
Correlating Access to Primary Medical Care and Veterinary Care Providers: A Novel Application of Spatial Gravity Modelling


{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Zoonoses
1.2. Floating Catchment Area Model
2. Materials and Methods
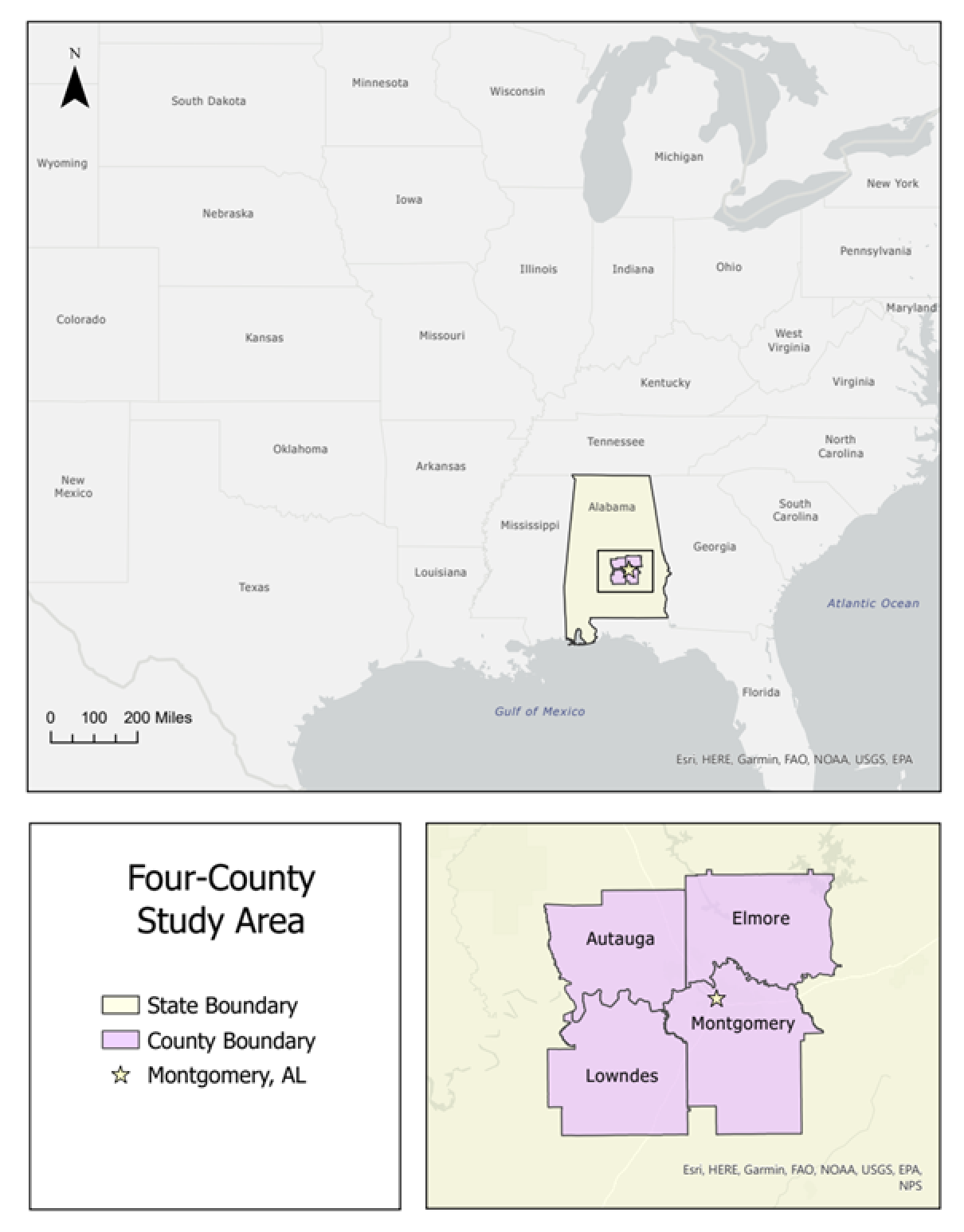
2.1. Study Area
2.2. Veterinary Service Supply
2.3. Human Health Care Service Supply
2.4. Enhanced Two-Step Floating Catchment Area Model
