
Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
Caries Assessment
2. Materials and Methods
2.1. Focused Question
2.2. Elegibility Criteria
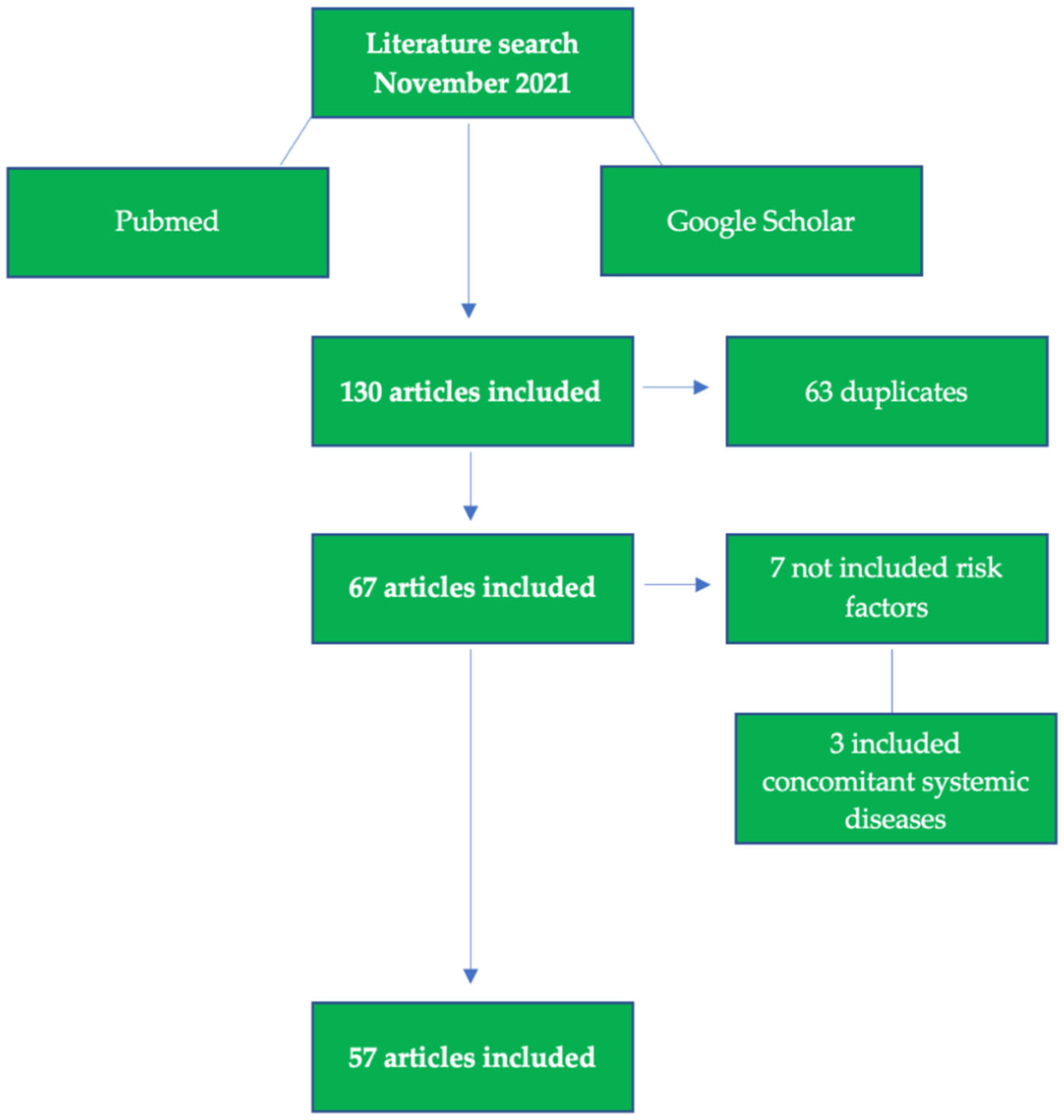
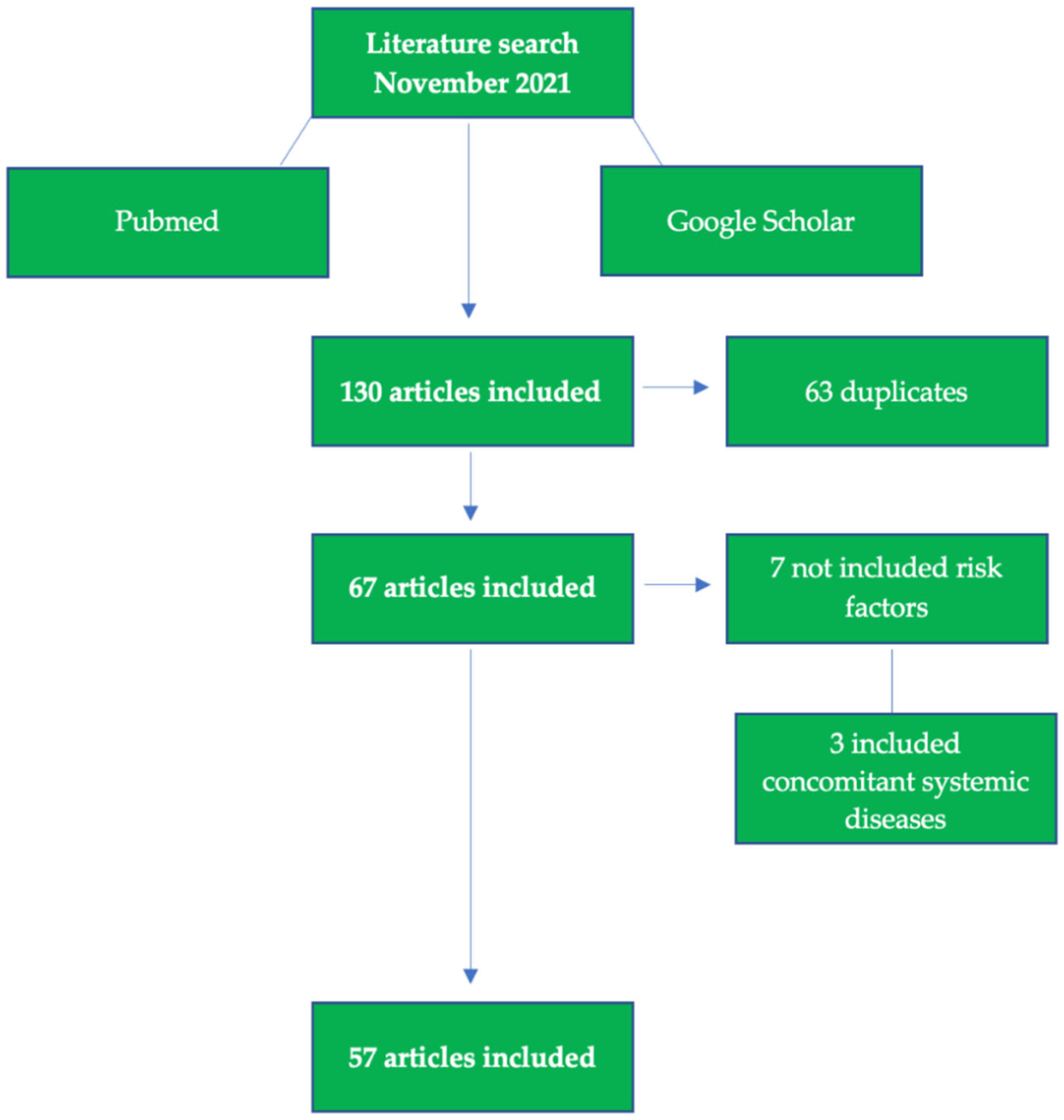
2.3. Search Strategy
2.4. Research
2.5. Screening and Selection of Articles
3. Results
4. Discussion
Possible Prevention Approches
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shaghaghian, S.; Bahmani, M.; Amin, M. Impact of oral hygiene on oral health-related quality of life of preschool children. Int. J. Dent. Hyg. 2015, 13, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Beljan, M.; Puharić, Z.; Žulec, M.; Borić, D.; Neumuller, K.R. Parent’s and Children’s Behavior and Knowledge about Oral Health. Acta Med. Croat. 2016, 70, 165–171. [Google Scholar]
- Trubey, R.J.; Moore, S.C.; Chestnutt, I.G. Children’s toothbrushing frequency: The influence of parents’ rationale for brushing, habits and family routines. Caries Res. 2015, 49, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Trubey, R.J.; Moore, S.C.; Chestnutt, I.G. The association between parents’ perceived social norms for toothbrushing and the frequency with which they report brushing their child’s teeth. Community Dent Health 2015, 32, 98–103. [Google Scholar] [PubMed]
- Shmueli, A.; Moskovitz, M.; Halperson, E.; Ram, D.; Fux-Noy, A. Epidemiology and Clinical Management of Early Childhood Caries in Israel. Front. Public Health 2019, 7, 280. [Google Scholar] [CrossRef]
- Joury, E. Syria Profile of the Epidemiology and Management of Early Childhood Caries Before and During the Time of Crisis. Front. Public Health 2019, 7, 271. [Google Scholar] [CrossRef]
- Castillo, J.L.; Palma, C.; Cabrera-Matta, A. Early Childhood Caries in Peru. Front. Public Health 2019, 7, 337. [Google Scholar] [CrossRef]
