
Pulmonary Vein Stenosis Associated with Germline PIK3CA Mutation


Abstract
:1. Introduction
2. Case Presentation

{kind=link}
{kind=link}
{kind=link}
| General | |
|---|---|
| Body weight | 4.8 kg |
| Age | 2 months |
| Sex | Female |
| Ethnicity | Asian (Korean) |
| Echocardiogram | |
| Pulmonary vein gradient | 5.6 mmHg |
| RV | Dilated with normal systolic function |
| LV | Normal size and function |
| TR gradient | 3.9 m/s TR jet in setting of large VSD |
| Interventricular septal position | Flattened |
| Atria | Normal size |
| Electrocardiogram | |
| Rhythm | Normal sinus rhythm |
| Heart rate | 146 per minute |
| QRS duration | 70 ms |
| PR interval | 100 ms |
| QTc interval | 451 ms |
| T wave | Normal |

3. Discussion
3.1. Case Discussion
3.2. PIK3CA
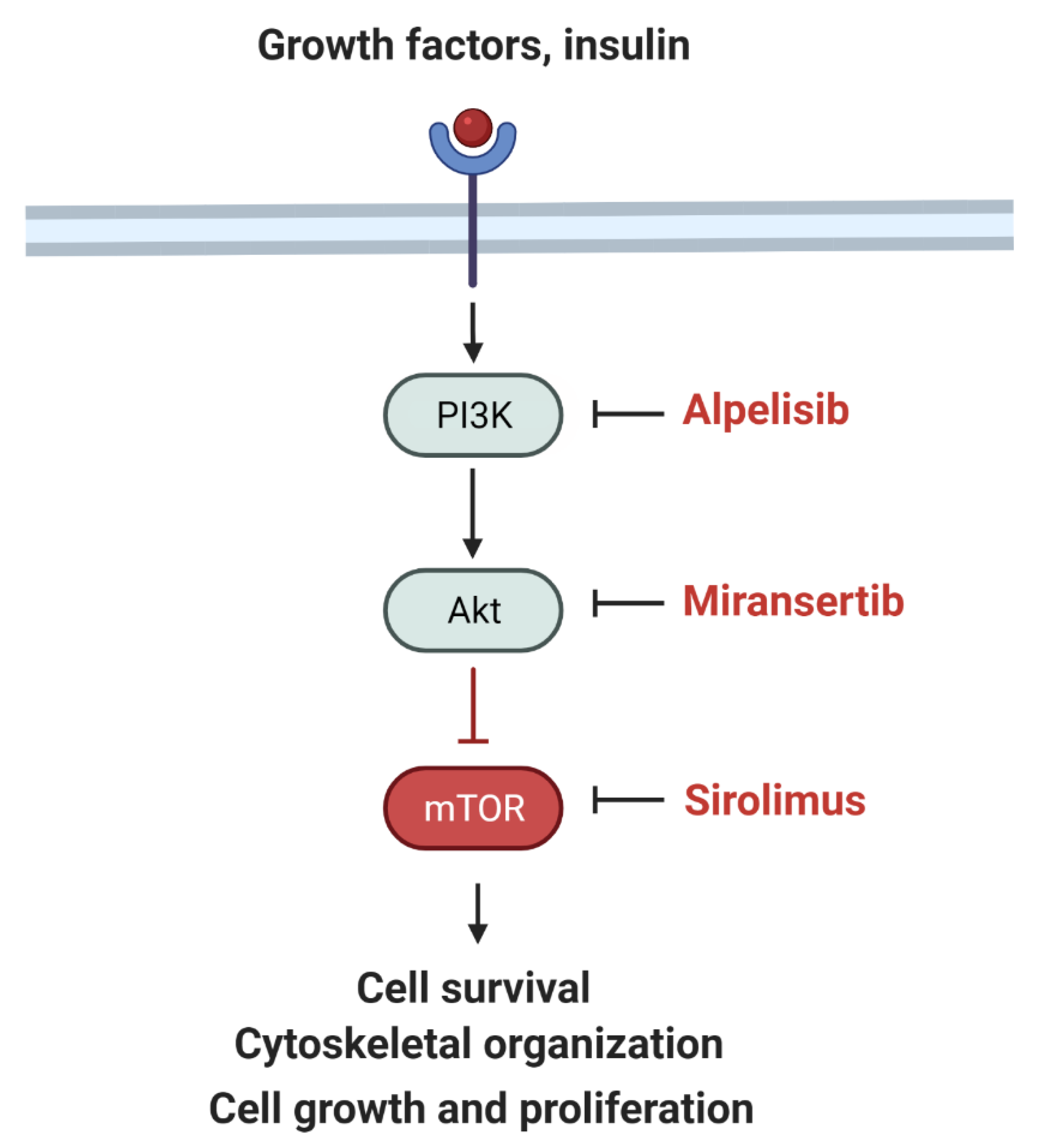
3.2.1. PI3K–AKT–mTOR Signaling Pathway
3.2.2. PIK3CA Mutations and Clinical Phenotypes
3.3. Alpelisib
3.4. Future Directions
4. Conclusions
- Main concern: PVS is a rare and frequently lethal childhood disease with few known genetic associations or treatments.
