
Per- and Polyfluoroalkyl Substances and Breastfeeding as a Vulnerable Function: A Systematic Review of Epidemiological Studies
 ,
,  , ,
, ,
Abstract
1. Introduction
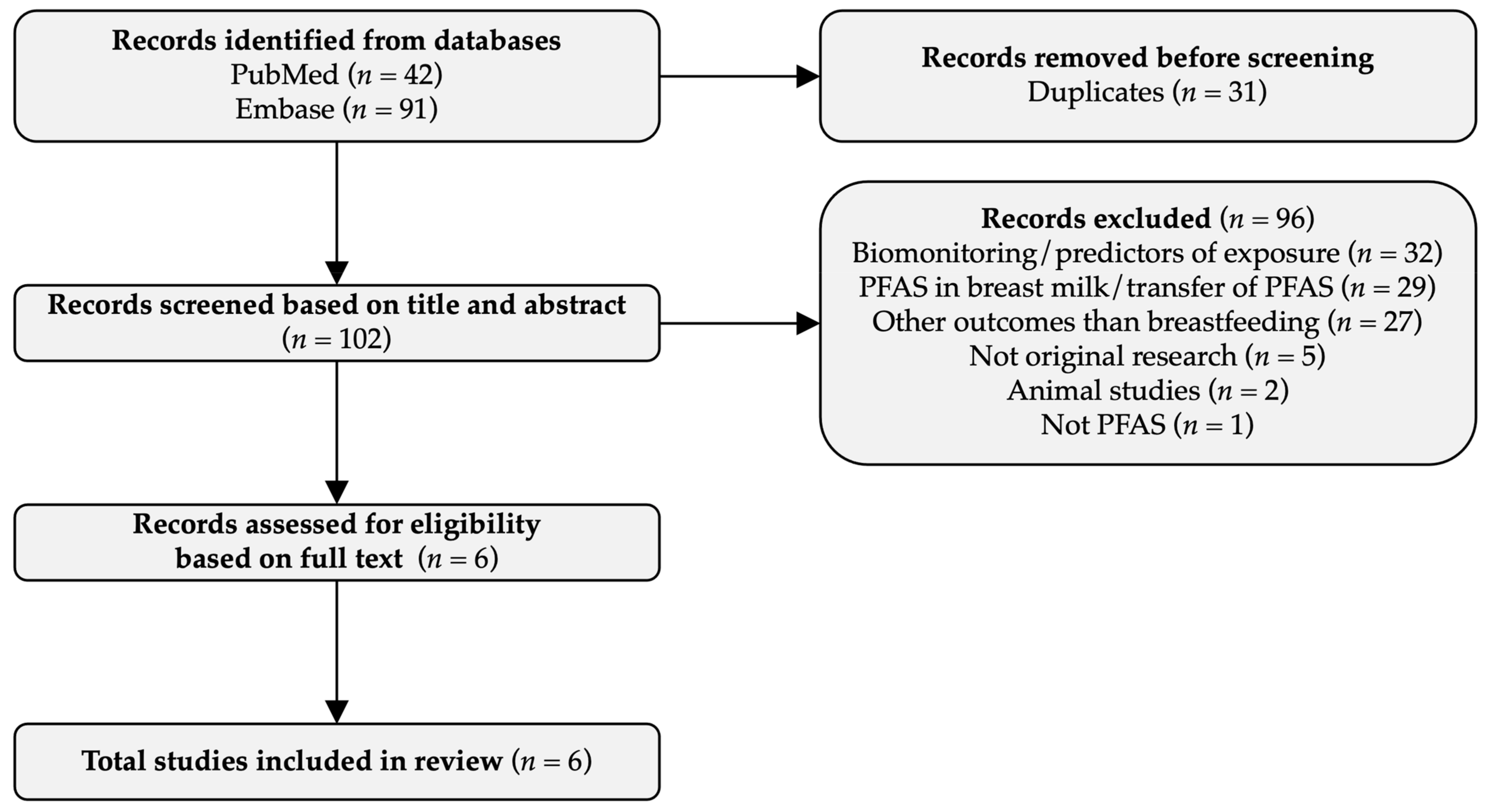
2. Materials and Methods
3. Results
3.1. Study Characteristics
3.2. Study Risk of Bias Assessment
3.3. Breastfeeding Initiation
3.4. Exclusive Breastfeeding
3.5. Total Breastfeeding
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Breastfeeding. 2022. Available online: https://www.who.int/health-topics/breastfeeding#tab=tab_1 (accessed on 14 March 2022).
- Andreas, N.J.; Kampmann, B.; Le-Doare, K.M. Human breast milk: A review on its composition and bioactivity. Early Hum. Dev. 2015, 91, 629–635. [Google Scholar] [CrossRef]
- Kalbermatter, C.; Fernandez Trigo, N.; Christensen, S.; Ganal-Vonarburg, S.C. Maternal Microbiota, Early Life Colonization and Breast Milk Drive Immune Development in the Newborn. Front. Immunol. 2021, 12, 683022. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Victora, C.G. Short-Term Effects of Breastfeeding: A Systematic Review of the Benefits of Breastfeeding on Diarhoea and Pneumonia Mortality; World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- Sankar, M.J.; Sinha, B.; Chowdhury, R.; Bhandari, N.; Taneja, S.; Martines, J.; Bahl, R. Optimal breastfeeding practices and infant and child mortality: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Soled, D.; Keim, S.A.; Rapoport, E.; Rosen, L.; Adesman, A. Breastfeeding Is Associated with a Reduced Risk of Attention-Deficit/Hyperactivity Disorder Among Preschool Children. J. Dev. Behav. Pediatr. 2021, 42, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Saravia-Bartra, M.M.; Cazorla, P.; Ignacio-Cconchoy, F.L.; Cazorla-Saravia, P. Exclusive breastfeeding as a protective factor of acute lymphoblastic leukemia. Andes Pediatr. 2021, 92, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; de Sousa, B.A.; de Mola, C.L. Breastfeeding and neurodevelopmental outcomes. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 174–178. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 96–113. [Google Scholar] [CrossRef]
- World Health Organisation. Infant and Young Child Feeding. 9 June 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding (accessed on 11 March 2022).