- Amalia, R.; Chairunisa, F.; Alfian, M.F.; Supartinah, A. Indonesia: Epidemiological Profiles of Early Childhood Caries. Front. Public Health 2019, 7, 210. [Google Scholar] [CrossRef] [Green Version]
- Harris, R.; Nicoll, A.D.; Adair, P.M.; Pine, C.M. Risk factors for dental caries in young children: A systematic review of the literature. Community Dent Health 2004, 21, 71–85. [Google Scholar]
- Pierce, A.; Singh, S.; Lee, J.; Grant, C.; De Jesus, V.C.; Schroth, R.J. The Burden of Early Childhood Caries in Canadian Children and Associated Risk Factors. Front. Public Health 2019, 7, 328. [Google Scholar] [CrossRef] [Green Version]
- Schroth, R.; Cheba, V. Determining the prevalence and risk factors for early childhood caries in a community dental health clinic. Pediatr. Dent. 2007, 29, 387–396. [Google Scholar]
- Alavi, G.; Alavi, A.; Saberfiroozi, M.; Sarbazi, A.; Motamedi, M.; Hamedani, S. Dental Erosion in Patients with Gastroesophageal Reflux Disease (GERD) in a Sample of Patients Referred to the Motahari Clinic, Shiraz, Iran. J. Dent. 2014, 15, 33–38. [Google Scholar]
- Reddy, V.K.; Poddar, P.; Mohammad, S.; Saha, S. Association between dental erosion and possible risk factors: A hospital-based study in gastroesophageal reflux disease patients. J. Indian Assoc. Public Health Dent. 2016, 14, 154. [Google Scholar]
- Loesche, W.J. Microbiology of Dental Decay and Periodontal Disease. In Medical Microbiology, 4th ed.; Baron, S., Ed.; University of Texas Medical Branch at Galveston: Galveston, TX, USA, 1996. [Google Scholar]
- Farooq, I.; Bugshan, A. The role of salivary contents and modern technologies in the remineralization of dental enamel: A narrative review. F1000Res 2020, 9, 171. [Google Scholar] [CrossRef] [PubMed]
