
Exploring the Mechanisms Underlying the Effectiveness of Psychosocial Aftercare in Pediatric Chronic Pain Treatment: A Qualitative Approach




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. PAC Intervention
2.4. Data Collection
2.5. Data Analysis
2.6. Rigor
2.7. Ethical Approval
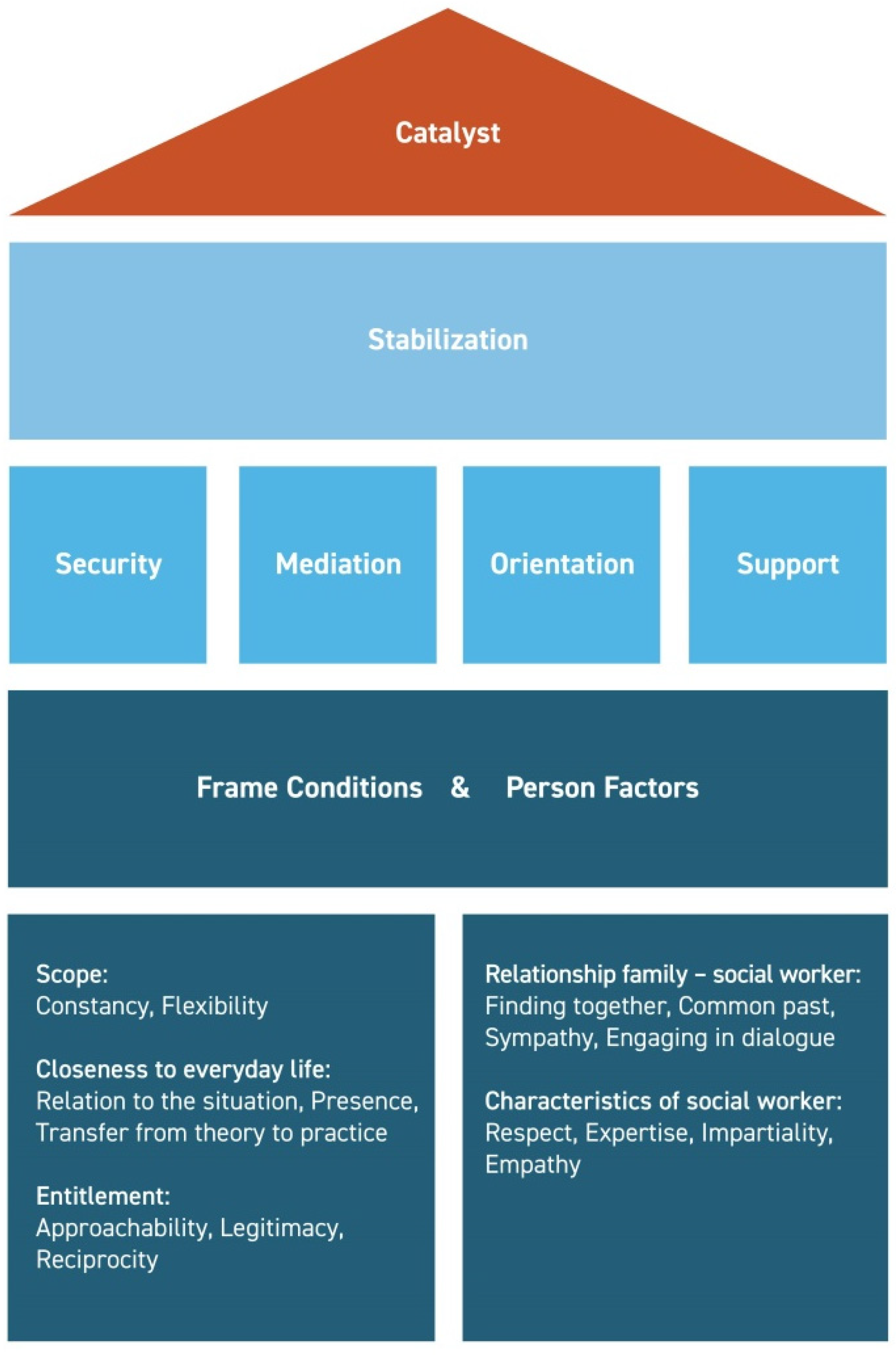
3. Results
3.1. Frame Conditions
3.2. Person Factors
3.3. Stabilization
3.3.1. Security
“We found it super positive to have this certainty that you have someone who you can ask for help. If things get worse, you are not left alone. I think, in all families, the level of stress is incredibly high when you are constantly worried about your child’s health. That doesn’t contribute to a relaxed situation at home. And just knowing that you can fall back on someone at any time—that is incredibly helpful.”(Case G—mother)
“So there was actually a situation where the pain was so bad that my mom said ‘why don’t you call the social worker?’, but I wanted to try it alone. So if it really hadn’t worked, then I definitely would have called. But I still want to try it on my own and if it really doesn’t get any better after a few hours, then I call someone.”(Case D—patient)
“Well, to know that in the back of my mind, if something is wrong, I can call her, I can get help, that’s very reassuring.”(Case E—patient)
“That’s what families tell me again and again: That it’s good to have someone to call.”(Social worker B)
3.3.2. Mediation
“Even when we had difficulties at school. Because they didn’t really want to understand what kind of illness it was. The PAC social worker supported us in talking to the school’s social worker and explaining the pain condition to him.”(Case A—mother)
“She was the only one who was up to date about how M. was feeling, how she was doing. They didn’t notice that in the pain center. She was practically the only one who noticed what had happened in the last three months since discharge. There was this third perspective.”(Case F—father)
“Well, she helped me a lot, because my parents, especially my mother, worried very much at the beginning. She always asked, ‘How are you? Are you in pain?’ Then the social worker talked to my mother on the phone and since then she has stopped asking me.”(Case D—patient)
3.3.3. Orientation
“And the whole thing caught up with me again when she got home. It was clear to me now that I was the number one contact person again. And if something happens, I have to decide what to do or how to react. Now we somehow have to keep on track ourselves. Honestly, I wouldn’t have minded if she had stayed there [on the ward] a few more weeks.”(Case G—mother)
“I thought it was good that someone was actually here again to observe our case. To check how our child had developed. I don’t think we would be as far as we are now if there hadn’t been someone pushing us in the right direction.”(Case F—father)
“Sometimes it’s just a small reassurance that makes a difference. The parents ask me: ‘I’ve sent my child to school although she was in pain. Was that OK?’ and I tell them: ‘It was OK’.”(Social worker C)
“My grandfather died recently, so I called her and we just had a chat. Actually, she always told me something that made me think; something that I hadn’t thought of before.”(Case F—patient)
3.3.4. Support
“And now I have specialized people by my side who are available to answer questions and who can give advice.”(Case C—mother)
