



Hemodynamic Effect of Pulsatile on Blood Flow Distribution with VA ECMO: A Numerical Study
Abstract
1. Introduction
2. Materials and Methods
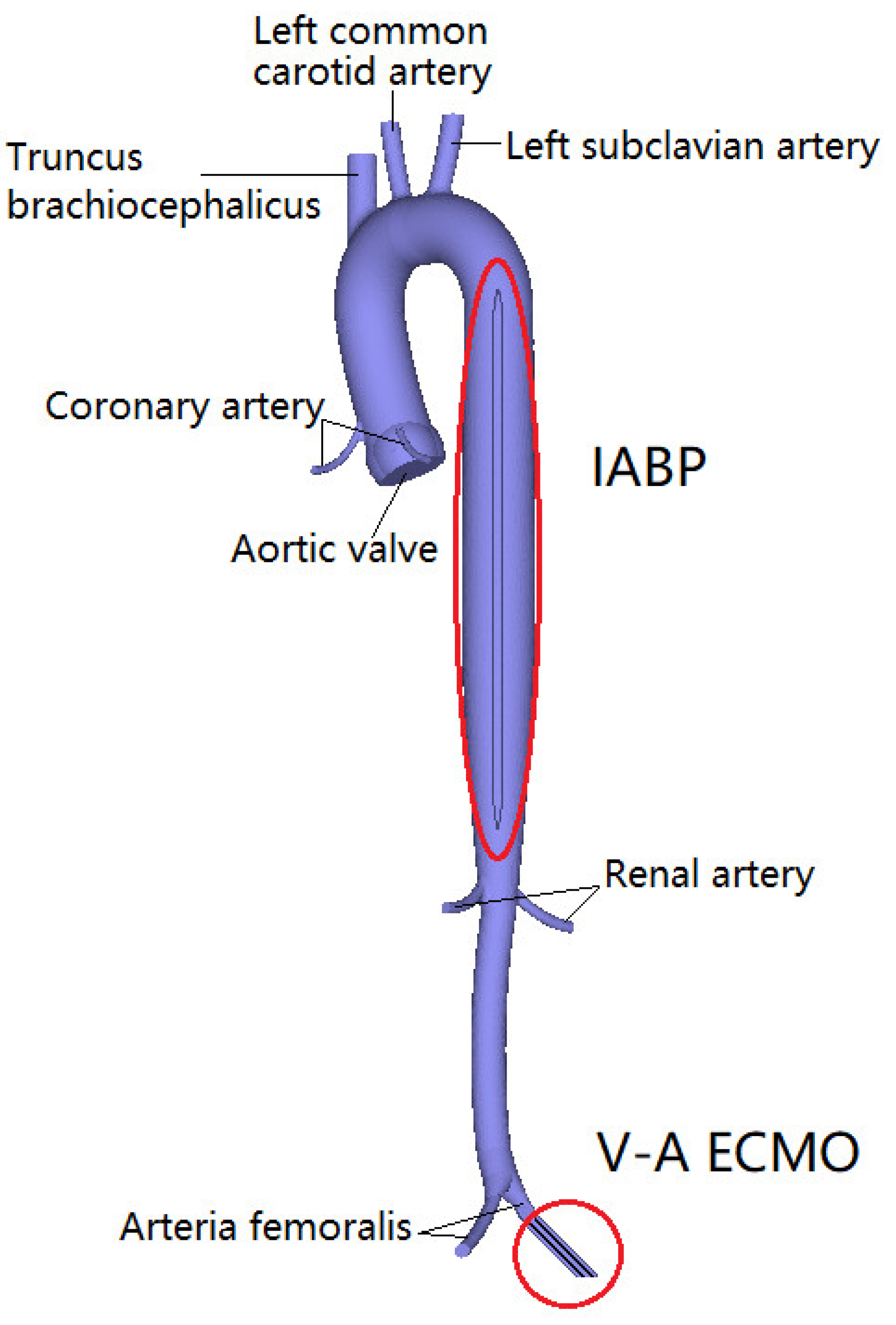
2.1. Reconstruction of Aortic, ECMO, and IABP Model
2.2. FE Model
2.3. Boundary Condition
2.4. Biomechanical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abrams, D.; Combes, A.; Brodie, D. Extracorporeal Membrane Oxygenation in Cardiopulmonary Disease in Adults. J. Am. Coll. Cardiol. 2014, 63, 2769–2778. [Google Scholar] [CrossRef]
- Borden, R.A.; Ball, C.; Grady, P.M.; Toth, A.J.; Lober, C.; Bakaeen, F.G.; Tong, M.Z.; Soltesz, E.G.; Blackstone, E.H.; Roselli, E.E. Microplegia vs. 4:1 Blood Cardioplegia: Effectiveness and Cost Savings in Complex Cardiac Operations. Ann. Thorac. Surg. 2020, 110, 1216–1224. [Google Scholar] [CrossRef]
- Keebler, M.E.; Haddad, E.V.; Choi, C.W.; McGrane, S.; Zalawadiya, S.; Schlendorf, K.H.; Brinkley, D.M.; Danter, M.R.; Wigger, M.; Menachem, J.N.; et al. Venoarterial extracorporeal membrane oxygenation in cardiogenic shock. JACC Heart Fail. 2018, 6, 503–516. [Google Scholar] [CrossRef]
- Vallabhajosyula, S.; Prasad, A.; Bell, M.R.; Sandhu, G.S.; Eleid, M.F.; Dunlay, S.M.; Schears, G.J.; Stulak, J.M.; Singh, M.; Gersh, B.J.; et al. Extracorporeal membrane oxygenation use in acute myocardial infarction in the United States, 2000 to 2014. Circ. Heart Fail. 2019, 12, e005929. [Google Scholar] [CrossRef]
- Pages, O.N.; Aubert, S.; Combes, A.; Luyt, C.E.; Pavie, A.; Léger, P.; Gandjbakhch, I.; Leprince, P. Paracorporeal pulsatile biventricular assist device versus extracorporal membrane oxygenation-extracorporal life support in adult fulminant myocarditis. J. Thorac. Cardiovasc. Surg. 2009, 137, 194–197. [Google Scholar] [CrossRef]
- Ji, B.; Undar, A. Comparison of perfusion modes on microcirculation during acute and chronic cardiac support: Is there a difference? Perfusion 2007, 22, 115–119. [Google Scholar] [CrossRef]
- Wang, S.; Spencer, S.B.; Kunselman, A.R.; Ündar, A. Novel ECG-Synchronized Pulsatile ECLS System with Various Heart Rates and Cardiac Arrhythmias: An In Vitro Study. Artif. Organs. 2017, 41, 55–65. [Google Scholar] [CrossRef]
- Gu, K.; Guan, Z.; Lin, X.; Feng, Y.; Feng, J.; Yang, Y.; Zhang, Z.; Chang, Y.; Ling, Y.; Wan, F. Numerical analysis of aortic hemodynamics under the support of venoarterial extracorporeal membrane oxygenation and intra-aortic balloon pump. Comput. Methods Programs Biomed. 2019, 182, 105041. [Google Scholar] [CrossRef]
- Shepard, R.B.; Simpson, D.C.; Sharp, J.F. Energy equivalent pressure. Arch. Surg. 1966, 93, 730–740. [Google Scholar] [CrossRef]
- Willey, J.Z.; Gavalas, M.V.; Trinh, P.N.; Yuzefpolskaya, M.; Garan, A.R.; Levin, A.P.; Takeda, K.; Takayama, H.; Fried, J.; Naka, Y.; et al. Outcomes after stroke complicating left ventricular assist device. J. Heart Lung Transplant. 2016, 35, 1003–1009. [Google Scholar] [CrossRef]