- Buzalaf, M.A.R.; Hannas, A.R.; Kato, M.T. Saliva and dental erosion. J. Appl. Oral Sci. 2012, 20, 493–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anil, S.; Anand, P.S. Early Childhood Caries: Prevalence, Risk Factors, and Prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef] [Green Version]
- de Jong-Lenters, M.; L’Hoir, M.; Polak, E.; Duijster, D. Promoting parenting strategies to improve tooth brushing in children: Design of a non-randomised cluster-controlled trial. BMC Oral Health 2019, 19, 210. [Google Scholar] [CrossRef] [Green Version]
- Wright, J.T.; Hanson, N.; Ristic, H.; Whall, C.W.; Estrich, C.G.; Zentz, R.R. Fluoride toothpaste efficacy and safety in children younger than 6 years: A systematic review. J. Am. Dent. Assoc. 2014, 145, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Walsh, T.; Worthington, H.; Glenny, A.-M.; Appelbe, P.; Marinho, V.C.; Shi, X. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2010, 1, CD007868. [Google Scholar] [CrossRef]
- American Dental Association Council on Scientific Affairs. Fluoride toothpaste use for young children. J. Am. Dent. Assoc. 2014, 145, 190–191. [Google Scholar] [CrossRef]
- Pitts, N.B.; Mayne, C. Making Cavities History: A Global Policy Consensus for Achieving a Dental Cavity–Free Future. JDR Clin. Transl. Res. 2021, 6, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Dikmen, B. Icdas Ii Criteria (International Caries Detection and Assessment System). J. Istanb. Univ. Fac. Dent. 2015, 49, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Pitts, N.B.; Ismail, A.I.; Martignon, S.; Ekstrand, K.; Douglas, G.V.A.; Longbottom, C.; Deery, C.; Ellwood, R.; Gomez, J.; Kolker, J.; et al. ICCMSTM Guide for Practitioners and Educators. ICDAS Foundation. 2014. Available online: https://www.iccms-web.com/uploads/asset/59284654c0a6f822230100.pdf (accessed on 13 December 2021).