- Meek, J.Y.; Noble, L.; Section on Breastfeeding. Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics 2022, 150, e2022057988. [Google Scholar] [CrossRef]
- Stuebe, A.M.; Horton, B.J.; Chetwynd, E.; Watkins, S.; Grewen, K.; Meltzer-Brody, S. Prevalence and risk factors for early, undesired weaning attributed to lactation dysfunction. J. Womens Health 2014, 23, 404–412. [Google Scholar] [CrossRef]
- Wambach, K.; Campbell, S.H.; Gill, S.L.; Dodgson, J.E.; Abiona, T.C.; Heinig, M.J. Clinical lactation practice: 20 years of evidence. J. Hum. Lact. 2005, 21, 245–258. [Google Scholar] [CrossRef]
- Ahluwalia, I.B.; Morrow, B.; Hsia, J. Why do women stop breastfeeding? Findings from the Pregnancy Risk Assessment and Monitoring System. Pediatrics 2005, 116, 1408–1412. [Google Scholar] [CrossRef]
- Li, R.; Fein, S.B.; Chen, J.; Grummer-Strawn, L.M. Why mothers stop breastfeeding: Mothers’ self-reported reasons for stopping during the first year. Pediatrics 2008, 122 (Suppl. 2), S69–S76. [Google Scholar] [CrossRef]
- Gianni, M.L.; Bettinelli, M.E.; Manfra, P.; Sorrentino, G.; Bezze, E.; Plevani, L.; Cavallaro, G.; Raffaeli, G.; Crippa, B.L.; Colombo, L.; et al. Breastfeeding Difficulties and Risk for Early Breastfeeding Cessation. Nutrients 2019, 11, 2266. [Google Scholar] [CrossRef]
- Lechosa-Muniz, C.; Paz-Zulueta, M.; Cayón-De las Cuevas, J.; Llorca, J.; Cabero-Pérez, M.J. Declared Reasons for Cessation of Breastfeeding during the First Year of Life: An Analysis Based on a Cohort Study in Northern Spain. Int. J. Environ. Res. Public Health 2021, 18, 8414. [Google Scholar] [CrossRef]
- Hannan, F.M.; Elajnaf, T.; Vandenberg, L.N.; Kennedy, S.H.; Thakker, R.V. Hormonal regulation of mammary gland development and lactation. Nat. Rev. Endocrinol. 2023, 19, 46–61. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Perfluoroalkyls. Draft for Public Comment; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Sunderland, E.M.; Hu, X.C.; Dassuncao, C.; Tokranov, A.K.; Wagner, C.C.; Allen, J.G. A review of the pathways of human exposure to poly- and perfluoroalkyl substances (PFASs) and present understanding of health effects. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 131–147. [Google Scholar] [CrossRef]
- EFSA CONTAM Panel; Schrenk, D.; Bignami, M.; Bodin, L.; Chipman, J.K.; del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Hoogenboom, L.; Leblanc, J.C.; et al. Risk to human health related to the presence of perfluoroalkyl substances in food. EFSA J. 2020, 18, e06223. [Google Scholar]
- United Nations Environment Programme. PFASs Listed under the Stockholm Convention. 2022. Available online: http://chm.pops.int/Implementation/IndustrialPOPs/PFAS/Overview/tabid/5221/Default.aspx (accessed on 19 August 2022).
- Rickard, B.P.; Rizvi, I.; Fenton, S.E. Per- and poly-fluoroalkyl substances (PFAS) and female reproductive outcomes: PFAS elimination, endocrine-mediated effects, and disease. Toxicology 2022, 465, 153031. [Google Scholar] [CrossRef]
- Fenton, S.E.; Ducatman, A.; Boobis, A.; DeWitt, J.C.; Lau, C.; Ng, C.; Smith, J.S.; Roberts, S.M. Per- and Polyfluoroalkyl Substance Toxicity and Human Health Review: Current State of Knowledge and Strategies for Informing Future Research. Environ. Toxicol. Chem. 2021, 40, 606–630. [Google Scholar] [CrossRef]
- Zheng, P.; Liu, Y.; An, Q.; Yang, X.; Yin, S.; Ma, L.Q.; Liu, W. Prenatal and postnatal exposure to emerging and legacy per-/polyfluoroalkyl substances: Levels and transfer in maternal serum, cord serum, and breast milk. Sci. Total Environ. 2022, 812, 152446. [Google Scholar] [CrossRef] [PubMed]
- Mogensen, U.B.; Grandjean, P.; Nielsen, F.; Weihe, P.; Budtz-Jørgensen, E. Breastfeeding as an Exposure Pathway for Perfluorinated Alkylates. Environ. Sci. Technol. 2015, 49, 10466–10473. [Google Scholar] [CrossRef] [PubMed]
- Verner, M.A.; Ngueta, G.; Jensen, E.T.; Fromme, H.; Völkel, W.; Nygaard, U.C.; Granum, B.; Longnecker, M.P. A Simple Pharmacokinetic Model of Prenatal and Postnatal Exposure to Perfluoroalkyl Substances (PFASs). Environ. Sci. Technol. 2016, 50, 978–986. [Google Scholar] [CrossRef]
- Muller, M.H.B.; Polder, A.; Brynildsrud, O.B.; Grønnestad, R.; Karimi, M.; Lie, E.; Manyilizu, W.B.; Mdegela, R.H.; Mokiti, F.; Murtadha, M.; et al. Prenatal exposure to persistent organic pollutants in Northern Tanzania and their distribution between breast milk, maternal blood, placenta and cord blood. Environ. Res. 2019, 170, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Criswell, R.L.; Wang, Y.; Christensen, B.; Botelho, J.C.; Calafat, A.M.; Peterson, L.A.; Huset, C.A.; Karagas, M.R.; Romano, M.E. Concentrations of Per- and Polyfluoroalkyl Substances in Paired Maternal Plasma and Human Milk in the New Hampshire Birth Cohort. Environ. Sci. Technol. 2023, 57, 463–472. [Google Scholar] [CrossRef]
- ATSDR. Toxicological Profile for Perfluoroalkyls; Agency for Toxic Substances and Disease Registry (ATSDR): Atlanta, GA, USA, 2021.
- Zhang, X.; Xue, L.; Deji, Z.; Wang, X.; Liu, P.; Lu, J.; Zhou, R.; Huang, Z. Effects of exposure to per- and polyfluoroalkyl substances on vaccine antibodies: A systematic review and meta-analysis based on epidemiological studies. Environ. Pollut. 2022, 306, 119442. [Google Scholar] [CrossRef]
- Grandjean, P.; Heilmann, C.; Weihe, P.; Nielsen, F.; Mogensen, U.B.; Timmermann, A.; Budtz-Jørgensen, E. Estimated exposures to perfluorinated compounds in infancy predict attenuated vaccine antibody concentrations at age 5-years. J. Immunotoxicol. 2017, 14, 188–195. [Google Scholar] [CrossRef]
- Lau, C.; Thibodeaux, J.R.; Hanson, R.G.; Narotsky, M.G.; Rogers, J.M.; Lindstrom, A.B.; Strynar, M.J. Effects of perfluorooctanoic acid exposure during pregnancy in the mouse. Toxicol. Sci. 2006, 90, 510–518. [Google Scholar] [CrossRef]
- White, S.S.; Calafat, A.M.; Kuklenyik, Z.; Villanueva, L.; Zehr, R.D.; Helfant, L.; Strynar, M.J.; Lindstrom, A.B.; Thibodeaux, J.R.; Wood, C.; et al. Gestational PFOA exposure of mice is associated with altered mammary gland development in dams and female offspring. Toxicol. Sci. 2007, 96, 133–144. [Google Scholar] [CrossRef]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121 Pt 1, 1027–1031. [Google Scholar] [CrossRef]
- ROBINS-E Development, Group; Higgins, J.; Morgan, R.; Rooney, A.; Taylor, K.; Thayer, K.; Silva, R.; Lemeris, C.; Akl, A.; Arroyave, W.; et al. Risk Of Bias In Non-randomized Studies-of Exposure (ROBINS-E). Launch Version. 2022. Available online: https://www.riskofbias.info/welcome/robins-e-tool (accessed on 21 March 2023).
