Abstract
With the widespread application of digital healthcare, mobile health (mHealth) services are also developing in maternal and child health, primarily through community-based services, such as Posyandu in Indonesia. Patients need media for consultation and decision-making, while health workers are constrained in responding quickly. This study aimed to obtain information from pregnant women and midwives in developing a decision tree model as material for building a semi-automated chatbot. Using an exploratory qualitative approach, semi-structured interviews were conducted through focus group discussions (FGD) with pregnant women (n = 10) and midwives (n = 12) in March 2022. The results showed 38 codes, 15 categories, and 7 subthemes that generated 3 major themes: maternal health education, information on maternal health services, and health monitoring. The decision tree method was applied from these themes based on the needs of users, evidence, and expert sources to ensure quality. In summary, the need to use a semi-automated chatbot can be applied to education about maternal health and monitoring, where severe cases should be provided with non-automated communication with midwives. Applying the decision tree method ensured quality content, supported a clinical decision, and assisted in early detection. Furthermore, future research needs to measure user evaluation.
1. Introduction
The internet and smartphones are increasingly popular both as means of accessing healthcare information and as tools for healthcare management [1,2]. Mobile health (mHealth) is defined as the use of mobile phones to support the achievement of health objectives or to deliver versatile and functional healthcare services [3,4]. In Indonesia, mobile health utilization has increased as internet users have grown from 66.2 million to 74.55 million between 2016 and 2020 [5]. With the widespread application (app) of digital healthcare, mHealth services also thrive in maternal and child health [6]. For example, a recent systematic literature review indicates that pregnant women need information access using mHealth to increase their knowledge and their adherence to the regularity of antenatal care [7]. Moreover, previous research also showed the high need for accurate information to support health decision-making among pregnant women [6,8].
Given that the priority agenda of the Indonesian government is reducing the high Maternal Mortality Rate (MMR) of 305/100,000 live births [9], strengthening primary health services through information, communication, and technology (ICT) innovative strategy is one of the efforts to solve this problem [10]. One such effort involves community-based activities, e.g., an integrated health service center/pos pelayanan terpadu (Posyandu), a socio-cultural embodiment of the primary health care approach [9,11]. In this case, one of the Posyandu-based digital health interventions has been realized through ‘iPosyandu’, an android-based mobile app by Rinawan et al., which is currently being extended in its features [12,13,14]. The previous version was mainly used for community health workers (CHWs) to store and manage Posyandu data. It also has a feature to share information about child development and maternal health. This app aims to build a “bridge” between the community and the national level [12]. The extended version is intended to optimize family services focusing on pregnant women.
The need for communication is still increasing among patients, especially in having remote consultations with health workers to make decisions [15]. To optimize the service, health workers need help responding promptly to patients [16]. In this case, Rinawan et al. added chatbots for educational purposes on the extended iPosyandu app, focusing on pregnant women in Indonesia. A chatbot, known as an intelligent bot, interactive agent, digital assistant, or artificial conversational entity, is a form of Artificial Intelligence (AI) used for simulating human conversations [17]. Chatbots can be a tool for providing health consultation and education [18]. Recently, chatbots have been widely used in healthcare for such purposes as improving mental health [19], promoting physical activities [20], supporting patients with chronic diseases [21], and education [22]. The reason is that chatbots can help patients manage their health and assist healthcare professionals in handling patient care, particularly decision-making [16,23]. Managing knowledge-based content containing a list of questions and answers in designing a chatbot is essential to support decision-making [24]. In this matter, content quality is considered in the development process to encourage pregnant women to adopt and use medical chatbots [25]. The chatbot’s knowledge system should be based on users’ needs and literature/evidence, and should then be compiled by health and informatics experts [26,27]. A recent systematic review pointed out that ensuring the content quality of a health chatbot can be realized using a decision tree method [28].
A decision tree is mainly used for classification and prediction using tree-shaped figures [29,30]. The practice of decision trees has been widely used in the health sector [31], such as for early detection of health conditions [32], predicting disease severity [30], determining telehealth services [33], and assisting admissions to intensive care units [34]. Overall, it is intended to help healthcare professionals make clinical decisions by maximizing effectiveness and minimizing harm [35]. It is also one of the most effective methods for developing chatbots in healthcare [24,30]. For example, in an AI system of a health chatbot, the decision tree method will be used in the back-end system for servicing a question from pregnant women through the chatbot [36,37]. From the front-end side, it can help users predict their health conditions using chatbots [38]. Thus, the accuracy of the information in this decision tree method can strengthen the quality of content in health chatbots [39]. A recent systematic review shows that the decision tree is one of the tools for consideration in assisting the patient/provider in decision-making. External validation is also needed to ensure that decisions are made with high-quality evidence [28]. In our app, the chatbot for pregnant women using a decision tree method was built by involving information on user needs and health experts as one of the strategies to support the decision-making.
Even though the decision tree chatbot is a form of AI designed to simulate human conversations in health education, it still has limitations [16,37,40]. Education using a chatbot is acceptable to the patient [41,42], but many healthcare professionals and experts have emphasized that fully-automated chatbots are not mature enough to diagnose a patient’s condition or replace the judgment of a healthcare professional [16,19,40,41,42]. These findings highlight the perception that chatbot technology can be helpful for promptly responding in less complex roles. On one side, it frequently affects self-diagnosed patients [16,23]. On the other side, it must be carefully considered when providing a fully automatic chatbot focusing on health education instead of self-diagnosis. For this case, a semi-automated chatbot approach with both automation and human conversation can be a strategy to overcome this problem [37,43]. The importance of combining automated chatbots and non-automatic chats directed to health workers is to provide rapid health education about patient problems that can be validated by health workers [16,40,41]. A recent systematic review identifies limited studies examining semi-automated chatbots, mainly for handling pregnant women’s health [44]. Therefore, this research aims to explore the need of pregnant women and midwives to develop a semi-automated chatbot through a user-centered approach, applying a decision tree method that increases the accuracy of clinical decisions among pregnant women and assists in early detection of their health problems [25].
2. Materials and Methods
2.1. Study Design
An exploratory qualitative approach was used to explore the needs of pregnant women and midwives in developing a semi-automated chatbot on the extended iPosyandu application. A focus group discussion (FGD) through semi-structured face-to-face interviews was conducted, with the topic guide designed based on a review of the existing literature that included chatbot competencies for online healthcare [18]. The qualitative data were used to apply the decision tree method in developing semi-automated chatbot mockups. The stages in this research process can be depicted in Figure 1.
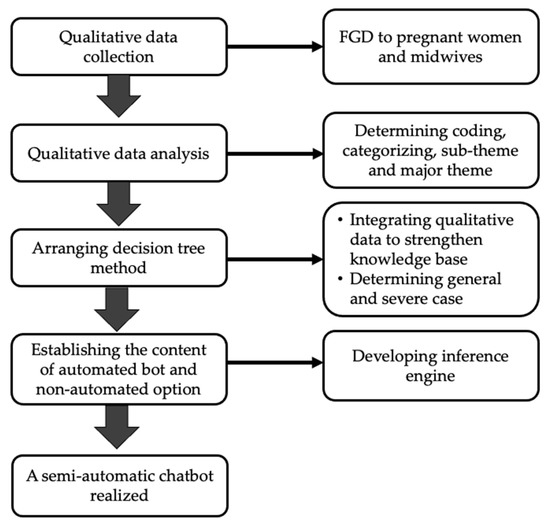
Figure 1.
Stages of the research process.
2.2. Participant Selection
Sampling was determined using a purposive sampling method, where the selection of participants was based on the researchers’ judgment about which potential participants would be most informative, such as midwives and pregnant women [45]. Collecting qualitative data was achieved through face-to-face FDGs conducted with 22 informants: pregnant women (n = 12) and midwives (n = 10). The number of participants per focus group ranged from 3 to 21, with a median of 10 [46].
The eligibility criteria of pregnant women respondents consisted of women in all trimesters who can operate smartphones and be willing to participate in the interview. Required midwife informants were working in the areas of the three public healthcare centers/Pusat kesehatan masyarakat (Puskesmas) and had attended iPosyandu training. Pregnant women with complications and mental disorders were excluded from this study. Excluded midwives were midwives known to have not carried out their duties for more than the last month. This means these midwives were not actively working and did not follow the dissemination and training about the iPosyandu app. No participants refused this interview. For each participant, the first interview began with questions about their socio-demographic data. Pregnant women’s characteristics are listed in Table 1, describing age; trimester; parity, which was divided into the categories of primiparous (women who had given birth once) versus multiparous (more than once) [47]; and educational level. Midwives’ characteristics are listed in Table 2, including age, educational level, and participation in iPosyandu app usage training.

Table 1.
Characteristics of Pregnant Women Respondents.
Table 2.
Characteristics of Midwife Respondents.
2.3. Setting
Data were collected in March 2022 and taken at 3 selected Puskesmas out of 20 Puskesmas in Purwakarta Regency, West Java Province, Indonesia. The selection of the Puskesmas followed the inclusion criteria in which health workers and CHWs had received dissemination and training on the app use. They also actively used it in the study areas (the Purwakarta, Koncara, and Pasawahan Puskesmas).
2.4. Interview Guide
The interview guide was compiled based on the content of conversational agents in previous research [18], including (1) treatment and monitoring, which is the implementation of treatment, management, support, and monitoring in health service; (2) health care service support, which includes connecting patients to health care services; (3) education, is providing information related to health care; (4) lifestyle behavior change, which supports users in overcoming various modifiable health risk factors, and (5) diagnosis, which identifies the nature of the disease or condition. First, we asked about the familiarity of informants with using chatbots on various platforms. Then, we proceeded by asking about the needs of pregnant women and midwife users regarding five chatbot functions, including chatbot for treatment and monitoring, health care service support, education, lifestyle behavior change, and diagnosis. The interview guide can be seen in Appendix A. Interviews lasted for 30–60 min and were audio recorded, and field notes were used to observe the data in the field. After the data reached data saturation, they were transcribed, and the researchers performed a member check with the informants. The theme references chatbot content or answers prepared as chatbot-based AI conversation materials. The structure of the interview can be seen in Figure 2.
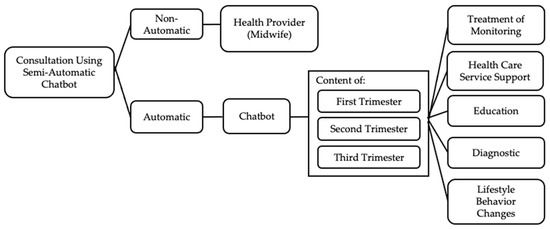
Figure 2.
Consultation structure via semi-automated chatbot.