- Kay, E.J.; Northstone, K.; Ness, A.; Duncan, K.; Crean, S.J. Is there a relationship between Birthweight and subsequent growth on the development of Dental Caries at 5 years of age? A cohort study. Community Dent. Oral Epidemiol. 2010, 38, 408–414. [Google Scholar] [CrossRef]
- Leverett, D.H.; Adair, S.M.; Vaughan, B.W.; Proskin, H.M.; Moss, M.E. Randomized Clinical Trial of the Effect of Prenatal Fluoride Supplements in Preventing Dental Caries. Caries Res. 1997, 31, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Ghazal, T.S.; Levy, S.M.; Childers, N.K.; Broffitt, B.A.; Cutter, G.R.; Wiener, H.W.; Kempf, M.C.; Warren, J.J.; Cavanaugh, J.E. Factors associated with early childhood caries incidence among high caries-risk children. Community Dent. Oral Epidemiol. 2015, 43, 366–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglass, J.M.; Tinanoff, N.; Tang, J.M.; Altman, D.S. Dental caries patterns and oral health behaviors in Arizona infants and toddlers. Community Dent. Oral Epidemiol. 2001, 29, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Meurman, P.; Pienihäkkinen, K. Factors Associated with Caries Increment: A Longitudinal Study from 18 Months to 5 Years of Age. Caries Res. 2010, 44, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Wendt, L.-K.; Birkhed, D. Dietary habits related to caries development and immigrant status in infants and toddlers living in Sweden. Acta Odontol. Scand. 1995, 53, 339–344. [Google Scholar] [CrossRef]
- Aaltonen, A.S. The frequency of mother-infant salivary close contacts and maternal caries activity affect caries occurrence in 4-year-old children. Proc. Finn. Dent. Soc. Suom. Hammaslaak. Toim. 1991, 87, 373–382. [Google Scholar]
- Seelan, R.G.; Kumar, A.; Maheswari, S.U.; Raja, J. Caries management by risk assessment: A review on current strategies for caries prevention and management. J. Pharm. Bioallied Sci. 2015, 7, 320–324. [Google Scholar] [CrossRef]
- Barnes, G.P.; A Parker, W.; Lyon, T.C., Jr.; A Drum, M.; Coleman, G.C. Ethnicity, location, age, and fluoridation factors in baby bottle tooth decay and caries prevalence of Head Start children. Public Health Rep. 1992, 107, 167–173. [Google Scholar]
- Hu, D.; Wan, H.; Li, S. The caries-inhibiting effect of a fluoride drop program: A 3-year study on Chinese kindergarten children. Chin. J. Dent. Res. 1998, 1, 17–20. [Google Scholar] [PubMed]
- Pitts, N.; Amaechi, B.; Niederman, R.; Acevedo, A.M.; Vianna, R.; Ganss, C.; Ismail, A.; Honkala, E. Global oral health inequalities: Dental caries task group—Research agenda. Adv. Dent. Res. 2011, 23, 211–220. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.T.; Tsai, C.L. Caries prevalence and bottle-feeding practices in 2-year-old children with cleft lip, cleft palate, or both in Taiwan. Cleft Palate Craniofac. J. 1999, 36, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M. The Clinical, Environmental, and Behavioral Factors That Foster Early Childhood Caries: Evidence for Caries Risk Assessment. Pediatr. Dent. 2015, 37, 217–225. [Google Scholar] [PubMed]
- Llena, C.; Calabuig, E.; Sanz, J.L.; Melo, M. Risk Factors Associated with Carious Lesions in Permanent First Molars in Children: A Seven-Year Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 1421. [Google Scholar] [CrossRef]
- Freeman, L.; Martin, S.; Rutenberg, G.; Shirejian, P.; Skarie, M. Relationships between DEF, demographic and behavioral variables among multiracial preschool children. ASDC J. Dent. Child. 1989, 56, 205–210. [Google Scholar]
- Kraljevic, I.; Filippi, C.; Filippi, A. Risk indicators of early childhood caries (ECC) in children with high treatment needs. Swiss Dent. J. 2017, 127, 398–410. [Google Scholar]
- Elamin, A.; Garemo, M.; Gardner, A. Dental caries and their association with socioeconomic characteristics, oral hygiene practices and eating habits among preschool children in Abu Dhabi, United Arab Emirates—The NOPLAS project. BMC Oral Health 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Çolak, H.; Dülgergil, C.T.; Dalli, M.; Hamidi, M.M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29–38. [Google Scholar]
- Johansson, I.; Holgerson, P.L.; Kressin, N.R.; Nunn, M.E.; Tanner, A.C. Snacking Habits and Caries in Young Children. Caries Res. 2010, 44, 421–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurlbutt, M.; Young, D.A. A Best Practices Approach to Caries Management. J. Évid.-Based Dent. Pract. 2014, 14, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Al-Mendalawi, M.D.; Karam, N.T. Risk factors associated with deciduous tooth decay in Iraqi preschool children. Avicenna J. Med. 2014, 4, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Mongkolchati, A.; Satchaiyan, G.; Rajchagool, S.; Pimpak, T. Sociobehavioral Factors Associated with Caries Increment: A Longitudinal Study from 24 to 36 Months Old Children in Thailand. Int. J. Environ. Res. Public Health 2014, 11, 10838–10850. [Google Scholar] [CrossRef] [Green Version]
