Pediatric Fatty Liver and Obesity: Not Always Just a Matter of Non-Alcoholic Fatty Liver Disease

 and
and
Abstract
1. Introduction
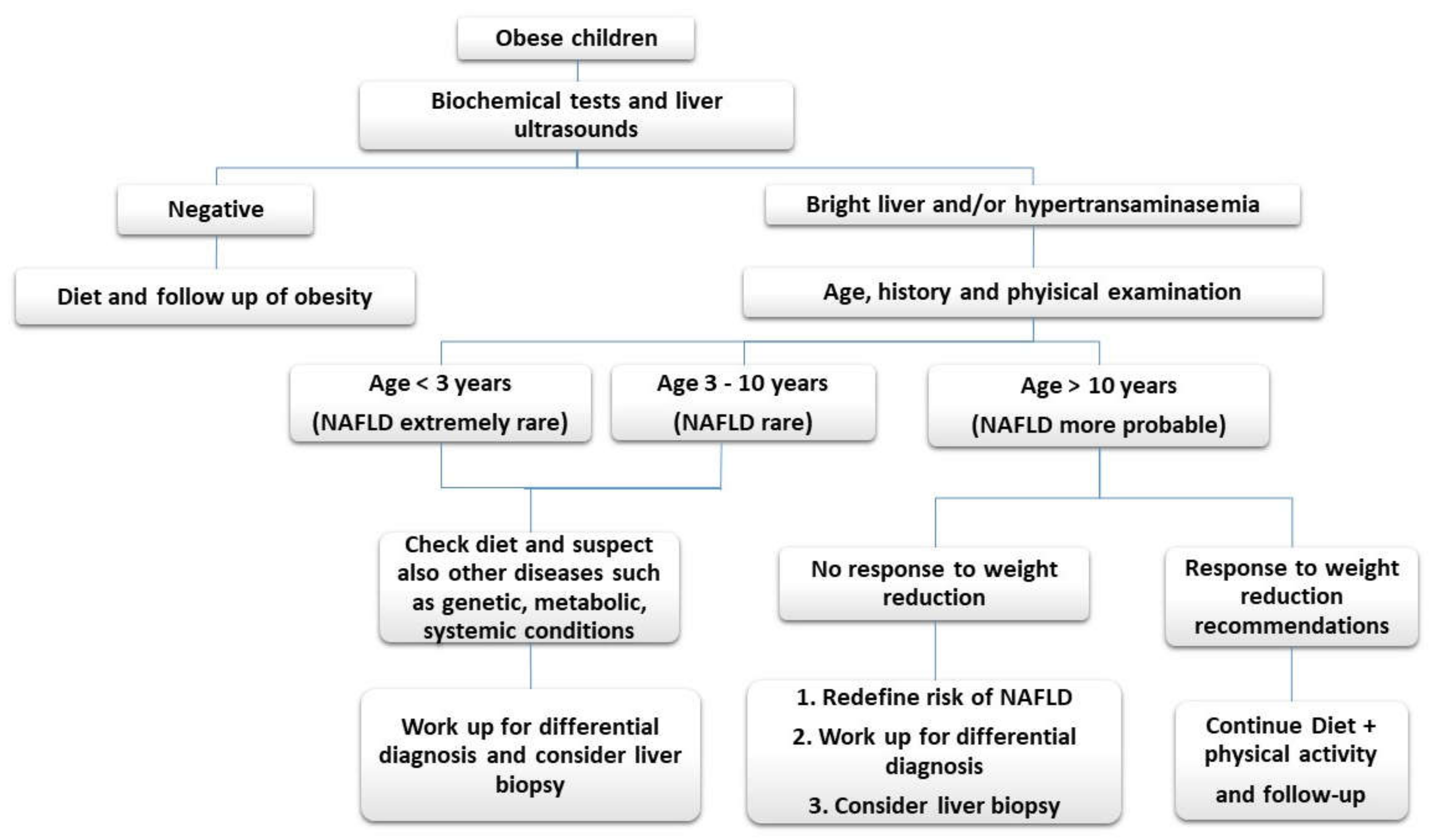
2. NAFLD
- a.
- not being in the classical age range for NAFLD, and
- b.