- Lauritzen, H.B.; Larose, T.L.; Øien, T.; Odland, J.Ø.; Van de Bor, M.; Jacobsen, G.W.; Sandanger, T.M. Factors Associated with Maternal Serum Levels of Perfluoroalkyl Substances and Organochlorines: A Descriptive Study of Parous Women in Norway and Sweden. PLoS ONE 2016, 11, e0166127. [Google Scholar] [CrossRef]
- Kronborg, H.; Foverskov, E.; Væth, M.; Maimburg, R.D. The role of intention and self-efficacy on the association between breastfeeding of first and second child, a Danish cohort study. BMC Pregnancy Childbirth 2018, 18, 454. [Google Scholar] [CrossRef]
- Fei, C.; McLaughlin, J.K.; Lipworth, L.; Olsen, J. Maternal concentrations of perfluorooctanesulfonate (PFOS) and perfluorooctanoate (PFOA) and duration of breastfeeding. Scand. J. Work Environ. Health 2010, 36, 413–421. [Google Scholar] [CrossRef]
- Nielsen, C.; Li, Y.; Lewandowski, M.; Fletcher, T.; Jakobsson, K. Breastfeeding initiation and duration after high exposure to perfluoroalkyl substances through contaminated drinking water: A cohort study from Ronneby, Sweden. Environ. Res. 2022, 207, 112206. [Google Scholar] [CrossRef]
- Rosen, E.M.; Brantsæter, A.L.; Carroll, R.; Haug, L.S.; Singer, A.B.; Zhao, S.; Ferguson, K.K. Maternal Plasma Concentrations of Per- and polyfluoroalkyl Substances and Breastfeeding Duration in the Norwegian Mother and Child Cohort. Environ. Epidemiol. 2018, 2, e027. [Google Scholar] [CrossRef]
- Timmermann, C.A.G.; Andersen, M.S.; Budtz-Jørgensen, E.; Boye, H.; Nielsen, F.; Jensen, R.C.; Bruun, S.; Husby, S.; Grandjean, P.; Jensen, T.K. Pregnancy Exposure to Perfluoroalkyl Substances and Associations With Prolactin Concentrations and Breastfeeding in the Odense Child Cohort. J. Clin. Endocrinol. Metab. 2022, 107, e631–e642. [Google Scholar] [CrossRef]
- Timmermann, C.A.G.; Budtz-Jørgensen, E.; Petersen, M.S.; Weihe, P.; Steuerwald, U.; Nielsen, F.; Jensen, T.K.; Grandjean, P. Shorter duration of breastfeeding at elevated exposures to perfluoroalkyl substances. Reprod. Toxicol. 2017, 68, 164–170. [Google Scholar] [CrossRef]
- Romano, M.E.; Xu, Y.; Calafat, A.M.; Yolton, K.; Chen, A.; Webster, G.M.; Eliot, M.N.; Howard, C.R.; Lanphear, B.P.; Braun, J.M. Maternal serum perfluoroalkyl substances during pregnancy and duration of breastfeeding. Environ. Res. 2016, 149, 239–246. [Google Scholar] [CrossRef]
- Mondal, D.; Weldon, R.H.; Armstrong, B.G.; Gibson, L.J.; Lopez-Espinosa, M.J.; Shin, H.M.; Fletcher, T. Breastfeeding: A potential excretion route for mothers and implications for infant exposure to perfluoroalkyl acids. Environ. Health Perspect. 2014, 122, 187–192. [Google Scholar] [CrossRef]
- Papadopoulou, E.; Sabaredzovic, A.; Namork, E.; Nygaard, U.C.; Granum, B.; Haug, L.S. Exposure of Norwegian toddlers to perfluoroalkyl substances (PFAS): The association with breastfeeding and maternal PFAS concentrations. Environ. Int. 2016, 94, 687–694. [Google Scholar] [CrossRef]
- Kärrman, A.; Ericson, I.; van Bavel, B.; Darnerud, P.O.; Aune, M.; Glynn, A.; Lignell, S.; Lindström, G. Exposure of perfluorinated chemicals through lactation: Levels of matched human milk and serum and a temporal trend, 1996–2004, in Sweden. Environ. Health Perspect. 2007, 115, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Von Holst, H.; Nayak, P.; Dembek, Z.; Buehler, S.; Echeverria, D.; Fallacara, D.; John, L. Perfluoroalkyl substances exposure and immunity, allergic response, infection, and asthma in children: Review of epidemiologic studies. Heliyon 2021, 7, e08160. [Google Scholar] [CrossRef] [PubMed]
- Liew, Z.; Goudarzi, H.; Oulhote, Y. Developmental Exposures to Perfluoroalkyl Substances (PFASs): An Update of Associated Health Outcomes. Curr. Environ. Health Rep. 2018, 5, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Kunz, C.; Rodriquez-Palmero, M.; Koletzko, B.; Jensen, R. Nutritional and biochemical properties of human milk, Part I: General aspects, proteins, and carbohydrates. Clin. Perinatol. 1999, 26, 307–333. [Google Scholar] [CrossRef] [PubMed]
- Abraham, K.; Mielke, H.; Fromme, H.; Völkel, W.; Menzel, J.; Peiser, M.; Zepp, F.; Willich, S.N.; Weikert, C. Internal exposure to perfluoroalkyl substances (PFASs) and biological markers in 101 healthy 1-year-old children: Associations between levels of perfluorooctanoic acid (PFOA) and vaccine response. Arch. Toxicol. 2020, 94, 2131–2147. [Google Scholar] [CrossRef]
- Forns, J.; Verner, M.A.; Iszatt, N.; Nowack, N.; Bach, C.C.; Vrijheid, M.; Costa, O.; Andiarena, A.; Sovcikova, E.; Høyer, B.B.; et al. Early Life Exposure to Perfluoroalkyl Substances (PFAS) and ADHD: A Meta-Analysis of Nine European Population-Based Studies. Environ. Health Perspect. 2020, 128, 57002. [Google Scholar] [CrossRef]
- Varsi, K.; Torsvik, I.K.; Huber, S.; Averina, M.; Brox, J.; Bjørke-Monsen, A.L. Impaired gross motor development in infants with higher PFAS concentrations. Environ. Res. 2022, 204 Pt D, 112392. [Google Scholar] [CrossRef]
- Timmermann, C.A.G.; Jensen, K.J.; Nielsen, F.; Budtz-Jørgensen, E.; van der Klis, F.; Benn, C.S.; Grandjean, P.; Fisker, A.B. Serum Perfluoroalkyl Substances, Vaccine Responses, and Morbidity in a Cohort of Guinea-Bissau Children. Environ. Health Perspect. 2020, 128, 87002. [Google Scholar] [CrossRef]