- Sanders, A.E.; Slade, G.D. Apgar score and dental caries risk in the primary dentition of five year olds. Aust. Dent. J. 2010, 55, 260–267. [Google Scholar] [CrossRef]
- Winter, J.; Glaser, M.; Heinzel-Gutenbrunner, M.; Pieper, K. Association of caries increment in preschool children with nutritional and preventive variables. Clin. Oral Investig. 2015, 19, 1913–1919. [Google Scholar] [CrossRef]
- Qin, M.; Li, J.; Zhang, S.; Ma, W. Risk factors for severe early childhood caries in children younger than 4 years old in Beijing, China. Pediatr. Dent. 2008, 30, 122–128. [Google Scholar]
- Al Ghanim, N.A.; Adenubi, J.O.; Wyne, A.A.; Khan, N.B. Caries prediction model in pre-school children in Riyadh, Saudi Arabia. Int. J. Paediatr. Dent. 1998, 8, 115–122. [Google Scholar] [CrossRef]
- Ekman, A. Dental caries and related factors—A longitudinal study of Finnish immigrant children in the north of Sweden. Swed. Dent. J. 1990, 14, 93–99. [Google Scholar]
- Gibson, S.; Williams, S. Dental caries in pre-school children: Associations with social class, toothbrushing habit and consumption of sugars and sugar-containing foods. Further analysis of data from the National Diet and Nutrition Survey of children aged 1.5–4.5 years. Caries Res. 1999, 33, 101–113. [Google Scholar] [CrossRef]
- Grindefjord, M.; Dahllöf, G.; Nilsson, B.; Modéer, T. Prediction of Dental Caries Development in 1-Year-Old Children. Caries Res. 1995, 29, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Lopez Del Valle, L.; Velazquez-Quintana, Y.; Weinstein, P.; Domoto, P.; Leroux, B. Early childhood caries and risk factors in rural Puerto Rican children. ASDC J. Dent. Child 1998, 65, 132–135. [Google Scholar]
- Al-Haj Ali, S.N.; Alsineedi, F.; Alsamari, N.; Alduhayan, G.; BaniHani, A.; Farah, R.I. Risk Factors of Early Childhood Caries Among Preschool Children in Eastern Saudi Arabia. Sci. Prog. 2021, 104, 368504211008308. [Google Scholar] [CrossRef] [PubMed]
- Smyth, E.; Caamaño, F. Factors related to dental health in 12-year-old children: A cross-sectional study in pupils. Gac. Sanit. 2005, 19, 113–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.B.; Zhang, W.; Zhou, X.B. Risk Factors associated with Early Childhood Caries. Chin. J. Dent. Res. 2017, 20, 97–104. [Google Scholar]
- Nobile, C.G.; Fortunato, L.; Bianco, A.; Pileggi, C.; Pavia, M. Pattern and severity of early childhood caries in Southern Italy: A preschool-based cross-sectional study. BMC Public Health 2014, 14, 206. [Google Scholar] [CrossRef] [Green Version]
- Warren, J.J.; Weber-Gasparoni, K.; Marshall, T.A.; Drake, D.R.; Dehkordi-Vakil, F.; Dawson, D.V.; Tharp, K.M. A longitudinal study of dental caries risk among very young low SES children. Community Dent. Oral Epidemiol. 2009, 37, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Yonezu, T.; Ushida, N.; Yakushiji, M. Longitudinal Study of Prolonged Breast- or Bottle-feeding on Dental Caries in Japanese Children. Bull. Tokyo Dent. Coll. 2006, 47, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Aaltonen, A.S.; Tenovuo, J. Association between mother-infant salivary contacts and caries resistance in children: A cohort study. Pediatr. Dent. 1994, 16, 110–116. [Google Scholar]
- Rayner, J.; Holt, R.; Blinkhorn, F.; Duncan, K.; British Society of Paediatric Dentistry. British Society of Paediatric Dentistry: A policy document on oral health care in preschool children. Int. J. Paediatr. Dent. 2003, 13, 279–285. [Google Scholar]
- Anonymous. Review of methods of identification of high caries risk groups and individuals. Fédération Dentaire Internationale Technical Report No. 31. Int. Dent. J. 1988, 38, 177–189. [Google Scholar]
- Freeman, R.; Breistein, B.; McQueen, A.; Stewart, M. The dental health status of five-year-old children in north and west Belfast. Community Dent. Health 1997, 14, 253–257. [Google Scholar] [PubMed]
- Fan, C.C.; Wang, W.H.; Xu, T.; Zheng, S.G. Risk factors of early childhood caries (ECC) among children in Beijing—A prospective cohort study. BMC Oral Health 2019, 19, 34. [Google Scholar] [CrossRef]