- being in the classical age range but with abnormalities in liver tests or hepatic ultrasounds not corresponding satisfactorily to a weight loss obtained by dietary/physical activity measures.
- a.
- NAFLD usually does not occur in extremely young children (those younger than 3 years) and it is rare in children younger than 10 years. In these cases, however, the coexistence of central adiposity (waist circumference >90th percentile), elevated body mass index(BMI) (>85th percentile), clinical or laboratory signs of insulin resistance, family history of NAFLD or type 2 diabetes mellitus (DM), and a sedentary lifestyle may be indicative of NAFLD [2].
- b.
- early onset liver steatosis (for those <5 years of age) or clinical phenotypes of acute liver failure, neonatal conjugated jaundice, or large organomegaly are indicative of liver diseases other than NAFLD.
3. Genetic and Metabolic Disorders
3.1. Urea Cycle Disorders
3.2. Citrin Deficiency
3.3. Glycogenosis (Glycogen Storage Diseases(GSD))
3.4. Hereditary Fructose Intolerance
3.5. Congenital Disorders of Glycosylation (CDG)
3.6. Cholesteryl Ester Storage (CESD)
3.7. Abetalipoproteinemia/hypobetalipoproteinemia
3.8. Alpha-1 Antitrypsin Deficiency(A1AT)
3.9. Wilson’s Disease (WD)
3.10. Cystic Fibrosis (CF)
3.11. Shwachman-Diamond Syndrome (SDS)
3.12. Down Syndrome
3.13. Turner Syndrome
4. Gastrointestinal and Nutritional Diseases
4.1. Celiac Disease
4.2. Inflammatory Bowel Diseases (IBD)
4.3. Malnutrition
5. Endocrine Diseases
5.1. Diabetes Mellitus
5.2. Hypothyroidism
5.3. Hypothalamic Diseases
6. Hepatitis
6.1. Chronic Viral Hepatitis
6.2. Autoimmune Hepatitis (AIH)
7. Iatrogenic Causes
7.1. Alcohol Consumption
7.2. Toxic Substances
7.3. Drug Toxicity
8. Myopathies
9. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2017. Available online: https://www.cdc.gov/nchs/products/databriefs/db288.htm (accessed on 13 December 2018).
- Vajro, P.; Lenta, S.; Socha, P.; Dhawan, A.; McKiernan, P.; Baumann, U.; Durmaz, O.; Lacaille, F.; McLin, V.; Nobili, V. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: Position paper of the ESPGHAN Hepatology Committee. J. Pediatr. Gastr. Nutr. 2012, 54, 700–713. [Google Scholar] [CrossRef]
- Braissant, O. Current concepts in the pathogenesis of urea cycle disorders. Mol. Genet. Metab. 2010, 100, S3–S12. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, R.C.; Lam, C.; Wong, D.; Cederbaum, S.; Sokol, R.J. Significant hepatic involvement in patients with ornithine transcarbamylase deficiency. J. Pediatr. 2014, 164, 720–725. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Yazaki, M.; Tanaka, N.; Sano, K.; Hashimoto, E.; Takei, Y.I.; Song, Y.Z.; Tanaka, E.; Kiyosawa, K.; Saheki, T.; et al. Citrin deficiency as a cause of chronic liver disorder mimicking non-alcoholic fatty liver disease. J. Hepatol. 2008, 49, 810–820. [Google Scholar] [CrossRef]
- Vajro, P.; Veropalumbo, C. Citrin deficiency: Learn more, and don’t forget to add it to the list of neonatal cholestasis and the NASH trash bin. J. Pediatr. Gastr. Nutr. 2010, 50, 578–579. [Google Scholar] [CrossRef] [PubMed]
- Kishnani, P.S.; Austin, S.L.; Arn, P.; Bali, D.S.; Boney, A.; Case, L.E.; Chung, W.K.; Desai, D.M.; El-Gharbawy, A.; Haller, R.; et al. Glycogen storage disease type III diagnosis and management guidelines. Genet. Med. 2010, 12, 446. [Google Scholar] [CrossRef] [PubMed]
