
Plant-Based Diet for Glycemic Control, Insulin Sensitivity, and Lipid Profile in Type 2 Diabetes: A Systematic Review

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
- Aims
- Research questions
2. Materials and Methods
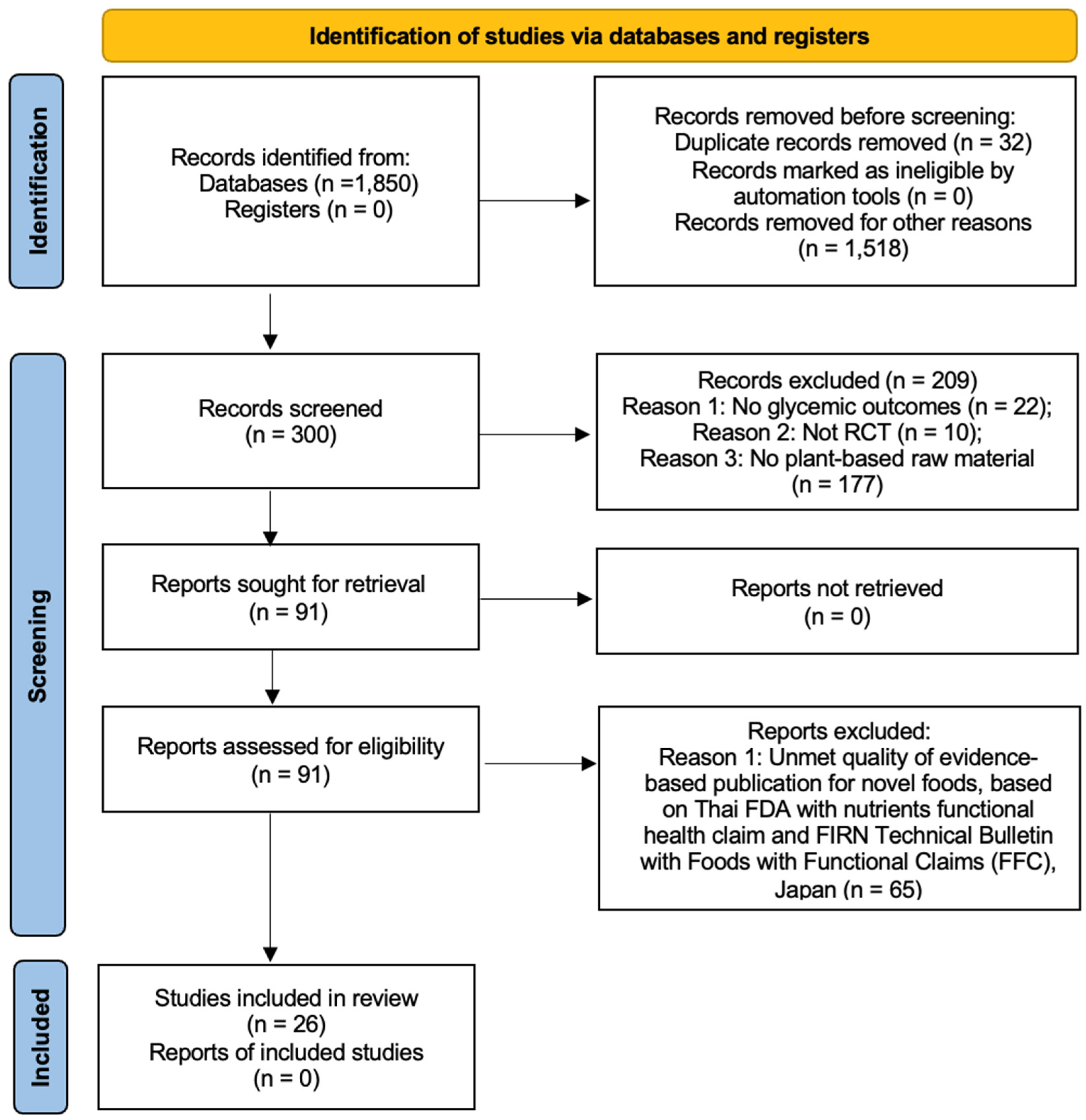
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
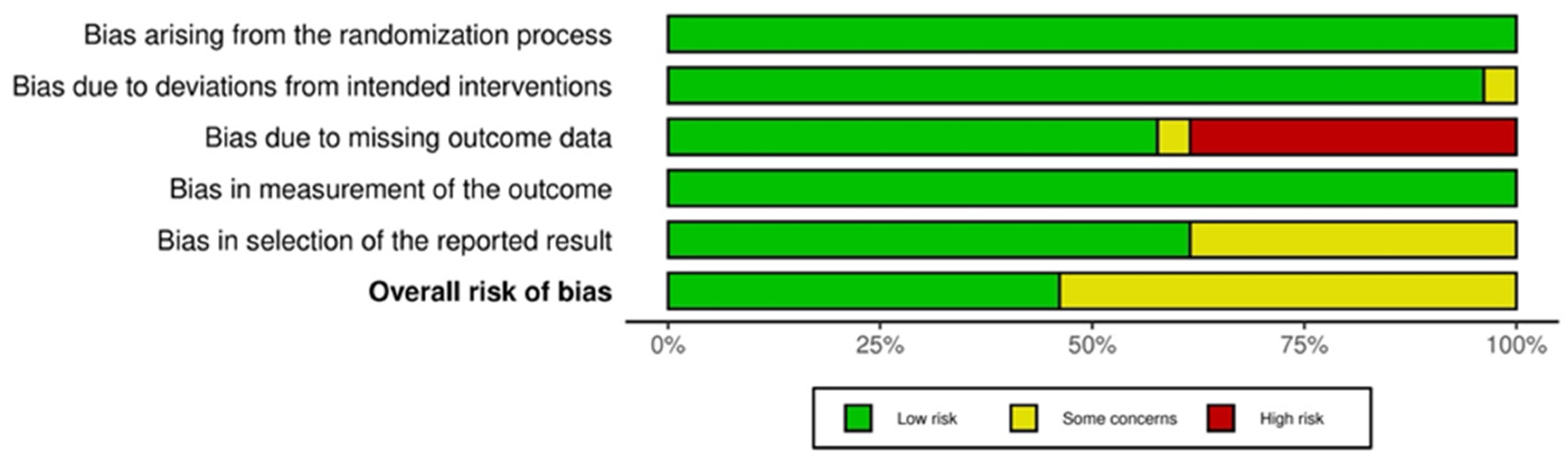
2.4.1. Risk of Bias Assessment
2.4.2. Functional Food Claim Japan Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Impact of the Plant or Plant Extract Intervention on Blood Sugar and HbA1c
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Releases 2023 Standards of Care in Diabetes to Guide Prevention, Diagnosis, and Treatment for People Living with Diabetes. Available online: https://diabetes.org/newsroom/american-diabetes-association-2023-standards-care-diabetes-guide-for-prevention-diagnosis-treatment-people-living-with-diabetes (accessed on 1 December 2024).
- National Institute of Diabetes and Digestive and Kidney Diseases. Diabetes. Available online: https://www.niddk.nih.gov/health-information/diabetes (accessed on 2 October 2024).
- Centers for Disease Control and Prevention. Preventing Type 2 Diabetes. Available online: https://www.cdc.gov/diabetes/prevention-type-2/index.html (accessed on 1 December 2024).
- Mohamed, A.; Staite, E.; Ismail, K.; Winkley, K. A systematic review of diabetes self-management education interventions for people with type 2 diabetes mellitus in the Asian western pacific (AWP) region. Nurs. Open 2019, 6, 1424–1437. [Google Scholar] [CrossRef] [PubMed]