2.5. Data Analysis and Decision Tree Method
Interviews were transcribed verbatim with the thematic analysis used to understand experiences, thoughts, or behaviors across a dataset [48]. The NVivo Release 1.6.1 (1137) software QSR International, Burlington, Massachusetts, United States of America tool was used to organize, obtain an overview of the data, and compile the coding. The analysis began with reading field notes and transcripts to receive a general sense of each transcript. Next, researchers read the transcription results repeatedly to understand the content clearly, and identified significant statements from the transcript to find codes. The codes were then grouped to represent categories as the basis for generating a small number of themes. The authors checked for the correctness of these processes and consistency. Subsequently, those categories were used to develop sub-themes and grouped into themes representing the main findings [49]. Then, the authors combined all the sub-themes and constructed meanings to describe the merged themes. Finally, the authors worked together iteratively to ensure that the narrative was representative of the data, which helped establish a credible interpretation.
The codes, categories, sub-themes and themes were then compiled into a conceptual map that shows the flow of ideas in the “findings” section. The flow can represent the theme from a more general picture to a more specific picture [49]. Concept maps were created alongside qualitative data analysis to capture all thoughts visually. In this study, the authors created a concept map using five different-colored markings to facilitate the process of generating the main findings. First, the authors determined codes marked in blue boxes representing the material for the question-and-answer items needed in developing semi-automated chatbots. Secondly, collected codes were grouped into categories marked with pink oval shapes representing the topics that would be the basis for the principal finding. In the third step, the writer connected the categories into sub-themes marked by orange boxes, then analyzed and merged them into the main findings or major themes. These themes became material for the development of the main topic. The illustration of the conceptual maps can be seen in Figure 3.
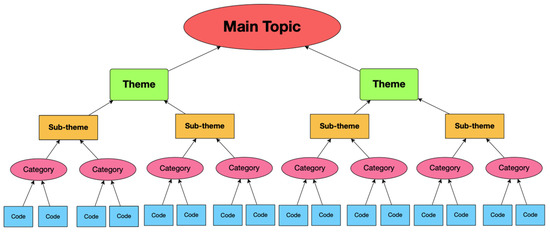
Figure 3.
An illustration of the conceptual map.
Afterward, a decision tree was built by synthesis of the qualitative data, collecting evidence and literature to strengthen the knowledge base system for creating a chatbot. The decision tree we made was in the form of questions with yes or no answers. It aimed to screen general conditions, where further complaints would be directed to the final decision to chat directly with a midwife. The function of the decision tree was also the most straightforward and feasible modeling for interventions in brief and mild conditions but less appropriate for addressing severe and long-term conditions [50]. The decision tree was generally constructed with two types of nodes: decision and terminal. A simple illustrative decision tree is presented in Figure 4.
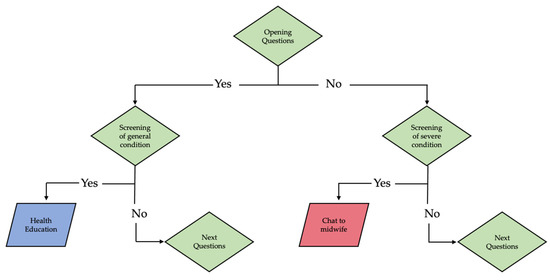
Figure 4.
An illustration of the hierarchical rules of a decision tree.
In Figure 4, the tree is a hierarchical rule directed from top to bottom, starting with a decision node (green diamond shape) as the root or initial decision. Then, each management strategy is followed by yes or no choices, representing certain events. Finally, the endpoints of decision trees are characterized by a leaf as a terminal node (parallelogram shape) consisting of blue for the education needed on general conditions and red as the option of talking to a midwife, representing severe conditions at the end of the tree. The outcome measures are generally attached to these endpoints [50]. Subsequently, the authors discussed this arrangement in realizing the creation of a chatbot.
Two main elements of AI: a knowledge base and an inference engine, shown in Figure 5, were performed to develop the chatbot. The knowledge base contained facts, theories, thoughts, and relationships [24]. The knowledge base was responsible for summarizing the system’s intelligence, consisting of keywords/phrases and responses that must be associated with each sentence. Furthermore, the chatbot design would be implemented using a chat script approach. This approach defined topics, objects (concepts), and rules. In addition, there was an inference engine that could draw conclusions based on knowledge.

Figure 5.
Main parts of AI.
3. Results
The results obtained comprised 38 codes, 15 categories, 7 sub-themes, and 3 major themes, (1) Maternal Health Education, (2) Information on Maternal Health Services and (3) Maternal Health Monitoring. The codes in the qualitative results were then compiled into a conceptual map showing the flow of ideas in the findings section [49], shown in Figure 6.
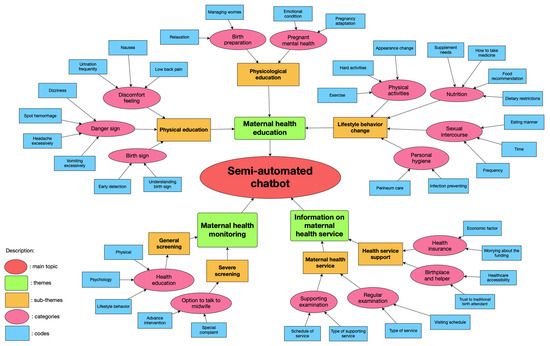
Figure 6.
The conceptual map.
Figure 6 shows the conceptual map as synthesized by the qualitative data. First, the researcher determined the coding, marked with blue boxes. This coding became the basis for categorizing, marked with a pink oval shape. Second, these categories were then grouped into sub-themes marked with orange boxes. Subsequently, they were merged into three major themes marked with green boxes as the main topics needed in the semi-automated chatbot.
3.1. Maternal Health Education
Chatbot-based semi-automatic teleconsultation could be one form of media for maternal health education. The semi-automated interaction education requires the design of stored and adapted answers to the information needs of pregnant women and midwives. The interviews showed that this education consisted of physical and psychological complaints and lifestyle changes. Those were critical educational topics and could be accessed quickly using automated chatbots.
3.1.1. Physical Education
The number of physical complaints experienced during pregnancy was one of the reasons for the importance of education and information about valid and fast answers. Semi-automated chatbot-based teleconsultation was considered a medium for health education, offering an immediate response to physical complaints experienced by mothers. Information on physical complaints summarized from the interview results included the danger signs of pregnancy, discomfort in pregnancy, and labor symptoms.
“…about complaints of nausea, vomiting and current condition … Yes, so we can consult quickly”(Pregnant Women’s FGD)
In addition to opinions from pregnant women, midwives also recommended providing education related to general physical complaints and early detection of labor signs.
“General danger signs, nausea and vomiting, signs of bleeding or heartburn maybe yes, dizziness, stomach pains like that. How to drink iron tablet (Fe), vitamins, all shown.”(Midwives’ FGD)
“Many people complain of back pain, I said because the baby is getting bigger and want to give birth”(Midwives’ FGD)
3.1.2. Psychological Education
Psychological complaints were one of the essential topics for pregnant women in preparation for childbirth and readiness to become a mother. According to informants, complaints about the mother’s mental condition during pregnancy could be served and supported through educational chatbots by providing answers automatically. The reason was that the mental preparation of pregnant women for childbirth needs to be carefully prepared. Mental health screening was also necessary. The informant hoped that chatbots could be a medium to overcome the mental health of pregnant women quickly.
“Because we are also often given mental screening for pregnant women in the health care programs, such as filling questionnaires like do you feel, for example, that you have not slept for three days or not? I think it’s important to give mental education by chatbot”(Midwives’ FGD)
“Ee.. that’s not all. The mental preparation before giving birth needs to be supported and educated”(Pregnant Women’s FGD)
3.1.3. Lifestyle Change Education
Changes in lifestyle needed in the discussion topics through this semi-automated chatbot service include information about daily activities, husband–wife relationships, changes in women’s appearance, changes in nutritional patterns, and personal hygiene.
“The way husband and wife may have sex in the first pregnancy. How many months or how many weeks is the inspection? Eating patterns, resting patterns, sleeping patterns”(Midwives FGD)
Some patients said pregnant women’s diet changes were significant as educational materials through chatbots. Besides, the lack of awareness of mothers in changing their appearance was also essential information conveyed. Good appearance changes supported and facilitated the pregnancy process.
“Avoiding unhealthy foods.. Not staying up late, sleeping regularly”(Midwives’ FGD)
“Yes, how do you do it every day to stay healthy. Dietary habit. How do you keep it clean.”(Pregnant Women FGD)
“Clothes. Some pregnant women still wear little pants. The pants are strict jeans normally. Then sandals are usually high heels for pregnant women”(Midwives’ FGD)
3.2. Information on Maternal Health Service
One of the topics frequently asked by pregnant women is that of maternal health services. According to pregnant women and midwives, this topic comprises general information that can be quickly responded to and does not need to wait for validation from health workers to provide it via an automated chatbot.
3.2.1. Mother’s Health Checkup
It consisted of general and supporting health checks, such as the schedule of visits, the type of service (pregnancy, family planning, repeat visits), and the number of controls.
“Schedule an appointment or consul meet with the midwife”(Pregnant women’s FGD)
“Pregnant women do not schedule repeat visits once a day, for example, once a month. Trimester from this to this. For those who are 8 months and over 2 weeks, once. So someone asked later to check again when yes. Later, if I control it again, I’m afraid I’ll forget again. But usually, if it’s like you’ve been to the health center, I’ll let you know the return visit”(Midwives’ FGD)
3.2.2. Mother’s Service Support
Teleconsultation media should provide information on health insurance, birthplace, and health workers’ recommendations to prepare for delivery in a health facility. According to pregnant women and midwives, information on health services during pregnancy was needed because there were still pregnant women who did not give birth to health workers. Supporting examinations also needed information given to pregnant women to increase knowledge on early detection.
“Lab checks. Ultrasound, screening”(Midwives’ FGD)
There was still trust in ‘paraji’ or traditional birth attendants, encouraging women to give birth with paraji instead of in a health facility. The reason was the hesitation of the cost of giving birth in health facilities. According to the midwife’s interview, information about the importance of giving birth to health workers, financing, and health insurance could be answered automatically through chatbots.
“There are also deliveries (by parajis), so maybe the education is lacking, yes, the education is like that. Ee..yes, the economy is too. The average is the economy. There are still some, but not many. It’s just… there are. The second first child is the same as the paraji, huh”(Midwives’ FGD)
Health insurance information is a solution in providing awareness about health care support that mothers can access.
“Sometimes, people who are economically dependent are thinking about costs. At least we should be educated about BPJS (national health insurance) problems from the start”(Midwives’ FGD)
3.3. Health Monitoring
3.3.1. General Health Monitoring
Chatbots were recommended to be able to answer complaints of a general condition. This aimed to avoid self-diagnosis, which may lead to misdiagnoses. Thus, the available monitoring information could be a solution to increase knowledge and support early detection.
“You can remind us that there are several programs, which are like a class for pregnant women, can you not include them so they can join. Even though we don’t…”(Pregnant Women’s FGD)
The midwife recommended helping to answer general complaints with a chatbot, but health workers must examine further complaints.