- Shieh, J.J.; Lu, Y.H.; Huang, S.W.; Huang, Y.H.; Sun, C.H.; Chiou, H.J.; Liu, C.; Lo, M.Y.; Lin, C.Y.; Niu, D.M. Misdiagnosis as steatohepatitis in a family with mild glycogen storage disease type 1a. Gene 2012, 509, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Ciacci, C.; Gennarelli, D.; Esposito, G.; Tortora, R.; Salvatore, F.; Sacchetti, L. Hereditary fructose intolerance and celiac disease: A novel genetic association. Clin. Gastroenterol. Hepatol. 2006, 4, 635–638. [Google Scholar] [CrossRef]
- Marques da Silva, D.; Dos Reis Ferreira, V.; Monticelli, M.; Janeiro, P.; Videira, P.A.; Witters, P.; Jaeken, J.; Cassiman, D. Liver involvement in congenital disorders of glycosylation (CDG). A systematic review of the literature. J. Inherit. Metab. Dis. 2017, 40, 195–207. [Google Scholar] [CrossRef]
- Vajro, P.; Zielinska, K.; Ng, B.G.; Maccarana, M.; Bengtson, P.; Poeta, M.; Mandato, C.; D’Acunto, E.; Freeze, H.H.; Eklund, E.A. Three unreported cases of TMEM199-CDG, a rare genetic liver disease with abnormal glycosylation. Orphanet. J. Rare Dis. 2018, 13, 4. [Google Scholar] [CrossRef]
- Bernstein, D.L.; Hülkova, H.; Bialer, M.G.; Desnick, R.J. Cholesteryl ester storage disease: Review of the findings in 135 reported patients with an underdiagnosed disease. J. Hepatol. 2013, 58, 1230–1243. [Google Scholar] [CrossRef] [PubMed]
- Himes, R.W.; Barlow, S.E.; Bove, K.; Quintanilla, N.M.; Sheridan, R.; Kohli, R. Lysosomal acid lipase deficiency unmasked in two children with nonalcoholic fatty liver disease. Pediatrics 2016, 138, e20160214. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, R.; Deheragoda, M.; Fitzpatrick, E.; Dhawan, A. Pediatric Fatty Liver Disease (PeFLD): All is not NAFLD-pathophysiological insights and approach to management. J. Hepatol. 2018, 68, 1286–1299. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Hegele, R.A. Abetalipoproteinemia and homozygous hypobetalipoproteinemia: A framework for diagnosis and management. J. Inherit. Metab. Dis. 2014, 37, 333–339. [Google Scholar] [CrossRef]
- Fairbanks, K.D.; Tavill, A.S. Liver disease in alpha 1-antitrypsin deficiency: A review. Am. J. Gastroenterol. 2008, 103, 2136. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.; Inada, N.; Izumi, A.; Kawanaka, M.; Kobashi, H.; Yamada, G. Wilson’s disease masquerading as nonalcoholic steatohepatitis. N. Am. J. Med. Sci. 2009, 1, 74. [Google Scholar]
- Vajro, P.; Maddaluno, S.; Veropalumbo, C. Persistent hypertransaminasemia in asymptomatic children: A stepwise approach. World J. Gastroenterol. 2013, 19, 2740. [Google Scholar] [CrossRef]
- Socha, P.; Janczyk, W.; Dhawan, A.; Baumann, U.; D’Antiga, L.; Tanner, S.; Iorio, R.; Vajro, P.; Houwen, R.; Fischler, B.; et al. Wilson’s Disease in Children: A Position Paper by the Hepatology Committee of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 334–344. [Google Scholar] [CrossRef]
- Staufer, K.; Halilbasic, E.; Trauner, M.; Kazemi-Shirazi, L. Cystic fibrosis related liver disease—Another black box in hepatology. Int. J. Mol. Sci. 2014, 15, 13529–13549. [Google Scholar] [CrossRef]
- Resti, M.; Lami, C.A.; Tucci, F.; Mannelli, F.; Rossi, M.E.; Azzari, C.; Vierucci, A. False diagnosis of non-A/non-B hepatitis hiding two cases of cystic fibrosis. Eur. J. Pediatr. 1990, 150, 97–99. [Google Scholar] [CrossRef]
