

Current Status of Oral Disease-Modifying Treatment Effects on Cognitive Outcomes in Multiple Sclerosis: A Scoping Review


Abstract
1. Introduction
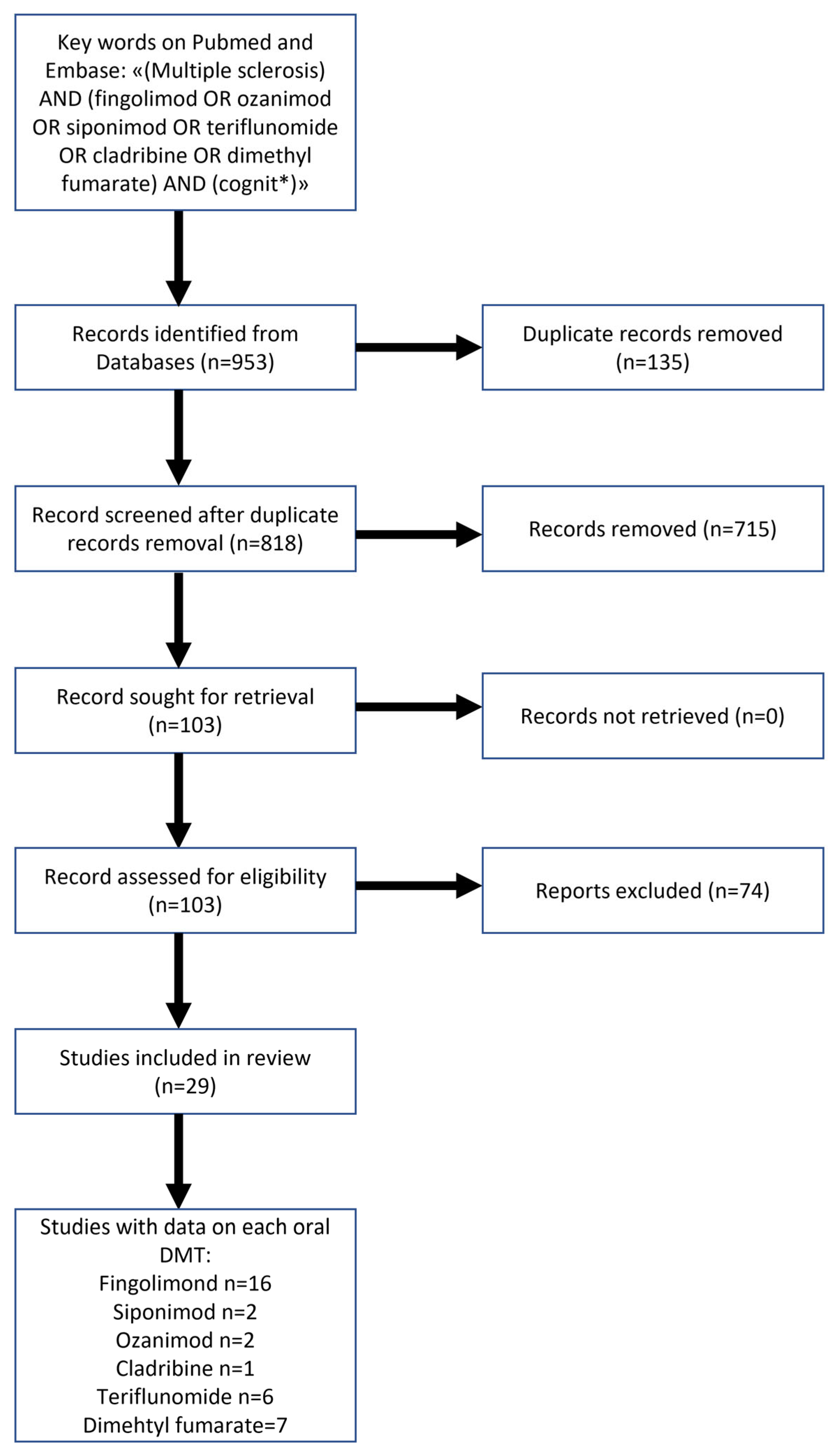
2. Methods and Search Strategy
3. Results
3.1. Sphingosinte-1-Phosphate Modulators
3.2. Dimethyl Fumarate (DMF)
3.3. Teriflunomide
3.4. Cladribine
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Achiron, A.; Chapman, J.; Magalashvili, D.; Dolev, M.; Lavie, M.; Bercovich, E.; Polliack, M.; Doniger, G.M.; Stern, Y.; Khilkevich, O.; et al. Modeling of cognitive impairment by disease duration in multiple sclerosis: A cross-sectional study. PLoS ONE 2013, 8, e71058. [Google Scholar] [CrossRef] [PubMed]
- Olazarán, J.; Cruz, I.; Benito-León, J.; Morales, J.M.; Duque, P.; Rivera-Navarro, J. Cognitive dysfunction in multiple sclerosis: Methods and prevalence from the GEDMA Study. Eur. Neurol. 2009, 61, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.M.; Leo, G.J.; Bernardin, L.; Unverzagt, F. Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction. Neurology 1991, 41, 685–691. [Google Scholar] [CrossRef]
- Hynčicová, E.; Vyhnálek, M.; Kalina, A.; Martinkovič, L.; Nikolai, T.; Lisý, J.; Hort, J.; Meluzínová, E.; Laczó, J. Cognitive impairment and structural brain changes in patients with clinically isolated syndrome at high risk for multiple sclerosis. J. Neurol. 2017, 264, 482–493. [Google Scholar] [CrossRef] [PubMed]
- Diker, S.; Has, A.C.; Kurne, A.; Göçmen, R.; Oğuz, K.K.; Karabudak, R. The association of cognitive impairment with gray matter atrophy and cortical lesion load in clinically isolated syndrome. Mult. Scler. Relat. Disord. 2016, 10, 14–21. [Google Scholar] [CrossRef]
- Labiano-Fontcuberta, A.; Martínez-Ginés, M.L.; Aladro, Y.; Ayuso, L.; Mitchell, A.J.; Puertas-Martín, V.; Cerezo, M.; Higueras, Y.; Benito-León, J. A comparison study of cognitive deficits in radiologically and clinically isolated syndromes. Mult. Scler. 2016, 22, 250–253. [Google Scholar] [CrossRef]
- Amato, M.P.; Ponziani, G.; Siracusa, G.; Sorbi, S. Cognitive dysfunction in early-onset multiple sclerosis: A reappraisal after 10 years. Arch. Neurol. 2001, 58, 1602–1606. [Google Scholar] [CrossRef]
- Lacy, M.; Hauser, M.; Pliskin, N.; Assuras, S.; Valentine, M.O.; Reder, A. The effects of long-term interferon-beta-1b treatment on cognitive functioning in multiple sclerosis: A 16-year longitudinal study. Mult. Scler. 2013, 19, 1765–1772. [Google Scholar] [CrossRef]
- Johnen, A.; Landmeyer, N.C.; Bürkner, P.C.; Wiendl, H.; Meuth, S.G.; Holling, H. Distinct cognitive impairments in different disease courses of multiple sclerosis-A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2017, 83, 568–578. [Google Scholar] [CrossRef]
- Bergendal, G.; Fredrikson, S.; Almkvist, O. Selective decline in information processing in subgroups of multiple sclerosis: An 8-year longitudinal study. Eur. Neurol. 2007, 57, 193–202. [Google Scholar] [CrossRef]
- Amato, M.P.; Portaccio, E.; Goretti, B.; Zipoli, V.; Iudice, A.; Della Pina, D.; Malentacchi, G.; Sabatini, S.; Annunziata, P.; Falcini, M.; et al. Relevance of cognitive deterioration in early relapsing-remitting MS: A 3-year follow-up study. Mult. Scler. 2010, 16, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Goretti, B.; Ghezzi, A.; Hakiki, B.; Niccolai, C.; Lori, S.; Moiola, L.; Falautano, M.; Viterbo, R.G.; Patti, F.; et al. Neuropsychological features in childhood and juvenile multiple sclerosis: Five-year follow-up. Neurology 2014, 83, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Deloire, M.S.; Ruet, A.; Hamel, D.; Bonnet, M.; Dousset, V.; Brochet, B. MRI predictors of cognitive outcome in early multiple sclerosis. Neurology 2011, 76, 1161–1167. [Google Scholar] [CrossRef]
- Klistorner, S.; Barnett, M.H.; Klistorner, A. Mechanisms of central brain atrophy in multiple sclerosis. Mult. Scler. 2022, 28, 2038–2045. [Google Scholar] [CrossRef]
- Houtchens, M.K.; Benedict, R.H.; Killiany, R.; Sharma, J.; Jaisani, Z.; Singh, B.; Weinstock-Guttman, B.; Guttmann, C.R.; Bakshi, R. Thalamic atrophy and cognition in multiple sclerosis. Neurology 2007, 69, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.H.; Ramasamy, D.; Munschauer, F.; Weinstock-Guttman, B.; Zivadinov, R. Memory impairment in multiple sclerosis: Correlation with deep grey matter and mesial temporal atrophy. J. Neurol. Neurosurg. Psychiatry 2009, 80, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Bartolozzi, M.L.; Zipoli, V.; Portaccio, E.; Mortilla, M.; Guidi, L.; Siracusa, G.; Sorbi, S.; Federico, A.; De Stefano, N. Neocortical volume decrease in relapsing-remitting MS patients with mild cognitive impairment. Neurology 2004, 63, 89–93. [Google Scholar] [CrossRef]