“For example, from the pregnant woman, there is this complaint. For example, all complaints are accommodated by the chatbot. Answered by chat, how is it? Later, they will ask again, if the chatbot has not been able to accommodate the patient’s answer, maybe they can be directed to the midwife as soon as possible”.(Midwives’ FGD)
3.3.2. Advanced Monitoring
Further management of pregnant women’s condition was required to be confirmed with health workers. Pregnant women considered getting information through a validated chatbot rather than looking for information on their own through the internet, whose source accuracy was unknown. Pregnant women preferred communicating with health professionals as experts to support decisions about their health conditions for severe cases.
“…about complaints… Yes, so we can consult with the person concerned, the health workers as well so that we know that we are not driven by google. So go straight to the experts…”(Pregnant Women’s FGD)
The midwife argued that the complaints of pregnant women could not be automatically controlled by communication machines such as chatbots. Clinical decisions on further patient complaints should be handled directly by the midwife.
“Well, for example, in my opinion, everything should be accommodated first. If there are 10 patients, try to be answered by the chatbot first. Well, later, if the patient has been accommodated with the chatbot’s answer, thank God. If the patient still feels anxious and wants to ask further questions, it can be brought up to communicate with the midwife”(Midwives’ FGD)
4. Development of the Chatbot
From the theme found in the qualitative data, the decision tree was developed to structure questions and answers along with decisions that will be realized on the chatbot. Figure 7 shows the chatbot development process from the initial process (knowledge engineering) to its user interface development. The chatbot consists of two main parts: (1) a user interface that deals directly with users and (2) an inference engine to seek answers to consultations or questions via chat. Software engineers built the first part to accommodate the needs of users (pregnant women) and stakeholders (midwives). These needs comprised three themes: (1) maternal health education, (2) health monitoring, and (3) information on maternal health services. Subsequently, when the user started a consultation using a chatbot, the inference engine sought answers from the consultation based on the knowledge acquired by the knowledge engineer. The knowledge was developed based on the latest literature and experts’ validation through the knowledge engineering process. The acquired knowledge was stored in a knowledge base with a decision tree structure.
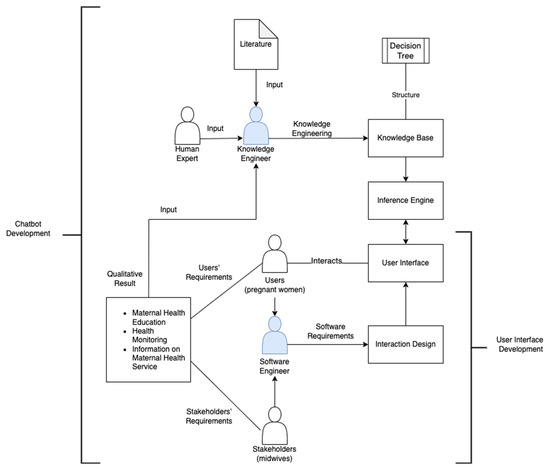
Figure 7.
The process of chatbot and its user interface development.
The decision tree started with a conversation about physiological complaints and then continued with pathological complaints with chat directions for professionals. It aimed to help patients obtain information to fill their knowledge gaps before visiting health workers [23]. The following decision tree for building a semi-automated chatbot for pregnant women is presented in Figure 8.
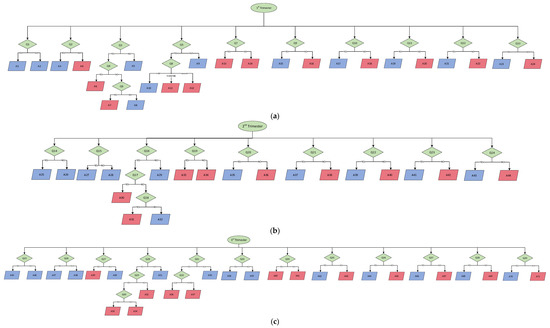
Figure 8.
(a) Decision tree of the semi-automated chatbot for 1st Trimester. (b) Decision tree of the semi-automated chatbot for 2nd Trimester. (c) Decision tree of the semi-automated chatbot for the 3rd Trimester.
From the decision tree method in Figure 8a–c, it can be seen that many codes were compiled, such as the Q codes, marked with a green oval shape as questions that are listed in Appendix B. Then, Code A, which means the answers are marked with a blue box, can be seen in Appendix C. From the decision tree method concept, the semi-automated chatbot is presented in Figure 9.
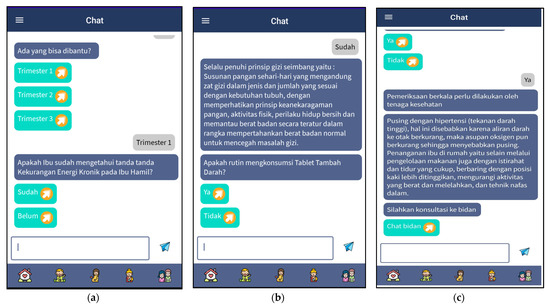
Figure 9.
The screen captures the semi-automated chatbot. (a) General health screening on a chatbot, (b) education on common complaints, and (c) chat options for midwives as further complaints.
In Figure 9, the chatbot appears in the extended iPosyandu app in Bahasa Indonesia. Aside from screening general questions at the beginning, shown in Figure 9a, health education according to patients’ queries and conditions is shown in Figure 9b. Afterward, the conversation ended with the recommendation of options to chat or talk to the midwife to strengthen health decisions mentioned in Bahasa Indonesia, “Silahkan konsultasi ke bidan”, which means “Please consult the midwife” Figure 9c.
5. Discussion
Qualitative data exploration methods have benefits and have become the basis for determining needs based on human perspectives and experiences [51]. As the intervention is intended for users, it is necessary to involve the target in developing research. The reason is that a health intervention tool can appropriately answer the requirements in its implementation if it concerns the user’s need [52]. A user-centered approach has become an effective method to determine the success of the intervention field [26,53]. User perspective can also help provide insight to researchers, application designers, and health providers in developing and evaluating health applications [15,53,54,55]. Other research explained that user evaluation through quantitative analysis after conducting qualitative methods could be used to strengthen the success of health intervention development studies [54,55,56]. However, previous studies have shown that several health applications successfully developed with qualitative exploratory methods [57,58]. Therefore, using qualitative design to explore information with a user-centered approach can be critical in application development research [12,59,60].
This qualitative research demonstrated the needs of pregnant women in the chatbot’s contents through three major themes: (1) maternal health education, (2) information on maternal health services, and (3) health monitoring. The content developed is in the form of question and answer, applying the decision tree method. Since the content is one factor that attracts clients to chatbots [22], the quality of the content must be considered according to the user’s needs, evidence, and expert recommendations [28]. All themes of chatbot content in this research were based on the user’s perspective and were related to the function of a chatbot as a preventive tool to support self-care and decision-making [61,62].
The first theme is maternal health education. In this theme, a chatbot is expected to be able to provide education about physical and psychological complaints and lifestyle behavior changes. This implies that chatbot technology is a good innovation with the capabilities of improving teaching and learning and all other aspects of education [22,57,63]. Furthermore, a recent systematic literature review study stated that chatbots for education have highly regarded benefits due to the integration of contents, quick access to educational information, motivation, and engagement because of their attractiveness, allowing multiple users simultaneously and immediate assistance [22]. Chatbots for education can also help deal with the physical complaints of pregnant women through a simple and exciting question-and-answer system [25]. Consequently, developing a chatbot that provides treatment for pregnant women’s physical complaints can be a strategy to increase knowledge and support early detection of their health problems.
Regarding the maternal health education theme, psychological issues often need to be one of the topics since they can become a problem during pregnancy and after giving birth. A systematic review found that anxiety symptoms reported during pregnancy had a combined prevalence of 22.9% across trimesters [64]. Chatbots can efficiently deal with increasing mental health problems [19,65,66,67], especially in motivating and overcoming anxiety or depression [68,69,70]. Patients feel comfortable using chatbots since it can reduce the fear of stigma when conducting health consultations using chatbots compared to humans [25,66]. Apart from psychological issues, lifestyle behavior changes for pregnant women should also be a maternal health education topic using mHealth [71,72]. A woman’s behavior during pregnancy impacts her mother and baby [72]. Previous research identified that chatbots could manage healthy lifestyle changes [20,73,74]. In this instance, chatbots can be virtual coaches, promoting physical activities and increasing human competence for healthy lifestyle education [18,65].
The second theme is information on maternal health services, which consist of routine and supporting examinations, as essential knowledge during pregnancy. The role of chatbots in increasing access to health services is shown in the previous research. Chatbots do not participate in providing health services but are an entry point for using health services [43]. Chatbots can deliver administrative-related benefits, especially in scheduling doctor appointments, finding health clinics, providing reminders for medication adherence, providing medication instructions, and answering commonly asked medication questions [16,75]. The main objective is to increase the efficiency of health services by reducing the effort and increasing the speed of access [16,75]. For that reason, chatbot providers can support maternal services by connecting patients with healthcare professionals, finding medical drugs online, or providing healthcare customer service tasks.
The third theme needed is health monitoring, another essential function of the health chatbot. Previous research states that chatbots can monitor symptoms to encourage healthy behavior [65]. However, ethically, the chatbot is not considered to be mature enough to perform health diagnostics [40,42]. A recent systematic literature review indicated that patient safety concerning chatbot consultation services needed to be observed since it might not recognize or respond appropriately when questioned about a serious health concern [59]. Chatbots are also associated with the risk that patients may self-diagnose too often and not understand the diagnosis, or patients may not feel connected to their primary physician [23,42]. This technology cannot substitute creditable health information sources from a health professional [16,41,42,76]. The chatbot designed on the extended iPosyandu application is only used for general complaints, where further or particular complaints are directed to non-automated consultations with midwives (semi-automated).
A primary step in developing a chatbot is strengthening the knowledge base. Building a decision tree can help to create a semi-automated chatbot with prediction and classification inside the knowledge base [77]. Since the benefits of decision trees method in the health sector include predicting disease, early detection, analyzing disease severity, and clinical decision-making [30,32,35,78], this method is suitable to help midwives and pregnant women to make health decisions through chatbots [38,62]. However, previous research has stated that a challenge in the use of the decision tree is the problem of overfitting. Overfitting usually occurs when the tree has too many nodes relative to the amount of training data available in machine learning [79]. To avoid this challenge, the semi-automated chatbot development in this study used forward chaining, or an expert data-based system that works with a set of known facts and applies rules to generate new facts whose premise matches the known facts to achieve the previously determined goal [80,81]. Forward chaining is also a natural solution to some problems, starting with information gathering. The decision tree in this study was applied to strengthen the knowledge base by exploring the needs of patients and health workers and reviewing literature or evidence, whose content was then validated by experts [28]. This method’s effectiveness and accuracy can help support clinical decisions with various suggestions and reasons [34,35].
Strengths and Limitations
One of the strengths of this research is that there is still rarely study on the development of semi-automated chatbots (a combination of automated chatbots and health workers’ communication), particularly for pregnant women. Besides, this semi-automated chatbot was developed through a decision tree method involving experts and using a user-centered approach to support the clinical decision. This research also highlighted strengthening knowledge-based in the development process using forward chaining to support quality content. Another strength is that this study used a focus group discussion to explore various opinions to provide a broad perspective regarding user needs and enrich the content of the educational chatbot for pregnant women.