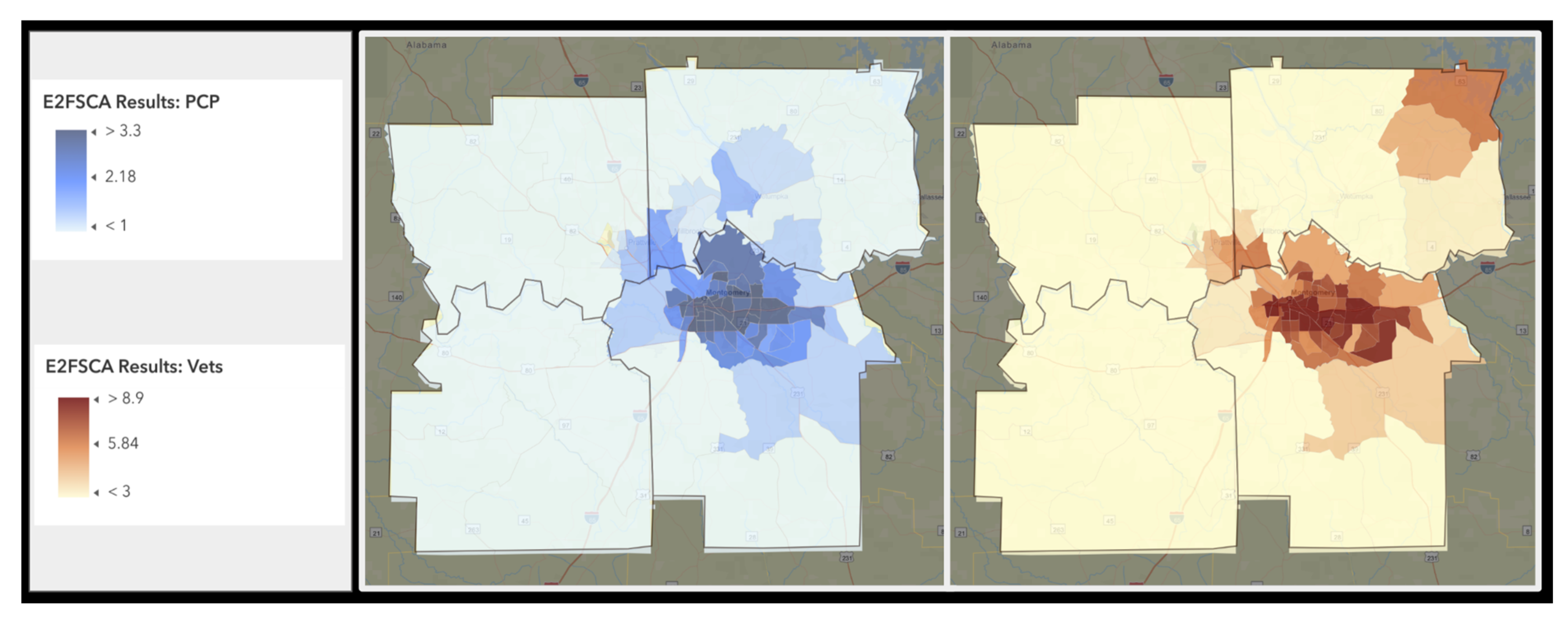
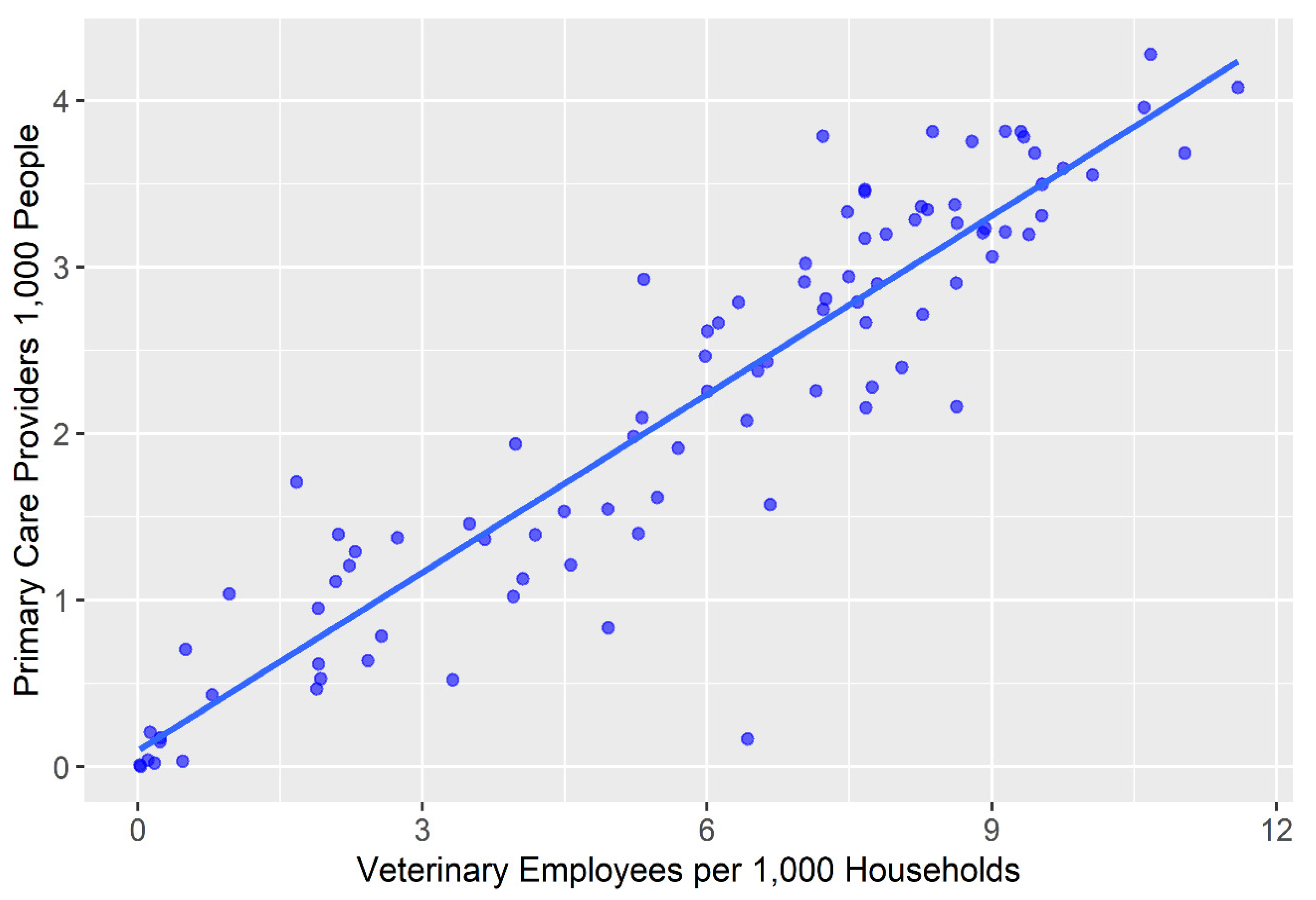
3. Results
4. Discussion
Limitations and Future Research
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- One Health|CDC. Available online: https://www.cdc.gov/onehealth/index.html (accessed on 31 July 2023).
- Primary Care. Available online: https://www.aafp.org/about/policies/all/primary-care.html (accessed on 2 August 2023).
- Veterinarians: Protecting the Health of Animals and People. Available online: https://www.avma.org/resources/pet-owners/yourvet/veterinarians-protecting-health-animals-and-people (accessed on 31 July 2023).
- Access to Veterinary Care: Barriers, Current Practices, and Public Policy. Available online: https://pphe.utk.edu/wp-content/uploads/2020/09/avcc-report.pdf (accessed on 5 January 2023).