- Nelson, F.; Datta, S.; Garcia, N.; Rozario, N.L.; Perez, F.; Cutter, G.; Narayana, P.A.; Wolinsky, J.S. Intracortical lesions by 3T magnetic resonance imaging and correlation with cognitive impairment in multiple sclerosis. Mult. Scler. 2011, 17, 1122–1129. [Google Scholar] [CrossRef]
- Benedict, R.H.; DeLuca, J.; Phillips, G.; LaRocca, N.; Hudson, L.D.; Rudick, R. Validity of the Symbol Digit Modalities Test as a cognition performance outcome measure for multiple sclerosis. Mult. Scler. 2017, 23, 721–733. [Google Scholar] [CrossRef]
- Chiaravalloti, N.D.; DeLuca, J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008, 7, 1139–1151. [Google Scholar] [CrossRef]
- Benedict, R.H.; Fischer, J.S.; Archibald, C.J.; Arnett, P.A.; Beatty, W.W.; Bobholz, J.; Chelune, G.J.; Fisk, J.D.; Langdon, D.W.; Caruso, L.; et al. Minimal neuropsychological assessment of MS patients: A consensus approach. Clin. Neuropsychol. 2002, 16, 381–397. [Google Scholar] [CrossRef] [PubMed]
- Carotenuto, A. Look beyond the door, not through the keyhole: Evidence from a cognitive assessment including social cognition evaluation in multiple sclerosis. Eur. J. Neurol. 2018, 25, 205–206. [Google Scholar] [CrossRef] [PubMed]
- Cotter, J.; Firth, J.; Enzinger, C.; Kontopantelis, E.; Yung, A.R.; Elliott, R.; Drake, R.J. Social cognition in multiple sclerosis: A systematic review and meta-analysis. Neurology 2016, 87, 1727–1736. [Google Scholar] [CrossRef]
- Denney, D.R.; Lynch, S.G.; Parmenter, B.A. A 3-year longitudinal study of cognitive impairment in patients with primary progressive multiple sclerosis: Speed matters. J. Neurol. Sci. 2008, 267, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Van Schependom, J.; D’Hooghe, M.B.; Cleynhens, K.; D’Hooge, M.; Haelewyck, M.C.; De Keyser, J.; Nagels, G. Reduced information processing speed as primum movens for cognitive decline in MS. Mult. Scler. 2015, 21, 83–91. [Google Scholar] [CrossRef]
- Fogarty, E.; Schmitz, S.; Tubridy, N.; Walsh, C.; Barry, M. Comparative efficacy of disease-modifying therapies for patients with relapsing remitting multiple sclerosis: Systematic review and network meta-analysis. Mult. Scler. Relat. Disord. 2016, 9, 23–30. [Google Scholar] [CrossRef]
- Faissner, S.; Gold, R. Oral Therapies for Multiple Sclerosis. Cold Spring Harb. Perspect. Med. 2019, 9, a032011. [Google Scholar] [CrossRef]
- Gil, A.; Martín-Montañez, E.; Valverde, N.; Lara, E.; Boraldi, F.; Claros, S.; Romero-Zerbo, S.Y.; Fernández, O.; Pavia, J.; Garcia-Fernandez, M. Neuronal Metabolism and Neuroprotection: Neuroprotective Effect of Fingolimod on Menadione-Induced Mitochondrial Damage. Cells 2020, 10, 34. [Google Scholar] [CrossRef]
- Gentile, A.; Musella, A.; Bullitta, S.; Fresegna, D.; De Vito, F.; Fantozzi, R.; Piras, E.; Gargano, F.; Borsellino, G.; Battistini, L.; et al. Siponimod (BAF312) prevents synaptic neurodegeneration in experimental multiple sclerosis. J. Neuroinflamm. 2016, 13, 207. [Google Scholar] [CrossRef]
- Musella, A.; Gentile, A.; Guadalupi, L.; Rizzo, F.R.; De Vito, F.; Fresegna, D.; Bruno, A.; Dolcetti, E.; Vanni, V.; Vitiello, L.; et al. Central Modulation of Selective Sphingosine-1-Phosphate Receptor 1 Ameliorates Experimental Multiple Sclerosis. Cells 2020, 9, 1290. [Google Scholar] [CrossRef]
- De Stefano, N.; Silva, D.G.; Barnett, M.H. Effect of Fingolimod on Brain Volume Loss in Patients with Multiple Sclerosis. CNS Drugs 2017, 31, 289–305. [Google Scholar] [CrossRef] [PubMed]
- Fronza, M.; Lorefice, L.; Frau, J.; Cocco, E. An Overview of the Efficacy and Safety of Ozanimod for the Treatment of Relapsing Multiple Sclerosis. Drug Des. Dev. Ther. 2021, 15, 1993–2004. [Google Scholar] [CrossRef] [PubMed]
- Cree, B.A.; Arnold, D.L.; Fox, R.J.; Gold, R.; Vermersch, P.; Benedict, R.H.; Bar-Or, A.; Piani-Meier, D.; Rouyrre, N.; Ritter, S.; et al. Long-term efficacy and safety of siponimod in patients with secondary progressive multiple sclerosis: Analysis of EXPAND core and extension data up to >5 years. Mult. Scler. 2022, 28, 1591–1605. [Google Scholar] [CrossRef] [PubMed]