- Hurley, E.; Barrett, M.P.J.; Kinirons, M.; Whelton, H.; Ryan, C.A.; Stanton, C.; Harris, H.M.B.; O’Toole, P.W. Comparison of the salivary and dentinal microbiome of children with severe-early childhood caries to the salivary microbiome of caries-free children. BMC Oral Health 2019, 19, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marthaler, T.M. Changes in dental caries 1953–2003. Caries Res. 2004, 38, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Geyer, S.; Schneller, T.; Micheelis, W. Social gradients and cumulative effects of income and education on dental health in the Fourth German Oral Health Study. Community Dent. Oral Epidemiol. 2010, 38, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.D.; Winter, G.B.; Downer, M.C.; Bellis, W.J.; Hay, I.S. Caries in pre-school children in Camden 1993/94. Br. Dent. J. 1996, 181, 405–410. [Google Scholar] [CrossRef]
- Karjalainen, S.; Söderling, E.; Sewón, L.; Lapinleimu, H.; Simell, O. A prospective study on sucrose consumption, visible plaque and caries in children from 3 to 6 years of age. Community Dent. Oral Epidemiol. 2001, 29, 136–142. [Google Scholar] [CrossRef]
- Li, Y.; Wang, W.; Caufield, P. The Fidelity of Mutans Streptococci Transmission and Caries Status Correlate with Breast–Feeding Experience among Chinese Families. Caries Res. 2000, 34, 123–132. [Google Scholar] [CrossRef]
- Oliveira, A.; Chaves, A.; Rosenblatt, A. The Influence of Enamel Defects on the Development of Early Childhood Caries in a Population with Low Socioeconomic Status: A Longitudinal Study. Caries Res. 2006, 40, 296–302. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, J.; Lo, E.; Lin, H. The Contribution of Life Course Determinants to Early Childhood Caries: A 2-Year Cohort Study. Caries Res. 2012, 46, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Hong, L.; Levy, S.; Warren, J.; Broffitt, B. Association between Enamel Hypoplasia and Dental Caries in Primary Second Molars: A Cohort Study. Caries Res. 2009, 43, 345–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seow, W.K.; Clifford, H.; Battistutta, D.; Morawska, A.; Holcombe, T. Case-Control Study of Early Childhood Caries in Australia. Caries Res. 2009, 43, 25–35. [Google Scholar] [CrossRef]
- Targino, A.G.R.; Rosenblatt, A.; Oliveira, A.F.; Chaves, A.M.B.; Santos, V.E. The relationship of enamel defects and caries: A cohort study. Oral Dis. 2011, 17, 420–426. [Google Scholar] [CrossRef]
- Pascoe, L.; Seow, W.K. Enamel hypoplasia and dental caries in Australian aboriginal children: Prevalence and correlation between the two diseases. Pediatr. Dent. 1994, 16, 193–199. [Google Scholar]
- Harrison, R.; Wong, T.; Ewan, C.; Contreras, B.; Phung, Y. Feeding practices and dental caries in an urban Canadian population of Vietnamese preschool children. ASDC J. Dent. Child. 1997, 64, 112–117. [Google Scholar]
- Isokangas, P.; Soderling, E.; Pienihakkinen, K.; Alanen, P. Occurrence of Dental Decay in Children after Maternal Consumption of Xylitol Chewing Gum, a Follow-up from 0 to 5 Years of Age. J. Dent. Res. 2000, 79, 1885–1889. [Google Scholar] [CrossRef]
- Tanaka, K.; Miyake, Y.; Sasaki, S.; Hirota, Y. Socioeconomic status and risk of dental caries in Japanese preschool children: The Osaka Maternal and Child Health Study. J. Public Health Dent. 2013, 73, 217–223. [Google Scholar] [CrossRef]
- Al-Meedani, L.A.; Al-Dlaigan, Y.H. Prevalence of dental caries and associated social risk factors among preschool children in Riyadh, Saudi. Pak. J. Med. Sci. 2016, 32, 452–456. [Google Scholar] [CrossRef]
- Kato, H.; Tanaka, K.; Shimizu, K.; Nagata, C.; Furukawa, S.; Arakawa, M.; Miyake, Y. Parental occupations, educational levels, and income and prevalence of dental caries in 3-year-old Japanese children. Environ. Health Prev. Med. 2017, 22, 80. [Google Scholar] [CrossRef]
- Özbek, C.D.; Eser, D.; Bektaş-Kayhan, K.; Ünür, M. Comparison of the Tooth Brushing Habits of Primary School Age Children and Their Parents. J. Istanb. Univ. Fac. Dent. 2015, 49, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.T.; Bule, M.; Ullah, R.; Nadeem, M.; Asif, S.; Niaz, K. The antioxidant components of milk and their role in processing, ripening, and storage: Functional food. Veter-World 2019, 12, 12–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Touger-Decker, R.; van Loveren, C. Sugars and dental caries. Am. J. Clin. Nutr. 2003, 78, 881S–892S. [Google Scholar] [CrossRef] [Green Version]
- Roberts, M.W.; Wright, J.T. Nonnutritive, Low Caloric Substitutes for Food Sugars: Clinical Implications for Addressing the Incidence of Dental Caries and Overweight/Obesity. Int. J. Dent. 2012, 2012, 1–8. [Google Scholar] [CrossRef]
- Ghasempour, M.; Rajabnia, R.; Irannejad, A.; Hamzeh, M.; Ferdosi, E.; Bagheri, M. Frequency, biofilm formation and acid susceptibility of streptococcus mutans and streptococcus sobrinus in saliva of preschool children with different levels of caries activity. Dent. Res. J. 2013, 10, 440–445. [Google Scholar]
- Strużycka, I. The Oral Microbiome in Dental Caries. Pol. J. Microbiol. 2014, 63, 127–135. [Google Scholar] [CrossRef]