- Main discovery: We present a patient with PVS and a PIK3CA mutation, who demonstrated a good response to the targeted inhibitor, alpelisib.
- Main take-home message: Future patients with PVS may benefit from further research with whole exome sequencing and alpelisib therapy.
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Drossner, D.M.; Kim, D.W.; Maher, K.O.; Mahle, W.T. Pulmonary vein stenosis: Prematurity and associated conditions. Pediatrics 2008, 122, e656–e661. [Google Scholar] [CrossRef] [PubMed]
- Backes, C.H.; Nealon, E.; Armstrong, A.K.; Cua, C.L.; Mitchell, C.; Krishnan, U.; Vanderlaan, R.D.; Song, M.K.; Viola, N.; Smith, C.V.; et al. Pulmonary Vein Stenosis in Infants: A Systematic Review, Meta-Analysis, and Meta-Regression. J. Pediatr. 2018, 198, 36–45.e33. [Google Scholar] [CrossRef] [PubMed]
- Frank, D.B.; Levy, P.T.; Stiver, C.A.; Boe, B.A.; Baird, C.W.; Callahan, R.M.; Smith, C.V.; Vanderlaan, R.D.; Backes, C.H. Primary pulmonary vein stenosis during infancy: State of the art review. J. Perinatol. 2021, 41, 1528–1539. [Google Scholar] [CrossRef] [PubMed]
- Latson, L.A.; Prieto, L.R. Congenital and acquired pulmonary vein stenosis. Circulation 2007, 115, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, A.H.; Yamada, J.M.; Miller, D.T.; McEnaney, K.; Ireland, C.; Roberts, A.E.; Gauvreau, K.; Jenkins, K.J.; Chen, M.H. Clinical Syndromic Phenotypes and the Potential Role of Genetics in Pulmonary Vein Stenosis. Children 2021, 8, 128. [Google Scholar] [CrossRef]
- Breinholt, J.P.; Hawkins, J.A.; Minich, L.A.; Tani, L.Y.; Orsmond, G.S.; Ritter, S.; Shaddy, R.E. Pulmonary vein stenosis with normal connection: Associated cardiac abnormalities and variable outcome. Ann. Thorac. Surg. 1999, 68, 164–168. [Google Scholar] [CrossRef]
- Pogoriler, J.E.; Kulik, T.J.; Casey, A.M.; Baird, C.W.; Mullen, M.P.; Jenkins, K.J.; Vargas, S.O. Lung Pathology in Pediatric Pulmonary Vein Stenosis. Pediatr. Dev. Pathol. 2016, 19, 219–229. [Google Scholar] [CrossRef]
- Riedlinger, W.F.; Juraszek, A.L.; Jenkins, K.J.; Nugent, A.W.; Balasubramanian, S.; Calicchio, M.L.; Kieran, M.W.; Collins, T. Pulmonary vein stenosis: Expression of receptor tyrosine kinases by lesional cells. Cardiovasc. Pathol. 2006, 15, 91–99. [Google Scholar] [CrossRef]
- Kanaan, U.B.; Mahle, W.T. New Paradigms for Pulmonary Vein Stenosis Treatment: When Surgery and Transcatheter Therapy Aren’t Good Enough. J. Pediatr. 2018, 198, 12–13. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Ide, H.; Fu, Y.Y.; Teichert, A.M.; Kato, H.; Weisel, R.D.; Maynes, J.T.; Coles, J.G.; Caldarone, C.A. Losartan ameliorates “upstream” pulmonary vein vasculopathy in a piglet model of pulmonary vein stenosis. J. Thorac. Cardiovasc. Surg. 2014, 148, 2550–2557. [Google Scholar] [CrossRef] [Green Version]
- Callahan, R.; Kieran, M.W.; Baird, C.W.; Colan, S.D.; Gauvreau, K.; Ireland, C.M.; Marshall, A.C.; Sena, L.M.; Vargas, S.O.; Jenkins, K.J. Adjunct Targeted Biologic Inhibition Agents to Treat Aggressive Multivessel Intraluminal Pediatric Pulmonary Vein Stenosis. J. Pediatr. 2018, 198, 29–35.e25. [Google Scholar] [CrossRef]
- Bromberg-Marin, G.; Tsimikas, S.; Mahmud, E. Treatment of recurrent pulmonary vein stenoses with endovascular stenting and adjuvant oral sirolimus. Catheter. Cardiovasc. Interv. 2007, 69, 362–368. [Google Scholar] [CrossRef]
- Callahan, R.; Esch, J.J.; Wang, G.; Ireland, C.M.; Gauvreau, K.; Jenkins, K.J. Systemic Sirolimus to Prevent In-Stent Stenosis in Pediatric Pulmonary Vein Stenosis. Pediatr. Cardiol. 2020, 41, 282–289. [Google Scholar] [CrossRef]