- Starling, R.C.; Moazami, N.; Silvestry, S.C.; Ewald, G.; Rogers, J.G.; Milano, C.A.; Rame, J.E.; Acker, M.A.; Blackstone, E.H.; Ehrlinger, J.; et al. Unexpected abrupt increase in left ventricular assist device thrombosis. N. Engl. J. Med. 2014, 370, 33–40. [Google Scholar] [CrossRef]
- Patel, A.C.; Dodson, R.B.; Cornwell, W.K.; Hunter, K.S.; Cleveland, J.C., Jr.; Brieke, A.; Lindenfeld, J.; Ambardekar, A.V. Dynamic changes in aortic vascular stiffness in patients bridged to transplant with continuous-flow left ventricular assist devices. JACC Heart Fail. 2017, 5, 449–459. [Google Scholar] [CrossRef]
- Undar, A.; Henderson, N.; Thurston, G.B.; Masai, T.; Beyer, E.A.; Frazier, O.H.; Fraser, C.D., Jr. The effects of pulsatile versus nonpulsatile perfusion on blood viscoelasticity before and after deep hypothermic circulatory arrest in a neonatal piglet model. Artif. Organs. 1999, 23, 717–721. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, J.; He, X.; Cao, W.; Peng, X.; Li, G. Pulsatility protects the endothelial glycocalyx during extracorporeal membrane oxygenation. Microcirculation 2021, 28, e12722. [Google Scholar] [CrossRef]
- Wang, S.; Kunselman, A.R.; Clark, J.B.; Ündar, A. In vitro hemodynamic evaluation of a novel pulsatile extracorporeal life support system: Impact of perfusion modes and circuit components on energy loss. Artif. Organs. 2015, 39, 59–66. [Google Scholar] [CrossRef]
- Russell, S.D.; Rogers, J.G.; Milano, C.A.; Dyke, D.B.; Pagani, F.D.; Aranda, J.M.; Klodell, C.T., Jr.; Boyle, A.J.; John, R.; Chen, L.; et al. HeartMate II Clinical Investigators, Renal and hepatic function improve in advanced heart failure patients during continuous-flow support with the HeartMate II left ventricular assist device. Circulation 2009, 120, 2352–2357. [Google Scholar] [CrossRef]
- Miller, L.W. Is pulsatile blood flow no longer essential? Circulation 2009, 120, 2313–2314. [Google Scholar] [CrossRef]
- Plonek, T.; Zak, M.; Burzynska, K.; Rylski, B.; Gozdzik, A.; Kustrzycki, W.; Beyersdorf, F.; Jasinski, M.; Filipiak, J. The combined impact of mechanical factors on the wall stress of the human ascending aorta—A finite elements study. BMC Cardiovas. Disord. 2017, 17, 297. [Google Scholar] [CrossRef]
- Rihal, C.S.; Naidu, S.S.; Givertz, M.M.; Szeto, W.Y.; Burke, J.A.; Kapur, N.K.; Kern, M.; Garratt, K.N.; Goldstein, J.A.; Dimas, V.; et al. Society for Cardiovascular Angiography and Interventions (SCAI); Heart Failure Society of America (HFSA); Society of Thoracic Surgeons (STS); American Heart Association (AHA), and American College of Cardiology (ACC). 2015 SCAI/ACC/HFSA/STS clinical expert consensus statement on the use of percutaneous mechanical circulatory support devices in cardiovascular care: Endorsed by the american heart association, the cardiological society of india, and sociedad latino americana de cardiologia intervencion; affirmation of value by the canadian association of interventional cardiology-association canadienne de cardiologie d’intervention. J. Am. Coll. Cardiol. 2015, 65, e7–e26. [Google Scholar] [CrossRef]
