
Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far?


Abstract
:1. Introduction
2. Incidence of Vaccine Related Myocarditis/Pericarditis
3. Causal Relation between mRNA Vaccine and Myocarditis/Pericarditis
4. Clinical Summary of Published Cases of Myocarditis and Pericarditis
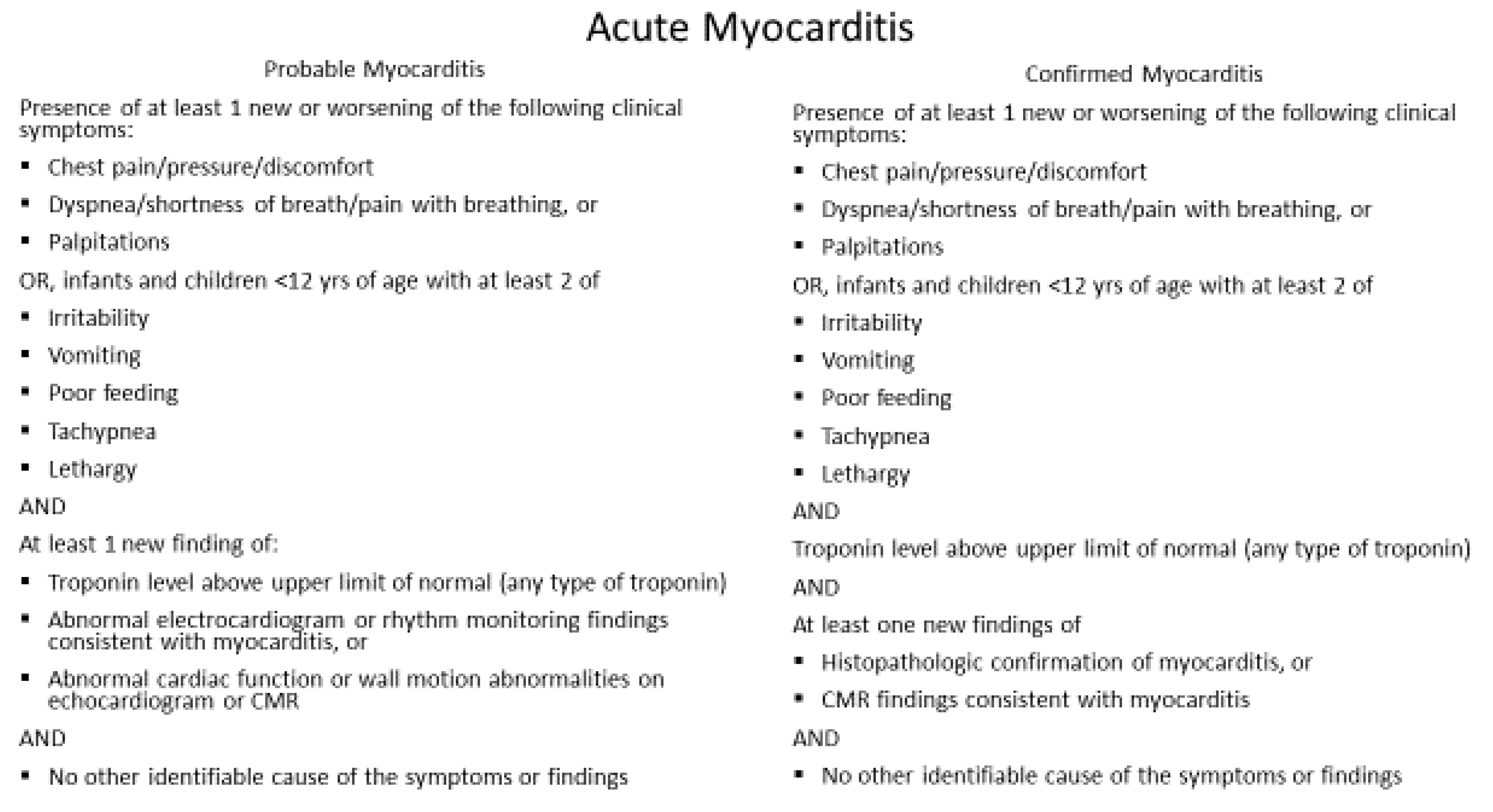
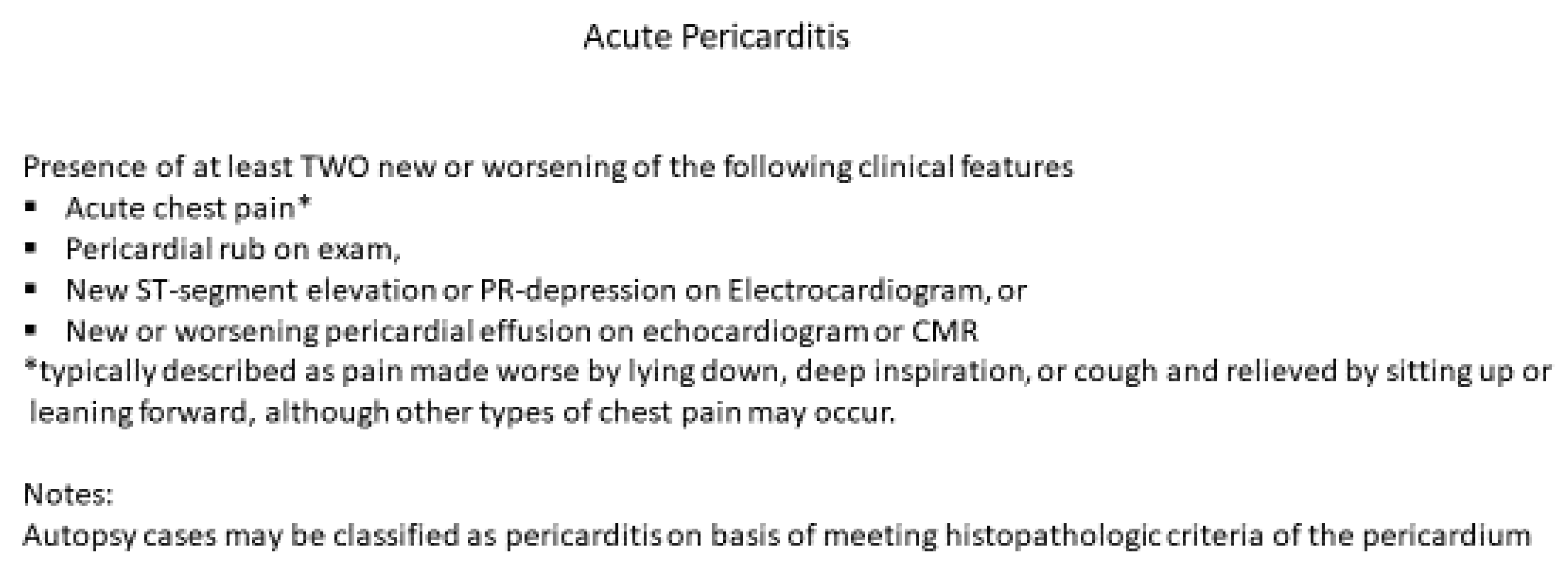
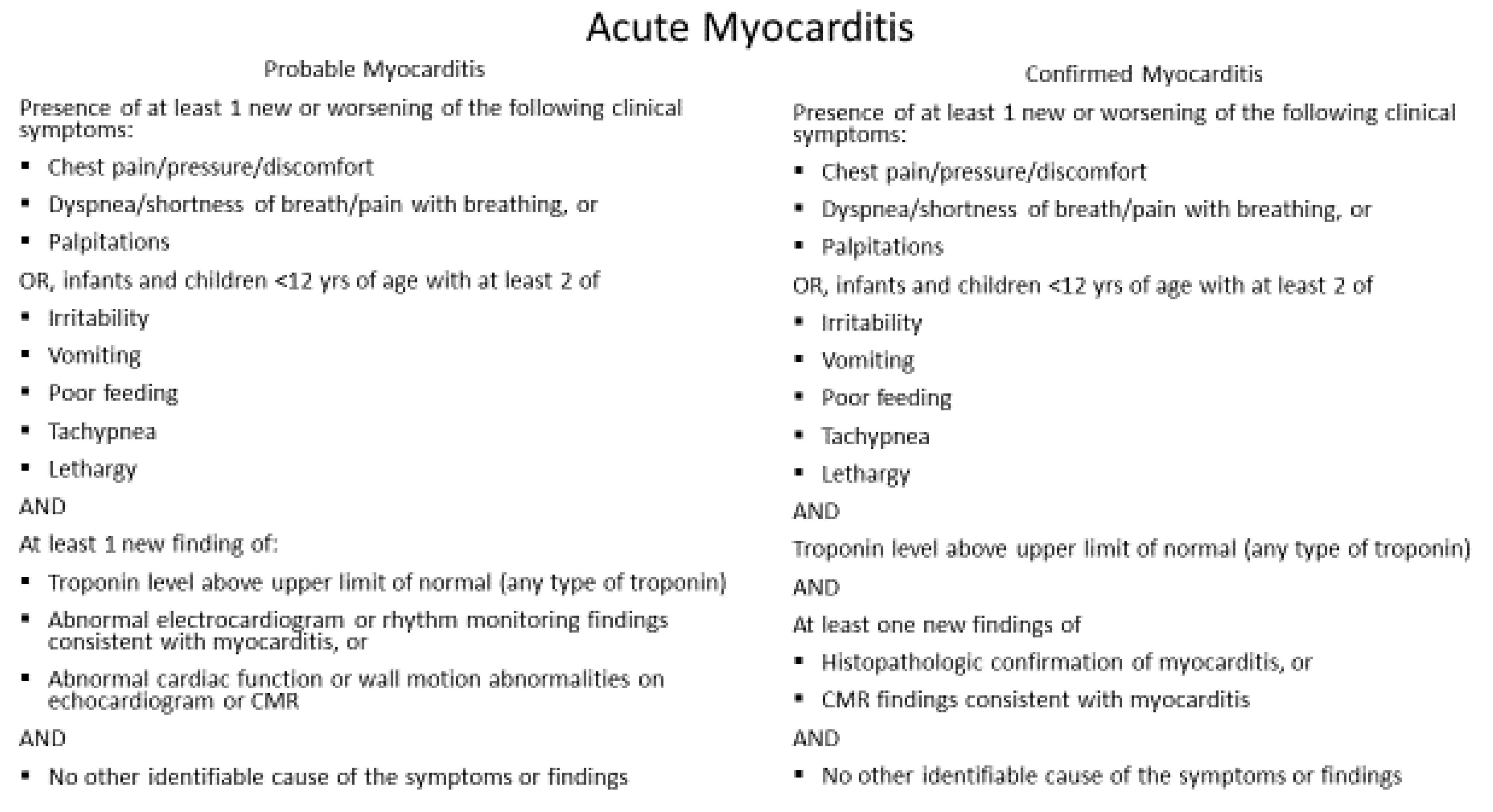
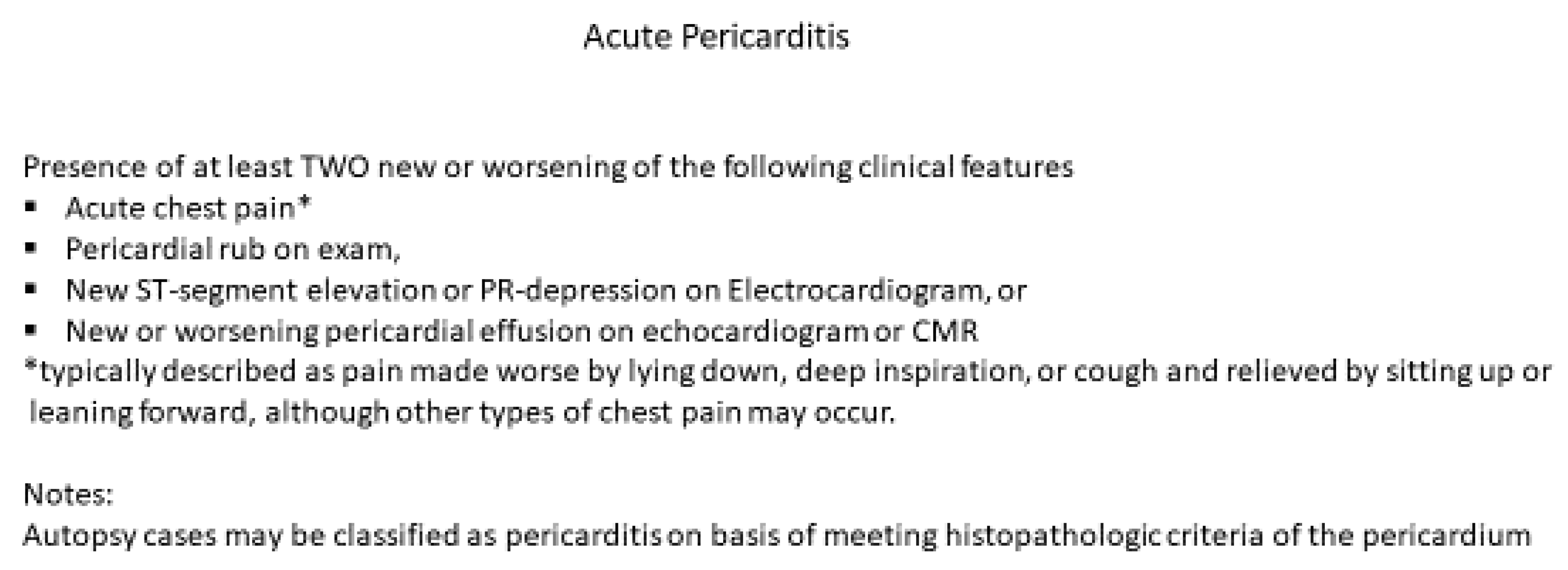
5. Diagnosis and Management
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| MIS-C | Multisystem inflammatory syndrome in children |