- Hardt, N.S.; Muhamed, S.; Das, R.; Estrella, R.; Roth, J. Neighborhood-Level Hot Spot Maps to Inform Delivery of Primary Care and Allocation of Social Resources. Perm J. 2013, 17, 4–9. [Google Scholar] [CrossRef]
- Spencer, T.; Behar-Horenstein, L.; Aufmuth, J.; Hardt, N.; Applebaum, J.W.; Emanuel, A.; Isaza, N. Factors That Influence Intake to One Municipal Animal Control Facility in Florida: A Qualitative Study. Animals 2017, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Stull, J.W.; Brophy, J.; Weese, J.S. Reducing the Risk of Pet-Associated Zoonotic Infections. CMAJ 2015, 187, 736–743. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, J. Zoonotic Infections from Common Household Pets. J. Nurse Pract. 2018, 14, 363–370. [Google Scholar] [CrossRef]
- Chomel, B.B. Emerging and Re-Emerging Zoonoses of Dogs and Cats. Animals 2014, 4, 434–445. [Google Scholar] [CrossRef]
- Whitfield, Y.; Smith, A. Household pets and zoonoses. Environ. Health Rev. 2014, 57, 41–49. [Google Scholar] [CrossRef]
- Zahnd, W.E.; Del Vecchio, N.; Askelson, N.; Eberth, J.M.; Vanderpool, R.C.; Overholser, L.; Madhivanan, P.; Hirschey, R.; Edward, J. Definition and Categorization of Rural and Assessment of Realized Access to Care. Health Serv. Res. 2022, 57, 693–702. [Google Scholar] [CrossRef]
- Levesque, J.-F.; Harris, M.F.; Russell, G. Patient-Centred Access to Health Care: Conceptualising Access at the Interface of Health Systems and Populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef]
- Ng, K.Y.; Ho, C.L.; Koh, K. Spatial-Temporal Accessibility and Inequality of Veterinary Service in Hong Kong: A Geographic Information System-Based Study. Front. Vet. Sci. 2022, 9, 857914. [Google Scholar] [CrossRef]
- Neal, S.M.; Greenberg, M.J. Putting Access to Veterinary Care on the Map: A Veterinary Care Accessibility Index. Front. Vet. Sci. 2022, 9, 857644. [Google Scholar] [CrossRef]
- Amiri, S.; Espenschied, J.R.; Roll, J.M.; Amram, O. Access to Primary Care Physicians and Mortality in Washington State: Application of a 2-Step Floating Catchment Area. J. Rural. Health 2020, 36, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, E.; Son, H. The Human–Companion Animal Bond: How Humans Benefit. Vet. Clin. N. Am. Small Anim. Pract. 2009, 39, 293–326. [Google Scholar] [CrossRef] [PubMed]
- Wells, D.L. The State of Research on Human–Animal Relations: Implications for Human Health. Anthrozoös 2019, 32, 169–181. [Google Scholar] [CrossRef]
- Rault, J.-L.; Waiblinger, S.; Boivin, X.; Hemsworth, P. The Power of a Positive Human–Animal Relationship for Animal Welfare. Front. Vet. Sci. 2020, 7, 590867. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, M.J.; O’Reilly, A. Access to Veterinary Care–A National Family Crisis and Case for One Health. Adv. Small Anim. Care 2023, in press. [Google Scholar] [CrossRef]
- Guagliardo, M.F. Spatial Accessibility of Primary Care: Concepts, Methods and Challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef]
- Joseph, A.E.; Bantock, P.R. Measuring Potential Physical Accessibility to General Practitioners in Rural Areas: A Method and Case Study. Soc. Sci. Med. 1982, 16, 85–90. [Google Scholar] [CrossRef]
- Khan, A.A. An Integrated Approach to Measuring Potential Spatial Access to Health Care Services. Socio-Econ. Plan. Sci. 1992, 26, 275–287. [Google Scholar] [CrossRef]
- Radke, J.; Mu, L. Spatial Decompositions, Modeling and Mapping Service Regions to Predict Access to Social Programs. Geogr. Inf. Sci. 2000, 6, 105–112. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef]