- Gajanan, G.; Brilakis, E.S.; Siller-Matula, J.M.; Zolty, R.L.; Velagapudi, P. The Intra-Aortic Balloon Pump. J. Vis. Exp. 2021, 5, e62132. [Google Scholar] [CrossRef]
- Huu, A.L.; Shum-Tim, D. Intra-aortic balloon pump: Current evidence & future perspectives. Future Cardiol. 2018, 14, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Chaney, M.A. Pulsatile versus nonpulsatile blood flow during cardiopulmonary bypass. Int. Anesthesiol. Clin. 2022, 60, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Onorati, F.; Cristodoro, L.; Bilotta, M.; Impiombato, B.; Pezzo, F.; Mastroroberto, P.; di Virgilio, A.; Renzulli, A. Intraaortic balloon pumping during cardioplegic arrest preserves lung function in patients with chronic obstructive pulmonary disease. Ann. Thorac. Surg. 2006, 82, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.J.; Ferenc, M.; Olbrich, H.G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. IABP-SHOCK II Trial Investigators, Intraaortic balloon support for myocardial infarction with cardiogenic shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Thelemann, N.; Neumann, F.J.; Hausleiter, J.; Abdel-Wahab, M.; Meyer-Saraei, R.; Fuernau, G.; Eitel, I.; Hambrecht, R.; et al. IABPSHOCK II Trial Investigators. Intraaortic balloon pump in cardiogenic shock complicating acute myocardial infarction: Long-term 6-year outcome of the randomized IABP-SHOCK II Trial. Circulation 2018, 118, 038201. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. Authors/Task Force Members; Document Reviewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Annamalai, S.K.; Buiten, L.; Esposito, M.L.; Paruchuri, V.; Mullin, A.; Breton, C.; Pedicini, R.; O’Kelly, R.; Morine, K.; Wessler, B.; et al. Acute hemodynamic effects of intra-aortic balloon counterpulsation pumps in advanced heart failure. J. Card. Fail. 2017, 23, 606–614. [Google Scholar] [CrossRef]
- Takayama, H.; Truby, L.; Koekort, M.; Uriel, N.; Colombo, P.; Mancini, D.M.; Jorde, U.P.; Naka, Y. Clinical outcome of mechanical circulatory support for refractory cardiogenic shock in the current era. J. Heart Lung Transplant. 2013, 32, 106–111. [Google Scholar] [CrossRef]
- Aso, S.; Matsui, H.; Fushimi, K.; Yasunaga, H. The effect of intraaortic balloon pumping under venoarterial extracorporeal membrane oxygenation on mortality of cardiogenic patients: An analysis using a nationwide inpatient database. Crit. Care Med. 2016, 44, 1974–1979. [Google Scholar] [CrossRef]
- Grandin, E.W.; Nunez, J.I.; Willar, B.; Kennedy, K.; Rycus, P.; Tonna, J.E.; Kapur, N.K.; Shaefi, S.; Garan, A.R. Mechanical Left Ventricular Unloading in Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation. J. Am. Coll Cardiol. 2022, 79, 1239–1250. [Google Scholar] [CrossRef]