- Shahaj, O.; Denneny, D.; Schwappach, A.; Pearce, G.; Epiphaniou, E.; Parke, H.L.; Taylor, S.J.C.; Pinnock, H. Supporting self-management for people with hypertension: A meta-review of quantitative and qualitative systematic reviews. J. Hypertens. 2019, 37, 264–279. [Google Scholar] [CrossRef] [PubMed]
- Mahlare, S.S.; Rasweswe, M.M.; Ramavhoy, T.I. Self-management challenges of adults with type 2 diabetes mellitus in Ekurhuleni district primary health care facilities amid COVID-19 lockdown. Afr. J. Prim. Health Care Fam. Med. 2024, 16, e1–e7. [Google Scholar] [CrossRef]
- Misra, R.; Adelman, M.M.; Kirk, B.; Sambamoorthi, U. Relationship Among Diabetes Distress, Health Literacy, Diabetes Education, Patient-Provider Communication and Diabetes Self-Care. Am. J. Health Behav. 2022, 46, 528–540. [Google Scholar] [CrossRef] [PubMed]
- Cangelosi, G.; Mancin, S.; Pantanetti, P.; Nguyen, C.T.T.; Morales Palomares, S.; Biondini, F.; Sguanci, M.; Petrelli, F. Lifestyle Medicine Case Manager Nurses for Type Two Diabetes Patients: An Overview of a Job Description Framework—A Narrative Review. Diabetology 2024, 5, 375–388. [Google Scholar] [CrossRef]
- Shin, S.A.; Kim, H.; Lee, K.; Lin, V.; Liu, G.; Shin, E. Effects of diabetic case management on knowledge, self-management abilities, health behaviors, and health service utilization for diabetes in Korea. Yonsei Med. J. 2015, 56, 244–252. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- FIRN. Technical Bulletin. Available online: https://firn.or.th/technical-bulletins-main (accessed on 1 May 2024).
- Guidelines for Use of Nutrition and Health Claims (CAC/GL 23-1997) Revised in 2004. Available online: https://www.fao.org/ag/humannutrition/32444-09f5545b8abe9a0c3baf01a4502ac36e4.pdf (accessed on 1 May 2024).