- Zivadinov, R.; Dwyer, M.G.; Carl, E.; Poole, E.M.; Cavalier, S.; Briassouli, P.; Bergsland, N. Slowing of brain atrophy with teriflunomide and delayed conversion to clinically definite MS. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420970754. [Google Scholar] [CrossRef]
- Dupuy, S.L.; Tauhid, S.; Hurwitz, S.; Chu, R.; Yousuf, F.; Bakshi, R. The Effect of Dimethyl Fumarate on Cerebral Gray Matter Atrophy in Multiple Sclerosis. Neurol. Ther. 2016, 5, 215–229. [Google Scholar] [CrossRef]
- Nakamura, K.; Mokliatchouk, O.; Arnold, D.L.; Yousry, T.A.; Kappos, L.; Richert, N.; Ayling-Rouse, K.; Miller, C.; Fisher, E. Effects of Dimethyl Fumarate on Brain Atrophy in Relapsing-Remitting Multiple Sclerosis: Pooled Analysis Phase 3 DEFINE and CONFIRM Studies. Front. Neurol. 2022, 13, 809273. [Google Scholar] [CrossRef]
- Riepl, E.; Pfeuffer, S.; Ruck, T.; Lohmann, H.; Wiendl, H.; Meuth, S.G.; Johnen, A. Alemtuzumab Improves Cognitive Processing Speed in Active Multiple Sclerosis-A Longitudinal Observational Study. Front. Neurol. 2017, 8, 730. [Google Scholar] [CrossRef]
- Mückschel, M.; Beste, C.; Ziemssen, T. Immunomodulatory treatments and cognition in MS. Acta Neurol. Scand. 2016, 134 (Suppl. 200), 55–59. [Google Scholar] [CrossRef]
- Comi, G.; Kappos, L.; Selmaj, K.W.; Bar-Or, A.; Arnold, D.L.; Steinman, L.; Hartung, H.P.; Montalban, X.; Kubala Havrdová, E.; Cree, B.A.C.; et al. Safety and efficacy of ozanimod versus interferon beta-1a in relapsing multiple sclerosis (SUNBEAM): A multicentre, randomised, minimum 12-month, phase 3 trial. Lancet Neurol. 2019, 18, 1009–1020. [Google Scholar] [CrossRef]
- Kappos, L.; Radue, E.W.; Chin, P.; Ritter, S.; Tomic, D.; Lublin, F. Onset of clinical and MRI efficacy occurs early after fingolimod treatment initiation in relapsing multiple sclerosis. J. Neurol. 2016, 263, 354–360. [Google Scholar] [CrossRef]
- Utz, K.S.; Lee, D.H.; Lämmer, A.; Waschbisch, A.; Linker, R.A.; Schenk, T. Cognitive functions over the course of 1 year in multiple sclerosis patients treated with disease modifying therapies. Ther. Adv. Neurol. Disord. 2016, 9, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Comi, G.; Patti, F.; Rocca, M.A.; Mattioli, F.C.; Amato, M.P.; Gallo, P.; Centonze, D.; Pozzilli, C.; Saccà, F.; Bergh, F.T.; et al. Efficacy of fingolimod and interferon beta-1b on cognitive, MRI, and clinical outcomes in relapsing-remitting multiple sclerosis: An 18-month, open-label, rater-blinded, randomised, multicentre study (the GOLDEN study). J. Neurol. 2017, 264, 2436–2449. [Google Scholar] [CrossRef] [PubMed]
- Cree, B.A.C.; Arnold, D.L.; Cascione, M.; Fox, E.J.; Williams, I.M.; Meng, X.; Schofield, L.; Tenenbaum, N. Phase IV study of retention on fingolimod versus injectable multiple sclerosis therapies: A randomized clinical trial. Ther. Adv. Neurol. Disord. 2018, 11, 1756286418774338. [Google Scholar] [CrossRef] [PubMed]
- Petsas, N.; De Giglio, L.; González-Quintanilla, V.; Giuliani, M.; De Angelis, F.; Tona, F.; Carmellini, M.; Mainero, C.; Pozzilli, C.; Pantano, P. Functional Connectivity Changes After Initial Treatment With Fingolimod in Multiple Sclerosis. Front. Neurol. 2019, 10, 153. [Google Scholar] [CrossRef]
- Guevara, C.; Villa, E.; Diaz, V.; Garrido, C.; Martinez, M.; Orellana, P.; Alarcón, P.; Silva-Rosas, C.; Barker, G.J.; Kempton, M.J.; et al. Inclusion of the Symbol Digit Modalities Test in a revised assessment of ‘no evidence of disease activity-4 (NEDA-4)’ in Latin-American patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 42, 102076. [Google Scholar] [CrossRef]
- Honce, J.M.; Nair, K.V.; Hoyt, B.D.; Seale, R.A.; Sillau, S.; Engebretson, E.; Schurr, B.; Corboy, J.R.; Vollmer, T.L.; Alvarez, E. Brain Atrophy Rates for Stable Multiple Sclerosis Patients on Long-Term Fingolimod versus Glatiramer Acetate. Front. Neurol. 2020, 11, 1045. [Google Scholar] [CrossRef]
- Preziosa, P.; Rocca, M.A.; Riccitelli, G.C.; Moiola, L.; Storelli, L.; Rodegher, M.; Comi, G.; Signori, A.; Falini, A.; Filippi, M. Effects of Natalizumab and Fingolimod on Clinical, Cognitive, and Magnetic Resonance Imaging Measures in Multiple Sclerosis. Neurotherapeutics 2020, 17, 208–217. [Google Scholar] [CrossRef]
- Bhattacharyya, P.K.; Lowe, M.J.; Sakaie, K.E.; Li, H.; Lin, J.; Fox, R.J. Changes in structural and functional connectivity during two years of fingolimod therapy for multiple sclerosis. Magn. Reson. Imaging 2020, 74, 113–120. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Tomic, D.; Cree, B.A.; Fox, R.; Giovannoni, G.; Bar-Or, A.; Gold, R.; Vermersch, P.; Pohlmann, H.; Wright, I.; et al. Siponimod and Cognition in Secondary Progressive Multiple Sclerosis: EXPAND Secondary Analyses. Neurology 2021, 96, e376–e386. [Google Scholar] [CrossRef]