- Toiviainen-Salo, S.; Durie, P.R.; Numminen, K.; Heikkilä, P.; Marttinen, E.; Savilahti, E.; Mäkitie, O. The Natural History of Shwachman-Diamond Syndrome–Associated Liver Disease from Childhood to Adulthood. J. Pediatr. 2009, 155, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Veropalumbo, C.; Campanozzi, A.; De Gregorio, F.; Correra, A.; Raia, V.; Vajro, P. Shwachman-Diamond syndrome with autoimmune-like liver disease and enteropathy mimicking celiac disease. Clin. Res. Hepatol. Gastroenterol. 2015, 39, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Bertapelli, F.; Pitetti, K.; Agiovlasitis, S.; Guerra-Junior, G. Overweight and obesity in children and adolescents with Down syndrome—Prevalence, determinants, consequences, and interventions: A literature review. Res. Dev. Disabil. 2016, 57, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Valentini, D.; Alisi, A.; Di Camillo, C.; Sartorelli, M.R.; Crudele, A.; Bartuli, A.; Nobili, V.; Villani, A. Nonalcoholic Fatty Liver Disease in Italian Children with Down Syndrome: Prevalence and Correlation with Obesity-Related Features. J. Pediatr. 2017, 189, 92–97. [Google Scholar] [CrossRef] [PubMed]
- De Matteo, A.; Vajro, P. Down Syndrome and Pediatric Nonalcoholic Fatty Liver Disease: A Causal or Casual Relationship? J. Pediatr. 2017, 189, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Parola, M.; Vajro, P. Nocturnal hypoxia in obese-related obstructive sleep apnea as a putative trigger of oxidative stress in pediatric NAFLD progression. J. Hepatol. 2016, 65, 470–472. [Google Scholar] [CrossRef]
- Roulot, D. Liver involvement in Turner syndrome. Liver Int. 2013, 33, 24–30. [Google Scholar] [CrossRef]
- Salerno, M.; Di Maio, S.; Gasparini, N.; Rizzo, M.; Ferri, P.; Vajro, P. Liver abnormalities in Turner syndrome. Eur. J. Pediatr. 1999, 158, 618–623. [Google Scholar] [CrossRef]
- Vajro, P.; Paolella, G.; Pisano, P.; Maggiore, G. Hypertransaminasemia and coeliac disease. Aliment. Pharm. Ther. 2012, 35, 202–203. [Google Scholar] [CrossRef]
- Marciano, F.; Savoia, M.; Vajro, P. Celiac disease-related hepatic injury: Insights into associated conditions and underlying pathomechanisms. Digest. Liver Dis. 2016, 48, 112–119. [Google Scholar] [CrossRef]
- Vajro, P.; Paolella, G.; Maggiore, G.; Giordano, G. Pediatric celiac disease, cryptogenic hypertransaminasemia, and autoimmune hepatitis. J. Pediatr. Gastr. Nutr. 2013, 56, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Franzese, A.; Iannucci, M.P.; Valerio, G.; Ciccimarra, E.; Spaziano, M.; Mandato, C.; Vajro, P. Atypical celiac disease presenting as obesity-related liver dysfunction. J. Pediatr. Gastroenterol. Nutr. 2001, 33, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Caprai, S.; Vajro, P.; Ventura, A.; Sciveres, M.; Maggiore, G. SIGENP Study Group for Autoimmune Liver Disorders in Celiac Disease. Autoimmune liver disease associated with celiac disease in childhood: A multicenter study. Clin. Gastroenterol. Hepatol. 2008, 6, 803–806. [Google Scholar] [CrossRef] [PubMed]
- Restellini, S.; Chazouillères, O.; Frossard, J.L. Hepatic manifestations of inflammatory bowel diseases. Liver Int. 2017, 37, 475–489. [Google Scholar] [CrossRef] [PubMed]
- Bessissow, T.; Le, N.H.; Rollet, K.; Afif, W.; Bitton, A.; Sebastiani, G. Incidence and predictors of nonalcoholic fatty liver disease by serum biomarkers in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2016, 22, 1937–1944. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.E.; Jones, P.; Long, M.D.; Barritt, A.S., IV. Changing shape of disease: Nonalcoholic fatty liver disease in Crohn’s disease—A case series and review of the literature. Inflamm. Bowel Dis. 2012, 18, 49–54. [Google Scholar] [CrossRef]
