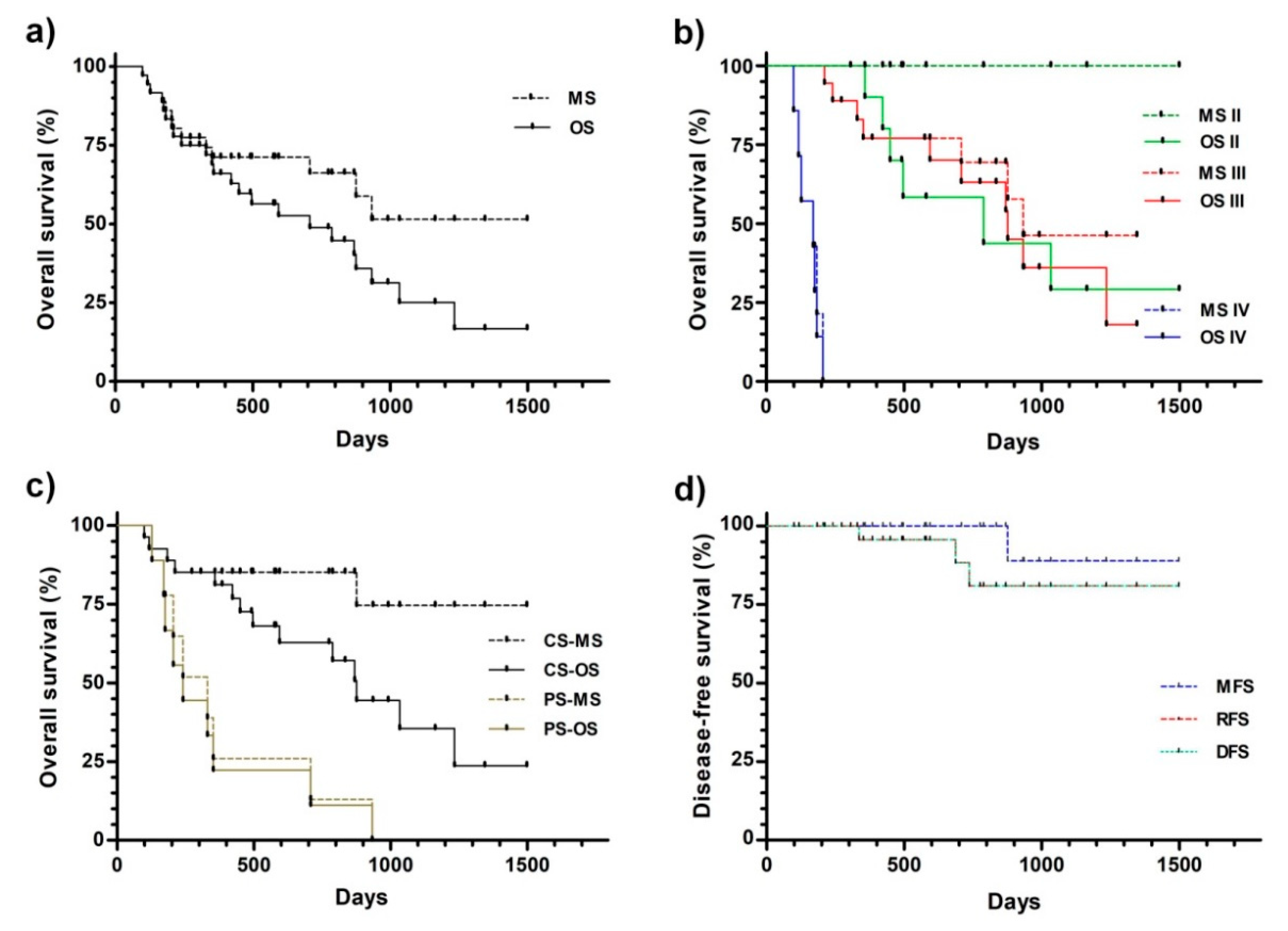
| Survival | n | Overall (to Any Cause): OS | Overall (to CMC): MS | OS vs. MS |
|---|---|---|---|---|
| All stages | 36 | 708 (99–498) | >1498 (99–1498) | NS |
| Stage II | 11 | 788 (306–1498) | >1498 (306–1498) | NS |
| Stage III | 18 | 876 (167–1345) | 932(167–1345) | NS |
| Stage IV | 7 | 170 (99–205) | 170 (99–205) | NS |
| Stage II vs. Stage III | NS | p < 0.0423 | - | |
| Stage II vs. Stage IV | p < 0.0001 | p < 0.0001 | ||
| Stage III vs. Stage IV | p < 0.0001 | p < 0.0001 | ||
| SURVIVAL (Days) | GT (n = 36) | CS vs. PS | |
|---|---|---|---|
| CS+GT (n = 26) | PS+GT (n = 10) | (p<) | |
| Overall (any cause): OS | 876 (99–498) | 241 (127–932) | 0.0006 |
| Overall (to CMC): MS | >1498 (99–1498) | 330 (127–932) | 0.0001 |
| Metastasis-free | Recurrence-free | Disease-free | |
| Survival (days) | >1498 (167–1498) | >1498 (99–1498) | >1498(99–1498) |
| Patients | GT (n = 36) | ||
|---|---|---|---|
| CS+GT (n = 26) | PS+GT (n = 10) | CS+GT vs. PS+GT | |
| n (%) | n (%) | p< | |
| Local disease-free | 24 (92.3) | 0 * (0) | 0.0001 |
| With local disease | 2 (7.7) | 10 * (100) | |
| Metastasis-free | 23 (88.5) | 6 (60.0) | NS |
| With metastasis | 3 (11.5) | 4 (40.0) | |
| Disease-free | 21 (80.8) | 0 * (0) | 0.0001 |
| With disease | 5 (19.2) | 10 (100) | |
| Alive | 7 (26.9) | 0 (0) | ND |
| Dead | 13 (50.0) | 10 (100) | |
| Dropped-out | 6 (23.1) | 0 (0) | |
| Death | n (%) | n (%) | p< |
| CMC-related | 4 (30.8) | 8 (80.0) | 0.0361 |
| CMC-unrelated | 9 (69.2) | 2 (20.0) | |