- DeLuca, J.; Schippling, S.; Montalban, X.; Kappos, L.; Cree, B.A.C.; Comi, G.; Arnold, D.L.; Hartung, H.P.; Sheffield, J.K.; Liu, H.; et al. Effect of Ozanimod on Symbol Digit Modalities Test Performance in Relapsing MS. Mult. Scler. Relat. Disord. 2021, 48, 102673. [Google Scholar] [CrossRef]
- Ozakbas, S.; Piri Cinar, B.; Yigit, P.; Baba, C.; Sagici, O. Five-year real-world data on fingolimod treatment’s effects on cognitive function. Mult. Scler. Relat. Disord. 2021, 54, 103089. [Google Scholar] [CrossRef] [PubMed]
- El Ayoubi, N.K.; Bou Reslan, S.W.; Baalbaki, M.M.; Darwish, H.; Khoury, S.J. Effect of fingolimod vs interferon treatment on OCT measurements and cognitive function in RRMS. Mult. Scler. Relat. Disord. 2021, 53, 103041. [Google Scholar] [CrossRef] [PubMed]
- Langdon, D.W.; Tomic, D.; Penner, I.K.; Calabrese, P.; Cutter, G.; Häring, D.A.; Dahlke, F.; Kappos, L. Baseline characteristics and effects of fingolimod on cognitive performance in patients with relapsing-remitting multiple sclerosis. Eur. J. Neurol. 2021, 28, 4135–4145. [Google Scholar] [CrossRef]
- Leppert, D. Blood Neurofilament Light in Progressive Multiple Sclerosis: Post Hoc Analysis of 2 Randomized Controlled Trials. Mult. Scler. 2022, 98, e2120–e2131. [Google Scholar] [CrossRef] [PubMed]
- Conway, D.S.; Planchon, S.M.; Oh, S.H.; Nakamura, K.; Thompson, N.R.; Sakaie, K.; Ontaneda, D. Measures of Thalamic Integrity are Associated with Cognitive Functioning in Fingolimod-treated Multiple Sclerosis Patients. Mult. Scler. Relat. Disord. 2021, 47, 102635. [Google Scholar] [CrossRef]
- Glasmacher, S.A.; Kearns, P.K.; Hassan, Z.; Connick, P.; Tauber, S.; Reetz, K.; Foley, P.; Chandran, S. The influence of disease-modifying therapy on hidden disability burden in people with newly diagnosed relapsing-remitting multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 63, 103837. [Google Scholar] [CrossRef]
- Hersh, C.M.; Altincatal, A.; Belviso, N.; Kapadia, S.; de Moor, C.; Rudick, R.; Williams, J.R.; Miller, C.; Koulinska, I. Real-world effectiveness of dimethyl fumarate versus fingolimod in a cohort of patients with multiple sclerosis using standardized, quantitative outcome metrics. Neurology 2022, 8, 20552173211069852. [Google Scholar] [CrossRef]
- Giovannoni, G.; Gold, R.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Marantz, J.L.; Yang, M.; Lee, A. Delayed-release dimethyl fumarate and disability assessed by the Multiple Sclerosis Functional Composite: Integrated analysis of DEFINE and CONFIRM. Mult. Scler. J.-Exp. Transl. Clin. 2016, 2, 2055217316634111. [Google Scholar] [CrossRef]
- Al-iedani, O.; Ribbons, K.; Lea, R.; Ramadan, S.; Lechner-Scott, J. A Longitudinal, Observational Study of the Effect of Dimethyl Fumarate on Hippocampal Metabolites in RRMS using 1H-MR Spectroscopy. J. Biomed. Sci. 2018, 7, 1–10. [Google Scholar] [CrossRef]
- Montes Diaz, G.; Fraussen, J.; Van Wijmeersch, B.; Hupperts, R.; Somers, V. Dimethyl fumarate induces a persistent change in the composition of the innate and adaptive immune system in multiple sclerosis patients. Sci. Rep. 2018, 8, 8194. [Google Scholar] [CrossRef]
- Amato, M.P.; Goretti, B.; Brescia Morra, V.; Gallo, P.; Zaffaroni, M.; Onofrj, M.; Cocco, E.; Borriello, G.; Zipoli, V.; Trojano, M. Effects of 2-year treatment with dimethyl fumarate on cognition and functional impairment in patients with relapsing remitting multiple sclerosis. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 3185–3193. [Google Scholar] [CrossRef]
- Piervincenzi, C.; Sbardella, E.; Altieri, M.; Ianniello, A.; Pantano, P.; Pozzilli, C.; Petsas, N. No Changes in Functional Connectivity After Dimethyl Fumarate Treatment in Multiple Sclerosis. Neurol. Ther. 2022, 11, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Sprenger, T.; Kappos, L. Effects of teriflunomide treatment on cognitive performance and brain volume in patients with relapsing multiple sclerosis: Post hoc analysis of the TEMSO core and extension studies. Mult. Scler. 2022, 28, 1719–1728. [Google Scholar] [CrossRef] [PubMed]