“It’s like an anchor. Sometimes I get along well with the fact that I’m sick. And sometimes I think ‘shit’. So it’s always a constant up and down. And when you have the feeling that everything is difficult, you then have the opportunity to turn to someone who might give you a little more motivation. So I think it’s important as, how should I put it, as an anchor, as a last resort if you get stuck.”(Case F—patient)
3.4. Catalyst
“I think that for the most part, perhaps, we would have fallen back into our old behavior patterns if we hadn’t always had the opportunity to refresh and build on the things achieved during inpatient treatment. And to reflect.”(Case B—mother)
4. Discussion
4.1. Implications for Clinical Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hechler, T.; Kanstrup, M.; Holley, A.L.; Simons, L.E.; Wicksell, R.; Hirschfeld, G.; Zernikow, B. Systematic Review on Intensive Interdisciplinary Pain Treatment of Children with Chronic Pain. Pediatrics 2015, 136, 115–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odell, S.; Logan, D. Pediatric pain management: The multidisciplinary approach. J. Pain Res. 2013, 6, 785–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ospina, M.; Harstall, C. Multidisciplinary Pain Programs for Chronic Pain: Evidence from Systematic Reviews; Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2003; p. 48. [Google Scholar]
- Stahlschmidt, L.; Zernikow, B.; Wager, J. Specialized Rehabilitation Programs for Children and Adolescents with Severe Disabling Chronic Pain: Indications, Treatment and Outcomes. Children 2016, 3, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palermo, T.M.; Law, E.F.; Fales, J.; Bromberg, M.H.; Jessen-Fiddick, T.; Tai, G. Internet-delivered cognitive-behavioral treatment for adolescents with chronic pain and their parents: A randomized controlled multicenter trial. Pain 2016, 157, 174. [Google Scholar] [CrossRef] [PubMed]
- Randall, E.T.; Smith, K.R.; Conroy, C.; Smith, A.M.; Sethna, N.; Logan, D.E. Back to Living. Clin. J. Pain 2018, 34, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Zernikow, B.; Ruhe, A.-K.; Stahlschmidt, L.; Schmidt, P.; Staratzke, T.; Frosch, M.; Wager, J. Clinical and Economic Long-Term Treatment Outcome of Children and Adolescents with Disabling Chronic Pain. Pain Med. 2017, 19, 16–28. [Google Scholar] [CrossRef] [Green Version]
- Barth, F.; Wager, J.; Hübner-Möhler, B.; Zernikow, B. Therapeutische Empfehlungen in einer pädiatrischen Schmerzambulanz. Der Schmerz 2016, 30, 233–240. [Google Scholar] [CrossRef]
- Brandelli, Y.N.; Chambers, C.T.; Tutelman, P.R.; Stinson, J.N.; Huber, A.M.; Wilson, J.P. Parent Pain Cognitions and Treatment Adherence in Juvenile Idiopathic Arthritis. J. Pediatr. Psychol. 2019, 44, 1111–1119. [Google Scholar] [CrossRef]
- Porz, F.; Diedrich, M.; Bartmann, P. Familienorientierte Nachsorge bei Frühgeborenen fördert die Mutter-Kind-Interaktion und reduziert die mütterlichen Belastungen—Ergebnisse einer randomisierten Studie. Neuropediatrics 2006, 210, V11. [Google Scholar] [CrossRef]
- Podeswik, A.; Porz, F.; Groeger, K.; Thyen, U. Sozialmedizinische Nachsorge für schwer und chronisch kranke Kinder. Ergeb. Der Physiol. 2009, 157, 129–135. [Google Scholar] [CrossRef]
- Dogan, M.; Hirschfeld, G.; Blankenburg, M.; Frühwald, M.; Ahnert, R.; Braun, S.; Wager, J. Effectiveness of a Psychosocial Aftercare Program for Youth Aged 8 to 17 Years with Severe Chronic Pain: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2127024. [Google Scholar] [CrossRef] [PubMed]