Nevertheless, this study also has limitations. The research method for developing a health intervention through the chatbot only used qualitative methods from the user’s perspective. However, previous studies on developing new applications used a mixed-method approach, from qualitative to quantitative, to strengthen the results [12,38]. For this reason, future research needs to measure users’ evaluation quantitatively.
6. Conclusions
Information needed by pregnant women and midwives from semi-automated chatbots includes maternal health education, maternal health services, and health monitoring. In health monitoring, an automated chatbot can provide general health screening. At the same time, for further complaints, patients are advised to direct chat or communicate with a midwife to avoid self-diagnosis (non-automatic). To ensure the quality of semi-automated chatbot development, the decision tree method, with the exploration of a user-centered approach, collecting literature, and expert recommendations, can be alternatives to support clinical decisions and assist in early detection for pregnant women and midwives.
Author Contributions
Conceptualization, I.W.P., F.R.R. and W.G.P.; methodology, I.W.P., F.R.R. and H.S.; writing—original draft preparation, I.W.P. and F.R.R.; writing—review and editing, I.W.P., F.R.R. and W.G.P.; software, W.G.P.; validation, I.W.P., F.R.R., W.G.P. and A.I.S.; formal analysis, I.W.P., F.R.R., H.S. and A.I.S.; visualization; I.W.P., W.G.P. and A.I.S.; supervision, F.R.R., W.G.P., H.S. and A.I.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research and publication was funded by the Indonesia Endowment Fund for Education, abbreviated LPDP (Lembaga Pengelola Dana Pendidikan), the Ministry of Finance, Indonesia, and Universitas Padjadjaran, Bandung, West Java, Indonesia.
Institutional Review Board Statement
The study was approved by the Faculty of Medicine Ethics Committee of Universitas Padjadjaran Bandung, Indonesia (etic code 255/UN6.KEP/EC/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are openly available at https://osf.io/esnt7/ (accessed on 15 October 2022).
Acknowledgments
The authors would like to express their deepest gratitude to the Indonesia Endowment Fund for Education, abbreviated as LPDP (Lembaga Pengelola Dana Pendidikan) under the Ministry of Finance, Indonesia, and Universitas Padjadjaran, Bandung, West Java, Indonesia for supporting the funding of the research and publication of the article; the Purwakarta Regency Health Office, West Java Indonesia, for permission to conduct the research; Puskesmas Purwakarta, Koncara, and Pasawahan, Purwakarta Regency, West Java, Indonesia for facilitating the research in the Posyandu; and the Informatics Engineering Study Program, Faculty of Engineering, Universitas Pasundan, Indonesia, for contributing to the development of the mobile application.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Guidelines for Focus Group Discussion.
Table A1.
Guidelines for Focus Group Discussion.
| No | Questions | Key Probing |
|---|---|---|
| A | Usage of Health Care Chatbots | |
| What do you think about using semi-automated chatbot-based teleconsultation in Posyandu services? | How familiar are people with the help of semi-automated chatbots | |
| B | Perceived benefits of healthcare chatbots | |
| What do you think about the benefits of using chatbots in healthcare for patients? | Treatment and monitoring Health care support Education Changes in lifestyle behavior Diagnosis | |
| C | Content and substance | |
| 1 | Treatment and Monitoring | |
| What information should the chatbot provide regarding treatment and health monitoring? | Pregnant women in all Trimesters Treatment: Iron Tablet, Folic Acid, calcium, nutrition General and severe complaint | |
| 2 | Health Care Services Support | |
| What information do you think the chatbot should provide regarding healthcare support? | Pregnant women in all Trimesters Place of delivery Supporting service Mental support | |
| 3 | Education | |
| In your opinion, what information should a chatbot provide regarding health education? | Pregnant women 1st Trimester (adaptation, discomfort, nutrition) Pregnant women 2nd Trimester (discomfort, complaints) Pregnant women 3rd Trimester (delivery plan, family planning) Prevention of eclampsia | |
| 4 | Lifestyle Behavioral Changes | |
| In your opinion, what information should be provided by chatbots regarding lifestyle and changes in health habits? | Nutrition Personal hygiene Exercise Daily habit | |
| 5 | Diagnosis tentative | |
| In your opinion, what information should be provided by chatbots and chat midwives regarding health diagnosis? | Pregnant women in all Trimesters Anemia Chronic energy deficiency Pre-eclampsia | |
Appendix B
Table A2.
The Question List of Decision Tree.
Table A2.
The Question List of Decision Tree.
| Code | Description |
|---|---|
| Q1 | Do you know the signs of chronic energy deficiency (CED) in pregnant women? |
| Q2 | Do you regularly take iron tablets? |
| Q3 | Do you feel dizzy? |
| Q4 | Does high blood pressure accompany it? |
| Q5 | Do you have nausea and vomiting? |
| Q6 | If not, is it accompanied by other complaints? |
| Q7 | Is there any spot bleeding from the vagina? |
| Q8 | How many times have you had nausea in the last 24 h? |
| Q9 | Do you know about prenatal care or antenatal care (ANC)? |
| Q10 | Do you know the purpose of antenatal care? |
| Q11 | Do you know the type and purpose of a repeat pregnancy visit? |
| Q12 | Do you know about supporting examinations during pregnancy? |
| Q13 | Do you already know about the financing of pregnancy and childbirth examinations? |
| Q14 | Do you have back pain? |
| Q15 | Do you feel the urge to urinate frequently? (Frequency about 10 times per day?) |
| Q16 | Do you feel dizzy? |
| Q17 | Is there any spot bleeding from the vagina? |
| Q18 | Does high blood pressure accompany it? |
| Q19 | If not, is it accompanied by other complaints? |
| Q20 | Do you know of prenatal care or antenatal care (ANC)? |
| Q21 | Do you know the purpose of antenatal care? |
| Q22 | Do you know the type and purpose of a repeat pregnancy visit? |
| Q23 | Do you know about supporting examinations during pregnancy? |
| Q24 | Do you already know about the financing of pregnancy and childbirth examinations? |
| Q25 | Do you have back pain? |
| Q26 | Do you feel the urge to urinate frequently? (Frequency about 10 times per day?) |
| Q27 | Do you feel a regular contractions? |
| Q28 | Do you feel dizzy or have a headache? |
| Q29 | If so, is it accompanied by high blood pressure of more than 140/90? |
| Q30 | If so, is it accompanied by swelling in the feet, hands, and face, or impaired vision/blurred vision? |
| Q31 | Do you feel the fetal movement is reduced? |
| Q32 | If yes, how many times did you feel fetal movements? |
| Q33 | Do you feel frequent hand and foot cramps? |
| Q34 | Do you often have trouble sleeping or feeling anxious? |
| Q35 | Do you know about prenatal care or antenatal care (ANC)? |
| Q36 | Do you know the purpose of antenatal care? |
| Q37 | Do you know the type and purpose of a repeat pregnancy visit? |
| Q38 | Do you know about supporting examinations during pregnancy? |
| Q39 | Do you already know about the financing of pregnancy and childbirth examinations? |
Appendix C
Table A3.
The Answer List of Decision Tree.
Table A3.
The Answer List of Decision Tree.
| Code | Description |
|---|---|
| A1 | Please comply with the principles of balanced nutrition, such as daily food composition containing nutrients according to the body’s needs, managing food diversity, physical activity, personal hygiene behavior, and maintaining body weight to prevent nutritional problems. |
| A2 | Chronic energy deficiency (CED) is a condition when pregnant women who have been malnourished for a long time (several months/years) and whose upper arm circumference is less than 23.5 cm. Pregnant women with CED will give birth to low birth weight (LBW). Based on the national research data (2013), this problem needs special attention as the prevalence of the risk of CED in pregnant women is 24.2%. |
| A3 | Go ahead and regularly check with the midwife. The required daily quantity of iron (Fe) in pregnant women is about 800 mg. This requirement consists of 300 mg needed for the fetus and 500 g to increase the mass of maternal hemoglobin. An excess of about 200 mg can be excreted through the intestines, skin, and urine. In the diets of pregnant women, every 100 calories can produce as much as 8–10 mg of Fe. Thus, the need for iron is still lacking in pregnant women, so they need additional intake in the form of Fe tablets. |
| A4 | It is recommended to take blood-added tablets during pregnancy. If you do not know your hemoglobin level, you should regularly undergo laboratory tests and check with the midwife/doctor. During the gestation period, through the estimated 288 days, pregnant women make about 100 mg of iron. Thus, the need for iron is still lacking in pregnant women, so they need additional intake in the form of Fe tablets. Please consult the midwife => Chat midwife. |
| A5 | Please continue to the other question. |
| A6 | If so, periodic checks need to be carried out by health workers. Dizziness with hypertension (high blood pressure) is due to reduced blood flow to the brain, so oxygen intake is reduced, causing dizziness. Besides food management, healthcare for mothers at home includes adequate rest and sleep, elevated legs, reducing strenuous and tiring activities, and deep breathing techniques can be alternative treatments for dizziness with hypertension (Hicks, 2015; Irianti et al., 2014). Please consult the midwife => and chat midwife. |
| A7 | If yes, please consult a midwife. Dizziness during pregnancy can be caused by anemia, hypertension, and low sugar levels. Anemia occurs due to increased blood plasma volume, which causes the mother’s hemoglobin level to decrease. Pregnant women with anemia should consume an additional iron tablet to increase hemoglobin levels or increase the intake of foods containing iron. Besides, pregnant women with low sugar levels can be supported with nutritionally balanced foods during pregnancy and a healthy lifestyle. Please consult the midwife => and chat midwife. |
| A8 | If not, please maintain a pattern of rest, nutrition and light exercise. Dizziness or feeling faint or light-headed are typical symptoms during pregnancy. This is more common in the first trimester, but the mother may experience it during pregnancy. Dizziness during pregnancy usually occurs due to the body trying to balance the increased blood circulation and the fetus’s growth. When entering the second trimester of pregnancy, the enlarged uterus can press on the blood vessels, causing headaches or dizziness. |
| A9 | Please continue to the other question. |
| A10 | Morning sickness is one of pregnancy’s earliest, most common, and most stressful symptoms. Nearly 50–90% of pregnant women experience nausea and vomiting in the first trimester. Nausea and vomiting are often overlooked because they are considered a consequence of early pregnancy, without regard to its severe impact on women. Most pregnant women who experience morning sickness will experience changes in the hormones progesterone and estrogen in the body, which cause morning sickness in the first trimester of pregnancy. Get plenty of rest to relieve stress and relieve fatigue. Consume foods that are high in protein, low in fat, and smooth in texture for easy swallowing and digestion. Eat food in small portions, but often. Avoid oily, spicy or strong-smelling foods that can trigger nausea. Drink more water to prevent dehydration, and consume drinks containing ginger to relieve nausea and warm the body. Use aromatherapy to reduce morning sicknesses, drinks containing ginger to ease nausea, warm the body and take pregnancy supplements to meet the need for vitamins and iron. |
| A11 | Please check with a health worker to get optimal treatment. Please consult the midwife => Chat midwife. |
| A12 | Please go to a health worker immediately to get optimal treatment. Please consult the midwife => Chat midwife. |
| A13 | If so, bleeding is one of the danger signs for pregnant women. Please consult a health worker. Please consult the midwife => and chat midwife. |
| A14 | Please consult the midwife => and chat midwife. |
| A15 | Please continue to the next question. |
| A16 | 1st Trimester: 1 visit at 0–13 weeks of gestation 2nd Trimester: 1 visit at 14–28 weeks of gestation 3rd Trimester: 2 trips at 28–36 weeks of pregnancy and 36–40 weeks. Every pregnant woman is advised to have a comprehensive and quality antenatal visit at least four times, i.e., once before the 4th month of pregnancy, then around the 6th month of pregnancy, and two times around the 8th and 9th month of pregnancy. The minimum standard for ANC examination consists of 10 steps: 1. Weighing each visit and record. 2. Measuring blood pressure, usually 110/80–below 140/90. 3. Determining the value of nutritional status by measuring the upper arm circumference (LILA). 4. Determining uterine fundal height (top of the uterus): monitor fetal development. 5. Giving TT (Tetanus Toxoid) immunization. 6. Determine fetal presentation and fetal heart rate (FHR). 7. Giving iron tablets. 8. Conducting laboratory tests (syphilis, Hepatitis B and HIV). 9. Providing case management. 10. Conducting interviews (counseling), including planning for delivery and post-delivery. If you still want to ask further, please get in touch with the midwife. |