- Coyle, P.K.; Khatri, B.; Edwards, K.R.; Meca-Lallana, J.E.; Cavalier, S.; Rufi, P.; Benamor, M.; Thangavelu, K.; Robinson, M.; Gold, R. Patient-reported outcomes in patients with relapsing forms of MS switching to teriflunomide from other disease-modifying therapies: Results from the global Phase 4 Teri-PRO study in routine clinical practice. Mult. Scler. Relat. Disord. 2018, 26, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Corallo, F.; Rifici, C.; Bonanno, L.; Di Cara, M.; Lo Buono, V.; Venuti, G.; Marino, S.; Ciurleo, R.; Torre, V.; D’Aleo, G.; et al. The role of teriflunamide in multiple sclerosis patient: An observational study. Psychol. Health Med. 2021, 27, 2204–2211. [Google Scholar] [CrossRef]
- Bencsik, K.; Dobos, E.; Jobbágy, Z.; Birkás, A.J.; Kovács, K.; Sátori, M.; Lencsés, G.; Bartok, G.; Losonczi, E.; Vécsei, L.; et al. Real-World Evidence for Favourable Quality-of-Life Outcomes in Hungarian Patients with Relapsing-Remitting Multiple Sclerosis Treated for Two Years with Oral Teriflunomide: Results of the Teri-REAL Study. Pharmaceuticals 2022, 15, 598. [Google Scholar] [CrossRef]
- Benedict, R.H.; Cookfair, D.; Gavett, R.; Gunther, M.; Munschauer, F.; Garg, N.; Weinstock-Guttman, B. Validity of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). J. Int. Neuropsychol. Soc. JINS 2006, 12, 549–558. [Google Scholar] [CrossRef]
- Langdon, D.W.; Amato, M.P.; Boringa, J.; Brochet, B.; Foley, F.; Fredrikson, S.; Hämäläinen, P.; Hartung, H.P.; Krupp, L.; Penner, I.K.; et al. Recommendations for a Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS). Mult. Scler. 2012, 18, 891–898. [Google Scholar] [CrossRef]
- Kalb, R.; Beier, M.; Benedict, R.H.; Charvet, L.; Costello, K.; Feinstein, A.; Gingold, J.; Goverover, Y.; Halper, J.; Harris, C.; et al. Recommendations for cognitive screening and management in multiple sclerosis care. Mult. Scler. 2018, 24, 1665–1680. [Google Scholar] [CrossRef]
- Goverover, Y.; Chiaravalloti, N.; Genova, H.; DeLuca, J. A randomized controlled trial to treat impaired learning and memory in multiple sclerosis: The self-GEN trial. Mult. Scler. 2018, 24, 1096–1104. [Google Scholar] [CrossRef]
- Sandroff, B.M.; Motl, R.W.; Deluca, J. The Influence of Cognitive Impairment on the Fitness-Cognition Relationship in Multiple Sclerosis. Med. Sci. Sport. Exerc. 2017, 49, 1184–1189. [Google Scholar] [CrossRef] [PubMed]
- Geisler, M.W.; Sliwinski, M.; Coyle, P.K.; Masur, D.M.; Doscher, C.; Krupp, L.B. The effects of amantadine and pemoline on cognitive functioning in multiple sclerosis. Arch. Neurol. 1996, 53, 185–188. [Google Scholar] [CrossRef]
- Morrow, S.A.; Rosehart, H.; Johnson, A.M. The effect of Fampridine-SR on cognitive fatigue in a randomized double-blind crossover trial in patients with MS. Mult. Scler. Relat. Disord. 2017, 11, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Sumowski, J.F.; Chiaravalloti, N.; Erlanger, D.; Kaushik, T.; Benedict, R.H.; DeLuca, J. L-amphetamine improves memory in MS patients with objective memory impairment. Mult. Scler. 2011, 17, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Morrow, S.A.; Smerbeck, A.; Patrick, K.; Cookfair, D.; Weinstock-Guttman, B.; Benedict, R.H. Lisdexamfetamine dimesylate improves processing speed and memory in cognitively impaired MS patients: A phase II study. J. Neurol. 2013, 260, 489–497. [Google Scholar] [CrossRef]
- Peyro Saint Paul, L.; Creveuil, C.; Heinzlef, O.; De Seze, J.; Vermersch, P.; Castelnovo, G.; Cabre, P.; Debouverie, M.; Brochet, B.; Dupuy, B.; et al. Efficacy and safety profile of memantine in patients with cognitive impairment in multiple sclerosis: A randomized, placebo-controlled study. J. Neurol. Sci. 2016, 363, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Huolman, S.; Hämäläinen, P.; Vorobyev, V.; Ruutiainen, J.; Parkkola, R.; Laine, T.; Hämäläinen, H. The effects of rivastigmine on processing speed and brain activation in patients with multiple sclerosis and subjective cognitive fatigue. Mult. Scler. 2011, 17, 1351–1361. [Google Scholar] [CrossRef]
- Krupp, L.B.; Christodoulou, C.; Melville, P.; Scherl, W.F.; MacAllister, W.S.; Elkins, L.E. Donepezil improved memory in multiple sclerosis in a randomized clinical trial. Neurology 2004, 63, 1579–1585. [Google Scholar] [CrossRef]
- Lovera, J.F.; Kim, E.; Heriza, E.; Fitzpatrick, M.; Hunziker, J.; Turner, A.P.; Adams, J.; Stover, T.; Sangeorzan, A.; Sloan, A.; et al. Ginkgo biloba does not improve cognitive function in MS: A randomized placebo-controlled trial. Neurology 2012, 79, 1278–1284. [Google Scholar] [CrossRef]