- Hibbs, R.; Magill, N.; Goddard, E.; Rhind, C.; Raenker, S.; Macdonald, P.; Todd, G.; Arcelus, J.; Morgan, J.F.; Beecham, J.; et al. Clinical effectiveness of a skills training intervention for caregivers in improving patient and caregiver health following in-patient treatment for severe anorexia nervosa: Pragmatic randomised controlled trial. BJPsych Open 2015, 1, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Heijden, L.B.; Feskens, E.J.M.; Janse, A.J. Maintenance interventions for overweight or obesity in children: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 798–809. [Google Scholar] [CrossRef] [PubMed]
- Jansen, Y.J.F.M.; Foets, M.M.E.; de Bont, A.A. The contribution of qualitative research to the development of tailor-made community-based interventions in primary care: A review. Eur. J. Public Health 2010, 20, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Gough, B.; Deatrick, J.A. Qualitative health psychology research: Diversity, power, and impact. Health Psychol. 2015, 34, 289–292. [Google Scholar] [CrossRef]
- Pope, C.; Mays, N. Qualitative Research: Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ 1995, 311, 42–45. [Google Scholar] [CrossRef]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual. Res. Sport Exerc. Health 2021, 13, 201–216. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V.; Hayfield, N.; Terry, G. Thematic Analysis. In Handbook of Research Methods in Health Sciences; Springer: Singapore, 2019. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Clarke, V.; Braun, V. Thematic analysis. In Encyclopedia of Critical Psychology; Springer: New York, NY, USA, 2014; pp. 1947–1952. [Google Scholar]
- Noble, H.; Smith, J. Issues of validity and reliability in qualitative research. Évid. Based Nurs. 2015, 18, 34–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, J.; Kizito, J.; Ezumah, N.; Mangesho, P.; Allen, E.; Chandler, C. Quality assurance of qualitative research: A review of the discourse. Health Res. Policy Syst. 2011, 9, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heale, R.; Forbes, D. Understanding triangulation in research. Évid. Based Nurs. 2013, 16, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Dongen-Melman, J.E. Developing psychosocial aftercare for children surviving cancer and their families. Acta Oncol. 2000, 39, 23–31. [Google Scholar] [CrossRef]
- Mitchell, W.; Clarke, S.; Sloper, P. Care and support needs of children and young people with cancer and their parents. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2006, 15, 805–816. [Google Scholar] [CrossRef]
- Trask, E.V.; Fawley-King, K.; Garland, A.F.; Aarons, G.A. Do aftercare mental health services reduce risk of psychiatric rehospitalization for children? Psychol. Serv. 2016, 13, 127–132. [Google Scholar] [CrossRef]
- Fontanella, C.A.; Hiance-Steelesmith, D.L.; Bridge, J.A.; Lester, N.; Sweeney, H.A.; Hurst, M.; Campo, J.V. Factors Associated with Timely Follow-Up Care After Psychiatric Hospitalization for Youths with Mood Disorders. Psychiatr. Serv. 2016, 67, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Golkaramnay, V.; Bauer, S.; Haug, S.; Wolf, M.; Kordy, H. The Exploration of the Effectiveness of Group Therapy through an Internet Chat as Aftercare: A Controlled Naturalistic Study. Psychother. Psychosom. 2007, 76, 219–225. [Google Scholar] [CrossRef]
- Kaminer, Y.; Napolitano, C. Dial for Therapy: Aftercare for Adolescent Substance Use Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 1171–1174. [Google Scholar] [CrossRef]
- Kivelitz, L.; Kriston, L.; Christalle, E.; Schulz, H.; Watzke, B.; Härter, M.; Götzmann, L.; Bailer, H.; Zahn, S.; Melchior, H. Effectiveness of telephone-based aftercare case management for adult patients with unipolar depression compared to usual care: A randomized controlled trial. PLoS ONE 2017, 12, e0186967. [Google Scholar] [CrossRef] [Green Version]