- Shimizu, T. Health claims on functional foods: The Japanese regulations and an international comparison. Nutr. Res. Rev. 2003, 16, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Consumer Affairs Agency, Government of Japan. Foods with Function Claims. Available online: https://www.caa.go.jp/policies/policy/food_labeling/information/ffc/ (accessed on 1 December 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Khajebishak, Y.; Payahoo, L.; Alivand, M.; Hamishehkar, H.; Mobasseri, M.; Ebrahimzadeh, V.; Alipour, M.; Alipour, B. Effect of pomegranate seed oil supplementation on the GLUT-4 gene expression and glycemic control in obese people with type 2 diabetes: A randomized controlled clinical trial. J. Cell. Physiol. 2019, 234, 19621–19628. [Google Scholar] [CrossRef]
- Mobasseri, M.; Ostadrahimi, A.; Tajaddini, A.; Asghari, S.; Barati, M.; Akbarzadeh, M.; Nikpayam, O.; Houshyar, J.; Roshanravan, N.; Alamdari, N.M. Effects of saffron supplementation on glycemia and inflammation in patients with type 2 diabetes mellitus: A randomized double-blind, placebo-controlled clinical trial study. Diabetes Metab Syndr. 2020, 14, 527–534. [Google Scholar] [CrossRef]
- Raeisi-Dehkordi, H.; Amiri, M.; Zimorovat, A.; Moghtaderi, F.; Zarei, S.; Forbes, S.C.; Salehi-Abargouei, A. curcumin compared with sesame and sesame-canola oil on glycaemic control and liver function in patients with type 2 diabetes: A three-way randomized triple-blind crossover trial. Diabetes Metab. Res. Rev. 2020, 37, e3399. [Google Scholar] [CrossRef] [PubMed]
- Asadi, S.; Gholami, M.S.; Siassi, F.; Qorbani, M.; Khamoshian, K.; Sotoudeh, G. Nano curcumin supplementation reduced the severity of diabetic sensorimotor polyneuropathy in patients with type 2 diabetes mellitus: A randomized double-blind placebo- controlled clinical trial. Complement. Ther. Med. 2019, 43, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Na, G.; Zhang, J.; Lv, D.; Chen, P.; Song, X.; Cai, F.; Zheng, S.; Wan, W.; Shan, Y. Germinated brown rice enhanced n-3 PUFA metabolism in type 2 diabetes patients: A randomized controlled trial. Clin. Nutr. 2023, 42, 579–589. [Google Scholar] [CrossRef]
- Aghasi, M.; Koohdani, F.; Qorbani, M.; Nasli-Esfahani, E.; Ghazi-Zahedi, S.; Khoshamal, H.; Keshavarz, A.; Sotoudeh, G. Beneficial effects of green cardamom on serum SIRT1, glycemic indices and triglyceride levels in patients with type 2 diabetes mellitus: A randomized double-blind placebo controlled clinical trial. J. Sci. Food Agric. 2019, 99, 3933–3940. [Google Scholar] [CrossRef]
- Dehghan, P.; Pourghassem Gargari, B.; Asghari Jafar-abadi, M. Oligofructose-enriched inulin improves some inflammatory markers and metabolic endotoxemia in women with type 2 diabetes mellitus: A randomized controlled clinical trial. Nutrition 2014, 30, 418–423. [Google Scholar] [CrossRef]
- Hoseini, A.; Namazi, G.; Farrokhian, A.; Reiner, Ž.; Aghadavod, E.; Bahmani, F.; Asemi, Z. The effects of resveratrol on metabolic status in patients with type 2 diabetes mellitus and coronary heart disease. Food Funct. 2019, 10, 6042–6051. [Google Scholar] [CrossRef]
- Sauder, K.A.; McCrea, C.E.; Ulbrecht, J.S.; Kris-Etherton, P.M.; West, S.G. Effects of pistachios on the lipid/lipoprotein profile, glycemic control, inflammation, and endothelial function in type 2 diabetes: A randomized trial. Metabolism 2015, 64, 1521–1529. [Google Scholar] [CrossRef] [PubMed]
- Karimzadeh, L.; Sohrab, G.; Hedayati, M.; Ebrahimof, S.; Emami, G.; Razavion, T. Effects of concentrated beetroot juice consumption on glycemic control, blood pressure, and lipid profile in type 2 diabetes patients: Randomized clinical trial study. Ir. J. Med. Sci. 2023, 192, 1143–1153. [Google Scholar] [CrossRef]
- Rafraf, M.; Malekiyan, M.; Asghari-Jafarabadi, M.; Aliasgarzadeh, A. Effect of fenugreek seeds on serum metabolic factors and adiponectin levels in Type 2 diabetic patients. Int. J. Vitam. Nutr. Res. 2014, 84, 196–205. [Google Scholar] [CrossRef]
- Seyed Hashemi, M.; Namiranian, N.; Tavahen, H.; Dehghanpour, A.; Rad, M.H.; Jam-Ashkezari, S.; Emtiazy, M.; Hashempur, M.H. Efficacy of pomegranate seed powder on glucose and lipid metabolism in patients with type 2 diabetes: A prospective randomized double-blind placebo-controlled clinical trial. Complement. Med. Res. 2021, 28, 226–233. [Google Scholar] [CrossRef]