- Mehler, P.S.; Brown, C. Anorexia nervosa–medical complications. Int. J. Eat. Disord. 2015, 3, 11. [Google Scholar] [CrossRef]
- Rosen, E.; Bakshi, N.; Watters, A.; Rosen, H.R.; Mehler, P.S. Hepatic complications of anorexia nervosa. Digest. Dis. Sci. 2017, 62, 2977–2981. [Google Scholar] [CrossRef]
- Nadeau, K.J.; Klingensmith, G.; Zeitler, P. Type 2 diabetes in children is frequently associated with elevated alanine aminotransferase. J. Pediatr. Gastr. Nutr. 2005, 41, 94–98. [Google Scholar] [CrossRef]
- Mandato, C.; D’Acunzo, I.; Vajro, P. Thyroid dysfunction and its role as a risk factor for non-alcoholic fatty liver disease: what’s new. Dig. Liver Dis. 2018, 50, 1163–1165. [Google Scholar] [CrossRef]
- Jung, D.; Seo, G.H.; Kim, Y.M.; Choi, J.H.; Yoo, H.W. Hepatopulmonary syndrome caused by hypothalamic obesity and nonalcoholic fatty liver disease after surgery for craniopharyngioma: A case report. Ann. Pediatr. Endocrinol. Metab. 2018, 23, 51. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, A.; Bootsveld, K.; Gebhardt, U.; Daubenbüchel, A.M.; Sterkenburg, A.S.; Müller, H.L. Nonalcoholic fatty liver disease and fatigue in long-term survivors of childhood-onset craniopharyngioma. Eur. J. Endocrinol. 2015, 173, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Pokorska-Śpiewak, M.; Kowalik-Mikołajewska, B.; Aniszewska, M.; Pluta, M.; Walewska-Zielecka, B.; Marczyńska, M. Liver steatosis in children with chronic hepatitis B and C: Prevalence, predictors, and impact on disease progression. Medicine 2017, 96, e5832. [Google Scholar] [CrossRef] [PubMed]
- Mateos-Lindemann, M.L.; Diez-Aguilar, M.; Galdamez, A.L.; Galán, J.C.; Moreno, A.; Pérez-Gracia, M.T. Patients infected with HIV are at high-risk for hepatitis E virus infection in Spain. J. Med. Virol. 2014, 86, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, Y.; Hokari, A. Autoimmune hepatitis: Current challenges and future prospects. Clin. Exp. Gastroenterol. 2017, 10, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Weiler-Normann, C.; Lohse, A.W. Nonalcoholic Fatty Liver Disease in Patients with Autoimmune Hepatitis: Further Reason for Teeth GNASHing? Digest. Dis. Sci. 2016, 61, 2462–2464. [Google Scholar] [CrossRef] [PubMed]
- Morean, M.E.; Kong, G.; Camenga, D.R.; Cavallo, D.A.; Connell, C.; Krishnan-Sarin, S. First drink to first drunk: Age of onset and delay to intoxication are associated with adolescent alcohol use and binge drinking. Alcohol. Clin. Exp. Res. 2014, 38, 2615–2621. [Google Scholar] [CrossRef]
- Llerena, S.; Arias-Loste, M.T.; Puente, A.; Cabezas, J.; Crespo, J.; Fábrega, E. Bingedrinking: Burden of liver disease and beyond. World J. Hepatol. 2015, 7, 2703–2715. [Google Scholar] [CrossRef]
- Danan, G.; Teschke, R. RUCAM in drug and herb induced liver injury: An update. Int. J. Mol. Sci. 2015, 17, 14. [Google Scholar] [CrossRef]
- Molleston, J.P.; Fontana, R.J.; Lopez, M.J.; Kleiner, D.E.; Gu, J.; Chalasani, N. Drug-Induced Liver Injury Network. Characteristics of idiosyncratic drug-induced liver injury in children: Results from the DILIN prospective study. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 182–189. [Google Scholar] [CrossRef]
- Bessone, F.; Dirchwolf, M.; Rodil, M.A.; Razori, M.V.; Roma, M.G. Review article: Drug-induced liver injury in the context of nonalcoholic fatty liver disease—A physiopathological and clinical integrated view. Aliment. Pharmacol. Ther. 2018, 48, 892–913. [Google Scholar] [CrossRef] [PubMed]