| A17 | Please continue to the next question. |
| A18 | 1. To optimize the mental and physical health of pregnant women. 2. To detect the risk of complications in pregnancy and childbirth. 3. To motivate the mother’s desire for the postpartum period and exclusive breastfeeding. If you still want to ask further, please get in touch with the midwife. |
| A19 | Please continue to the next question. |
| A20 | 1. The first visit in the first trimester (16 weeks) was carried out to screen and treat anemia, plan for delivery and treat complications due to medication. 2. The second visit in the second trimester (<28 weeks) was conducted for complications due to medication and medication screening for preeclampsia, Gemelli, infections of the reproductive organs, and urinary tract. 3. The third visit in the third trimester (<36 weeks) and the fourth visit in the third trimester (> 36 weeks) were carried out to identify any abnormalities in the location and presentation, strengthen delivery plans, and recognize signs of labor. If you still want to ask further, please get in touch with the midwife. |
| A21 | Please continue to the next question. |
| A22 | Urine test 1. The urine test is essential to the 1st-trimester pregnancy check. It aims to detect a positive pregnancy and whether there are other diseases that the pregnant woman suffers from. Some of the things that become the benchmark for urine tests are: 1. The protein and sugar levels in pregnant women’s urine tend to be low. In addition, the urine of pregnant women also contains the hormone HCG (Human Chorionic Gonadotropin) at relatively high levels. 2. If the urine contains high levels of ketones and sugar, it means that the pregnant woman has gestational diabetes. 3. Proteins in pregnant women signify that the mother has pre-eclampsia or certain bacterial infections. Blood Test 1. Determination of blood type, whether the mother’s blood type is A, B, AB or O. 2. Determination of rhesus blood, whether rhesus positive or negative. This rhesus examination is essential and will later be matched with the baby’s rhesus. The sign is standard if the mother and baby have the same rhesus. However, suppose the mother’s rhesus is different from the baby’s. If the mother is rhesus positive and the baby is rhesus negative, the baby will suffer from blood disorders. 3. Checking hemoglobin. It is also important to detect whether the mother has anemia. Pregnant women have hemoglobin levels of about 10–16 g per liter in their blood. 4. Hepatitis B and C examination is conducted to determine whether there is a viral infection in the mother’s liver. A pregnant woman with hepatitis is at risk of passing the disease on to her fetus. 5. Examination for rubella, a measles disease in which the mother’s body develops a red rash. This disease is a risk for mothers at under five months of gestational age. Generally, the rubella virus is transmitted through sneezing, saliva and coughing by the sufferer. Ultrasound test (ultrasonography) An examination that doctors offer to pregnant women is an ultrasound test. Today’s technology is very sophisticated. This makes it possible to detect the fetus from an early age (first trimester). This ultrasound test has many uses, including: 1. Observing the structure of the fetus in the stomach. 2. Checking the normal condition of the uterus, placenta, and amniotic fluid. 3. Observing the growth of the fetus. 4. Estimating gestational age. 5. Detecting the presence or absence of abnormalities or physical defects in the fetus. Triple Elimination Check Laboratory personnel carries out a capillary blood examination to determine the results of HIV, syphilis and hepatitis tests. Reasons to have a triple elimination check 1. Stopping the growth of HIV, syphilis, and hepatitis B in the bod 2. Protecting sexual partner from the transmission of HIV, syphilis, and hepatitis B 3. Having children who are free from HIV, syphilis, and hepatitis B If you still want to ask further, please get in touch with the midwife => chat midwife |
| A23 | Please continue to the next question. |
| A24 | To receive Indonesian National Health Insurance (JKN), please register first. During pregnancy, management JKN can cover 3 services, divided into: - Trimester 1: carried out once at 1–12 weeks of pregnancy - Trimester 2: carried out once at 13–28 weeks of pregnancy - Trimester 3: carried two times at 29–40 weeks of pregnancy JKN can cover the cost of ultrasonography services when pregnant women are referred by a First Level Health Facility (FKTP). The cost of pregnancy checks borne by JKN: 1. Pre-delivery or antenatal care (ANC) examination - In the form of a package with a maximum of 4 visits, worth IDR 200,000. - ANC checks that are not only carried out in one place are worth IDR 50,000 per visit. 2. Normal delivery or vaginal delivery - Normal delivery performed by a midwife is worth IDR 700,000. - Normal delivery performed by a doctor is worth IDR 800,000. - Normal delivery with basic emergency measures at the Puskesmas is covered by Rp. 950,000. 3. Deliveries referred to advanced-level health facilities Under certain conditions, pregnant women participating in JKN who cannot give birth typically, and must be referred to help through a cesarean section due to limited experts and medical equipment, can be covered by JKN. If you still want to ask further, please get in touch with the midwife. |
| A25 | If so, this is normal in the 3rd trimester due to the enlargement of the uterus. Regular exercise is a critical component of lifestyle interventions recommended for pregnant women as part of antenatal care (ANC) to prevent excessive weight gain during pregnancy. Pregnant women with low back and pelvic pain usually improve within a few months after birth (WHO, 2016). |
| A26 | Please continue to the other question. |
| A27 | If so, this is normal for pregnant women in the 2nd trimester due to pressure on the bladder from the enlarged uterus. |
| A28 | Please continue to the other question. |
| A29 | Please continue to the other question. |
| A30 | If so, periodic checks need to be carried out by health workers. Dizziness with hypertension (high blood pressure) is due to reduced blood flow to the brain, so oxygen intake is reduced, causing dizziness. Besides food management, healthcare for mothers at home includes adequate rest and sleep, elevated legs, reduced strenuous and tiring activities, and deep breathing techniques can be alternative treatments for dizziness with hypertension (Hicks, 2015; Irianti et al., 2014). Please consult the midwife => and chat midwife. |
| A31 | If yes, please consult a midwife. Dizziness during pregnancy can be caused by anemia, hypertension, and low sugar levels. Anemia occurs due to increased blood plasma volume, which causes the mother’s hemoglobin level to decrease. Pregnant women with anemia should consume an additional iron tablet to increase hemoglobin levels or increase the intake of foods containing iron. Besides, pregnant women with low sugar levels can be supported with nutritionally balanced foods during pregnancy and a healthy lifestyle. Please consult the midwife => and chat midwife. |
| A32 | If not, please maintain a pattern of rest, nutrition, and light exercise. Dizziness or feeling faint or light-headed is typical symptoms during pregnancy. This is more common in the first trimester, but the mother may experience it during her pregnancy. Dizziness during pregnancy usually occurs due to the body trying to balance the increased blood circulation and the fetus’s growth. When entering the second trimester of pregnancy, the enlarged uterus can press on the blood vessels, causing headaches or dizziness. |
| A33 | If so, bleeding is one of the danger signs for pregnant women. Please consult a health worker. Please consult the midwife => and chat midwife. |
| A34 | Please consult the midwife => and chat midwife. |
| A35 | Please continue to the next question. |
| A36 | 1st trimester: 1 visit at 0–13 weeks of gestation 2nd trimester: 1 visit at 14–28 weeks of gestation 3rd trimester: 2 trips at 28–36 weeks of pregnancy and 36–40 weeks. Every pregnant woman is advised to have a comprehensive and quality antenatal visit at least four times, i.e., once before the 4th month of pregnancy, then around the 6th month of pregnancy, and two times around the 8th and 9th month of pregnancy. The minimum standard for ANC examination consists of 10 steps: 1. Weighing at each visit and recording. 2. Measuring blood pressure, usually 110/80–below 140/90. 3. Determining the value of nutritional status by measuring the upper arm circumference (LILA). 4. Determining uterine fundal height (top of the uterus): monitor fetal development. 5. Giving TT (Tetanus Toxoid) immunization. 6. Determine fetal presentation and fetal heart rate (FHR). 7. Giving iron tablets. 8. Conducting laboratory tests (syphilis, Hepatitis B and HIV). 9. Providing case management. 10. Conducting interviews (counseling), including planning for delivery and post-delivery. If you still want to ask further, please get in touch with the midwife. |
| A37 | Please continue to the next question. |
| A38 | 1. To optimize the mental and physical health of pregnant women. 2. To detect the risk of complications in pregnancy and childbirth 3. To motivate the mother’s desire for the postpartum period and exclusive breastfeeding. If you still want to ask further, please get in touch with the midwife |
| A39 | Please continue to the next question. |
| A40 | 1. The first visit in the 1st trimester (16 weeks) was carried out to screen and treat anemia, plan for delivery, and treat complications due to medication. 2. The second visit in the 2nd trimester (<28 weeks) was conducted for complications due to medication and medication screening for preeclampsia, Gemelli, infections of the reproductive organs, and urinary tract. 3. The third visit in the 3rd trimester (<36 weeks) and the fourth visit in the 3rd trimester (>36 weeks) were carried out to identify any abnormalities in the location and presentation, strengthen delivery plans, and recognize signs of labor. If you still want to ask further, please get in touch with the midwife. |
| A41 | Please continue to the next question. |
| A42 | Urine test 1. The urine test is essential to the 1st-trimester pregnancy check. It aims to detect a positive pregnancy and whether there are other diseases that the pregnant woman suffers from. Some of the things that become the benchmark for urine tests are: 1. The protein and sugar levels in pregnant women’s urine tend to be low. In addition, the urine of pregnant women also contains the hormone HCG (Human Chorionic Gonadotropin) at relatively high levels. 2. If the urine contains high levels of ketones and sugar, the pregnant woman has gestational diabetes. 3. Proteins in pregnant women signify that the mother has pre-eclampsia or certain bacterial infections. Blood Test 1. Determination of blood type, whether the mother’s blood type is A, B, AB, or O. 2. Determination of rhesus blood, whether rhesus positive or negative. This rhesus examination is essential, which will later be matched with the baby’s rhesus. The sign is standard if the mother and baby have the same rhesus. However, suppose the mother has a different rhesus from the baby. In that case, if the mother is rhesus positive and the baby is rhesus negative, the baby suffers from blood disorders. 3. Checking of hemoglobin. It is also important to detect whether the mother has anemia. Pregnant women have hemoglobin levels of about 10–16 g per liter in their blood. 4. Hepatitis B and C examination is to determine whether there is a viral infection in the mother’s liver or not. A pregnant woman with hepatitis is at risk of passing the disease on to her fetus. 5. Examination for rubella, a measles disease in which the mother’s body develops a red rash. This disease is a risk for mothers under five months of gestational age. Generally, the rubella virus is transmitted through the sneezing, saliva, and coughing of the sufferer. Ultrasound test (ultrasonography) An examination that doctors offer to pregnant women is an ultrasound test. Today’s technology is very sophisticated. This makes it possible to detect the fetus from an early age (first trimester). This ultrasound test has many uses, including: 1. Observing the structure of the fetus in the stomach 2. Checking the normal condition of the uterus, placenta, and amniotic fluid 3. Observing the growth of the fetus 4. Estimating gestational age 5. Detecting the presence or absence of abnormalities or physical defects in the fetus Triple Elimination Check Laboratory personnel carries out a capillary blood examination to determine the results of HIV, syphilis, and hepatitis tests. Reasons to undergo a triple elimination check: 1. Stopping the growth of HIV, syphilis, and hepatitis B in the bod 2. Protecting sexual partner from the transmission of HIV, syphilis, and hepatitis B 3. Having children who are free from HIV, syphilis, and hepatitis B If you still want to ask further, please get in touch with the midwife. |