| # | Breed | Initial Age (Years) | Stage | Surgery Type | Local Relapse | Response to Additional Local GT | Cause of Death | Survival (Days) |
|---|---|---|---|---|---|---|---|---|
| 1 | Cocker spaniel | 8 | II | CS | Yes | PR | Alive | >2263 |
| 2 | German shepherd | 8 | II | CS | Yes | PR | Related | 325 |
| 3 | Mixed breed | 15 | II | CS | Yes | SD | Related | 365 |
| 4 | Golden retriever | 9 | III | CS | Yes | CR | Unrelated | 1263 |
| 5 | Mixed breed | 15 | IV | PS | * Yes | PR | Related | 167 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finocchiaro, L.M.E.; Spector, A.I.M.; Agnetti, L.; Arbe, M.F.; Glikin, G.C. Combination of Suicide and Cytokine Gene Therapies as Surgery Adjuvant for Canine Mammary Carcinoma. Vet. Sci. 2018, 5, 70. https://doi.org/10.3390/vetsci5030070
Finocchiaro LME, Spector AIM, Agnetti L, Arbe MF, Glikin GC. Combination of Suicide and Cytokine Gene Therapies as Surgery Adjuvant for Canine Mammary Carcinoma. Veterinary Sciences. 2018; 5(3):70. https://doi.org/10.3390/vetsci5030070
Chicago/Turabian StyleFinocchiaro, Liliana M. E., Agustina I. M. Spector, Lucrecia Agnetti, M. Florencia Arbe, and Gerardo C. Glikin. 2018. "Combination of Suicide and Cytokine Gene Therapies as Surgery Adjuvant for Canine Mammary Carcinoma" Veterinary Sciences 5, no. 3: 70. https://doi.org/10.3390/vetsci5030070
APA StyleFinocchiaro, L. M. E., Spector, A. I. M., Agnetti, L., Arbe, M. F., & Glikin, G. C. (2018). Combination of Suicide and Cytokine Gene Therapies as Surgery Adjuvant for Canine Mammary Carcinoma. Veterinary Sciences, 5(3), 70. https://doi.org/10.3390/vetsci5030070