- Lambert, M.J.; Barley, D.E. Research summary on the therapeutic relationship and psychotherapy outcome. Psychother. Theory Res. Pract. Train. 2001, 38, 357. [Google Scholar] [CrossRef]
- Russell, B.S.; Guite, J.W.; Homan, K.J.; Tepe, R.M.; Williams, S.E. Complementary Parent Components for Pediatric Pain Families: Innovations in Treatment. Children 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.A.; Richardson, C. Nurses’ in the multi-professional pain team: A study of attitudes, beliefs and treatment endorsements. Eur. J. Pain 2006, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Krosnick, J.A. National surveys via RDD telephone interviewing versus the Internet: Comparing sample representativeness and response quality. Public Opin. Q. 2009, 73, 641–678. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Case | Interview Partner | Sex 1 | Age 1 | Pain Location 1 | Pain Duration at IIPT Admission 1 | Mean Pain Intensity at IIPT Admission 1,2 | Mean Pain Intensity 6 Months after IIPT Discharge 1,2 | Pain-Related School Absence at IIPT Admission 3 | Pain-Related School Absence 6 Months after IIPT Discharge 3 |
|---|---|---|---|---|---|---|---|---|---|
| A | patient; mother | male | 13 | head | 2–3 years | 6 | 5 | 3 | 2 |
| B | patient; mother | female | 10 | musculoskeletal | 1–2 years | 8 | 3 | 4 | 0 |
| C | patient; mother | female | 14 | head | >3 years | 9 | 5 | 6 | 2 |
| D | patient; mother | female | 16 | musculoskeletal | >3 years | 5 | 0 | 0 | 0 |
| E | patient; mother | female | 14 | abdomen | 6–12 months | 6 | 6 | 7 | 5 |
| F | patient; mother and father | female | 16 | head | 2–3 years | 4 | 0 | 1 | 2 |
| G | mother | male | 9 | abdomen | 1–2 years | 7 | 4 | 1 | 0 |
| 1. Scope | 2. Closeness to Everyday Life | 3. Entitlement | ||||||
|---|---|---|---|---|---|---|---|---|
| Subcategories | 1.1. Constancy | 1.2. Flexibility | 2.1. Relation to the Situation | 2.2. Presence | 2.3. Transfer from Theory to Practice | 3.1. Approachability | 3.2. Legitimacy | 3.3. Reciprocity |
| Description | The structure of PAC comprises regular interpersonal contact. This results in a positively received constancy for the families. | PAC is flexible within its program structure. This enables the families to reach out to the social worker in various modalities and in needs-oriented time intervals. | In contrast to inpatient treatment, the PAC program provides help to the families’ normal everyday lives. This advantage makes it possible to refer to specific situations and give advice in practice. | After inpatient treatment, the PAC team keeps in touch with the families, e.g., via home visits. This presence is perceived as very helpful by the families. | During inpatient treatment, patients learn many techniques and coping strategies. PAC helps families with implementing those tools in everyday life. | The families are encouraged to approach the social worker whenever needed. Due to this experienced approachability, PAC can be easily incorporated in the families’ lives. | PAC is an officially established program provided to the families. Viewing the social worker as a legitimate support decreases the inhibition threshold to seek help. | During the PAC program, the social worker and the families are familiarized through consistent interaction. This is an advantage not only for the families but also for the social worker, who is enabled to increase the personalization of PAC. |