- Moradi, A.; Tarrahi, M.-J.; Ghasempour, S.; Shafiepour, M.; Clark, C.C.T.; Safavi, S.-M. The effect of okra (Abelmoschus esculentus) on lipid profiles and glycemic indices in Type 2 diabetic adults: Randomized double blinded trials. Phytother. Res. 2020, 34, 3325–3332. [Google Scholar] [CrossRef]
- Tajaddini, A.; Roshanravan, N.; Mobasseri, M.; Haleem Al-Qaim, Z.; Hadi, A.; Aeinehchi, A.; Sefid-Mooye Azar, P.; Ostadrahimi, A. The effect of saffron (Crocus sativus L.) on glycemia, lipid profile, and antioxidant status in patients with type-2 diabetes mellitus: A randomized placebo-controlled trial. Phytother. Res. 2023, 37, 388–398. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, Z.; Ghadiri-Anari, A.; Mehrjardi, A.V.; Dehghani, A.; Zardini, H.Z.; Nadjarzadeh, A. Effect of Ziziphus jujube fruit infusion on lipid profiles, glycaemic index and antioxidant status in type 2 diabetic patients: A randomized controlled clinical trial. Phytother. Res. 2017, 31, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, F.; Haines, D.; Al-Ozairi, E.; Dashti, A. Effect of black tea consumption on intracellular cytokines, regulatory T cells and metabolic biomarkers in type 2 diabetes patients. Phytother. Res. 2016, 30, 454–462. [Google Scholar] [CrossRef]
- Huseini, H.F.; Hasani-Rnjbar, S.; Nayebi, N.; Heshmat, R.; Sigaroodi, F.K.; Ahvazi, M.; Alaei, B.A.; Kianbakht, S. Capparis spinosa L. (Caper) fruit extract in treatment of type 2 diabetic patients: A randomized double-blind placebo-controlled clinical trial. Complement. Ther. Med. 2013, 21, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, A.; Shahbazian, H.; Rezazadeh, A.; Haidari, F.; Jahanshahi, A.; Mahmoud Latifi, S.M.; Shirbeigi, E. The effect of soy nut on serum total antioxidant, endothelial function and cardiovascular risk factors in patients with type 2 diabetes. Diabetes Metab. Syndr. 2019, 13, 1387–1391. [Google Scholar] [CrossRef]
- Khodabandehloo, H.; Seyyedebrahimi, S.; Esfahani, E.N.; Razi, F.; Meshkani, R. Resveratrol supplementation decreases blood glucose without changing the circulating CD14+CD16+ monocytes and inflammatory cytokines in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled study. Nutr. Res. 2018, 54, 40–51. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Javid, A.Z.; Dehghan, P. The effect of enriched chicory inulin on liver enzymes, calcium homeostasis and hematological parameters in patients with type 2 diabetes mellitus: A randomized placebo-controlled trial. Prim. Care Diabetes 2016, 10, 265–271. [Google Scholar] [CrossRef]
- Atkin, M.; Laight, D.; Cummings, M.H. The effects of garlic extract upon endothelial function, vascular inflammation, oxidative stress and insulin resistance in adults with type 2 diabetes at high cardiovascular risk. A pilot double blind randomized placebo-controlled trial. J. Diabetes Complicat. 2016, 30, 723–727. [Google Scholar] [CrossRef]
- McGeoch, S.C.; Johnstone, A.M.; Lobley, G.E.; Adamson, J.; Hickson, K.; Holtrop, G.; Fyfe, C.; Clark, L.F.; Pearson, D.W.; Abraham, P.; et al. A randomized crossover study to assess the effect of an oat-rich diet on glycaemic control, plasma lipids and postprandial glycaemia, inflammation and oxidative stress in type 2 diabetes. Diabet. Med. 2013, 30, 1314–1323. [Google Scholar] [CrossRef] [PubMed]
- Dicks, L.; Kirch, N.; Gronwald, D.; Wernken, K.; Zimmermann, B.F.; Helfrich, H.P.; Ellinger, S. Regular intake of a usual serving size of flavanol-rich cocoa powder does not affect cardiometabolic parameters in stably treated patients with type 2 diabetes and hypertension-A double-blinded, randomized, placebo-controlled trial. Nutrients 2018, 10, 1435. [Google Scholar] [CrossRef]
- Honsek, C.; Kabisch, S.; Kemper, M.; Gerbracht, C.; Arafat, A.M.; Birkenfeld, A.L.; Dambeck, U.; Osterhoff, M.A.; Weickert, M.O.; Pfeiffer, A.F.H. Fibre supplementation for the prevention of type 2 diabetes and improvement of glucose metabolism: The randomised controlled Optimal Fibre Trial (OptiFiT). Diabetologia 2018, 61, 1295–1305. [Google Scholar] [CrossRef]
- Barre, D.E.; Mizier-Barre, K.A.; Griscti, O.; Hafez, K. Flaxseed oil supplementation manipulates correlations between serum individual mol % free fatty acid levels and insulin resistance in type 2 diabetics. Insulin resistance and percent remaining pancreatic β-cell function are unaffected. Endocr. Regul. 2016, 50, 183–193. [Google Scholar] [CrossRef]