- Luo, W.; Qi, Y. An Enhanced Two-Step Floating Catchment Area (E2SFCA) Method for Measuring Spatial Accessibility to Primary Care Physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Weibull, J.W. An Axiomatic Approach to the Measurement of Accessibility. Reg. Sci. Urban Econ. 1976, 6, 357–379. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Spatial Accessibility to Primary Care and Physician Shortage Area Designation: A Case Study in Illinois with GIS Approaches. In Geographic Information Systems and Health Applications; IGI Global: Hershey, PA, USA, 2003; pp. 260–278. [Google Scholar]
- Luo, J. Integrating the Huff Model and Floating Catchment Area Methods to Analyze Spatial Access to Healthcare Services. Trans. GIS 2014, 18, 436–448. [Google Scholar] [CrossRef]
- Yang, D.-H.; Goerge, R.; Mullner, R. Comparing GIS-Based Methods of Measuring Spatial Accessibility to Health Services. J Med. Syst. 2006, 30, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Lyu, H.; Zhao, Y.; Zhou, D. An Improved Two-Step Floating Catchment Area (2SFCA) Method for Measuring Spatial Accessibility to Elderly Care Facilities in Xi’an, China. Int. J. Environ. Res. Public Health 2022, 19, 11465. [Google Scholar] [CrossRef]
- Polo, G.; Acosta, C.M.; Dias, R.A. Spatial Accessibility to Vaccination Sites in a Campaign against Rabies in São Paulo City, Brazil. Prev. Vet. Med. 2013, 111, 10–16. [Google Scholar] [CrossRef]
- McGrail, M.R.; Humphreys, J.S. Measuring Spatial Accessibility to Primary Care in Rural Areas: Improving the Effectiveness of the Two-Step Floating Catchment Area Method. Appl. Geogr. 2009, 29, 533–541. [Google Scholar] [CrossRef]
- Berrada, M.; Ndiaye, Y.; Raboisson, D.; Lhermie, G. Spatial Evaluation of Animal Health Care Accessibility and Veterinary Shortage in France. Sci. Rep. 2022, 12, 13022. [Google Scholar] [CrossRef]
- Lenz, N.; Caduff, U.; Jörg, R.; Beglinger, C.; Rieder, S. Spatial accessibility to animal health care—A GIS based analysis. Schweiz Arch. Tierheilkd. 2020, 162, 377–386. [Google Scholar] [CrossRef]
- Langford, M.; Higgs, G. Measuring Potential Access to Primary Healthcare Services: The Influence of Alternative Spatial Representations of Population. Prof. Geogr. 2006, 58, 294–306. [Google Scholar] [CrossRef]
- Wang, L. Immigration, Ethnicity, and Accessibility to Culturally Diverse Family Physicians. Health Place 2007, 13, 656–671. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Rosenberg, M.; Lo, L. Ethnicity and Utilization of Family Physicians: A Case Study of Mainland Chinese Immigrants in Toronto, Canada. Soc. Sci. Med. 2008, 67, 1410–1422. [Google Scholar] [CrossRef] [PubMed]
- Access to Care|Alabama Department of Public Health (ADPH). Available online: https://www.alabamapublichealth.gov/healthrankings/access-to-care.html (accessed on 2 August 2023).
- 2020 Health Workforce Brief. Available online: https://aohw.org/2020-health-workforce-brief (accessed on 13 August 2023).
- Applebaum, J.W.; Peek, C.W.; Zsembik, B.A. Examining U.S. Pet Ownership Using the General Social Survey. Soc. Sci. J. 2023, 60, 110–119. [Google Scholar] [CrossRef]
- United States—Esri Demographics Regional Data|Documentation. Available online: https://doc.arcgis.com/en/esri-demographics/latest/regional-data/united-states.htm (accessed on 6 August 2023).
- Guerra, L. What’s New in Esri Demographics (June 2019). Available online: https://www.esri.com/arcgis-blog/products/esri-demographics/announcements/whats-new-in-esri-demographics-june-2019/ (accessed on 2 August 2023).