| CRP | C-reactive protein; LV: left ventricle |
| RV | Right ventricle; CMR: cardiac magnetic resonance |
| CDC | Center for Disease Control and Prevention |
| FDA | Food and Drug Administration |
| VAERS | Vaccine Adverse Event Reporting System |
| VSD | Vaccine safety data |
| VRBPAC | Vaccine Related Biological Products Advisory Committee |
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Oliver, S.E.; Gargano, J.W.; Marin, M.; Wallace, M.; Curran, K.G.; Chamberland, M.; McClung, N.; Campos-Outcalt, D.; Morgan, R.; Mbaeyi, S.; et al. The Advisory Committee on Immunization Practices’ interim recommendation for use of Pfizer-BioNTech COVID-19 vaccine—United States, December 2020. MMWR Morb. Mortal Wkly Rep. 2020, 69, 1922–1924. [Google Scholar] [CrossRef]
- Wallace, M.; Woodworth, K.R.; Gargano, J.W.; Scobie, H.M.; Blain, A.E.; Moulia, D.; Chamberland, M.; Reisman, N.; Hadler, S.C.; MacNeil, J.R.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendation for using Pfizer-BioNTech COVID-19 Vaccine in Adolescents Aged 12–15 Years—United States, May 2021. MMWR 2021, 70, 749–752. [Google Scholar]
- Dalgaard, J.B. Fatal myocarditis following smallpox vaccination. Am. Heart J. 1957, 54, 156–157. [Google Scholar] [CrossRef]
- Mei, R.; Raschi, E.; Forcesi, E.; Diemberger, I.; De Ponti, F.; Poluzzi, E. Myocarditis and pericarditis after immunization: Gaining insights through the vaccine adverse event reporting system. Int. J. Cardiol. 2018, 273, 183–186. [Google Scholar] [CrossRef]
- Kime, P. Pentagon Tracking 14 cases of Heart Inflammation in Troops after COVID-19 Shots. Published 26 April 2021. Available online: https://www.military.com/daily-news/2021/04/26/pentagon-tracking-14-cases-of-heart-inflammation-troops-after-covid-19-shots.html (accessed on 16 May 2021).