- Baraniya, D.; Chen, T.; Nahar, A.; Alakwaa, F.; Hill, J.; Tellez, M.; Ismail, A.; Puri, S.; Al-Hebshi, N.N. Supragingival mycobiome and inter-kingdom interactions in dental caries. J. Oral Microbiol. 2020, 12, 1729305. [Google Scholar] [CrossRef] [Green Version]
- Carey, C.M. Focus on Fluorides: Update on the Use of Fluoride for the Prevention of Dental Caries. J. Évid.-Based Dent. Pract. 2014, 14, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Horst, J.A.; Tanzer, J.M.; Milgrom, P.M. Fluorides and Other Preventive Strategies for Tooth Decay. Dent. Clin. N. Am. 2018, 62, 207–234. [Google Scholar] [CrossRef]
- Newbrun, E. Topical Fluorides in Caries Prevention and Management: A North American Perspective. J. Dent. Educ. 2001, 65, 1078–1083. [Google Scholar] [CrossRef]
- Reynolds, E.C. Calcium phosphate-based remineralization systems: Scientific evidence? Aust. Dent. J. 2008, 53, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Lin, X.; Zhong, T.; Xie, F. Evaluation of the efficacy of casein phosphopeptide-amorphous calcium phosphate on remineralization of white spot lesions in vitro and clinical research: A systematic review and meta-analysis. BMC Oral Health 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bröseler, F.; Tietmann, C.; Bommer, C.; Drechsel, T.; Heinzel-Gutenbrunner, M.; Jepsen, S. Randomised clinical trial investigating self-assembling peptide P11-4 in the treatment of early caries. Clin. Oral Investig. 2020, 24, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Alkilzy, M.; Tarabaih, A.; Santamaria, R.; Splieth, C. Self-assembling Peptide P11-4 and Fluoride for Regenerating Enamel. J. Dent. Res. 2018, 97, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Kondelova, P.S.; Mannaa, A.; Bommer, C.; Abdelaziz, M.; Daeniker, L.; Di Bella, E.; Krejci, I. Efficacy of P11-4 for the treatment of initial buccal caries: A randomized clinical trial. Sci. Rep. 2020, 10, 20211. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Pascadopoli, M.; Gallo, S.; Lelli, M.; Tarterini, F.; Giglia, F.; Scribante, A. SEM/EDS Evaluation of the Mineral Deposition on a Polymeric Composite Resin of a Toothpaste Containing Biomimetic Zn-Carbonate Hydroxyapatite (microRepair®) in Oral Environment: A Randomized Clinical Trial. Polymers 2021, 13, 2740. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Dermenaki Farahani, M.R.; Marino, G.; Matera, C.; Rodriguez, Y.; Baena, R.; Lanteri, V.; Butera, A. Biomimetic Effect of Nano-Hydroxyapatite in Demineralized Enamel before Orthodontic Bonding of Brackets and Attachments: Visual, Adhesion Strength, and Hardness in In Vitro Tests. Biomed. Res. Int. 2020, 2020, 6747498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossù, M.; Saccucci, M.; Salucci, A.; DI Giorgio, G.; Bruni, E.; Uccelletti, D.; Sarto, M.S.; Familiari, G.; Relucenti, M.; Polimeni, A. Enamel remineralization and repair results of Biomimetic Hydroxyapatite toothpaste on deciduous teeth: An effective option to fluoride toothpaste. J. Nanobiotechnol. 2019, 17, 17. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2021, 9, 69. [Google Scholar] [CrossRef]

{kind=link}
| Low Risk | Medium Risk | High Risk |
|---|---|---|
| Tooth brushing 2/day with a fluoride toothpaste (≥1000 ppm), following the dental team instructions | Tooth brushing 2/day with a fluoride toothpaste (≥1450 ppm), following the dental team instructions | Tooth brushing 2/day with a fluoride toothpaste (≥1450 ppm), following the dental team instructions |
| General Behaviour Modification in Oral Health | General Behaviour Modification in Oral Health | |
| Prescribed Fluoride mouth rinse | Prescribed Fluoride mouth rinse | |
| Motivational engagement (discuss with patients how to improve oral health behaviours—including amount of sugar), maintain dental visits at risk-based intervals | ||
| Sealants Fluoride varnish 2 times/year Fluoride gel or solution Recalls up to every 3 months: professional cleaning and topical fluoride- application on active lesions | Sealants Fluoride varnish 2 times/year Fluoride gel or solution Recalls up to every 3 months: professional cleaning and topical fluoride- application on active lesions | |
| Motivational interviewing One-to-one dietary intake interventions Altering medication-induced hyposalivation Reducing the use of recreational drugs | Motivational interviewing One-to-one dietary intake interventions Altering medication-induced hyposalivation Reducing the use of recreational drugs | |
| Increase fluoride varnish to 4 times/year | ||
| Topical fluoride application, counseling: reduce sugar amount and frequency | ||
| Risk Factors Associated with Caries | ||
|---|---|---|