| Example | “As I do shift work, the fixed dates were quite good. [It was useful] that you could just mutually agree on the best dates.” (Case F—Mother) | “That you do not depend on appointments, but that you can simply monitor yourself; if I now notice, ‘oh, I need someone now, I have to talk to someone now’ that you then have the flexibility to say, ‘I’m not waiting until we have our appointment again next week, but I’ll just call her now’. That suits me more.” (Case E—Patient) “They have my email address. They text me or they give me a quick call and leave a voice message. I immediately call back when I’m at the office.” (Social worker A) | “Returning to everyday life, of course, you get into your old behavioral structures and your old stumbling blocks and there is this chance to observe everything close to everyday life. And everyday life, to be able to discuss it practically in parallel, that’s pretty good, I would say.” (Case F—Patient) | “There was also such a reality of life, which then became accessible to the social worker, who advised me, who supported me. It just became more alive and she could perhaps understand us differently again.” (Case G—Mother) | “The social worker reminded me again and again of the things I had learned during inpatient treatment. For example, that I should keep going to school despite of the pain.” (Case A—Patient) | “And also to teach the patient that you are not alone. ‘If you have a problem in any way, don’t be afraid to call us’. We’ve spoken to [the social worker] a few times and just talked. ‘We are there for you’. That’s a good feeling.” (Case F—Father) | “That there is the possibility that one can still contact the clinic again, that there is, so to speak, an official offer, which is accepted, I think that is great.” (Case B—Mother) | “And on the other hand, it has to be said that I thought it was quite good that the social worker also came [to my home]. So she also got an insight of how I live here.” (Case E—Patient) |
| 1. Relationship Family–Social Worker | 2. Characteristics of Social Worker | |||||||
|---|---|---|---|---|---|---|---|---|
| Sub-categories | 1.1. Finding Together | 1.2. Common Past | 1.3. Sympathy | 1.4. Engaging in Dialogue | 2.1. Respect | 2.2. Expertise | 2.3. Impartiality | 2.4. Empathy |
| Description | At the beginning of PAC, it might require some effort on the part of the social worker to win the confidence of the patients. Therefore, this first step in the PAC program needs special focus. | The fact that the social worker is part of the clinic facilitates connections with the inpatient treatment and enables families to open up more easily. | Families describe getting along well with the social worker as essential for the utilization of PAC. | Maintaining contact with each other and being able to talk about topics beyond the pain condition solidifies the relationship between the family and the social worker. | Patients, especially, emphasize the necessity of being taken seriously and of their wishes being respected. | Families express their desire for a contact who knows about their pain conditions. Furthermore, they positively perceive being able to talk to someone who is psychologically and pedagogically trained. | Families emphasize the importance of an impartial social worker during PAC, especially if they were not satisfied with inpatient treatment. | For the PAC program to be accepted by the families, the social worker needs to be sensitive to the families’ personal boundaries. |