- Massart, J.; Begriche, K.; Moreau, C.; Fromenty, B. Role of nonalcoholic fatty liver disease as risk factor for drug-induced hepatotoxicity. J. Clin. Transl. Res. 2017, 3, 212–232. [Google Scholar]
- Farinelli, E.; Giampaoli, D.; Cenciarini, A.; Cercado, E.; Verrotti, A. Valproic acid and non-alcoholic fatty liver disease: A possible association? World J. Hepatol. 2015, 7, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Paolella, G.; Pisano, P.; Albano, R.; Cannaviello, L.; Mauro, C.; Esposito, G.; Vajro, P. Fatty liver disease and hypertransaminasemia hiding the association of clinically silent Duchenne muscular dystrophy and hereditary fructose intolerance. Ital. J. Pediatr. 2012, 38, 64. [Google Scholar] [CrossRef] [PubMed]
- Veropalumbo, C.; Del Giudice, E.; Capuano, G.; Gentile, C.; Di Cosmo, N.; Vajro, P. Duchenne and Becker muscular dystrophy presenting as nonalcoholic fatty liver disease. J. Pediatr. Gastr. Nutr. 2011, 53, 463–464. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.L.; Connor, E.L.; Wolfgram, P.M.; Eickhoff, J.C.; Reeder, S.B.; Allen, D.B. Predicting hepatic steatosis in a racially and ethnically diverse cohort of adolescent girls. J. Pediatr. 2014, 165, 319–325. [Google Scholar] [CrossRef]
- Vos, M.B.; Lavine, J.E. Dietary fructose in nonalcoholic fatty liver disease. Hepatology 2013, 57, 2525–2531. [Google Scholar] [CrossRef]
- Dasarathy, S.; Dasarathy, J.; Khiyami, A.; Joseph, R.; Lopez, R.; McCullough, A.J. Validity of real time ultrasound in the diagnosis of hepatic steatosis: A prospective study. J. Hepatol. 2009, 51, 1061–1067. [Google Scholar] [CrossRef]
- Shannon, A.; Alkhouri, N.; Carter-Kent, C.; Monti, L.; Devito, R.; Lopez, R.; Feldstein, A.E.; Nobili, V. Ultrasonographic quantitative estimation of hepatic steatosis in children with nonalcoholic fatty liver disease (NAFLD). J. Pediatr. Gastr. Nutr. 2011, 53, 190. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, J.M.; Han, J.K.; Lee, J.Y.; Lee, K.H.; Han, C.J.; Jo, J.Y.; Yi, N.J.; Suh, K.S.; Shin, K.S.; et al. Hepatic macrosteatosis: Predicting appropriateness of liver donation by using MR imaging—Correlation with histopathologic findings. Radiology 2006, 240, 116–129. [Google Scholar] [CrossRef]
- Bohte, A.E.; van Werven, J.R.; Bipat, S.; Stoker, J. The diagnostic accuracy of US, CT, MRI and 1H-MRS for the evaluation of hepatic steatosis compared with liver biopsy: A meta-analysis. Eur. Radiol. 2011, 21, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Hudert, C.A.; Tzschätzsch, H.; Rudolph, B.; Bläker, H.; Loddenkemper, C.; Müller, H.P.; Henning, S.; Bufler, P.; Hamm, B.; Braun, J.; et al. Tomoelastography for the Evaluation of Pediatric Nonalcoholic Fatty Liver Disease. Investig. Radiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.B.; Abrams, S.H.; Barlow, S.E.; Caprio, S.; Daniels, S.R.; Kohli, R.; Mouzaki, M.; Sathya, P.; Schwimmer, J.B.; Sundaram, S.S.; et al. NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 319–334. [Google Scholar] [PubMed]