- Ammirati, E.; Cavalotti, C.; Milazzo, A.; Pedrotti, P.; Soriano, F. Temporal relation between second dose BNT162b2 mRNA COVID-19 vaccine and cardiac involvement in a patient with previous SARS-CoV-2 infection. IJC Heart Vasc. 2021, 34, 100774. [Google Scholar] [CrossRef]
- Marshall, M.; Ferguson, I.D.; Lewis, P.; Jaggi, P.; Gagliardo, C.; Collins, J.S.; Shaughnessya, R.; Carona, R.; Fuss, C.; Corbin, K.J.E.; et al. Symptomatic acute myocarditis in seven adolescents following Pfizer-BioNTech COVID-19 vaccination. Pediatrics 2021. [Google Scholar] [CrossRef] [PubMed]
- Snapiri, O.; Vanziger, C.R.; Chairman, N.; Weissbach, A.; Lowenthal, A.; Ayalon, I.; Adam, D.; Yarden-Bilavsky, H.; Bilavsky, E. Transient cardiac injury in adolescents receiving the BNT162b2 mRNA COVID-19 vaccine. Pediatr. Infect. Dis. J. 2021. [CrossRef]
- Rosner, C.M.; Genovese, L.; Tehrani, B.; Atkins, M.; Bakhshi, H.; Chaudhri, S.; Damluji, A.A.; de Lemos, J.A.; Desai, S.S.; Emaminia, A.; et al. Myocarditis temporarily associated with COVID-19 Vaccination. Circulation 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Larson, K.F.; Ammirati, E.; Adler, E.D.; Cooper, L.T.; Hong, K.N.; Saponara, G.; Couri, D.; Cereda, A.; Procopio, A.; Cavalotti, C.; et al. Myocarditis after BNT1622b2 and mRNA Vaccination. Circulation 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- AAP News. Available online: https://www.aappublications.org/news/2021/06/10/covid-vaccine-myocarditis-rates-061021 (accessed on 18 June 2021).
- AHA Statement on 23 May 2021. Available online: https://newsroom.heart.org/news/covid-19-vaccine-benefits-still-outweigh-risks-despite-possible-rare-heart-complications (accessed on 18 June 2021).
- Recent Update on mRNA Vaccine. Available online: https://www.cdc.gov/vaccines/acip/meetings/slides-2021-06.html (accessed on 26 June 2021).
- Food and Drug Administration. Pfizer-BioNTech COVID-19 Vaccine Emergency Use Authorization; US Department of Health and Human Services, Food and Drug Administration: Silver Spring, MD, USA, 2021. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccine (accessed on 26 June 2021).
- Vaccine and Related Biological Products Advisory Committee (VRBPAC) 10 June 2021, Meeting Presentation. Available online: https://www.fda.gov/media/150054/download (accessed on 15 June 2021).
- Montgomery, J.; Ryan, M.; Engler, R.; Hoffman, D.; McCleanathan, B.; Collins, L.; Loran, D.; Hrncir, D.; Herring, K.; Platzer, M.; et al. Myocarditis following immunization with mRNA COVID-19 vaccine in memebrs of the US military. JAMA Cardiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Vogel, G.; Couzin-Frankel, J. Israel reports link between rare cases of heart inflammation and COVID-19 vaccination in young men. Science 2021. [Google Scholar] [CrossRef]
- Source: ema.europa.eu. Available online: https://www.ema.europa.eu/en/news/comirnaty-spikevax-possible-link-very-rare-cases-myocarditis-pericarditis (accessed on 12 July 2021).
- Grimaud, M.; Starck, J.; Levy, M.; Marais, C.; Chareyre, J.; Khraiche, D.; Leruez-Ville, M.; Quartier, P.; Léger, P.L.; Geslain, G.; et al. Acute myocarditis and multisystem inflammatory emerging disease following SARS-CoV-2 infection in critically ill children. Ann. Intensive Care. 2020, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Muthukumar, A.; Narasimhan, M.; Li, Q.Z.; Mahimainathan, L.; Hitto, I.; Fuda, F.; Batra, K.; Jiang, X.; Zhu, C.; Schoggins, J.; et al. In depth evaluation of a case of presumed myocarditis following the second dose of COVID-19 mRNA vaccine. Circulation 2021. [Google Scholar] [CrossRef]