| A43 | Please continue to the next question. |
| A44 | To receive Indonesian National Health Insurance (JKN), please register first. During pregnancy, management JKN can cover 3 services, divided into: - Trimester 1: carried out once at 1–12 weeks of pregnancy - Trimester 2: carried out once at 13–28 weeks of pregnancy - Trimester 3: carried two times at 29–40 weeks of pregnancy JKN can cover the cost of ultrasonography services when pregnant women are referred by a First Level Health Facility (FKTP). The cost of pregnancy checks borne by JKN: 1. Pre-delivery or antenatal care (ANC) examination - In the form of a package with a maximum of 4 visits worth IDR 200,000. - ANC checks that are not only carried out in one place are worth IDR 50,000 per visit. 2. Normal delivery or vaginal delivery - Normal delivery performed by a midwife, worth IDR 700,000. - Normal delivery performed by a doctor, worth IDR 800,000. - Normal delivery with basic emergency measures at the Puskesmas is covered by Rp. 950,000. 3. Deliveries referred to advanced-level health facilities Under certain conditions, pregnant women participating in JKN who cannot give birth typically, and must be referred to help through a cesarean section due to limited experts and medical equipment, can be covered by JKN. If you still want to ask further, please get in touch with the midwife. |
| A45 | If so, this is normal in the 3rd trimester due to the enlargement of the uterus. Regular exercise is a critical component of lifestyle interventions recommended for pregnant women as part of the ANC to prevent excessive weight gain during pregnancy. Regular exercise is an essential component of lifestyle interventions recommended for pregnant women as part of the ANC to avoid excessive weight gain during pregnancy. Pregnant women with low back and pelvic pain usually improve within a few months after birth (WHO, 2016). |
| A46 | Please continue to the other question. |
| A47 | If so, this is normal in the 3rd trimester of pregnant women due to pressure on the bladder from the enlargement of the uterus. |
| A48 | Please continue to the other question. |
| A49 | If so, these are signs of labor. Immediately prepare for the delivery process and go to the intended delivery service: => and chat midwife. |
| A50 | Please continue to other questions. |
| A51 | If not, please take a break and if the complaint continues, contact the midwife. Dizziness in pregnancy is a complaint that often occurs because changes in pregnancy hormones make blood vessels dilate. Dizziness in pregnancy is expected, but it is advisable to remain vigilant if dizziness is accompanied by other symptoms, such as blurred vision, abdominal pain, difficulty speaking, chest pain, tingling, rapid pulse, or vaginal bleeding. |
| A52 | If not, please take a break and if the complaint continues, contact the midwife. |
| A53 | If so, this is a sign of immediate danger to health workers. Chat to a midwife. |
| A54 | If not, please take a break and if the complaint continues, contact the midwife. |
| A55 | Please continue to the other question. |
| A56 | This is a sign of danger. Seek medical attention immediately. The reduced movement of the baby is one thing that needs to be watched out for directly by the health workers. => Chat Midwife. |
| A57 | This is a sign of danger. Seek medical attention immediately. Chat to a midwife. |
| A58 | Leg cramps usually occur twice a week or less frequently, usually at night, last a few seconds to a few minutes, and mostly go away on their own. Leg cramps occur in about 50% of pregnant women and subside after delivery. The mechanism of cramping is unknown and may be idiopathic. However, it could be due to physiological changes in neuromuscular performance, weight gain, joint weakness in the later stages of pregnancy, the insufficient blood supply to lower body organs, and increased pressure on the leg muscles during pregnancy. Pressure on the blood vessels and nerves due to an enlarged uterus, an imbalance between the intake and output of electrolytes and vitamins, and insufficient information on minerals may be other reasons for cramps (Mandouri, 2017). |
| A59 | Please continue to other questions. |
| A60 | If yes, this reflects an awareness that the pregnancy is nearing the end, so there is a fear of an abnormal delivery process, anxiety about whether the baby can be delivered safely, and worry if the baby is born in an abnormal condition. Do exercise, mindfulness, and relaxation (prenatal yoga). Physiological relaxation exercises will cause a relaxing effect that involves the parasympathetic nerves in the central nervous system, where one of the functions of the parasympathetic nerves is to reduce the production of the hormone adrenaline or epinephrine (stress hormone) and increase the secretion of the hormone noradrenaline or norepinephrine (relaxing hormone) so that there is a decrease in anxiety and tension in pregnant women, which causes them to become more relaxed and calmer (Davenport, 2007) => chat to a midwife. |
| A61 | Please consult the midwife => and chat midwife. |
| A62 | Please continue to the next question. |
| A63 | 1st trimester: 1 visit at 0–13 weeks of gestation 2nd trimester: 1 visit at 14–28 weeks of gestation 3rd trimester: 2 trips at 28–36 weeks of pregnancy and 36–40 weeks. Every pregnant woman is advised to have a comprehensive and quality antenatal visit at least four times, i.e., once before the 4th month of pregnancy, then around the 6th month of pregnancy, and two times around the 8th and 9th month of pregnancy. The minimum standard for ANC examination consists of 10 steps: 1. Weighing at each visit and recording. 2. Measuring blood pressure, usually 110/80–below 140/90. 3. Determining the value of nutritional status by measuring the upper arm circumference (LILA). 4. Determining uterine fundal height (top of the uterus): monitoring fetal development. 5. Giving TT (Tetanus Toxoid) immunization. 6. Determining fetal presentation and fetal heart rate (FHR). 7. Giving iron tablets 8. Conducting laboratory tests (syphilis, Hepatitis B and HIV). 9. Providing case management. 10. Conducting interviews (counseling), including planning for delivery and post-delivery. If you still want to ask further, please get in touch with the midwife. |
| A64 | Please continue to the next question. |
| A65 | 1. To optimize the mental and physical health of pregnant women. 2. To detect the risk of complications in pregnancy and childbirth 3. To motivate the mother’s desire for the postpartum period and exclusive breastfeeding. If you still want to ask further, please get in touch with the midwife. |
| A66 | Please continue to the next question. |
| A67 | 1. The first visit in the 1st trimester (16 weeks) was carried out to screen and treat anemia, plan for delivery, and treat complications due to medication. 2. Visit second in the 2nd trimester (<28 weeks) was conducted for complications due to medication and medication screening for preeclampsia, Gemelli, infections of the reproductive organs, and urinary tract. 3. The third visit in the 3rd trimester (<36 weeks) and the fourth visit in the 3rd trimester (>36 weeks) were carried out to identify any abnormalities in the location and presentation, strengthen delivery plans, and recognize signs of labor. If you still want to ask further, please get in touch with the midwife. |
| A68 | Please continue to the next question. |
| A69 | Urine test 1. The urine test is essential to the 1st-trimester pregnancy check. It aims to detect a positive pregnancy and whether there are other diseases that the pregnant woman suffers from. Some of the things that have become the benchmark for urine tests are: 1. The protein and sugar levels in pregnant women’s urine tend to be low. In addition, the urine of pregnant women also contains the hormone HCG (Human Chorionic Gonadotropin) at relatively high levels. 2. If the urine contains high levels of ketones and sugar, the pregnant woman has gestational diabetes. 3. Proteins in pregnant women signify that the mother has pre-eclampsia or certain bacterial infections. Blood Test 1. Determination of blood type, whether the mother’s blood type is A, B, AB, or O. 2. Determination of rhesus blood, whether rhesus positive or negative. This rhesus examination is essential and will later be matched with the baby’s rhesus. The sign is standard if the mother and baby have the same rhesus. However, suppose the mother’s rhesus is different from the baby’s. If the mother is rhesus positive and the baby is rhesus negative, the baby will suffer from blood disorders. 3. Check hemoglobin. It is also important to detect whether the mother has anemia. Pregnant women have hemoglobin levels of about 10–16 g per liter in their blood. 4. Hepatitis B and C examination is to determine whether there is a viral infection in the mother’s liver or not. A pregnant woman with hepatitis is at risk of passing the disease on to her fetus. 5. Examination for rubella, a measles disease in which the mother’s body develops a red rash. This disease is a risk for mothers under five months of gestational age. Generally, the rubella virus is transmitted through sneezing, saliva, and coughing by the sufferer. Ultrasound test (ultrasonography) An examination that doctors offer to pregnant women is an ultrasound test. Moreover, today’s technology is very sophisticated. This makes it possible to detect the fetus from an early age (first trimester). This ultrasound test has many uses, including: 1. Observing the structure of the fetus in the stomach 2. Checking the normal condition of the uterus, placenta, and amniotic fluid 3. Observing the growth of the fetus 4. Estimating gestational age 5. Detecting the presence or absence of abnormalities or physical defects in the fetus Triple Elimination Check Laboratory personnel carries out a capillary blood examination to determine the results of HIV, syphilis, and hepatitis tests. Reasons to do a triple elimination check: 1. Stopping the growth of HIV, syphilis, and hepatitis B in the bod 2. Protecting sexual partner from the transmission of HIV, syphilis, and hepatitis B 3. Having children who are free from HIV, syphilis, and hepatitis B If you still want to ask further, don’t hesitate to get in touch with the midwife. |
| A70 | Please continue to the next question. |
| A71 | To receive Indonesian National Health Insurance (JKN), please register first. During pregnancy, management JKN can cover 3 services, divided into: - Trimester 1: carried out once at 1–12 weeks of pregnancy - Trimester 2: carried out once at 13–28 weeks of pregnancy - Trimester 3: carried two times at 29–40 weeks of pregnancy JKN can cover the cost of ultrasonography services when pregnant women are referred by a First Level Health Facility (FKTP. The cost of pregnancy checks borne by JKN: 1. Pre-delivery or antenatal care (ANC) examination - In the form of a package with a maximum of 4 visits, worth IDR 200,000. - ANC checks that are not only carried out in one place are worth IDR 50,000 per visit. 2. Normal delivery or vaginal delivery - Normal delivery performed by a midwife, worth IDR 700,000. - Normal delivery performed by a doctor, worth IDR 800,000. - Normal delivery with basic emergency measures at the puskesmas is covered by Rp. 950,000. 3. Deliveries referred to advanced-level health facilities Under certain conditions, pregnant women participating in JKN who cannot give birth typically, and must be referred to help through a cesarean section due to limited experts and medical equipment, can be covered by JKN. If you still want to ask further, please get in touch with the midwife. |
References
- Mosa, M.; Yoo, I.; Sheets, L. A systematic review of healthcare applications for smartphones. BMC Med. Inform. Decis. Mak. 2012, 12, 67. [Google Scholar] [CrossRef] [PubMed]
- Ernsting, C.; Dombrowski, S.U.; Oedekoven, M.; O’Sullivan, J.L.; Kanzler, E.; Kuhlmey, A.; Gellert, P. Using smartphones and health apps to change and manage health behaviors: A population-based survey. J. Med. Internet Res. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. mHealth: New horizons for health through mobile technologies. Observatory 2011, 3, 66–71. [Google Scholar] [CrossRef]
- Iyawa, G.E.; Hamunyela, S. MHealth Apps and Services for Maternal Healthcare in Developing Countries. In Proceedings of the 2019 IST-Africa Week Conference, IST-Africa 2019, Nairobi, Kenya, 8–10 May 2019. [Google Scholar] [CrossRef]
- BPS-Statistics Indonesia. Telecommunication Statistics In Indonesia 2020. BPS-Statistics Indonesia. 2020. Available online: https://www.bps.go.id/publication/2021/10/11/e03aca1e6ae93396ee660328/statistik-telekomunikasi-indonesia-2020.html (accessed on 18 August 2022).