- Veauthier, C.; Radbruch, H.; Gaede, G.; Pfueller, C.F.; Dörr, J.; Bellmann-Strobl, J.; Wernecke, K.D.; Zipp, F.; Paul, F.; Sieb, J.P. Fatigue in multiple sclerosis is closely related to sleep disorders: A polysomnographic cross-sectional study. Mult. Scler. 2011, 17, 613–622. [Google Scholar] [CrossRef]
- Murphy, R.; O’Donoghue, S.; Counihan, T.; McDonald, C.; Calabresi, P.A.; Ahmed, M.A.; Kaplin, A.; Hallahan, B. Neuropsychiatric syndromes of multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2017, 88, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Arnett, P.A.; Higginson, C.I.; Randolph, J.J. Depression in multiple sclerosis: Relationship to planning ability. J. Int. Neuropsychol. Soc. 2001, 7, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Arnett, P.A.; Higginson, C.I.; Voss, W.D.; Bender, W.I.; Wurst, J.M.; Tippin, J.M. Depression in multiple sclerosis: Relationship to working memory capacity. Neuropsychology 1999, 13, 546–556. [Google Scholar] [CrossRef]
- Arnett, P.A.; Higginson, C.I.; Voss, W.D.; Wright, B.; Bender, W.I.; Wurst, J.M.; Tippin, J.M. Depressed mood in multiple sclerosis: Relationship to capacity-demanding memory and attentional functioning. Neuropsychology 1999, 13, 434–446. [Google Scholar] [CrossRef] [PubMed]
- Morrow, S.A.; Rosehart, H.; Pantazopoulos, K. Anxiety and Depressive Symptoms Are Associated With Worse Performance on Objective Cognitive Tests in MS. J. Neuropsychiatry Clin. Neurosci. 2016, 28, 118–123. [Google Scholar] [CrossRef]
- Portaccio, E. Differential diagnosis, discerning depression from cognition. Acta Neurol. Scand. 2016, 134 (Suppl. 200), 14–18. [Google Scholar] [CrossRef]
- Patel, V.P.; Walker, L.A.; Feinstein, A. Processing speed and distractibility in multiple sclerosis: The role of sleep. Mult. Scler. Relat. Disord. 2017, 11, 40–42. [Google Scholar] [CrossRef]
- Braley, T.J.; Kratz, A.L.; Kaplish, N.; Chervin, R.D. Sleep and Cognitive Function in Multiple Sclerosis. Sleep 2016, 39, 1525–1533. [Google Scholar] [CrossRef]
- Sumowski, J.F.; Benedict, R.; Enzinger, C.; Filippi, M.; Geurts, J.J.; Hamalainen, P.; Hulst, H.; Inglese, M.; Leavitt, V.M.; Rocca, M.A.; et al. Cognition in multiple sclerosis: State of the field and priorities for the future. Neurology 2018, 90, 278–288. [Google Scholar] [CrossRef]
- Roar, M.; Illes, Z.; Sejbaek, T. Practice effect in Symbol Digit Modalities Test in multiple sclerosis patients treated with natalizumab. Mult. Scler. Relat. Disord. 2016, 10, 116–122. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Gillies, J.; Jaworski, M.G., 3rd; Wilding, G.E.; Youngs, M.; Weinstock-Guttman, B.; Benedict, R.H. Repeated forms, testing intervals, and SDMT performance in a large multiple sclerosis dataset. Mult. Scler. Relat. Disord. 2022, 68, 104375. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Type of Study | No. of Patients | Disease Form | Comparator (n) | Duration | Cognitive Outcome Measure | Results | Brain Atrophy Measure |
|---|---|---|---|---|---|---|---|---|
| Kappos et al., 2016 [40] | Post hoc analysis of 2 RCT FREEDOMS and FREEDOMS II (FTY) | 783 | RRMS | Placebo (773) | 2 y | PASAT | PASAT improvements in FTY groups compare to placebo p < 0.0001. | 37% higher BVL in placebo group. |
| Utz et al., 2016 [41] | Prospective (FTY) | 22 | RRMS | NTZ (11) IFN (7) | 1 y | SPART/SPARTDR/PASAT 3/digit span forward/digit span backward/spatial span forward/spatial span backward/logical memory/go–no-go RT/go–no-go errors/divided attentions/visual search RT/visual search MT | No differences between groups. SDMT and PASAT 3 improved longitudinally in all groups. | |
| Comi et al., 2017 [42] | Multicentre randomised study (FTY) | 97 | RRMS | IFN1b (30) | 18 m | Rao’s BRB-NT | RAO’s BRB-NT (0–18 months) improve significantly in both groups. No significant differences between groups. | PBVC significantly higher in IFN1b. |
| Cree et al., 2018 [43] | Phase 4 RCT PREFERMS (FTY) | 433 | RRMS | iDMTs (428) | 1 y | SDMT | Increases were greater with FTY than with iDMTs at all assessments, but the between-group differences were not significant except at last assessment among patients taking the oral test. | In FTY group, PBVC and cortical GM volume reductions were significantly lower. |
| Petsas et al., 2019 [44] | Prospective (FTY) | 32 | RRMS | None | 6 m | PASAT 2′/PASAT 3′ | Improvement compared to baseline p = 0.016 (PASAT 3′) and p = 0.01 (PASAT 2′). | 0.27% of BVL at the end of observation. |