- Methodology Statement: 2019/2024 Esri Updated Demographics. Available online: https://downloads.esri.com/esri_content_doc/dbl/us/J10268_Methodology_Statement_2019-2024_Esri_US_Demographic_Updates.pdf (accessed on 5 January 2023).
- Obstetrics and Gynecology|Careers in Medicine. Available online: https://careersinmedicine.aamc.org/explore-options/specialty-profiles/obstetrics-and-gynecology (accessed on 2 August 2023).
- Methodology Statement: 2020/2025 Esri Updated Demographics. Available online: https://downloads.esri.com/esri_content_doc/dbl/us/J10268_Methodology_Statement_2020-2025_Esri_US_Demographic_Updates.pdf (accessed on 5 January 2023).
- Neal, S.M.; Greenberg, M.J. Veterinary Care Deserts: What Is the Capacity and Where Is It? J. Shelter. Med. Community Anim. Health 2022, 1, 1–8. [Google Scholar] [CrossRef]
- Luo, W.; Whippo, T. Variable Catchment Sizes for the Two-Step Floating Catchment Area (2SFCA) Method. Health Place 2012, 18, 789–795. [Google Scholar] [CrossRef]
- Ni, J.; Wang, J.; Rui, Y.; Qian, T.; Wang, J. An Enhanced Variable Two-Step Floating Catchment Area Method for Measuring Spatial Accessibility to Residential Care Facilities in Nanjing. Int. J. Environ. Res. Public Health 2015, 12, 14490–14504. [Google Scholar] [CrossRef]
- McGrail, M.R. Spatial Accessibility of Primary Health Care Utilising the Two Step Floating Catchment Area Method: An Assessment of Recent Improvements. Int. J. Health Geogr. 2012, 11, 50. [Google Scholar] [CrossRef]
- Chen, X.; Jia, P. A Comparative Analysis of Accessibility Measures by the Two-Step Floating Catchment Area (2SFCA) Method. Int. J. Geogr. Inf. Sci. 2019, 33, 1739–1758. [Google Scholar] [CrossRef]
- Langford, M.; Higgs, G.; Jones, S. Understanding Spatial Variations in Accessibility to Banks Using Variable Floating Catchment Area Techniques. Appl. Spat. Anal. Policy 2021, 14, 449–472. [Google Scholar] [CrossRef]
- Wan, N.; Zou, B.; Sternberg, T. A Three-Step Floating Catchment Area Method for Analyzing Spatial Access to Health Services. Int. J. Geogr. Inf. Sci. 2012, 26, 1073–1089. [Google Scholar] [CrossRef]
- Subal, J.; Paal, P.; Krisp, J.M. Quantifying Spatial Accessibility of General Practitioners by Applying a Modified Huff Three-Step Floating Catchment Area (MH3SFCA) Method. Int. J. Health Geogr. 2021, 20, 9. [Google Scholar] [CrossRef] [PubMed]
- Marx, M.B.; Stallones, L.B.; Garrity, T.F.; Johnson, T.P. Demographics of Pet Ownership among U.S. Adults 21 to 64 Years of Age. Anthrozoös 1988, 2, 33–37. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neal, S.M. Correlating Access to Primary Medical Care and Veterinary Care Providers: A Novel Application of Spatial Gravity Modelling. Vet. Sci. 2023, 10, 565. https://doi.org/10.3390/vetsci10090565
Neal SM. Correlating Access to Primary Medical Care and Veterinary Care Providers: A Novel Application of Spatial Gravity Modelling. Veterinary Sciences. 2023; 10(9):565. https://doi.org/10.3390/vetsci10090565
Chicago/Turabian StyleNeal, Sue M. 2023. "Correlating Access to Primary Medical Care and Veterinary Care Providers: A Novel Application of Spatial Gravity Modelling" Veterinary Sciences 10, no. 9: 565. https://doi.org/10.3390/vetsci10090565
APA StyleNeal, S. M. (2023). Correlating Access to Primary Medical Care and Veterinary Care Providers: A Novel Application of Spatial Gravity Modelling. Veterinary Sciences, 10(9), 565. https://doi.org/10.3390/vetsci10090565