- Zhang, P.; Dong, L.; Chen, H.; Chai, Y.; Liu, J. The rise and need for mobile apps for maternal and child health care in China: Survey based on app markets. JMIR Mhealth Uhealth 2018, 6, e9302. [Google Scholar] [CrossRef] [PubMed]
- Kusyanti, T.; Wirakusumah, F.F.; Rinawan, F.R.; Muhith, A. Technology-Based (Mhealth) and Standard/Traditional Maternal Care for Pregnant Woman: A Systematic Literature Review. Healthcare 2022, 10, 1287. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.S.L.; Goonawardene, N. Internet health information seeking and the patient-physician relationship: A systematic review. J. Med. Internet Res. 2017, 19, e5729. [Google Scholar] [CrossRef] [PubMed]
- Health Ministry of Republic Indonesia. Indonesia Health Profil 2020. 2021. Available online: https://www.kemkes.go.id/folder/view/01/structure-publikasi-pusdatin-profil-kesehatan.html (accessed on 7 February 2022).
- Jokowi. Presidential Decree No. 18 Year of 2020. National Mid-Term Development Plan 2015–2019. 2020, pp. 1–300. Available online: https://peraturan.bpk.go.id/Home/Details/131386/perpres-no-18-tahun-2020 (accessed on 10 June 2022).
- Soedirham, O. Integrated Services Post (Posyandu) as Sociocultural Approach for Primary Health Care Issue. Kesmas Natl. Public Health J. 2012, 7, 195. [Google Scholar] [CrossRef]
- Rinawan, F.R.; Susanti, A.I.; Amelia, I.; Ardisasmita, M.N.; Dewi, R.K.; Ferdian, D.; Purnama, W.S.; Purbasari, A. Understanding mobile application development and implementation for monitoring Posyandu data in Indonesia: A 3-year hybrid action study to build “ a bridge ” from the community to the national scale. BMJ Public Health 2021, 21, 1024. [Google Scholar] [CrossRef]
- Rinawan, F.R.; Faza, A.; Susanti, A.I.; Purnama, W.G.; Indraswari, N.; Ferdian, D.; Fatimah, S.N.; Purbasari, A.; Zulianto, A.; Sari, A.N.; et al. Posyandu Application for Monitoring Children Under-Five: A 3-Year Data Quality Map in Indonesia. ISPRS Int. J. Geo-Inf. 2022, 11, 399. [Google Scholar] [CrossRef]
- Stellata, A.G.; Rinawan, F.R.; Nyarumenteng, G.; Winarno, A.; Susanti, A.I.; Purnama, W.G. Exploration of Telemidwifery: An Initiation of Application Menu in Indonesia. Int. J. Environ. Res. Public Health 2022, 19, 10713. [Google Scholar] [CrossRef]
- Baudier, P.; Kondrateva, G.; Ammi, C.; Chang, V.; Schiavone, F. Patients’ perceptions of teleconsultation during COVID-19: A cross-national study. Technol. Forecast. Soc. Chang. 2021, 163, 120510. [Google Scholar] [CrossRef] [PubMed]
- Palanica, A.; Flaschner, P.; Thommandram, A.; Li, M.; Fossat, Y. Physicians’ perceptions of chatbots in health care: Cross-sectional web-based survey. J. Med. Internet Res. 2019, 21, e12887. [Google Scholar] [CrossRef] [PubMed]
- Adamopoulou, E.; Moussiades, L. An Overview of Chatbot Technology. In IFIP International Conference on Artificial Intelligence Applications and Innovations; Springer: Cham, Switzerland, 2020; Volume 584. [Google Scholar] [CrossRef]
- Car, L.T.; Dhinagaran, D.A.; Kyaw, B.M.; Kowatsch, T.; Joty, S.; Theng, Y.L.; Atun, R. Conversational Agents in Health Care: Scoping Review and Conceptual Analysis. J. Med. Internet Res. 2020, 22, e17158. [Google Scholar] [CrossRef]
- Abd-Alrazaq, A.A.; Rababeh, A.; Alajlani, M.; Bewick, B.M.; Househ, M. Effectiveness and safety of using chatbots to improve mental health: Systematic review and meta-analysis. J. Med. Internet Res. 2020, 22, e16021. [Google Scholar] [CrossRef]
- Oh, Y.J.; Zhang, J.; Fang, M.L.; Fukuoka, Y. A systematic review of artificial intelligence chatbots for promoting physical activity, healthy diet, and weight loss. International. J. Behav. Nutr. Phys. Act. 2021, 18, 160. [Google Scholar] [CrossRef]
- Schachner, T.; Keller, R.; Wangenheim, F. Artificial intelligence-based conversational agents for chronic conditions: Systematic literature review. J. Med. Internet Res. 2020, 22, e20701. [Google Scholar] [CrossRef]
- Okonkwo, C.W.; Ade-Ibijola, A. Chatbots applications in education: A systematic review. Comput. Educ. Artif. Intell. 2021, 2, 100033. [Google Scholar] [CrossRef]
- Fan, X.; Chao, D.; Zhang, Z.; Wang, D.; Li, X.; Tian, F. Utilization of self-diagnosis health chatbots in real-world settings: Case study. J. Med. Internet Res. 2021, 23, 9–12. [Google Scholar] [CrossRef]
- Alaaeldin, R.; Asfoura, E.; Abdel-Haq, M.S. Developing Chatbot System To Support Decision Making Based on Big Data Analytics. J. Manag. Inf. Decis. Sci. 2021, 24, 1–15. [Google Scholar]
- Chung, K.; Cho, H.Y.; Park, J.Y. A chatbot for perinatal women’s and partner’s obstetric and mental health care: Development and usability evaluation study. JMIR Med. Inform. 2021, 9, e18607. [Google Scholar] [CrossRef]
- Farao, J.; Malila, B.; Conrad, N.; Mutsvangwa, T.; Rangaka, M.X.; Douglas, T.S. A user-centred design framework for mHealth. PLoS ONE 2020, 15, e0237910. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Gómez, E.; Martín-Salvador, A.; Luque-Vara, T.; Sánchez-Ojeda, M.A.; Navarro-Prado, S.; Enrique-Mirón, C. Content validation through expert judgment of an instrument on the nutritional knowledge, beliefs, and habits of pregnant women. Nutrients 2020, 12, 1136. [Google Scholar] [CrossRef] [PubMed]
- Brnabic, A.; Hess, L.M. Systematic literature review of machine learning methods used in the analysis of real-world data for patient-provider decision making. BMC Med. Inform. Decis. Mak. 2021, 21, 54. [Google Scholar] [CrossRef] [PubMed]
- Podgorelec, V.; Kokol, P.; Stiglic, B.; Rozman, I. Decision Trees: An Overview and Their Use in Medicine. J. Med. Syst. 2002, 103, 239–248. [Google Scholar] [CrossRef]
- Li, H.; Wu, T.T.; Yang, D.L.; Guo, Y.S.; Liu, P.C.; Chen, Y.; Xiao, L.P. Decision tree model for predicting in-hospital cardiac arrest among patients admitted with acute coronary syndrome. Clin. Cardiol. 2019, 42, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.Y.; Lu, Y. Decision tree methods: Applications for classification and prediction. Shanghai Arch. Psychiatry 2015, 27, 130–135. [Google Scholar] [CrossRef]
- Wang, B.; He, Z.; Yi, Z.; Yuan, C.; Suo, W.; Pei, S.; Li, Y.; Ma, H.; Wang, H.; Xu, B.; et al. Application of a decision tree model in the early identification of severe patients with severe fever with thrombocytopenia syndrome. PLoS ONE 2021, 16, e0255033. [Google Scholar] [CrossRef] [PubMed]
- Chern, C.C.; Chen, Y.J.; Hsiao, B. Decision tree-based classifier in providing telehealth service. BMC Med. Inform. Decis. Mak. 2019, 19, 104. [Google Scholar] [CrossRef]
- Chang, C.C.; Yeh, J.H.; Chiu, H.C.; Chen, Y.M.; Jhou, M.J.; Liu, T.C.; Lu, C.J. Utilization of Decision Tree Algorithms for Supporting the Prediction of Intensive Care Unit Admission of Myasthenia Gravis: A Machine Learning-Based Approach. J. Pers. Med. 2022, 12, 32. [Google Scholar] [CrossRef]
- Bae, J.-M. Clinical Decision Analysis using Decision Tree. Epidemiol. Health 2014, 36, e2014025. [Google Scholar] [CrossRef]
- Patel, H.H.; Prajapati, P. Study and Analysis of Decision Tree Based Classification Algorithms. Int. J. Comput. Sci. Eng. 2018, 6, 74–78. [Google Scholar] [CrossRef]
- Bhirud, N.; Tataale, S.; Randive, S.; Nahar, S. A Literature Review On Chatbots In Healthcare Domain. Int. J. Sci. Technol. Res. 2019, 8, 225–231. [Google Scholar]
- Park, E.Y.; Yi, M.; Kim, H.S.; Kim, H. A decision tree model for breast reconstruction of women with breast cancer: A mixed method approach. Int. J. Environ. Res. Public Health 2021, 18, 3579. [Google Scholar] [CrossRef] [PubMed]
- Siddique, S.; Chow, J.C.L. Machine Learning in Healthcare Communication. Encyclopedia 2021, 1, 21. [Google Scholar] [CrossRef]
- Parviainen, J.; Rantala, J. Chatbot breakthrough in the 2020s ? An ethical reflection on the trend of automated consultations in health care. Med. Health Care Philos. 2021, 25, 61–71. [Google Scholar] [CrossRef]
- Nadarzynski, T.; Miles, O.; Cowie, A.; Ridge, D. Acceptability of artificial intelligence (AI)-led chatbot services in healthcare: A mixed-methods study. Digit. Health 2019, 5, 2055207619871808. [Google Scholar] [CrossRef]
- Miles, O.; West, R.; Nadarzynski, T. Health chatbots acceptability moderated by perceived stigma and severity: A cross-sectional survey. Digit. Health 2021, 7, 20552076211063012. [Google Scholar] [CrossRef]