| Comi et al., 2019 [39] | RCT phase 3 SUNBEAM (OZN) | 447 (OZN 1 mg); 451 (OZN 0.5 mg) | RRMS | IFN beta 1a (448) | 1 y | SDMT | Both OZN groups improved SDMT significantly compared to IFN. | Both OZN groups reduced BVL significantly compared to IFN. |
| Guevara et al., 2020 [45] | Prospective (FTY) | 8 | RRMS | TFL (4)/IFN (23)/GA (6) | 2 y | SDMT | At 1 year and 2 year, 16% (7/45) and 20% (8/45) of patients had a SDMT decreased 4 points or more, respectively. | In all patients from baseline to 1.8 years WM volume, peripheral GM and whole brain volume decreased significantly. |
| Honce et al., 2020 [46] | Prospective (FTY) | 44 | RRMS | GA (43) | 2 y | SDMT/PASAT 2′/CVLTII/BVMTR/COWAT/DKEFS | Significant improvement over time in both groups in most all cognitive assessments. No differences between groups except for DKEFS (better in FTY group). | No differences between the two groups in terms of annualised PBVC. |
| Preziosa et al., 2020 [47] | Prospective (FTY) | 25 | RRMS | NTZ (30) | 2 y | Rao’s BRB-NT | Both groups improved at the end of study. No differences between groups. | Progressive atrophy during observation. No differences between groups. |
| Bhattacharyya et al., 2020 [48] | Prospective (FTY) | 25 | RRMS | None | 2 y | PASAT/SDMT | Significant improvement in PASAT score. No changes in SDMT. | |
| Benedict et al., 2020 [49] | Secondary analysis of RCT phase 3 EXPAND (SIP) | 1099 | SPMS | Placebo | 2 y | SDMT, PASAT, BVMTR | SDMT improved in SIP group compared to placebo. SIP-treated patients were at significantly lower risk for having a 4-point sustained decrease in SDMT score. | |
| Deluca et al., 2020 [50] | Post hoc analysis of SUNBEAN (OZN) | 447 (OZN 1 mg); 451 (OZN 0.5 mg) | RRMS | IFN beta 1a (448) | 1 y | SDMT | Both OZN groups improved SDMT significantly compared to IFN (p < 0.05). | |
| Ozakbas et al., 2021 [51] | Real world prospective (FTY) | 356 | RRMS | None | 5 y | BICAMS | Significant improvement from baseline to year 5 on each BICAMS component. | |
| El Ayoubi et al., 2021 [52] | Prospective (FTY) | 71 | RRMS | Interferons (56) | 1 y | SDMT/MoCA/total recall/delayed recall | SDMT improved longitudinally in both groups. MoCA and total recall worsened in interferon group and improved in FTY. | |
| Langdon et al., 2021 [53] | Post hoc analysis of 2 RCTs FREEDOMS and FREEDOMS II (FTY) | 783 | RRMS | Placebo (773) | 10 y | PASAT 3 | PASAT 3 improvements in FTY groups compared to placebo p < 0.0001. | Low EDSS and low BV correlates with better PASAT results. |
| Leppert et al., 2022 [54] | Post hoc analysis of RCTs INFORMS and EXPAND (FTY and SIP) | 303 (FTY) 1272 (SIP) | PPMS and SPMS | Placebo (1033) | 2 and 3 y | PASAT/SDMT | High pNFL correlates with CI. FTY and SIP reduced pNFL p < 0.05 and p < 0.01 | High pNFL correlates with BVL. |
| Cree et al., 2022 [33] | Secondary analysis of RCT phase 3 EXPAND (SIP) and up to >5 y extension (ongoing) | 593 | SPMS | Placebo until y 2, then SIP. | 5 y | SDMT | Six-month CCW risk significantly lower in continuous SIP vs. placebo-SIP. | Continuous SIP has significantly lower PBVC and thalamic volume reduction. |
| Conway et al., 2022 [55] | Prospective (FTY) | 15 | RRMS | Healthy controls (5) | 1 y | BVMTR/ SDMT/ DKEFS/SRT | Significant improvement over time in SDMT, BVMTR (total recall), DKEFS (number letter switching) in RRMS group. No differences between groups. | Thalamic volume and cortical thickness are significant predictors of CI. |
| Glasmacher et al., 2022 [56] | Prospective (DMTS category 2 FTY and CLAD) | 10 (FTY) 13 (CLAD) | RRMS | Category 1 ATZ (25) and NTZ/Category 3 DMF (148) and TFL (11)/No DMTS (117) | 1 y | PASAT | Category 2 associated with significant improvement; Category 1 not associated with improvement or worsening; Category 3 associated with significant worsening. | |
| Hersh et al., 2022 [57] | Real-world prospective (FTY) | 541 | RRMS | DMF (632) | 1 y | PST | At baseline, FTY group had higher PST score. No significant changes over time between FTY and DMF groups. sNFL data available for some patients at single timepoint (7 months): higher levels in FTY group. |
| Study | Type of Study | No. of Patients | Disease Form | Comparator (n) | Duration | Cognitive Outcome Measure | Results | Brain atrophy Measure |
|---|---|---|---|---|---|---|---|---|
| Giovannoni et al., 2016 [58] | Integrated analysis of phase 3 RCTs (CONFIRM and DEFINE) | 769 | RRMS | Placebo (771) | 96 w | PASAT 3′ (mean change) | Mean change in PASAT 3′ z-scores was 0.178 for DMF and 0.123 for placebo (p = 0.0016). | |