- Tessari, P.; Lante, A. A multifunctional bread rich in beta glucans and low in starch improves metabolic control in type 2 diabetes: A controlled trial. Nutrients 2017, 9, 297. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Syn. Meth. 2020, 12, 55–61. [Google Scholar] [CrossRef]
- McMacken, M.; Shah, S. A plant-based diet for the prevention and treatment of type 2 diabetes. J. Geriatr. Cardiol. 2017, 14, 342–354. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Reference No. | Participant Enrollment and Retention | Clinical Subgroup | Average Age (Standard Deviation or Range), in Years | Intervention Details | Intervention Protocol | Intervention Details for the Control Group | Treatment Protocols for the Control Group and the Therapist | Effect Size of HbA1c (d) | Secondary Outcomes (Intervention vs. Control) | Time After Initial Assessment (Weeks) | Quality (Novel Food Score) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 16 | 60/52 | 60 Obese T2D | 30–50 | Clinical/ Pomegranate seed oil supplementation (PSO) | Consumed 3 capsule/day (1 g PSO) | No intervention | No intervention | No significant changes of HbA1c | -PSO group demonstrated significant improvements in both fasting blood sugar (FBS) and the quantitative insulin sensitivity check index. -PSO treatment led to increased GLUT-4 gene expression in diabetic patients without any observed adverse effects. | 8 | B |
| 17 | 60/60 | 60 T2D | 50–60 | Clinical/ Saffron supplement-ation | Consumed 1 capsule/day (100 mg saffron powder) | No intervention | Starch capsule 100 mg/day | N/A | -Fasting Blood Glucose (FBG): After 8 weeks, saffron group exhibited a statistically significant reduction in FBG levels compared to the placebo group (130.93 ± 21.21 vs. 135.13 ± 23.03 mg/dl, p = 0.012). -Tumor Necrosis Factor-alpha (TNF-α): Saffron supplementation led to a significant decrease in serum TNF-α levels compared to placebo (114.40 ± 24.28 vs. 140.90 ± 25.49 pg/mL, p < 0.001). -Gene Expression: The mRNA levels revealed that saffron significantly downregulated the expression of both TNF-α (p = 0.035) and IL-6 (p = 0.014). | 8 | B |
| 18 | 51 males, 51 females/ 46 males, 49 females | 95 T2D | 18–60 | Clinical/Sesame (SO), canola (CO), and sesame–canola (SCO: a blend) oils | SO, CO, or SCO (40% SO and 60% CO) substituted common edible oils/9 weeks with 4 weeks wash out period | No intervention | No intervention | N/A | -All treatment oils resulted in significant improvements in fasting serum insulin (FSI) and insulin sensitivity (HOMA2-%S) (p < 0.05). -SO and SCO led to favorable changes in insulin resistance (HOMA2-IR) and quantitative insulin sensitivity check index (QUICKI) (p < 0.05). -CO and SCO treatments revealed significant decrease in beta-cell function (HOMA2-%B) (p < 0.05). -FSI and HOMA2-IR were decreased after SO compared to CO in males (p = 0.024). -Serum gamma-glutamyltransferase (GGT) was significantly lower following SO compared to CO in females (p = 0.02), also no significant difference (p = 0.058). | 9 | B |
| 19 | 80/80 | 80 T2D | 30–60 | Clinical/nano-curcumin | Nano-curcumin80 mg/day | placebo capsules | Placebo capsules | Significant reduction in HbA1c (p < 0.001) | -Nano-curcumin significantly lowered FBS levels (p = 0.004). -Nano-curcumin significantly improved neuropathic symptoms compared to placebo group by lower total neuropathy scores (p < 0.001), total reflex scores (p = 0.04), and temperature (p = 0.01). | 8 | B |
| 20 | 112/61 females, 51 males | 112 T2D | 18–70 | Clinical/Germinated brown rice (GBR) | Diet with 100 g GBR/day for 3 months (n = 56) | No Intervention (n = 56) | No Intervention (n = 56) | N/A | -GBR group reduced in mean dietary inflammation index (DII), a positive impact on mitigating inflammation. -GBR significantly lower FBG, HbA1c, total cholesterol (TC), and high-density lipoprotein (HDL). -GBR intervention led to alterations in fatty acid composition, with significant increases observed in n-3 polyunsaturated fatty acids (PUFAs) and the n-3/n-6 PUFA ratio. -GBR group elevated levels of n-3 metabolites, including RVE, MaR1, and PD1, which are associated with reduced inflammation. | 12 | B |