- Timmermann, C.A.G.; Pedersen, H.S.; Weihe, P.; Bjerregaard, P.; Nielsen, F.; Heilmann, C.; Grandjean, P. Concentrations of tetanus and diphtheria antibodies in vaccinated Greenlandic children aged 7–12 years exposed to marine pollutants, a cross sectional study. Environ. Res. 2022, 203, 111712. [Google Scholar] [CrossRef]
- Gladen, B.C.; Rogan, W.J. DDE and shortened duration of lactation in a northern Mexican town. Am. J. Public Health 1995, 85, 504–508. [Google Scholar] [CrossRef]
- Rogan, W.J.; Gladen, B.C.; McKinney, J.D.; Carreras, N.; Hardy, P.; Thullen, J.; Tingelstad, J.; Tully, M.A. Polychlorinated biphenyls (PCBs) and dichlorodiphenyl dichloroethene (DDE) in human milk: Effects on growth, morbidity, and duration of lactation. Am. J. Public Health 1987, 77, 1294–1297. [Google Scholar] [CrossRef]
- Kasper, N.; Peterson, K.E.; Zhang, Z.; Ferguson, K.K.; Sánchez, B.N.; Cantoral, A.; Meeker, J.D.; Téllez-Rojo, M.M.; Pawlowski, C.M.; Ettinger, A.S. Association of Bisphenol A Exposure with Breastfeeding and Perceived Insufficient Milk Supply in Mexican Women. Matern. Child Health J. 2016, 20, 1713–1719. [Google Scholar] [CrossRef]
- Mehlsen, A.; Høllund, L.; Boye, H.; Frederiksen, H.; Andersson, A.M.; Bruun, S.; Husby, S.; Jensen, T.K.; Timmermann, C.A. Pregnancy exposure to bisphenol A and duration of breastfeeding. Environ. Res. 2022, 206, 112471. [Google Scholar] [CrossRef]
- White, S.S.; Stanko, J.P.; Kato, K.; Calafat, A.M.; Hines, E.P.; Fenton, S.E. Gestational and chronic low-dose PFOA exposures and mammary gland growth and differentiation in three generations of CD-1 mice. Environ. Health Perspect. 2011, 119, 1070–1076. [Google Scholar] [CrossRef]
- Macon, M.B.; Villanueva, L.R.; Tatum-Gibbs, K.; Zehr, R.D.; Strynar, M.J.; Stanko, J.P.; White, S.S.; Helfant, L.; Fenton, S.E. Prenatal perfluorooctanoic acid exposure in CD-1 mice: Low-dose developmental effects and internal dosimetry. Toxicol. Sci. 2011, 122, 134–145. [Google Scholar] [CrossRef]
- Tucker, D.K.; Macon, M.B.; Strynar, M.J.; Dagnino, S.; Andersen, E.; Fenton, S.E. The mammary gland is a sensitive pubertal target in CD-1 and C57Bl/6 mice following perinatal perfluorooctanoic acid (PFOA) exposure. Reprod. Toxicol. 2015, 54, 26–36. [Google Scholar] [CrossRef]
- White, S.S.; Kato, K.; Jia, L.T.; Basden, B.J.; Calafat, A.M.; Hines, E.P.; Stanko, J.P.; Wolf, C.J.; Abbott, B.D.; Fenton, S.E. Effects of perfluorooctanoic acid on mouse mammary gland development and differentiation resulting from cross-foster and restricted gestational exposures. Reprod. Toxicol. 2009, 27, 289–298. [Google Scholar] [CrossRef]
- Cope, H.A.; Blake, B.E.; Love, C.; McCord, J.; Elmore, S.A.; Harvey, J.B.; Chappell, V.A.; Fenton, S.E. Latent, sex-specific metabolic health effects in CD-1 mouse offspring exposed to PFOA or HFPO-DA (GenX) during gestation. Emerg. Contam. 2021, 7, 219–235. [Google Scholar] [CrossRef]
- Edwards, T. An Oral (Gavage) Reproduction/Developmental Toxicity Screening Study of H-28548 in Mice (DuPont); WIL Research Laboratories, LLC: Ashland, OH, USA, 2010. [Google Scholar]
- Itoh, S.; Araki, A.; Mitsui, T.; Miyashita, C.; Goudarzi, H.; Sasaki, S.; Cho, K.; Nakazawa, H.; Iwasaki, Y.; Shinohara, N.; et al. Association of perfluoroalkyl substances exposure in utero with reproductive hormone levels in cord blood in the Hokkaido Study on Environment and Children’s Health. Environ. Int. 2016, 94, 51–59. [Google Scholar] [CrossRef]
- Lee, C.K.; Kang, S.G.; Lee, J.T.; Lee, S.W.; Kim, J.H.; Kim, D.H.; Son, B.C.; Kim, K.H.; Suh, C.H.; Kim, S.Y.; et al. Effects of perfluorooctane sulfuric acid on placental PRL-family hormone production and fetal growth retardation in mice. Mol. Cell. Endocrinol. 2015, 401, 165–172. [Google Scholar] [CrossRef]
- Yang, Q.; Kurotani, R.; Yamada, A.; Kimura, S.; Gonzalez, F.J. Peroxisome proliferator-activated receptor alpha activation during pregnancy severely impairs mammary lobuloalveolar development in mice. Endocrinology 2006, 147, 4772–4780. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Chen, Q. Mediating Roles of PPARs in the Effects of Environmental Chemicals on Sex Steroids. PPAR Res. 2017, 2017, 3203161. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.M.; Vaught, D.B.; Joly, M.M.; Hicks, D.J.; Sanchez, V.; Owens, P.; Rahman, B.; Elion, D.L.; Balko, J.M.; Cook, R.S. ErbB3 drives mammary epithelial survival and differentiation during pregnancy and lactation. Breast Cancer Res. 2017, 19, 105. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.; Harlow, S.D.; Randolph, J.F., Jr.; Loch-Caruso, R.; Park, S.K. Perfluoroalkyl and polyfluoroalkyl substances (PFAS) and their effects on the ovary. Hum. Reprod. Update 2020, 26, 724–752. [Google Scholar] [CrossRef] [PubMed]
- Hapon, M.B.; Simoncini, M.; Via, G.; Jahn, G.A. Effect of hypothyroidism on hormone profiles in virgin, pregnant and lactating rats, and on lactation. Reproduction 2003, 126, 371–382. [Google Scholar] [CrossRef]