- Segal, Y.; Shoenfeld, Y. Vaccine-induced autoimmunity: The role of molecular mimicry an immune cross-reaction. Cell Mol. Immunol. 2018, 15, 586–594. [Google Scholar] [CrossRef]
- Root-Berstein, R.; Fairweather, D. Unresolved issues in theories of autoimmune disease varying myocarditis as a framework. J. Theor. Biol. 2015, 375, 101–123. [Google Scholar] [CrossRef] [Green Version]
- Perez-Bermejo, J.A.; Kang, S.; Rockwood, S.J.; Simoneau, C.R.; Joy, D.A.; Ramadoss, G.N.; Silva, A.C.; Flanigan, W.R.; Li, H.; Nakamura, K.; et al. SARS-CoV-2 infection of human iPSC-derived cardiac cells reflect cytopathic features in hearts of patients with COVID-19. Sci. Transl. Med. 2021, 30, eabf7872. [Google Scholar] [CrossRef] [PubMed]
- Marchiano, S.; Hsiang, T.Y.; Khanna, A.; Higashi, T.; Whitmore, L.S.; Bargehr, J.; Davaapil, H.; Chang, J.; Smith, E.; Ong, L.P.; et al. SARS-CoV-2 infects human pluripotent stem cell-derived cardiomyocytes, impairing electrical and mechanical function. Stem Cell Rep. 2021, 16, 478–492. [Google Scholar] [CrossRef]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef]
- Das, B.B. Role of endomyocardial biopsy for children presenting with acute systolic heart failure. Pediatr. Cardiol. 2014, 35, 191–196. [Google Scholar] [CrossRef]
- Law, Y.M.; Lal, A.K.; Chen, S.; Cihakova, D.; Cooper, L.T.; Deshpande, S.; Godown, J.; Grosse-Wortmann, L.; Robinson, J.D.; Towbin, J.A. Diagnosis and management of myocarditis in Children. A Scinetific Statement from the American Heart Association. Circulation 2021, 144. [Google Scholar] [CrossRef]
- Radunski, U.K.; Lund, G.K.; Sharing, D.; Bohnen, S.; Stehning, S.; Schnackenburg, B.; Avanesov, M.; Tahir, E.; Adam, G.; Blankenberg, S.; et al. T1, and T2 mapping cardiovascular resonance imaging technique reveal unapparent myocardial injury in patients with myocarditis. Clin. Res. Cardiol. 2017, 106, 10–17. [Google Scholar] [CrossRef]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020, 13, e007405. [Google Scholar] [CrossRef] [PubMed]
- AAP Recommendations in “COVID-19 Interim Guidance: Return to Sports”. Available online: https://www.aappublications.org/news/2020/12/04/sportsguidance120420 (accessed on 15 June 2021).
- Maron, B.J.; Udelson, J.E.; Bonow, R.O.; Nishimura Raackerman, M.J.; Estes, N.M., III. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: A scientific statement from the American Heart Association and American College of Cardiology. Circulation 2015, 132, e273–e280. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Age Years and Gender | mRNA Vaccine Dose | Days from Vaccination to Sx | COVID Serology | Symptoms | CRP | Tn | ECG | ECHO | CMR | Treatment | Hospitalization in Days |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. 16 M [9] | 2nd | 2 | + | Fever Chest pain | ↑ | ↑ | ST↑ Junctional rhythm | NL LV Fx | LGE+ | IVIG Steroid NSAID | 6 |
| 2. 19 M [9] | 2nd | 3 | - | Fever, Myalgia, Weakness | ↑ | ↑ | Diffuse ST changes | NL LV Fx | LGE + | NSAID Colchicine | 2 |
| 3. 17 M [9] | 2nd | 2 | + | Chest pain | ↑ | ↑ | Diffuse ST changes | NL LV Fx | Edema+ LGE+ | NSAID | None |
| 4. 18 M [9] | 2nd | Immediately after vaccine | + | Chest pain | NA | ↑ | ST↑ | NL LV Fx | NA | IVIG NSAID | 3 |