| 21 | 83/83 | 83 Obese T2D | 30–60 | Clinical/green cardamom | Received 3 g of green cardamom/ 10 weeks | Clinical | Received 3 g rusk powder/ 10 weeks | HbA1C Decreased (−0.4%) | -A significant decrease in serum HbA1c (−0.4%), insulin (−2.8 μIU dL−1), HOMA-IR (−1.7), and TG (−39.9 mg dL−1), and an increase in SIRT1 (2.3 ngmL−1) was observed in cardamom group. -No significant changes (p < 0.05) in serum TC, HDL-c, and low density lipoprotein (LDL-c) levels. | 10 | B |
| 22 | 70/54 | 54 (M = BMI > 25 kg/m2 but <35 kg/m2 with T2D) | 20–65 | Clinical/oligofructose-enriched inulin | Received 10 g oligofructose-enriched inulin/day (Fruta fit IQ, Sensus, Borchwef 3, 4704 RG Roosendaal, Netherlands/8 weeks | Clinical | Received 10 g maltodextrin/day as a placebo (Jiujiang Hurirong Trade Co., Ltd, JiuJiang, China) | N/A | -Oligofructose-enriched inulin supplementation led to a significant reduction in FBS levels (19.2 mg/dL; 9.50%), HbA1c (1.0%; 8.40%), interleukin-6 (IL-6) (1.3 pg/mL; 8.15%), TNF-α (3.0 pg/mL; 19.80%), and plasma lipopolysaccharide (LPS) (6.0 EU/mL; 21.95%) compared to maltodextrin (p < 0.05). -Decreases were observed in interferon-gamma (IFN-γ) (0.3 pg/mL; 16.50%) and high-sensitivity C-reactive protein (hs-CRP) (3.9 ng/mL; 31.70%), while interleukin-10 (IL-10) levels increased (0.4 pg/mL, 11.50%). | 8 | B |
| 23 | 56/56 | 56 T2D and CHD | 35–70 | Clinical/resveratrol | -Received 500 mg resveratrol /day for 4 weeks | No intervention | No intervention | N/A | -Resveratrol reduced fasting glucose (β −10.04 mg dL−1; 95% CI, −18.23, −1.86; p = 0.01), insulin (β −1.09 μIU mL−1; 95% CI, −1.93, −0.24; p = 0.01), and insulin resistance (β −0.48; 95% CI, −0.76, −0.21; p = 0.001). -Significantly increased insulin sensitivity (β 0.006; 95% CI, 0.001, 0.01; p = 0.02). Resveratrol significantly increased HDL cholesterol levels (β 3.38 mg dL−1; 95% CI, 1.72, 5.05; p < 0.001) and significantly decreased the total-/HDL cholesterol ratio (β −0.36; 95% CI, −0.59, −0.13; p = 0.002). -Resveratrol caused a significant increase in total antioxidant capacity (TAC) (β 58.88 mmol L−1; 95% CI, 17.33, 100.44; p = 0.006) and a significant reduction in malondialdehyde (MDA) levels (β −0.21 μmol L−1; 95% CI, −0.41, −0.005; p = 0.04). -Resveratrol upregulated PPAR-γ (p = 0.01) and sirtuin 1 (SIRT1) (p = 0.01) in the peripheral blood mononuclear cells (PBMCs). | 4 | B |
| 24 | 30/30 | 30 T2D post menopause women BMI of 18.5–45.0 kg/m2 | 40–74 | Clinical/pistachios | Consumed nutritionally adequate diets with (contributing 20% of total energy) pistachios for 4 weeks each, separated by a 2-week washout. (Fresno, CA, USA) | No intervention | Normal diet | Decreased HbA1c by 0.4% | -Pistachio improved fasting glucose levels. -Significant reductions in fasting glucose, insulin, and HOMA-IR with pistachio intake. | 2 | B |
| Reference No. | Participant Enrollment and Retention | Clinical Subgroup | Average Age (Standard Deviation or Range), in Years | Intervention Details | Intervention Protocol | Intervention Details for the Control Group | Treatment Protocols for the Control Group and the Therapist | Effect Size of HbA1c (d) | Secondary Outcomes (Intervention vs. Control) | Time After Initial Assessment (Weeks) | Quality (Novel Food Score) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 25 | 46/38 | 38 T2D | 54 | Clinical/concentrated beetroot juice (BJ) | Consumed BJ 24 mL/day/12 weeks | No intervention | No intervention | No significant between two groups (p = 0.05) | -Plasma nitric oxide (NO) had a higher non -significant increase (8.57 ± 23.93 vs. 2.31 ± 15.98, p = 0.128). -Significant reductions in plasma insulin (14.55 ± 7.85 vs. 10.62 ± 6.96, p = 0.014) and HOMA-B (3.96 ± 0.83 vs. 3.63 ± 0.75, p = 0.038). -Significant reduction in HDL-C (70.81 ± 11.24 vs. 65.44 ± 6.46, p = 0.058) were observed in the control group after 12 weeks. -Diastolic blood pressure (DBP) was significantly reduced in the BJ group compared with the baseline (74.73 ± 16.78 vs. 72.36 ± 16.09, p = 0.046). -No significant effect on the levels of fasting plasma glucose (FPG), HbA1c, HOMA-β, HOMA-IR, TC, LDL, HDL, triglycerides (TG), and blood pressure (BP) was observed. | NA | C |
| 26 | 90/88 | 88T2D | 40–41 | Clinical/powdered whole fenugreek seeds | Consumed powdered whole fenugreek seeds 10 g/day /8 weeks | Placebo | Consumed wheat starch 5 g/day | Significant decreased (p = 0.0001) | -Significant decrease was observed in FPG levels (p = 0.007), serum insulin concentrations (p = 0.03), TC levels (p = 0.005), and TG levels (p = 0.0001). | NA | C |