- Boesen, S.A.H.; Long, M.; Wielsøe, M.; Mustieles, V.; Fernandez, M.F.; Bonefeld-Jørgensen, E.C. Exposure to Perflouroalkyl acids and foetal and maternal thyroid status: A review. Environ. Health 2020, 19, 107. [Google Scholar] [CrossRef]
- Davidsen, N.; Ramhøj, L.; Lykkebo, C.A.; Kugathas, I.; Poulsen, R.; Rosenmai, A.K.; Evrard, B.; Darde, T.A.; Axelstad, M.; Bahl, M.I.; et al. PFOS-induced thyroid hormone system disrupted rats display organ-specific changes in their transcriptomes. Environ. Pollut. 2022, 305, 119340. [Google Scholar] [CrossRef]
- Bruun, S.; Buhl, S.; Husby, S.; Jacobsen, L.N.; Michaelsen, K.F.; Sørensen, J.; Zachariassen, G. Breastfeeding, Infant Formula, and Introduction to Complementary Foods-Comparing Data Obtained by Questionnaires and Health Visitors’ Reports to Weekly Short Message Service Text Messages. Breastfeed. Med. 2017, 12, 554–560. [Google Scholar] [CrossRef]
- Newhook, J.T.; Newhook, L.A.; Midodzi, W.K.; Murphy Goodridge, J.; Burrage, L.; Gill, N.; Halfyard, B.; Twells, L. Poverty and Breastfeeding: Comparing Determinants of Early Breastfeeding Cessation Incidence in Socioeconomically Marginalized and Privileged Populations in the FiNaL Study. Health Equity 2017, 1, 96–102. [Google Scholar] [CrossRef]
- Buekers, J.; Colles, A.; Cornelis, C.; Morrens, B.; Govarts, E.; Schoeters, G. Socio-Economic Status and Health: Evaluation of Human Biomonitored Chemical Exposure to Per- and Polyfluorinated Substances across Status. Int. J. Environ. Res. Public Health 2018, 15, 2818. [Google Scholar] [CrossRef]
- Weisskopf, M.G.; Webster, T.F. Trade-offs of Personal Versus More Proxy Exposure Measures in Environmental Epidemiology. Epidemiology 2017, 28, 635–643. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Olsen, G.W.; Burris, J.M.; Ehresman, D.J.; Froehlich, J.W.; Seacat, A.M.; Butenhoff, J.L.; Zobel, L.R. Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ. Health Perspect. 2007, 115, 1298–1305. [Google Scholar] [CrossRef]
- Chen, L.; Tong, C.; Huo, X.; Zhang, J.; Tian, Y.; Cohort, S.B. Prenatal exposure to perfluoroalkyl and polyfluoroalkyl substances and birth outcomes: A longitudinal cohort with repeated measurements. Chemosphere 2021, 267, 128899. [Google Scholar] [CrossRef]
- Banwell, C.; Housen, T.; Smurthwaite, K.; Trevenar, S.; Walker, L.; Todd, K.; Rosas, M.; Kirk, M. Health and social concerns about living in three communities affected by per- and polyfluoroalkyl substances (PFAS): A qualitative study in Australia. PLoS ONE 2021, 16, e0245141. [Google Scholar] [CrossRef]
- Cousins, I.T.; DeWitt, J.C.; Glüge, J.; Goldenman, G.; Herzke, D.; Lohmann, R.; Ng, C.A.; Scheringer, M.; Wang, Z. The high persistence of PFAS is sufficient for their management as a chemical class. Environ. Sci. Process. Impacts 2020, 22, 2307–2312. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Guidance on PFAS Exposure, Testing, and Clinical Follow-Up; National Academies Press: Washington, DC, USA, 2022. [Google Scholar]
- Post, G.B. Recent US State and Federal Drinking Water Guidelines for Per- and Polyfluoroalkyl Substances. Environ. Toxicol. Chem. 2020, 40, 550–563. [Google Scholar] [CrossRef]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Criswell, R.; Crawford, K.A.; Bucinca, H.; Romano, M.E. Endocrine-disrupting chemicals and breastfeeding duration: A review. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 388–395. [Google Scholar] [CrossRef]
- Lee, S.; Kelleher, S.L. Biological underpinnings of breastfeeding challenges: The role of genetics, diet, and environment on lactation physiology. Am. J. Physiol. Endocrinol. Metab. 2016, 311, E405–E422. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Facet 1 | PFAS Perfluoroalkyl substances Polyfluoroalkyl substances PFOS PFOA |
| Facet 2 | Breastfeeding (Title) Breast Feeding (Mesh/key term) |
| Restrictions | English language |
| Exclusions | Reviews |
| PubMed Search | (“PFAS” OR “Perfluoroalkyl Substances” OR “polyfluoroalkyl substances” OR “PFOS” OR “PFOA”) AND (“Breastfeeding” [Title] OR “Breast Feeding” [Mesh]) NOT (Review [Publication Type]) Filter: “English” |
| Embase (Ovid) Search | (1) PFAS.af. (2) Perfluoroalkyl Substances.af. (3) Polyfluoroalkyl substances.af. (4) PFOS.af. (5) PFOA.af. (6) Breastfeeding.m_titl. (7) exp breast feeding/ (8) 1 or 2 or 3 or 4 or 5 (9) 6 or 7 (10) 8 and 9 (11) limit 10 to English language (12) limit 11 to “review” (13) 11 not 12 |
| Population | Human: Pregnant women or new mothers |
| Exposure | Per- and polyfluoroalkyl substance (PFAS) exposure |
| Comparator | Increasing exposure or high versus low exposure |
| Outcomes | Total duration of breastfeeding Duration of exclusive breastfeeding Breastfeeding initiation |
| First Author (Publication Year) | Country | Study Design | N | PFAS Concentrations (Median, ng/mL) | Breastfeeding Duration (Median, Months) |
|---|---|---|---|---|---|
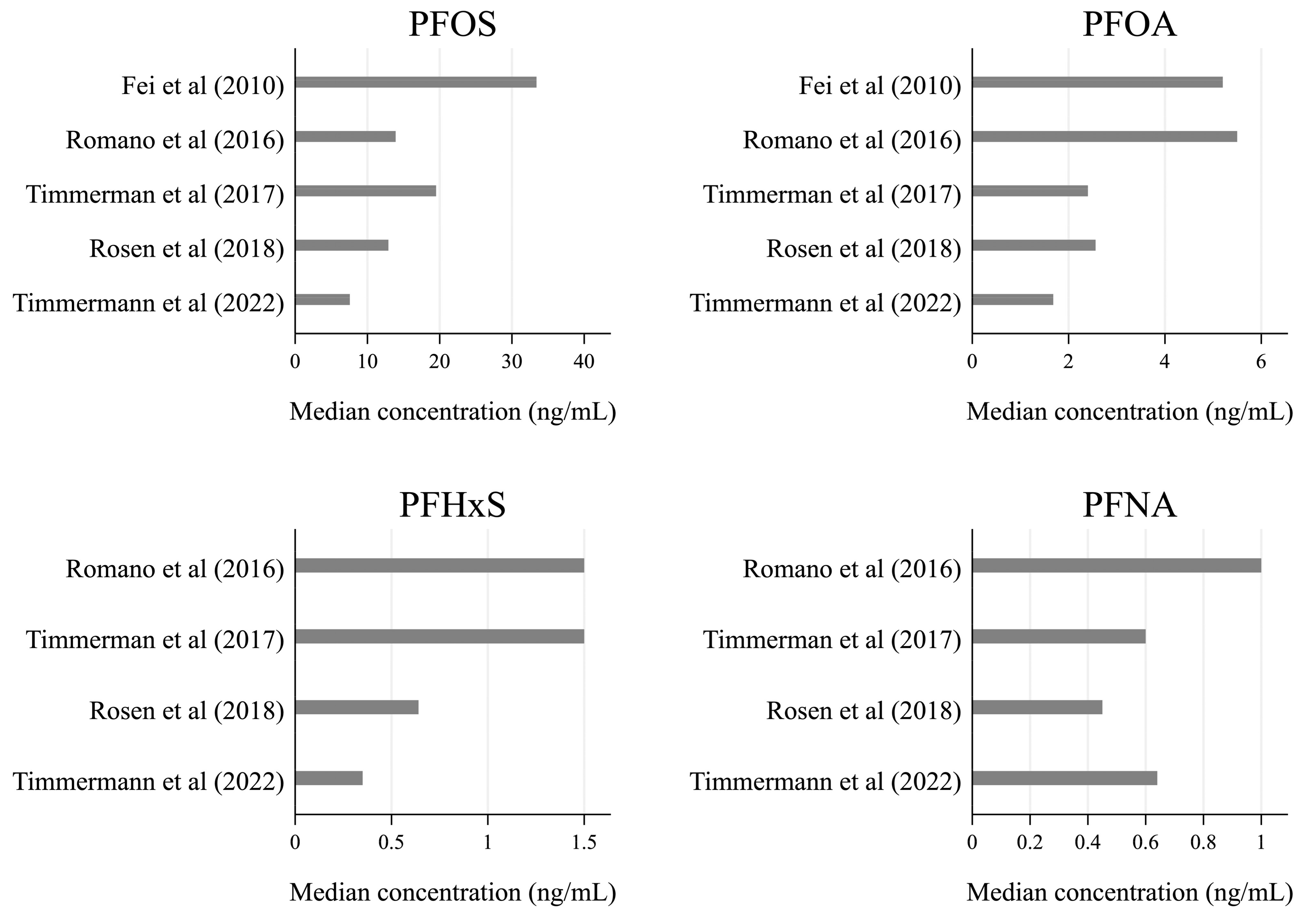
| Fei et al. (2010) [40] | Denmark | Prospective cohort study: Danish National Birth Cohort with data collection in years 1996–2002. | 1346 | PFOS: 33.4 PFOA: 5.2 | Total: 7.9 Exclusive: 3.9 |