- Li, Y.; Yan, S.; Gao, S.; Liu, M.; Lou, S.; Liu, G.; Ji, B.; Gao, B. Effect of an intra-aortic balloon pump with venoarterial extracorporeal membrane oxygenation on mortality of patients with cardiogenic shock: A systematic review and meta-analysisdagger. Eur. J. Cardiothorac. Surg. 2019, 55, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Giddens, D.P.; Molony, D.; Yang, C.; Samady, H.; Zheng, J.; Mintz, G.S.; Maehara, A.; Wang, L.; Pei, X.; et al. Combining ivus and optical coherence tomography for more accurate coronary cap thickness quantification and stress/strain calculations: A patient-specific three-dimensional fluid-structure interaction modeling approach. J. Biomech. Eng. 2018, 140, 0410051–04100512. [Google Scholar] [CrossRef] [PubMed]
- Sprigg, N.; Gray, L.J.; Bath, P.M.; Boysen, G.; De Deyn, P.P.; Friis, P.; Leys, D.; Marttila, R.; Olsson, J.E.; O’Neill, D.; et al. TAIST Investigators. Relationship between outcome and baseline blood pressure and other haemodynamic measures in acute ischaemic stroke: Data from the TAIST trial. J. Hypertens. 2006, 24, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Palanzo, D.; Qiu, F.; Baer, L.; Clark, J.B.; Myers, J.L.; Undar, A. Evolution of the extracorporeal life support circuitry. Artif. Organs. 2010, 34, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Moroi, M.K.; Force, M.; Kunselman, A.R.; Ündar, A. Impact of Heart Rate on Pulsatile Hemodynamic performance in a neonatal ECG-synchronized ecls system. Artif. Organs. 2019, 43, 81–89. [Google Scholar] [CrossRef]
- Ostadal, P.; Mlcek, M.; Gorhan, H.; Simundic, I.; Strunina, S.; Hrachovina, M.; Krüger, A.; Vondrakova, D.; Janotka, M.; Hala, P.; et al. Electrocardiogram-synchronized pulsatile extracorporeal life support preserves left ventricular function and coronary flow in a porcine model of cardiogenic shock. PLoS ONE 2018, 13, e0196321. [Google Scholar] [CrossRef]
- Hong, T.H.; Byun, J.H.; Yoo, B.H.; Hwang, S.W.; Kim, H.Y.; Park, J.H. Successful left-heart decompression during extracorporeal membrane oxygenation in an adult patient by percutaneous transaortic catheter venting. Korean J. Thorac. Cardiovasc. Surg. 2015, 48, 210–213. [Google Scholar] [CrossRef]
- Hatano, M.; Kinugawa, K.; Shiga, T.; Kato, N.; Endo, M.; Hisagi, M.; Nishimura, T.; Yao, A.; Hirata, Y.; Kyo, S.; et al. Less frequent opening of the aortic valve and a continuous flow pump are risk factors for postoperative onset of aortic insufficiency in patients with a left ventricular assist device. Circ. J. 2011, 75, 1147–1155. [Google Scholar] [CrossRef]
- Santise, G.; Panarello, G.; Ruperto, C.; Turrisi, M.; Pilato, G.; Giunta, A.; Sciacca, S.; Pilato, M. Extracorporeal membrane oxygenation for graft failure after heart transplantation: A multidisciplinary approach to maximize weaning rate. Int. J. Artif. Organs. 2014, 37, 706–714. [Google Scholar] [CrossRef]