| 27 | 65/60 | 60T2D | 62–63 | Clinical/Pomegranate seed powder (PSP) | Consumed PSP 5 g twice daily/8 weeks | Placebo | Consumed High molecular weight polyethylene glycol (HWPEG) 5 g twice/day | Significant difference (p = 0.05) | -Mean differences of FBG, HbA1c, cholesterol, and TG were significantly decreased in PSP group (p < 0.05). -Post-intervention values of FBG and HbA1c were significantly lower in PSP group (p = 0.02 and 0.01, respectively). -No significant differences in TC and TG (p = 0.51 and 0.26, respectively). | NA | C |
| 28 | 60/48 | 48 T2D | 30–75 | Clinical/Okra powder | Consumedokra powder 10 g blended in 150 g yogurt along with dinner and lunch/8 weeks | Placebo | Consumed conventional yogurt alone, along with dinner and lunch | No significant difference | FBG (p = 0.02), HOMA-IR (p = 0.01), QUICKI (p = 0.004), TG (p = 0.001), TC (p = 0.004), LDL cholesterol (p = 0.02), and the ratio of LDL cholesterol to HDL cholesterol (p = 0.01) all demonstrated statistically significant reductions. | NA | C |
| 29 | 70/60 | 60T2D | 51 | Clinical/saffron supplement | Consumed saffron supplement 100 mg/day /8 weeks | Placebo | Consumed starch 100 mg/day | No significant difference | -Significant reductions in TG levels by 22.72% and LDL cholesterol by 13.17% (p = 0.05). -Decreasing of nitric oxide and malondialdehyde by 26.29 and 16.35%. | Clinical | C |
| 30 | 116/110 | 110 T2D | 49–51 | Clinical/ Ziziphus jujube Fruit (ZJF) | Consumed ZJF 300 mL/day before main meals balanced diet with 55% carbohydrate, 15% energy protein 30% energy fat | Placebo | Balanced diet (500 kcal/day deficit from estimated energy requirements) with (55% carbohydrate, 15% energy protein 30% energy fat) | Significant improvement (p = 0.03) | -Statistically significant decrease in TC, TG, and LDL-C levels. -The ratios of LDL-C to HDL-C and TC to HDL-C were significantly reduced. -Statistically significant based on the following p-values: TC (p = 0.02), TG (p = 0.05), LDL-C (p = 0.01), LDL-C/HDL-C ratio (p = 0.01), and TC/HDL-C ratio (p = 0.02). | NA | C |
| 31 | 34/30 | 30T2D | 49–57 | Clinical/Black tea | Consumed three cups (three tea bags in 600 mL)/day/3 weeks | Intervention | Consumed one cup (one teabag in 200 mL)/day | Significantly lowered HbA1c levels in higher intake group (p < 0.05) | -Higher levels of regulatory T cells (Tregs), including CD3 + CD4 + CD25 + FOXP3 and CD3 + CD4 + IL-10 + cells. | NA | C |
| 32 | 60/54 | 54T2D | 53–55 | Clinical/ caper fruit extract | Consumed 400 mg caper fruit extract (1200 mg hydro-alcoholic caper fruit extract = 5 g dry caper fruit) three times a day | Placebo | Placebo capsule three times/day | Significantly decreased HbA1c (p = 0.043) | -Significantly decreased in FBG level (p = 0.037) and serum TG level (p = 0.29) compared with control group. | NA | C |
| 33 | 22 | 22 T2D | 68–69 | Clinical/ Beta glucan | Consumed functional bread, low in starch, rich in fibers (7 g/100 g) with a beta glucan/starch ratio of (7.6:100, g/g) | Clinical/ 24 weeks | Consumed regular white bread | Significant reduction (p = 0.027). | -Experimental group has better post-prandial plasma glucose (p = 0.011) greater TG concentrations (p < 0.015) when compared to the control group. | NA | C |
| 34 | 40/32 | 32 T2D | 60–61 | Clinical/ Flaxseed oil | LA rich (~57.2 weight %) flaxseed oil (60 mg ALA/kg body weight/ day) | Clinical/ 12 weeks | Approximately 103 mg of safflower oil/kg body weight/day | NA | -Homeostatic high doses of flaxseed oil have no statisticallysignificant effect on HOMA-IR or HOMA-%β. | 3 months | C |
| 35 | 70/70 | 70 T2D | 50 | Clinical/ Soy nut diet | Consumed 60 g soy nut diet in two inter-meals of morning and afternoon | Placebo/ 8 weeks | The usual diet | NA | -Significantly decreased FBG (p = 0.03) TC (p < 0.01), LDL-c (p = 0.01), and E-Selectin (p < 0.01). -Increased capacity of serum total antioxidants (p < 0.01), brachial blood flow (p < 0.01). | NA | C |
| 36 | 26/26 | 26 T2D | 50–55 | Clinical/ Aged garlic extract (AGE) | Consumed (AGE) (kyolic) 4 capsules/day (1200 mg) for 4 weeks then a 4-week washout period then placebo for 4 weeks | placebo 4 weeks, 4 weeks wash out, then 4 weeks | Daily consumption of Placebo for 4 weeks, nothing 4 weeks, then 4 weeks with placebo | No significant effect | No clinical benefit of adding AGE, in the short term. | NA | C |