- Jovanovic, M.; Baez, M.; Casati, F. Chatbots as Conversational Healthcare Services. IEEE Internet Comput. 2021, 25, 44–51. [Google Scholar] [CrossRef]
- Laranjo, L.; Dunn, A.G.; Tong, H.L.; Kocaballi, A.B.; Chen, J.; Bashir, R.; Surian, D.; Gallego, B.; Magrabi, F.; Lau, A.Y.S.; et al. Conversational agents in healthcare: A systematic review. J. Am. Med. Inform. Assoc. 2018, 25, 1248–1258. [Google Scholar] [CrossRef]
- Moser, A.; Korstjens, I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. Eur. J. Gen. Pract. 2018, 24, 9–18. [Google Scholar] [CrossRef]
- Nyumba, T.O.; Wilson, K.; Derrick, C.J.; Mukherjee, N. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods Ecol. Evol. 2018, 9, 20–32. [Google Scholar] [CrossRef]
- Cunningham, F.G. Williams Obstetrics, 25th ed.; McGraw-Hill: New York, NY, USA, 2018. [Google Scholar]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Creswell, J.D. Research Design, 5th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Haji Ali Afzali, H.; Karnon, J. Specification and Implementation of Decision Analytic Model Structures for Economic Evaluation of Health Care Technologies. In Encyclopedia of Health Economics; Elsevier: Amsterdam, The Netherlands, 2014; pp. 340–347. [Google Scholar] [CrossRef]
- Anderson, K.; Burford, O.; Emmerton, L. Mobile health apps to facilitate self-care: A qualitative study of user experiences. PLoS ONE 2016, 11, 1–21. [Google Scholar] [CrossRef]
- Binyamin, S.S. Proposing a mobile apps acceptance model for users in the health area : A systematic literature review and meta-analysis. Health Inform. J. 2021, 27, 1460458220976737. [Google Scholar] [CrossRef] [PubMed]
- Luca, E.J.; Ulyannikova, Y. Towards a User-Centred Systematic Review Service: The Transformative Power of Service Design Thinking. J. Aust. Libr. Inf. Assoc. 2020, 69, 357–374. [Google Scholar] [CrossRef]
- Bueno, M.; Stevens, B.; Rao, M.; Riahi, S.; Lanese, A.; Li, S. Usability, acceptability, and feasibility of the Implementation of Infant Pain Practice Change (ImPaC) Resource. Paediatr. Neonatal Pain 2020, 2, 82–92. [Google Scholar] [CrossRef]
- Alqudah, A.A.; Al-Emran, M. applied sciences Technology Acceptance in Healthcare: A Systematic Review. Appl. Sci. 2021, 11, 10537. [Google Scholar] [CrossRef]
- Pais, S.; Petrova, K.; Parry, D. Enhancing system acceptance through user-centred design: Integrating patient generated wellness data. Sensors 2022, 22, 45. [Google Scholar] [CrossRef]
- Kaur, A.; Singh, S.; Chandan, J.S.; Robbins, T.; Patel, V. Qualitative exploration of digital chatbot use in medical education: A pilot study. Digit. Health 2021, 7, 20552076211038151. [Google Scholar] [CrossRef]
- Arefyev, A.; Lechauve, J.-B.; Gay, C.; Gerbaud, L.; Chérillat, M.S.; Figueiredo, I.T.; Plan-Paquet, A.; Coudeyre, E. Mobile application development through qualitative research in education program for chronic low back patients. Ann. Phys. Rehabil. Med. 2017, 60, e102–e103. [Google Scholar] [CrossRef]
- Kowatsch, T.; Otto, L.; Harperink, S.; Cotti, A.; Schlieter, H. A design and evaluation framework for digital health interventions. IT-Inf. Technol. 2019, 61, 253–263. [Google Scholar] [CrossRef]
- Zhou, L.; Bao, J.; Setiawan, I.M.A.; Saptono, A.; Parmanto, B. The mhealth app usability questionnaire (MAUQ): Development and validation study. JMIR Mhealth Uhealth 2019, 7, e11500. [Google Scholar] [CrossRef] [PubMed]
- Mokmin, N.A.M.; Ibrahim, N.A. The evaluation of chatbot as a tool for health literacy education among undergraduate students. Educ. Inf. Technol. 2021, 26, 6033–6049. [Google Scholar] [CrossRef] [PubMed]
- Ngo, E.; Truong, M.B.T.; Nordeng, H. Use of decision support tools to empower pregnant women: Systematic review. J. Med. Internet Res. 2020, 22, e19436. [Google Scholar] [CrossRef]
- Masoi, T.J.; Kibusi, S.M. Improving pregnant women’s knowledge on danger signs and birth preparedness practices using an interactive mobile messaging alert system in Dodoma region, Tanzania: A controlled quasi experimental study. Reprod. Health 2019, 16, 177. [Google Scholar] [CrossRef]
- Dennis, C.L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef]
- Pereira, J. Using Health Chatbots for Behavior Change : A Mapping Study. J. Med. Syst. 2019, 43, 135. [Google Scholar] [CrossRef]
- Boucher, E.M.; Harake, N.R.; Ward, H.E.; Stoeckl, S.E.; Vargas, J.; Minkel, J.; Parks, A.C.; Zilca, R. Artificially intelligent chatbots in digital mental health interventions: A review. Expert Rev. Med. Devices 2021, 18, 37–49. [Google Scholar] [CrossRef]
- Vaidyam, A.N.; Wisniewski, H.; Halamka, J.D.; Kashavan, M.S.; Torous, J.B. Chatbots and Conversational Agents in Mental Health: A Review of the Psychiatric Landscape. Can. J. Psychiatry 2019, 64, 456–464. [Google Scholar] [CrossRef]
- Ye, B.J.; Kim, J.Y.; Suh, C.; Choi, S.P.; Choi, M.; Kim, D.H.; Son, B.C. Development of a Chatbot Program for Follow-Up Management of Workers’ General Health Examinations in Korea : A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 2170. [Google Scholar] [CrossRef]
- Liu, H.; Peng, H.; Song, X.; Xu, C.; Zhang, M. Using AI chatbots to provide self-help depression interventions for university students: A randomized trial of effectiveness. Internet Interv. 2022, 27, 100495. [Google Scholar] [CrossRef] [PubMed]
- Kretzschmar, K.; Tyroll, H.; Pavarini, G. Can Your Phone Be Your Therapist ? Young People ’ s Ethical Perspectives on the Use of Fully Automated Conversational Agents (Chatbots) in Mental Health Support. Biomed. Inform. Insights 2019, 11, 1178222619829083. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Le, J.H.; Vittinghoff, E.; Fukuoka, Y. mHealth Physical Activity Intervention: A Randomized Pilot Study in Physically Inactive Pregnant Women. Matern. Child Health J. 2016, 20, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Morris, T.; Strömmer, S.; Vogel, C.; Harvey, N.C.; Cooper, C.; Inskip, H.; Woods-Townsend, K.; Baird, J.; Barker, M.; Lawrence, W.; et al. Improving pregnant women’s diet and physical activity behaviours: The emergent role of health identity. BMC Pregnancy Childbirth 2020, 20, 244. [Google Scholar] [CrossRef] [PubMed]
- Avila-Tomas, J.F.; Olano-Espinosa, E.; Minué-Lorenzo, C.; Martinez-Suberbiola, F.J.; Matilla-Pardo, B.; Serrano-Serrano, M.E.; Escortell-Mayor, E.; the Group Dej@lo. Effectiveness of a chat-bot for the adult population to quit smoking: Protocol of a pragmatic clinical trial in primary care (Dejal@). BMC Med. Inform. Decis. Mak. 2019, 19, 249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Oh, Y.J.; Lange, P.; Yu, Z.; Fukuoka, Y. Artificial intelligence chatbot behavior change model for designing artificial intelligence chatbots to promote physical activity and a healthy diet: Viewpoint. J. Med. Internet Res. 2020, 22, e22845. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Decary, M. Artificial intelligence in healthcare : An essential guide for health leaders. Healthc. Manag. Forum. 2020, 33, 10–18. [Google Scholar] [CrossRef]
- Greene, A.; Greene, C.C.; Greene, C. Artificial intelligence, chatbots, and the future of medicine. Lancet Oncol. 2019, 20, 481–482. [Google Scholar] [CrossRef]
- Zhang, M.; Zhu, B.; Yuan, C.; Zhao, C.; Wang, J.; Ruan, Q.; Han, C.; Bao, Z.; Chen, J.; Arceneaux, K.; et al. A parsimonious approach for screening moderate-to-profound hearing loss in a community-dwelling geriatric population based on a decision tree analysis. BMC Geriatr. 2019, 19, 693. [Google Scholar] [CrossRef]
- Chen, L.; Miao, M. Application of Decision Tree Intelligent Algorithm in Data Analysis of Physical Health Test. J. Healthc. Eng. 2022, 2022, 8584377. [Google Scholar] [CrossRef]
- Rokach, L.; Maimon, O. Data Mining With Decision Trees. In Proactive Data Mining with Decision Trees; Springer: New York, NY, USA, 2014; Volume 7. [Google Scholar]
- Al-Ajlan, A. The Comparison between Forward and Backward Chaining. Int. J. Mach. Learn. Comput. 2015, 5, 106–113. [Google Scholar] [CrossRef]
- Prambudi, D.A.; Widodo, C.E.; Widodo, A.P. Expert System Application of Forward Chaining and Certainty Factors Method for the Decision of Contraception Tools. In E3S Web of Conferences; EDP Sciences: Les Ulis, France, 2018; Volume 31. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).