- Patel, J.D.; Briones, M.; Mandhani, M.; Jones, S.; Suthar, D.; Gray, R.; Pettus, J.; McCracken, C.; Thomas, A.; Petit, C.J. Systemic Sirolimus Therapy for Infants and Children with Pulmonary Vein Stenosis. J. Am. Coll. Cardiol. 2021, 77, 2807–2818. [Google Scholar] [CrossRef]
- Choi, C.; Gauvreau, K.; Levy, P.; Callahan, R.; Jenkins, K.J.; Chen, M. Longer Exposure to Left-to-Right Shunts Is a Risk Factor for Pulmonary Vein Stenosis in Patients with Trisomy 21. Children 2021, 8, 19. [Google Scholar] [CrossRef]
- Niccum, M.; Callahan, R.; Gauvreau, K.; Jenkins, K.J. Aspiration Is Associated with Poor Treatment Response in Pediatric Pulmonary Vein Stenosis. Children 2021, 8, 783. [Google Scholar] [CrossRef]
- Manickam, K.; McClain, M.R.; Demmer, L.A.; Biswas, S.; Kearney, H.M.; Malinowski, J.; Massingham, L.J.; Miller, D.; Yu, T.W.; Hisama, F.M.; et al. Exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability: An evidence-based clinical guideline of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 2021, 23, 2029–2037. [Google Scholar] [CrossRef]
- Kuo, J.A.; Petit, C.J. Pulmonary Vein Stenosis in Children: A Programmatic Approach Employing Primary and Anatomic Therapy. Children 2021, 8, 663. [Google Scholar] [CrossRef]
- Gymnopoulos, M.; Elsliger, M.A.; Vogt, P.K. Rare cancer-specific mutations in PIK3CA show gain of function. Proc. Natl. Acad. Sci. USA 2007, 104, 5569–5574. [Google Scholar] [CrossRef] [Green Version]
- Douzgou, S.; Rawson, M.; Baselga, E.; Danielpour, M.; Faivre, L.; Kashanian, A.; Keppler-Noreuil, K.M.; Kuentz, P.; Mancini, G.M.S.; Maniere, M.C.; et al. A standard of care for individuals with PIK3CA-related disorders: An international expert consensus statement. Clin. Genet. 2022, 101, 32–47. [Google Scholar] [CrossRef]
- Keppler-Noreuil, K.M.; Rios, J.J.; Parker, V.E.; Semple, R.K.; Lindhurst, M.J.; Sapp, J.C.; Alomari, A.; Ezaki, M.; Dobyns, W.; Biesecker, L.G. PIK3CA-related overgrowth spectrum (PROS): Diagnostic and testing eligibility criteria, differential diagnosis, and evaluation. Am. J. Med. Genet. A 2015, 167a, 287–295. [Google Scholar] [CrossRef] [Green Version]
- Mirzaa, G.; Timms, A.E.; Conti, V.; Boyle, E.A.; Girisha, K.M.; Martin, B.; Kircher, M.; Olds, C.; Juusola, J.; Collins, S.; et al. PIK3CA-associated developmental disorders exhibit distinct classes of mutations with variable expression and tissue distribution. JCI Insight 2016, 1, e87623. [Google Scholar] [CrossRef] [Green Version]
- Venot, Q.; Blanc, T.; Rabia, S.H.; Berteloot, L.; Ladraa, S.; Duong, J.P.; Blanc, E.; Johnson, S.C.; Hoguin, C.; Boccara, O.; et al. Targeted therapy in patients with PIK3CA-related overgrowth syndrome. Nature 2018, 558, 540–546. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yung, D.; Freeman, K.; Mirzaa, G. Pulmonary Vein Stenosis Associated with Germline PIK3CA Mutation. Children 2022, 9, 671. https://doi.org/10.3390/children9050671
Yung D, Freeman K, Mirzaa G. Pulmonary Vein Stenosis Associated with Germline PIK3CA Mutation. Children. 2022; 9(5):671. https://doi.org/10.3390/children9050671
Chicago/Turabian StyleYung, Delphine, Kaitlyn Freeman, and Ghayda Mirzaa. 2022. "Pulmonary Vein Stenosis Associated with Germline PIK3CA Mutation" Children 9, no. 5: 671. https://doi.org/10.3390/children9050671
APA StyleYung, D., Freeman, K., & Mirzaa, G. (2022). Pulmonary Vein Stenosis Associated with Germline PIK3CA Mutation. Children, 9(5), 671. https://doi.org/10.3390/children9050671