| Dietary factors | High sugar consumptions (snacks, soft drinks, sugary bed-time drinks) | [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45] |
| Oral hygiene | Frequency of toothbrushing, plaque accumulation | [36,37,38,40,41,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58] |
| Presence of Streptococcus mutans | [29,59,60,61,62,63,64,65,66] | |
| Breastfeeding | Up to 6 months | [40,50,55,67,68,69,70,71] |
| Hypoplasia | [38,72,73,74,75,76,77] | |
| Socio-economic factors | Educational parental level, rural or urban domicile | [28,37,38,39,41,57,58,63,78,79,80,81,82] |
| Factors | Low Risk | Medium Risk | High Risk |
|---|---|---|---|
| DMFT and Caries activity | / | Within 24 months | Within 12 months |
| Enamel defects and dental erosion | / | On a few elements | Spread in both arcades |
| Frequency of sugars and carbohydrates intake | During the main meals | During main meals and in the morning and/or afternoon break | During main meals, in the morning and/or afternoon break and at night |
| Saliva quality and quantity | Abundant flow, high buffering capacity, low acidity | Medium flow, medium buffer capacity, medium acidity and medium bacterial charge | Low flow, low buffer capacity, high acidity and high bacterial load |
| Remineralization (fluoride, substituted fluoride as biomimetic hydroxyapatite and calcium phosphate) | Daily | Occasional | Absent |
| Eating disorders | / | / | Anorexia, bulimia, binge eating, gastroesophageal reflux |
| Oral hygiene (Silness & Loe plate index evaluation) | No bacterial stratification | Plaque along the gingival margin, free but biofilm interdental spaces visible to the naked eye | Plaque along the gingival margin and in the interdental spaces |
| Socioeconomic status and oral family health | High/no caries | Medium/low caries rate | Low/high caries rate |
| Special conditions | / | / | Asthmatic patients undergoing radiotherapy, with systemic pathologies, with orthodontic devices |
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Primary prevention | Oral hygiene instructions: 2 min of brushing, preferably after each main meal | Oral hygiene instructions: 2 min of brushing, preferably after each main meal | Oral hygiene instructions: 2 min of brushing, preferably after each main meal |
| Collection of information on the eating habits and oral health of children and families | Collection of information on the eating habits and oral health of children and families | Collection of information on the eating habits and oral health of children and families | |
| Professional oral hygiene every 6 months | Professional oral hygiene every 4 months | Professional oral hygiene every 3 months | |
| Professional use of remineralizing agents: fluoride-based, casein phosphopeptide-amorphous calcium phosphate or zinc-substituted hydroxyapatite gel or mousse, self-assembling oligopeptide SAP-P11-4 | Professional use of remineralizing agents: fluoride-based, casein phosphopeptide-amorphous calcium phosphate or zinc-substituted hydroxyapatite gel or mousse, self-assembling oligopeptide SAP-P11-4 | Professional use of remineralizing agents: fluoride-based, casein phosphopeptide-amorphous calcium phosphate or zinc-substituted hydroxyapatite gel or mousse, self-assembling oligopeptide SAP-P11-4 | |
| Home use of remineralizing agents, as toothpastes containing fluoride or zinc-substituted hydroxyapatite | Home use of remineralizing agents, as toothpastes containing fluoride or zinc-substituted hydroxyapatite and mousse with zinc-substituted hydroxyapatite once a day for 10 days, for about 10 min | Home use of remineralizing agents, as toothpastes containing fluoride or zinc-substituted hydroxyapatite and mousse with zinc-substituted hydroxyapatite once a day for 10 days, for about 10 min |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Trombini, J.; Scribante, A. Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations. Children 2022, 9, 262. https://doi.org/10.3390/children9020262
Butera A, Maiorani C, Morandini A, Simonini M, Morittu S, Trombini J, Scribante A. Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations. Children. 2022; 9(2):262. https://doi.org/10.3390/children9020262
Chicago/Turabian StyleButera, Andrea, Carolina Maiorani, Annalaura Morandini, Manuela Simonini, Stefania Morittu, Julia Trombini, and Andrea Scribante. 2022. "Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations" Children 9, no. 2: 262. https://doi.org/10.3390/children9020262
APA StyleButera, A., Maiorani, C., Morandini, A., Simonini, M., Morittu, S., Trombini, J., & Scribante, A. (2022). Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations. Children, 9(2), 262. https://doi.org/10.3390/children9020262