- Molleston, J.P.; Schwimmer, J.B.; Yates, K.P.; Murray, K.F.; Cummings, O.W.; Lavine, J.E.; Brunt, E.M.; Scheimann, A.O.; Unalp-Arida, A. NASH Clinical Research Network. Histological abnormalities in children with nonalcoholic fatty liver disease and normal or mildly elevated alanine aminotransferase levels. J. Pediatr. 2014, 164, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Vuppalanchi, R.; Unalp, A.; Van Natta, M.L.; Cummings, O.W.; Sandrasegaran, K.E.; Hameed, T.; Tonascia, J.; Chalasani, N. Effects of liver biopsy sample length and number of readings on sampling variability in nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Harwood, J.; Bishop, P.; Liu, H.; Nowicki, M. Safety of Blind Percutaneous Liver Biopsy in Obese Children a Retrospective Analysis. J. Clin. Gastroenterol. 2010, 44, e253–e255. [Google Scholar] [CrossRef]
- Mancini, M.; Summers, P.; Faita, F.; Brunetto, M.R.; Callea, F.; De Nicola, A.; Di Lascio, N.; Farinati, F.; Gastaldelli, A.; Gridelli, B.; et al. Digital liver biopsy: Bio-imaging of fatty liver for translational and clinical research. World J. Hepatol. 2018, 10, 231–245. [Google Scholar] [CrossRef]


{kind=link}
| Gastrointestinal/Nutritional/ Endocrine/Hepatic Causes | Genetic and Metabolic Causes | Toxics and Drugs |
|---|---|---|
| Celiac disease | α- and β-oxidation defects | Cocaine |
| Inflammatory bowel disease | Abeta or hypobetalipoproteinemia | Ecstasy |
| Anorexia nervosa | Cholesterol ester storage disease | Ethanol |
| Obesity | Citrin deficiency | Pesticides |
| Severe malnutrition | Cystic fibrosis | Solvents |
| Diabetes mellitus type 1 | Glycogen storage disease | Amiodarone |
| Hypothalamic-pituitary disorders | Hereditary fructose intolerance | Antiretroviral drugs |
| Hypothyroidism | Mitochondrial and peroxisomal defects | Aspirin |
| Polycystic ovary syndrome | Shwachman-Diamond syndrome | Glucocorticoids |
| Autoimmune hepatitis | Turner syndrome | Methotrexate |
| Viral hepatitis | Urea cycle disorders | Sodium valproate |
| Wilson’s disease | Tetracycline |
| 1st Step | 2nd Step |
|---|---|
| Blood counts and standard liver function tests (AST, ALT, GGT, coagulation, bilirubin, total protein and electrophoresis, total Ig) | Clinically oriented hormonal tests (e.g. cortisol) |
| Lipid profile, glucose, insulin (eventually OGTT) | Serum copper, 24h urinary copper |
| FT3, FT4,TSH | Sweat test/molecular test for CFTR |
| EMA, tTgasiIgA | AMA, SMA, LKM, LC1 |
| Viral markers (HBV, HCV) | A1-antitrypsin |
| Ceruloplasmin | Amino and organic acids, acyl carnitine profile, serum lactate, ammonium, CDG and LAL test, urinary reducing substances |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfani, R.; Vassallo, E.; De Anseris, A.G.; Nazzaro, L.; D'Acunzo, I.; Porfito, C.; Mandato, C.; Vajro, P. Pediatric Fatty Liver and Obesity: Not Always Just a Matter of Non-Alcoholic Fatty Liver Disease. Children 2018, 5, 169. https://doi.org/10.3390/children5120169
Alfani R, Vassallo E, De Anseris AG, Nazzaro L, D'Acunzo I, Porfito C, Mandato C, Vajro P. Pediatric Fatty Liver and Obesity: Not Always Just a Matter of Non-Alcoholic Fatty Liver Disease. Children. 2018; 5(12):169. https://doi.org/10.3390/children5120169
Chicago/Turabian StyleAlfani, Renata, Edoardo Vassallo, Anna Giulia De Anseris, Lucia Nazzaro, Ida D'Acunzo, Carolina Porfito, Claudia Mandato, and Pietro Vajro. 2018. "Pediatric Fatty Liver and Obesity: Not Always Just a Matter of Non-Alcoholic Fatty Liver Disease" Children 5, no. 12: 169. https://doi.org/10.3390/children5120169
APA StyleAlfani, R., Vassallo, E., De Anseris, A. G., Nazzaro, L., D'Acunzo, I., Porfito, C., Mandato, C., & Vajro, P. (2018). Pediatric Fatty Liver and Obesity: Not Always Just a Matter of Non-Alcoholic Fatty Liver Disease. Children, 5(12), 169. https://doi.org/10.3390/children5120169