| Romano et al. (2016) [45] | USA | Prospective cohort study: The Health Outcomes and Measures of the Environment study with data collection in years 2003–2006. | 336 | PFOS: 13.9 PFOA: 5.5 PFHxS: 1.5 PFNA: 1.0 | Total: 6 1 Exclusive: 0.07 1 |
| Timmerman et al. (2017) [44] | Faroe Islands | Prospective cohort study: Two birth cohorts with data collection in years 1997–2000 and 2007–2009. | 987 | PFOS: 19.5 PFOA: 2.4 PFHxS: 1.5 PFNA: 0.6 PFDA: 0.3 | Total: 9 Exclusive: 5 |
| Rosen et al. (2018) [42] | Norway | Prospective cohort study: Norwegian Mother and Child Cohort Study with data collection in years 1999–2008. | 1716 | PFOS: 12.9 PFOA: 2.56 PFHxS: 0.64 PFNA: 0.45 PFDA: 0.09 PFHpS: 0.14 PFUnDA: 0.19 PFDoDA: 0.04 PFTrDA: 0.04 | Total: > 6 2 Exclusive: NA |
| Nielsen et al. (2022) [41] | Sweden | Natural experiment (contamination of drinking water): Municipality of Ronneby plus reference group from nearby municipality, children born in years 1999–2009. | 2374 | NA 3 | Total: 6–7 Exclusive: NI |
| Timmermann et al. (2022) [43] | Denmark | Prospective cohort study: Odense Child Cohort with data collection in years 2010–2012. | 925 | PFOS: 7.56 PFOA: 1.68 PFHxS: 0.35 PFNA: 0.64 PFDA: 0.29 ∑PFAS: 10.86 | Total: 7.6 Exclusive: 2.5 |
| First Author (Publication Year) | Statistical Analysis Model | Effect Estimate |
|---|---|---|
| Fei et al. (2010) [40] | Cox regression + logistic regression |
|
| Romano et al. (2016) [45] | Poisson regression with robust standard errors + Cox regression |
|
| Timmerman et al. (2017) [44] | Linear regression |
|
| Rosen et al. (2018) [42] | Cox regression with censoring at 3 or 6 months + logistic regression. Excluded women who never initiated breastfeeding. |
|
| Nielsen et al. (2022) [41] | Modified Poisson regression with robust error variance + Cox regression with censoring at 6/12 months for exclusive/total breastfeeding |
|
| Timmermann et al. (2022) [43] | Cox regression. Women terminating breastfeeding for reasons not related to insufficient lactation or with no reason given were censured. |
|
| First Author (Publication Year) | Bias Due to Confounding | Bias Arising from Measurement of the Exposure | Bias in Selection of Participants | Bias Due to Post-Exposure Interventions | Bias Due to Missing Data | Bias Arising from Measurements of the Outcome | Bias in Selection of the Reported Results | Overall Risk of Bias | |
|---|---|---|---|---|---|---|---|---|---|
| Confounding from Previous Breastfeeding | Other Confounding | ||||||||
| Fei et al. (2010) [40] | Low risk. Stratification by parity. | Low risk. Adjusted for parity, maternal age at delivery, pre-pregnancy body mass index, maternal socioeconomic status, alcohol consumption, and smoking during pregnancy, and gestational age at blood drawing. | Low risk. Blood samples, GA 4–14 weeks. | Low risk. Selection was not affected by the exposure or outcome. | Low risk. Participants were unaware of their exposure. | Low risk. Few data were missing and controlled for. | Low risk of bias towards null. Interviews at 6 and 18 months after birth. | Low risk. Multiple analyses were performed, but all estimates were provided. | Low |
| Romano et al. (2016) [45] | Low risk. Adjustment for total duration of breastfeeding previous children and stratification by parity. | Low risk. Adjusted for parity, maternal age, race/ethnicity, marital status, household income, maternal serum cotinine during pregnancy, alcohol use during pregnancy, and gestational week at blood draw. | Low risk of bias towards null. Blood samples, GA 16 weeks (85%), 26 weeks (10%), or delivery (5%). | Low risk. Selection was not affected by the exposure or outcome. | Low risk. Participants were unaware of their exposure. | Low risk. The proportion of missing data was most likely similar across groups. | Low risk of bias towards null. Standardized surveys by phone every 3 months until breastfeeding was discontinued or the child’s third birthday. | Low risk. Multiple analyses were performed, but all estimates were provided. | Low |
| Timmerman et al. (2017) [44] | Low risk. Tested interaction between PFAS and parity. | Low risk. Adjusted for parity, cohort, maternal age, pre-pregnancy BMI, pregnancy alcohol intake, pregnancy smoking, education, and employment. | Low risk of bias towards null. Blood samples, GA 34–36 weeks (older cohort) or two weeks after their term date (younger cohort). | Low risk. Selection was not affected by the exposure or outcome. | Low risk. Participants were unaware of their exposure. | Low risk. Few data were missing and controlled for. | Low risk of bias towards null. Questionnaire followed by an interview at 18 months (only younger cohort) and 5 years after birth. | Low risk. Multiple analyses were performed, but all estimates were provided. | Low |