- Gass, A.; Palaniswamy, C.; Aronow, W.S.; Kolte, D.; Khera, S.; Ahmad, H.; Cuomo, L.J.; Timmermans, R.; Cohen, M.; Tang, G.H.; et al. Peripheral venoarterial extracorporeal membrane oxygenation in combination with intra-aortic balloon counterpulsation in patients with cardiovascular compromise. Cardiology 2014, 129, 137–143. [Google Scholar] [CrossRef]
- Bréchot, N.; Demondion, P.; Santi, F.; Lebreton, G.; Pham, T.; Dalakidis, A.; Gambotti, L.; Luyt, C.E.; Schmidt, M.; Hekimian, G.; et al. Intra-aortic balloon pump protects against hydrostatic pulmonary oedema during peripheral venoarterial-extracorporeal membrane oxygenation. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Ma, P.; Zhang, Z.; Song, T.; Yang, Y.; Meng, G.; Zhao, J.; Wang, C.; Gu, K.; Peng, J.; Jiang, B.; et al. Combining ECMO with IABP for the treatment of critically Ill adult heart failure patients. Heart Lung Circ. 2014, 23, 363–368. [Google Scholar] [CrossRef]
- Itoh, H.; Ichiba, S.; Ujike, Y.; Douguchi, T.; Obata, H.; Inamori, S.; Iwasaki, T.; Kasahara, S.; Sano, S.; Ündar, A. Effect of the pulsatile extracorporeal membrane oxygenation on hemodynamic energy and systemic microcirculation in a piglet model of acute cardiac failure. Artif. Organs. 2016, 40, 19–26. [Google Scholar] [CrossRef]
- Peng-Lin, Y.; Yue-Chun, L. Pulse pressure index (pulse pressure/systolic pressure) may be better than pulse pressure for assessment of cardiovascular outcomes. Med. Hypotheses. 2009, 72, 729–731. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, M.P.; Alie, R.; Guo, L.R.; Myers, M.L.; Murkin, J.M.; Ellis, C.G. Microvascular Responsiveness to Pulsatile and Nonpulsatile Flow During Cardiopulmonary Bypass. Ann. Thorac. Surg. 2018, 105, 1745–1753. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, J.C.; Jang, D.H.; Hallisey, S.D.; Gutsche, J.T.; Horak, J.; Acker, M.A.; Bermudez, C.A.; Zhou, V.L.; Chatterjee, S.; Shofer, F.S.; et al. Severe Impairment of Microcirculatory Perfused Vessel Density Is Associated With Postoperative Lactate and Acute Organ Injury After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2021, 35, 106–115. [Google Scholar] [CrossRef]
- Miyamoto, T.; Karimov, J.H.; Fukamachi, K. Effects of continuous and pulsatile flows generated by ventricular assist devices on renal function and pathology. Expert Rev. Med. Devices 2018, 15, 171–182. [Google Scholar] [CrossRef]
- Sezai, A.; Shiono, M.; Orime, Y.; Nakata, K.; Hata, M.; Yamada, H.; Iida, M.; Kashiwazaki, S.; Kinishita, J.; Nemoto, M.; et al. Renal circulation and cellular metabolism during left ventricular assisted circulation: Comparison study of pulsatile and nonpulsatile assists. Artif. Organs. 1997, 21, 830–835. [Google Scholar] [CrossRef]