| 5. 17 M [9] | 2nd | 3 | + | Chest pain Fever | NA | ↑ | ST↑ | NL LV Fx | NA | IVIG Steroid | 3 |
| 6. 16 M [9] | 2nd | 3 | + | Fever Chest pain | NA | ↑ | ST↑ | NA | Edema LGE+ | IVIG Prednisone | 3 |
| 7. 14 M [9] | 2nd | 3 | - | Fever Chest pain | NA | ↑ | Diffuse ST changes | LV Fx ↓ | Edema LGE+ | NSAID | 3 |
| 8. 17 M [10] | 2nd | 3 | NA | Chest pain | ↑ | ↑ | ST↑ RBBB | NL LV Fx | NA | NA | 4 |
| 9. 16 M [10] | 2nd | 1 | + | Chest pain | ↑ | ↑ | Diffuse ST changes | NL LV Fx PE | NA | NA | 6 |
| 10. 16 M [10] | 2nd | 2 | NA | Chest pain | ↑ | ↑ | Diffuse ST changes | LV Fx ↓ | NA | NA | 6 |
| 11. 16 M [10] | 2nd | 3 | + | Chest pain Nausea | ↑ | ↑ | ST↑ | NL LV Fx PE | NA | NA | 4 |
| 12. 17 M [10] | 2nd | 1 | + | Chest pain Headache | ↑ | ↑ | ST↓ | NL LV Fx | NA | NA | 5 |
| 13. 16 M [10] | 1st | 2 | + | Chest pain Fever Dyspnea | ↑ | ↑ | ST↑ | NL LV Fx | NA | NA | 5 |
| 14. 17 M [10] | 2nd | 3 | + | Chest pain Dyspnea | ↑ | ↑ | NL | NL LV Fx | NA | NA | 3 |
| 15. 28 M [11] | Janssen | 5 | NA | Chest pain | NA | NA | ST↑ | LV Fx ↓ | LGE + | NA | NA |
| 16. 39 M [9] | 2nd | 3 | NA | Chest pain Dyspnea | NA | NA | Inverted T wave | RV Fx ↓ | LGE+ | NA | NA |
| 17. 39 M [11] | 2nd | 4 | NA | Fever Chest pain Dyspnea | NA | NA | NL | NL LV Fx | LGE+ | NA | NA |
| 18. 24 M [11] | 1st | 7 | NA | Chest pain | NA | NA | NL | NL LV Fx | Edema+ LGE+ | NA | NA |
| 19. 19 M [11] | 2nd | 2 | NA | Chest pain | NA | NA | Non-spec. ST changes | NL LV Fx | LGE+ | NA | NA |
| 20. 20 M [11] | 2nd | 3 | NA | Chest pain | NA | NA | ST↑ | LV Fx ↓ | LGE+ | NA | NA |
| 21. 23 M [11] | 2nd | 3 | NA | Fever Chest pain | NA | NA | Diffuse ST changes | NA | LGE+ | NA | NA |
| 22. 22 M [12] | 2nd | 3 | NA | Fever Chest pain | ↑ | ↑ | Diffuse ST↑ | LV Fx ↓ | LGE+ | NSAID Prednisone | NA |
| 23. 31 M [12] | 2nd | 3 | NA | Fever Chest pain Dyspnea | ↑ | ↑ | NL | LV Fx ↓ | LGE+ | No | NA |
| 24. 40 M [12] | 1st | 2 | NA | Chest pain | ↑ | ↑ | Diffuse ST changes | LV Fx ↓ | LGE+ | Prednisone Colchicine | NA |
| 25. 56 M [12] | 2nd | 3 | NA | Chest pain | ↑ | ↑ | Peak T waves | NL LV Fx | LGE+ | Np | NA |
| 26. 26 M [12] | 2nd | 3 | NA | Fever, cough Chest pain | NA | ↑ | ST↑ | LV Fx ↓ | LGE+ PE | Colchicine | 2 |
| 27. 35 M [12] | 2nd | 2 | NA | Fever Chest pain | ↑ | ↑ | Diffuse ST changes | LV Fx ↓ | Edema LGE+ | NSAID | 4 |
| 28. 21 M [12] | 2nd | 4 | NA | Fever Chest pain | ↑ | ↑ | Diffuse ST changes | LV Fx ↓ | Edema LGE+ | NSAID | NA MCS NS VT |
| 29. 22 M [12] | 2nd | 4 | NA | Chest pain | ↑ | ↑ | Diffuse ST changes | LV Fx ↓ | Edema LGE+ | NA | NA NS VT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Das, B.B.; Moskowitz, W.B.; Taylor, M.B.; Palmer, A. Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far? Children 2021, 8, 607. https://doi.org/10.3390/children8070607
Das BB, Moskowitz WB, Taylor MB, Palmer A. Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far? Children. 2021; 8(7):607. https://doi.org/10.3390/children8070607
Chicago/Turabian StyleDas, Bibhuti B., William B. Moskowitz, Mary B. Taylor, and April Palmer. 2021. "Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far?" Children 8, no. 7: 607. https://doi.org/10.3390/children8070607
APA StyleDas, B. B., Moskowitz, W. B., Taylor, M. B., & Palmer, A. (2021). Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far? Children, 8(7), 607. https://doi.org/10.3390/children8070607