| Example | “At the beginning I was insecure. But the social worker didn’t just say goodbye immediately after checking how I was doing now. Instead, I was encouraged to talk about my family situation, and she didn’t at all sound like she didn’t care. So the aftercare goes a bit further than inpatient treatment.” (Case F—Patient) | “I also believe that even if it is only a very small part of the common past, these four weeks that we have spent more or less together are conducive to keeping in touch later, because you shared something with each other. I think that’s what makes it work.” (Case G—Mother) | “Especially if it’s about mental health, the social worker has to be likeable; otherwise I don’t open up to a person at all.” (Case F—Mother) | “We talked about the situation with my headaches and also about my hobbies; about my everyday life. And then the better we knew each other, we also talked more about my day and about my friends. How well I got along with them and things like that. So actually, we talked about everything a little bit.” (Case C—Patient) | “The decisions have to be made together, and not like ‘we’re talking to your parents about it now, whether you agree or not’.” (Case E—Patient) | “That I have someone by my side who knows that I’m not the only child who has this pain, but also many others, and that this person also works with many children, and that they have already accompanied and helped many of them. Then you get the feeling that you are talking to someone who really understands.” (Case D—Patient) | “Over there you have the specialists of the clinic, over here you have the parents, and then the social worker joins as a third party who can describe her own impression [of the situation]. It does not have to coincide with the parents neither with the clinic, but this could then be a third perspective, a third view on things.” (Case F—Father) | “She [the social worker] always let me know when she wanted to ask questions that might have been a little more private. That’s when she said that I don’t have to give an answer, or [asked] if it was okay for me if we talked about it. And that was super pleasant. I could have said that I don’t want to talk about some things, and she would have been okay with that. So I felt super comfortable there.” (Case A—Patient) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dogan, M.; Hartenstein-Pinter, A.; Lopez Lumbi, S.; Blankenburg, M.; Frühwald, M.C.; Ahnert, R.; Braun, S.; Marschall, U.; Zernikow, B.; Wager, J. Exploring the Mechanisms Underlying the Effectiveness of Psychosocial Aftercare in Pediatric Chronic Pain Treatment: A Qualitative Approach. Children 2022, 9, 407. https://doi.org/10.3390/children9030407
Dogan M, Hartenstein-Pinter A, Lopez Lumbi S, Blankenburg M, Frühwald MC, Ahnert R, Braun S, Marschall U, Zernikow B, Wager J. Exploring the Mechanisms Underlying the Effectiveness of Psychosocial Aftercare in Pediatric Chronic Pain Treatment: A Qualitative Approach. Children. 2022; 9(3):407. https://doi.org/10.3390/children9030407
Chicago/Turabian StyleDogan, Meltem, Almut Hartenstein-Pinter, Susanne Lopez Lumbi, Markus Blankenburg, Michael C. Frühwald, Rosemarie Ahnert, Sarah Braun, Ursula Marschall, Boris Zernikow, and Julia Wager. 2022. "Exploring the Mechanisms Underlying the Effectiveness of Psychosocial Aftercare in Pediatric Chronic Pain Treatment: A Qualitative Approach" Children 9, no. 3: 407. https://doi.org/10.3390/children9030407
APA StyleDogan, M., Hartenstein-Pinter, A., Lopez Lumbi, S., Blankenburg, M., Frühwald, M. C., Ahnert, R., Braun, S., Marschall, U., Zernikow, B., & Wager, J. (2022). Exploring the Mechanisms Underlying the Effectiveness of Psychosocial Aftercare in Pediatric Chronic Pain Treatment: A Qualitative Approach. Children, 9(3), 407. https://doi.org/10.3390/children9030407