| 37 | 42/42 | 42 T2D and Hypertensive | 64–66 | Clinical/ Flavanol-rich cocoa | Consumed capsules with 2.5 g/day of a flavanol-rich cocoa (ACTICOA™ cocoa) | Placebo/ 12 weeks | Consumed cocoa-free capsules (4 capsules/ day) | No significant difference | -Does not appear to have any significant impact on blood pressure, blood sugar levels, or the way the body processes fats. | NA | C |
| 38 | 49/45 | 45T2D | 57–67 | Clinical/ Resveratrol | Consumed resveratrol (99% pure trans-resveratrol; Mega Resveratrol, Southampton, UK) 400 mg capsules twice a day/8 weeks | Placebo/ 8 weeks | Placebo capsule (Completely inert micro cellulose) | Significantly reduced (p < 0.001) | Reduced FPG (p < 0.001), 2 h plasma glucose (p < 0.001). | NA | C |
| 39 | 27/27 | 27 T2D | 61–62 | Clinical/Oat-enriched diet | -Managed diet and lifestyle only for two consecutive 8-week periods following with the oat-enriched diet containing 30% oats (selected commercially available oat-based products including cereals, oatcakes, bread, cereal bars) with lower saturated fat and refined sugar contents at each meal with an oat-based product, to include 60–100 g of oats per day | Managed diet and lifestyle only for two consecutive 8-week periods following withre-enforced standard dietary advice | Consumed 400 mg completely inert micro cellulose capsules, twice a day | NA | -An oat-enriched diet did not affect blood sugar control or insulin levels after a meal. -Diet did lead to a small decrease in TC levels (p = 0.019). -Levels of adiponectin, a hormone involved in regulating blood sugar and fat metabolism, decreased after a meal (p = 0.009). | NA | C |
| 40 | 180/180 | 180 Impaired glucose tolerance | 60–70 | Clinical/Cereal fiber supplement from oat hulls | The 12-month PREDIAS intervention included 12 two-hour sessions: eight core lessons over eight weeks, and four booster sessions over the following ten months. Participants received an insoluble cereal fiber supplement from oat hulls; Vitacel OF 560-30 ; Rettenmaier &Söhne (70% cellulose, 25% hemicellulose, 3–5% lignin) | Placebo/ 2 years | A 12-month lifestyle intervention (PREDIAS) included eight core 2-h lessons over 8 weeks, followed by four booster sessions over the next 10 months, and then a 2-year placebo period | NA | Both groups saw lower 2-h oral glucose tolerance test (OGTT) levels after one year, but the difference between the groups was not significant. | NA | C |
| 41 | 54/49 | 49 Obese T2D | 49–62 | Chicory oral | Chicory inulin enriched with oligofructose 10 g/day (Frutafit IQ, Sensus, Borchwef 3, 4704 RG Roosendaal, The Netherlands) for 8 weeks | Placebo | Maltodextrin 10 g/day (Jiujiang Hurirong Trade Co., Ltd., JiuJiang city, Jiangxi, China) | Intervention 7.74 ± 0.75 Control 8.43 ± 1.06, p = 0.001 | SBP 004 vs. 0.048 | NA | C |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thaiudom, S.; Posridee, K.; Liangchawengwong, S.; Chiaranai, C.; Chularee, S.; Samanros, A.; Oonsivilai, A.; Singha-Dong, N.; Oonsivilai, R. Plant-Based Diet for Glycemic Control, Insulin Sensitivity, and Lipid Profile in Type 2 Diabetes: A Systematic Review. Foods 2025, 14, 1919. https://doi.org/10.3390/foods14111919
Thaiudom S, Posridee K, Liangchawengwong S, Chiaranai C, Chularee S, Samanros A, Oonsivilai A, Singha-Dong N, Oonsivilai R. Plant-Based Diet for Glycemic Control, Insulin Sensitivity, and Lipid Profile in Type 2 Diabetes: A Systematic Review. Foods. 2025; 14(11):1919. https://doi.org/10.3390/foods14111919
Chicago/Turabian StyleThaiudom, Siwatt, Kakanang Posridee, Sunthara Liangchawengwong, Chantira Chiaranai, Saranya Chularee, Aoitip Samanros, Anant Oonsivilai, Naruemol Singha-Dong, and Ratchadaporn Oonsivilai. 2025. "Plant-Based Diet for Glycemic Control, Insulin Sensitivity, and Lipid Profile in Type 2 Diabetes: A Systematic Review" Foods 14, no. 11: 1919. https://doi.org/10.3390/foods14111919
APA StyleThaiudom, S., Posridee, K., Liangchawengwong, S., Chiaranai, C., Chularee, S., Samanros, A., Oonsivilai, A., Singha-Dong, N., & Oonsivilai, R. (2025). Plant-Based Diet for Glycemic Control, Insulin Sensitivity, and Lipid Profile in Type 2 Diabetes: A Systematic Review. Foods, 14(11), 1919. https://doi.org/10.3390/foods14111919