| Rosen et al. (2018) [42] | Low risk. Adjustment for previous breastfeeding duration and stratification by parity. | Low risk. Adjusted for parity, maternal age at birth, smoking during pregnancy, pre-pregnancy BMI, and prior study status. | Low risk. Blood samples GA 17–20 weeks. | Low risk. Combined data from two prior nested case-control studies. Selection was not affected by the exposure or outcome. | Low risk. Participants were unaware of their exposure. | Low risk. Missing data were imputed using the Markov chain Monte Carlo method. | Low risk of bias towards null. Self-reported questionnaire 6 months after delivery. | Low risk. Multiple analyses were performed, but all estimates were provided. | Low |
| Nielsen et al. (2022) [41] | Low risk. Use of residential address (and stratification by parity). | Low risk. Adjusted for parity, maternal age, BMI, education level, country of birth, and tobacco use during pregnancy. | Low risk of bias towards null. Residential addresses of mothers during the 5-year window before delivery. | Low risk. Participants were selected based on residential address. Selection was not related to the outcome. | Low risk. Participants were aware of their exposure risk, but all were advised to breastfeed. | Low risk. Few data were missing. | Moderate risk of bias towards null. Child health care charts. Information on breastfeeding and formula feeding was available monthly during the first year and less frequently thereafter. | Low risk. Multiple analyses were performed, but all estimates were provided. | Low |
| Timmermann et al. (2022) [43] | Low risk. Tested interaction between PFAS and parity. | Low risk. Adjusted for education, body mass index, national origin, and expectations of giving formula, parity, smoking, duration of previous breastfeeding, and previous inadequate lactation. | Low risk. Blood samples, median GA 12 weeks (5th–95th percentiles, 10–16 weeks). | Low risk. Selection was not affected by the exposure or outcome. | Low risk. Participants were unaware of their exposure. | Low risk. The proportion of missing data was most likely similar across groups. | Low risk of bias towards null. Self-reported questionnaire 3 and 18months post-partum. Weekly text messages from a subgroup of women. Additional information from health visitor contacts for early weaners. | Low risk. Multiple analyses were performed, but all estimates were provided. | Low |
| First Author (Publication Year) | Total Breastfeeding (All) | Total Breastfeeding (Primiparous) | Exclusive Breastfeeding (All) | Exclusive Breastfeeding (Primiparous) | Author Conclusion |
|---|---|---|---|---|---|
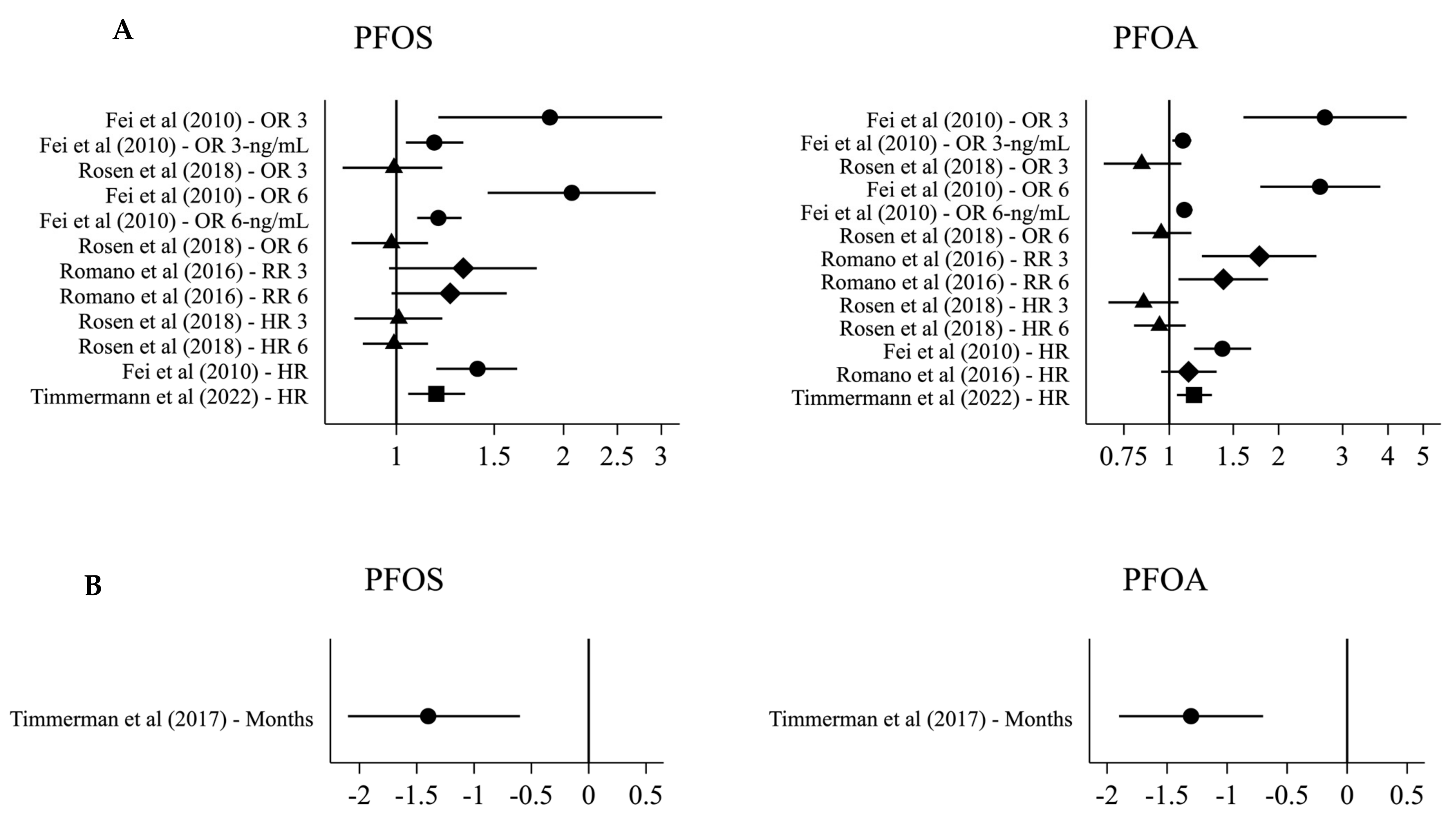
| Fei et al. (2010) [40] | PFOS: HR: 1.40 (1.18; 1.65) OR 3: 1.89 (1.19; 3.01) OR 6: 2.07 (1.46; 2.93) OR 3-ng/mL: 1.17 (1.04; 1.32) OR 6-ng/mL: 1.19 (1.09; 1.31) PFOA: HR: 1.40 (1.17; 1.68) OR 3: 2.68 (1.60; 4.50) OR 6: 2.60 (1.78; 3.81) OR 3-ng/mL: 1.09 (1.02; 1.15) OR 6-ng/mL: 1.10 (1.05; 1.16) | PFOS: HR: 1.17 (0.90; 1.52) OR 3: 1.24 (0.62–2.46) OR 6: 1.52 (0.89; 2.60) OR 3-ng/mL: 1.12 (0.94; 1.34) OR 6-ng/mL: 1.20 (1.04; 1.37) PFOA: HR: 0.98 (0.69; 1.38) OR 3: 1.82 (0.66; 5.07) OR 6: 1.50 (0.74; 3.06) OR 3-ng/mL: 1.02 (0.93; 1.10) OR 6-ng/mL: 1.03 (0.97; 1.10) | PFOS: HR: 1.37 (1.14; 1.64) OR 1: 1.55 (0.89; 2.71) OR 4: 1.86 (1.24; 2.79) OR 1-ng/mL: 1.09 (0.93; 1.27) OR 4-ng/mL: 1.14 (1.02; 1.27) PFOA: HR: 1.37 1.12–1.69 OR 1: 2.19 1.16; 4.14 OR 4: 2.59 1.66; 4.04 OR 1-ng/mL: 1.05 (0.98; 1.13) OR 4-ng/mL: 1.06 (1.00; 1.12) | PFOS: HR: 1.23 (0.93; 1.64) OR 1: 0.78 (0.35; 1.70) OR 4: 1.19 (0.66; 2.15) OR 1-ng/mL: 0.98 (0.78; 1.23) OR 4-ng/mL: 1.04 (0.89; 1.22) PFOA: HR: 1.16 0.81; 1.66 OR 1: 0.55 0.21;1.42 OR 4: 0.91 0.43;1.89 OR 1-ng/mL: (0.93 0.82; 1.06) OR 4-ng/mL: (0.98 (0.91; 1.06) | These findings suggest that PFOA and PFOS may reduce the ability to lactate, but could equally reflect reverse causation since no association was seen in primiparous women. |
| Romano et al. (2016) [45] | PFOS: | PFOS: | PFOS: | Maternal serum PFOA concentrations were inversely related to the duration of any breastfeeding. Maternal serum PFAS concentrations were not associated with exclusive breastfeeding. | |
| RR 3: 1.32 (0.97; 1.79) | RR 3: 1.21 (0.71; 2.08) 1 | RR 3: 0.98 (0.87; 1.10) | |||
| RR 6: 1.25 (0.98; 1.58) | RR 6: 1.07 (0.70; 1.61) 1 | ||||
| PFOA: | PFOA: | PFOA: | |||
| HR: 1.13 (0.95; 1.35) | RR 3: 2.17 (1.17; 4.01) 1 | RR 3: 1.12 (0.98; 1.28) | |||
| RR 3: 1.77 (1.23; 2.54) | RR 6: 1.41 (0.85; 2.32) 1 | ||||
| RR 6: 1.41 (1.06; 1.87) | |||||
| PFHxS: | PFHxS: | ||||
| RR 3: 1.39 (0.99; 1.96) | RR 3: 0.94 (0.84; 1.06) | ||||
| RR 6: 1.22 (0.96; 1.55) | |||||
| PFNA: | PFNA: | ||||
| RR 3: 1.12 (0.81; 1.53) | RR 3: 0.96 (0.85; 1.08) | ||||
| RR 6: 1.13 (0.90; 1.43) | |||||
| Timmerman et al. (2017) [44] | PFOS months: −1.4 (−2.1; −0.6) PFOA months: −1.3 (−1.9; −0.7) PFHxS months: −0.2 (−0.5; 0.2) PFNA months: −1.3 (−2.0; −0.7) PFDA months: −0.8 (−1.4; −0.3) | PFOS months: −1.3 (−2.3; −0.3) PFOA months: −1.1 (−2.0; −0.1) PFHxS months: −0.1 (−0.5; 0.3) PFNA months: −1.6 (−2.6; −0.6) PFDA months: −1.6 (−2.6; −0.7) | PFOS months: −0.3 (−0.6; −0.1) PFOA months: −0.5 (−0.7; −0.3) PFHxS months: −0.1 (−0.2; 0.1) PFNA months: −0.2 (−0.5; −0.0) PFDA months: −0.2 (−0.4; 0.0) | PFOS months: −0.2 (−0.6; 0.1) PFOA months: −0.4 (−0.8; 0.0) PFHxS months: −0.0 (−0.1; 0.1) PFNA months: −0.3 (−0.8; 0.1) PFDA months: −0.5 (−0.9; −0.1) | Increased maternal serum PFAS concentrations are associated with a decreased duration of breastfeeding. |