- Peigh, G.; Cavarocchi, N.; Keith, S.W.; Hirose, H. Simple new risk score model for adult cardiac extracorporeal membrane oxygenation: Simple cardiac ECMO score. J. Surg. Res. 2015, 198, 273–279. [Google Scholar] [CrossRef]
- Distelmaier, K.; Roth, C.; Binder, C.; Schrutka, L.; Schreiber, C.; Hoffelner, F.; Heinz, G.; Lang, I.M.; Maurer, G.; Koinig, H.; et al. Urinary output predicts survival in patients undergoing extracorporeal membrane oxygenation following cardiovascular surgery. Crit. Care Med. 2016, 44, 531–538. [Google Scholar] [CrossRef]
- Natanov, R.; Khalikov, A.; Gueler, F.; Maus, U.; Boyle, E.C.; Haverich, A.; Kühn, C.; Madrahimov, N. Four hours of veno-venous extracorporeal membrane oxygenation using bi-caval cannulation affects kidney function and induces moderate lung damage in a mouse model. Intensive Care Med. Exp. 2019, 72, 7. [Google Scholar] [CrossRef] [PubMed]
- Vinclair, C.; De Montmollin, E.; Sonneville, R.; Reuter, J.; Lebut, J.; Cally, R.; Mourvillier, B.; Neuville, M.; Ruckly, S.; Timsit, J.F.; et al. Factors associated with major adverse kidney events in patients who underwent veno-arterial extracorporeal membrane oxygenation. Ann. Intensive Care 2020, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- von Horn, C.; Minor, T. Isolated kidney perfusion: The influence of pulsatile flow. Scand. J. Clin. Lab. Invest. 2018, 78, 131–135. [Google Scholar] [CrossRef]
- Dhawan, S.S.; Avati Nanjundappa, R.P.; Branch, J.R.; Taylor, W.R.; Quyyumi, A.A.; Jo, H.; McDaniel, M.C.; Suo, J.; Giddens, D.; Samady, H. Shear stress and plaque development. Expert Rev. Cardiovasc. Ther. 2010, 8, 545–556. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | Group C | |||
|---|---|---|---|---|---|
| CO (L/min) | CO (L/min) | ECMO (L/min) | CO (L/min) | ECMO (L/min) | IABP (mL) |
| 1.5 | 1.5 | 3.0 | 1.5 | 3.0 | 30 |
| 2.0 | 2.5 | 2.0 | 2.5 | ||
| 2.5 | 2.0 | 2.5 | 2.0 | ||
| 3.0 | 1.5 | 3.0 | 1.5 | ||
| 3.5 | 1.0 | 3.5 | 1.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, K.; Gao, S.; Zhang, Z.; Ji, B.; Chang, Y. Hemodynamic Effect of Pulsatile on Blood Flow Distribution with VA ECMO: A Numerical Study. Bioengineering 2022, 9, 487. https://doi.org/10.3390/bioengineering9100487
Gu K, Gao S, Zhang Z, Ji B, Chang Y. Hemodynamic Effect of Pulsatile on Blood Flow Distribution with VA ECMO: A Numerical Study. Bioengineering. 2022; 9(10):487. https://doi.org/10.3390/bioengineering9100487
Chicago/Turabian StyleGu, Kaiyun, Sizhe Gao, Zhe Zhang, Bingyang Ji, and Yu Chang. 2022. "Hemodynamic Effect of Pulsatile on Blood Flow Distribution with VA ECMO: A Numerical Study" Bioengineering 9, no. 10: 487. https://doi.org/10.3390/bioengineering9100487
APA StyleGu, K., Gao, S., Zhang, Z., Ji, B., & Chang, Y. (2022). Hemodynamic Effect of Pulsatile on Blood Flow Distribution with VA ECMO: A Numerical Study. Bioengineering, 9(10), 487. https://doi.org/10.3390/bioengineering9100487