| Al Iedani et al., 2018 [59] | Prospective | 20 | RRMS | Healthy controls | 2 y | SDMT | SDMT score stable at year 2 in MS patients. | No substantial change was observed in the average annualised rate of brain volume loss between 1st and 2nd year of treatment with DMF. |
| Montes Diaz et al., 2018 [60] | Prospective | 16 | RRMS | None | 1 y | PASAT | Significant improvement after 3 months. | |
| Amato et al., 2020 [61] | Prospective | 156 | RRMS | None | 2 y | Stroop test and BRB-NT | CI in 22.6% patients at baseline, in 27.2% at 1 year, and 9.7% at 2 years. Compared to year 1, 37.2% improved, 10.7% worsened, and 52.1% remained unchanged at 2 years. | |
| Hersh et al., 2022 [57] | Real-world prospective | 632 | RRMS | FTY (541) | 1 y | PST | At baseline, FTY group had higher PST score. No significant changes over time between FTY and DMF groups. sNFL data available for some patients: higher baseline levels in FTY group. | |
| Piervincenzi et al., 2022 [62] | Prospective | 27 | RRMS | None | 1 y | PASAT 3′, SDMT | PASAT improvement at month 12 (p = 0.022). SDMT unchanged. | −0.12% BVL at month 6; −0.24% at month 12. |
| Glasmacher et al., 2022 [56] | Prospective (DMTS category 3 DMF and TFL) | 148 (DMF) 11 (TFL) | RRMS | Category 1 ATZ (25) and NTZ/Category 2 FTY (10) and CLAD (13)/No DMTS (117) | 1 y | PASAT | Category 2 associated with significant improvement; Category 1 not associated with improvement or worsening. Category 3 associated with significant worsening. |
| Study | Type of Study | No. of Patients | Disease Form | Comparator (n) | Duration | Cognitive Outcome Measure | Results | Brain atrophy Measure |
|---|---|---|---|---|---|---|---|---|
| Coyle et al., 2018 [64] | Open-label multicentre Phase IV Study (Teri PRO) | 594 | RRMS | None | 2 y | SDMT | SDMT results remained stable at week 48. CI reported by patients on MSPS remained stable. | |
| Guevara et al., 2020 [45] | Prospective | 4 | RRMS | FTY (8)/IFN (23)/GA (6) | 2 y | SDMT | At 1 year and 2 year, 16% (7/45) and 20% (8/45) of patients had a SDMT decreased 4 points or more, respectively. | In all patients from baseline to 1.8 years after baseline, WM volume, peripheral GM, and whole brain volume decreased significantly. |
| Corallo et al., 2021 [65] | Prospective | 30 | RRMS | Healthy controls (30) | 1 y | Rao’s BRB-NT | No significant changes from baseline in each cognitive test of BRB-NT. | Mild increase in GM volume. No WM volume loss. |
| Bencsik et al., 2022 [66] | Real-world study (TERI REAL) analysis | 146 | RRMS | None | 2 y | BICAMS | Mild improvement at month 12 and 24 p < 0.05 of each BICAMS component. | |
| Sprenger et al., 2022 [63] | Post hoc analysis of RCT TEMSO and its extension | 235 | RRMS | Placebo | 252 w | PASAT 3′ | PASAT 3′ Z-scores increased through week 252 post-TFL initiation. Patients who received 14 mg TFL in the core study and extension had higher PASAT 3′ Z-scores through week 252 compared with those who switched at the extension. | Lower BVL on TFL treatment correlated with higher PASAT 3′ scores. |
| Glasmacher et al., 2022 [56] | Prospective (DMTs Category 3 DMF and TFL) | 148 (DMF) 11 (TFL) | RRMS | Category 1 ATZ (25) and NTZ/Category 2 FTY (10) and CLAD (13)/no DMTs (117) | 1 y | PASAT | Category 2 associated with significant improvement; Category 1 not associated with improvement or worsening; Category 3 associated with significant worsening. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlomagno, V.; Mirabella, M.; Lucchini, M. Current Status of Oral Disease-Modifying Treatment Effects on Cognitive Outcomes in Multiple Sclerosis: A Scoping Review. Bioengineering 2023, 10, 848. https://doi.org/10.3390/bioengineering10070848
Carlomagno V, Mirabella M, Lucchini M. Current Status of Oral Disease-Modifying Treatment Effects on Cognitive Outcomes in Multiple Sclerosis: A Scoping Review. Bioengineering. 2023; 10(7):848. https://doi.org/10.3390/bioengineering10070848
Chicago/Turabian StyleCarlomagno, Vincenzo, Massimiliano Mirabella, and Matteo Lucchini. 2023. "Current Status of Oral Disease-Modifying Treatment Effects on Cognitive Outcomes in Multiple Sclerosis: A Scoping Review" Bioengineering 10, no. 7: 848. https://doi.org/10.3390/bioengineering10070848
APA StyleCarlomagno, V., Mirabella, M., & Lucchini, M. (2023). Current Status of Oral Disease-Modifying Treatment Effects on Cognitive Outcomes in Multiple Sclerosis: A Scoping Review. Bioengineering, 10(7), 848. https://doi.org/10.3390/bioengineering10070848