| Rosen et al. (2018) [42] | PFOS: | PFOS: | Unexpected observation of inverse associations of PFNA, PFDA, and PFUnDA with breastfeeding cessation. A positive association of PFOS with breastfeeding was observed when accounting for other exposures. No association between PFOA and breastfeeding was observed. | ||
| HR 3: 1.01 (0.84; 1.21) | HR 3: 0.94 (0.77; 1.16) | ||||
| HR 6: 0.99 (0.87; 1.14) | HR 6: 0.94 (0.81; 1.09) | ||||
| OR 3: 0.99 (0.80; 1.21) | |||||
| OR 6: 0.98 (0.83; 1.14) | |||||
| PFOA: | PFOA: | ||||
| HR 3: 0.85 (0.68; 1.06) | HR 3: 0.84 (0.67; 1.04) | ||||
| HR 6: 0.94 (0.80; 1.11) | HR 6: 0.91 (0.78; 1.06) | ||||
| OR 3: 0.84 (0.66; 1.08) | |||||
| OR 6: 0.95 (0.79; 1.15) | |||||
| PFHxS: | PFHxS: | ||||
| HR 3: 0.88 (0.75; 1.03) | HR 3: 0.93 (0.78; 1.11) | ||||
| HR 6: 0.92 (0.82; 1.03) | HR 6: 0.96 (0.84; 1.09) | ||||
| OR 3: 0.86 (0.72; 1.03) | |||||
| OR 6: 0.91 (0.80; 1.05) | |||||
| PFNA: | PFNA: | ||||
| HR 3: 0.77 (0.63; 0.93) | HR 3: 0.72 (0.58; 0.88) | ||||
| HR 6: 0.84 (0.73; 0.97) | HR 6: 0.81 (0.69; 0.95) | ||||
| OR 3: 0.73 (0.59; 0.91) | |||||
| OR 6: 0.83 (0.70; 0.98) | |||||
| PFDA: | PFDA: | ||||
| HR 3: 0.73 (0.62; 0.86) | HR 3: 0.69 (0.58; 0.82) | ||||
| HR 6: 0.82 (0.72; 0.92) | HR 6: 0.78 (0.68; 0.89) | ||||
| OR 3: 0.70 (0.58; 0.84) | |||||
| OR 6: 0.80 (0.69; 0.93) | |||||
| PFHpS: | PFHpS: | ||||
| HR 3: 0.96 (0.81; 1.14) | HR 3: 0.95 (0.77; 1.16) | ||||
| HR 6: 0.96 (0.85; 1.08) | HR 6: 0.96 (0.83; 1.11) | ||||
| OR 3: 0.96 (0.79; 1.15) | |||||
| OR 6: 0.96 (0.83; 1.11) | |||||
| PFUnDA: | PFUnDA: | ||||
| HR 3: 0.73 (0.62; 0.86) | HR 3: 0.68 (0.57; 0.81) | ||||
| HR 6: 0.81 (0.72; 0.93) | HR 6: 0.78 (0.68; 0.90) | ||||
| OR 3: 0.70 (0.58; 0.84) | |||||
| OR 6: 0.79 (0.68; 0.91) | |||||
| PFDoDA: | PFDoDA: | ||||
| HR 3: 0.97 (0.68; 1.41) | HR 3: 0.97 (0.64; 1.46) | ||||
| HR 6: 0.90 (0.69; 1.17) | HR 6: 0.88 (0.65; 1.19) | ||||
| OR 3: 0.97 (0.65; 1.45) | |||||
| OR 6: 0.88 (0.65; 1.19) | |||||
| PFTrDA: | PFTrDA: | ||||
| HR 3: 0.99 (0.69; 1.40) | HR 3: 0.87 (0.58; 1.30) | ||||
| HR 6: 0.98 (0.76; 1.26) | HR 6: 0.98 (0.74; 1.29) | ||||
| OR 3: 0.97 (0.66; 1.43) | |||||
| OR 6: 0.97 (0.72; 1.29) | |||||
| Nielsen et al. (2022) [41] | ∑PFAS: RR initiation: 2.37 (0.84; 6.69) RR 6: 1.17 (0.07–1.40) HR 0: 1.58 (1.12; 2.22) HR 3: 1.32 (1.06; 1.63) HR 6: 1.09 (0.93; 1.29) HR 10: 0.86 (0.65; 1.14) | ∑PFAS: RR initiation: 2.92 (0.34; 23.01) RR 6: 1.56 (1.16; 2.11) HR 0: 2.49 (1.50; 4.14) HR 3: 1.82 (1.32; 2.51) HR 6: 1.33 (1.05; 1.69) HR 10: 0.88 (0.59; 1.30) | ∑PFAS: RR 3: 1.12 (0.92; 1.37) HR: 1.14 (0.92; 1.40) | ∑PFAS: RR 3: 1.21 (0.92; 1.61) HR: 1.30 (0.96; 1.76) | Exposure to high levels of PFAS seemed to be associated with increased risks of not initiating breastfeeding and shorter breastfeeding duration in primiparous women. The findings imply that the ability of first-time mothers to establish breastfeeding is a sensitive outcome after high exposure to PFAS. |
| Timmermann et al. (2022) [43] | PFOS HR: 1.18 (1.05; 1.33) PFOA HR: 1.17 (1.05; 1.31) PFHxS HR: 1.05 (0.96; 1.14) PFNA HR: 1.17 (1.04; 1.31) PFDA HR: 1.02 (0.93; 1.12) ∑PFAS HR: 1.23 (1.08; 1.40) | PFOS HR: 1.15 (1.00; 1.33) PFOA HR: 1.19 (1.04; 1.37) PFHxS HR: 1.04 (0.93; 1.16) PFNA HR: 1.18 (1.02; 1.36) PFDA HR: 1.03 (0.91; 1.16) ∑PFAS HR: 1.21 (1.03; 1.43) | PFOS HR: 0.94 (0.85; 1.04) PFOA HR: 1.02 (0.93; 1.12) PFHxS HR: 0.92 (0.86; 0.98) PFNA HR: 0.91 (0.82; 1.01) PFDA HR: 0.97 (0.89; 1.06) ∑PFAS HR: 0.94 (0.84; 1.05) | PFOS HR: 0.95 (0.84; 1.08) PFOA HR: 0.98 (0.87; 1.12) PFHxS HR: 0.94 (0.85; 1.03) PFNA HR: 0.89 (0.78; 1.02) PFDA HR: 0.97 (0.86; 1.09) ∑PFAS HR: 0.94 (0.81; 1.09) | Higher serum PFAS concentrations were associated with a shorter duration of breastfeeding. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timmermann, A.; Avenbuan, O.N.; Romano, M.E.; Braun, J.M.; Tolstrup, J.S.; Vandenberg, L.N.; Fenton, S.E. Per- and Polyfluoroalkyl Substances and Breastfeeding as a Vulnerable Function: A Systematic Review of Epidemiological Studies. Toxics 2023, 11, 325. https://doi.org/10.3390/toxics11040325
Timmermann A, Avenbuan ON, Romano ME, Braun JM, Tolstrup JS, Vandenberg LN, Fenton SE. Per- and Polyfluoroalkyl Substances and Breastfeeding as a Vulnerable Function: A Systematic Review of Epidemiological Studies. Toxics. 2023; 11(4):325. https://doi.org/10.3390/toxics11040325
Chicago/Turabian StyleTimmermann, Amalie, Oyemwenosa N. Avenbuan, Megan E. Romano, Joseph M. Braun, Janne S. Tolstrup, Laura N. Vandenberg, and Suzanne E. Fenton. 2023. "Per- and Polyfluoroalkyl Substances and Breastfeeding as a Vulnerable Function: A Systematic Review of Epidemiological Studies" Toxics 11, no. 4: 325. https://doi.org/10.3390/toxics11040325
APA StyleTimmermann, A., Avenbuan, O. N., Romano, M. E., Braun, J. M., Tolstrup, J. S., Vandenberg, L. N., & Fenton, S. E. (2023). Per- and Polyfluoroalkyl Substances and Breastfeeding as a Vulnerable Function: A Systematic Review of Epidemiological Studies. Toxics, 11(4), 325. https://doi.org/10.3390/toxics11040325