Abstract
Inflammatory bowel disease (IBD) comprises a group of relapsing, chronic diseases of the gastrointestinal tract that, in addition to adults, can affect children and adolescents. To detect relapses of inflammation, these patients require close observation, frequent follow-up, and therapeutic adjustments. While reference standard diagnostics include anamnestic factors, laboratory and stool sample assessment, performing specific imaging in children and adolescents is much more challenging than in adults. Endoscopic and classic cross-sectional imaging modalities may be invasive and often require sedation for younger patients. For this reason, intestinal ultrasound (IUS) is becoming increasingly important for the non-invasive assessment of the intestine and its inflammatory affection. In this review, we would like to shed light on the current state of the art and provide an outlook on developments in this field that could potentially spare these patients more invasive follow-up procedures.
1. Introduction
Crohn’s disease (CD) and ulcerative colitis (UC) are chronic, relapsing inflammatory conditions of the gastrointestinal tract [1]. The exact etiology and pathogenesis of such inflammatory bowel diseases (IBDs) remain not completely understood [2]. An underlying unregulated inflammatory immune response and interaction with the intestinal microbiota in genetically predisposed individuals is hypothesized [3,4]. Exogenous environmental influences and the composition of the intestinal microbiome also play a role in disease development [5]. IBDs in children and adolescents often have unusual manifestations, are exhibited more frequently, and are usually more severe and more difficult to treat [6]. Disease progression occurs in 31 or 49% of pediatric patients with CD or UC, respectively, while stable localization is observed in 90 or 80% of patients with first manifestation in adulthood.
For example, the increase in activity during the first years of the disease, the need for immunosuppressive therapy, and the need for surgery are significantly higher in pediatric IBD than in adult patients [6].
CD can be localized throughout the gastrointestinal (GI) tract and is characterized by segmental, discontinuous involvement and inflammatory changes affecting all layers of the intestinal wall [7]. Initial clinical symptoms are often nonspecific and include abdominal pain, usually bloodless diarrhea, weight loss, and fever. Especially in children, an appendicitis-like clinical picture may present if the terminal ileum is affected. More commonly than in adults, 51% of pediatric CD patients show an affection of the upper gastrointestinal tract, with the anatomic extent increasing in 39% of patients within 2 years [8].
In contrast, UC affects the distal rectum and continuously spreads orally. The clinical symptoms are often bloody, mucopurulent diarrhea accompanied by fever and abdominal pain, which often occurs as tenesmus in the left lower abdomen before defecation [9]. Symptoms ranging from bleeding with iron deficiency and anemia to massive blood loss and a dilated toxic megacolon with risk of developing peritonitis, sepsis, and perforation are among the major intestinal complications [10]. In childhood, about two thirds of patients display pancolitis upon manifestation of UC [11]. Macroscopically, the clinical picture is characterized by extensive redness and swelling of the mucosa with contact hemorrhages and, during the course of the disease, the formation of inflammatory pseudopolyps. Besides affecting intestinal organs, CD and UC may present with extraintestinal manifestations including affection of the skin, eyes, joints, and liver. Such manifestations include erythema nodosum, conjunctivitis, arthritis, and primary sclerosing cholangitis (PSC) [12].
The current therapeutic strategies include modulation of the immune system and targeting of major cytokine pathways [13,14]. Some examples are blocking agents of pro-inflammatory tumor necrosis factor alpha (TNFα) [15], leucocyte adhesion molecules such as α4β7-Integrin or signal kinases [16], and inhibitor of T-cell Janus kinases (JAKs) [17].
In both Western industrialized and developing countries, an increase in the prevalence and incidence of IBD has been observed in recent decades [18,19,20]. This trend can also be observed in pediatric patients, along with an increasingly early onset of disease in this group [11,21]. In approximately 20–30% of all affected patients, IBD manifests in childhood [11]. In Germany, the incidence of CD is estimated to be 6.6 per 100,000 habitants, with a prevalence of approximately 100–200, while the incidence of UC is reported to be 3.0–3.9, with a prevalence at approximately 160–250 [22]. The diagnosis of IBD is based on a synopsis of history, clinical examination findings, imaging results, endoscopy with histology, and laboratory values (so-called Porto diagnostic criteria) [23,24,25]. Generally, the incidence of IBDs may increase with age, and the peak incidence is around 14 to 15 years, as reported in a large European cohort [26]. As intestinal ultrasound (IUS) is an emerging non-invasive point-of-care tool for accurately detecting and monitoring disease activity [27,28,29,30,31], this narrative review article will provide current state-of-the-art and novel developments in the field of non-invasive imaging of the intestine in pediatric IBD.
2. Diagnostic Imaging and Surveillance Approaches in Pediatric IBD
IBDs are often challenging, both from a diagnostic and therapeutic point of view. While deep-seated anatomic structures are difficult to assess via US alone, diagnostic imaging also includes magnetic resonance imaging (MRI). Commonly, oral mannitol administration is used—termed magnetic resonance enterography (MRE)—in order to better visualize the small intestine [23] and pelvic MRI to assess anal fistulas or perianal abscesses. However, the evaluation of the upper GI-tract (stomach and duodenum) is difficult via IUS. In comparison to US where data is scarce, MRE shows good performance in detecting IBD in pediatric patients [32]. A meta-analysis in 687 patients demonstrated a sensitivity of 83% and specificity of 93% for the detection of active inflammation with known or suspected IBD [33]. Therefore, MRI/MRE has its value in establishing the diagnosis and providing support in distinguishing between CD and UC. Likewise, gastrointestinal endoscopy is invasive, expensive, and time-consuming. In contrast, US is safe, fast, and cheap, and does not require any anesthesia, while it can be used both for monitoring children with IBD and for children suspected of having IBD [34]. With respect to very young patients (very early onset, VEO-IBD), the European Society of Paediatric Radiology abdominal imaging task force recommends the first-line use of US [35]. MRE is used for further work-ups in the case of unclear US findings, while the use of computed tomography techniques is limited to specific situations. In the adult IBD context, gastrointestinal endoscopy and MRE are the gold standard tests to establish a diagnosis for IBD (Porto criteria) [36]. Consequently, the evaluation and monitoring of disease activity may be complemented by using US.
Intestinal US is teachable to healthcare physicians in a training curriculum for instance, and is then able to bring at least moderate diagnostic accuracy while not having to be exclusively performed by experienced radiologists [37]. However, there is a lack of consensus on how a specific training curriculum for children should look. Moreover, US is generally well accepted by pediatric patients, and therefore, their preferred diagnostic modality [38,39].
3. US in Pediatric Inflammatory Bowel Disease
3.1. US Anatomy of the Intestinal Wall
Intestinal US, especially in pediatrics, is performed with frequency transducers, typically in the range of 7.5–17 MHz. In almost all cases, supine positioning of the patient is recommended [40]. This way, the intestinal wall presents with a typical layered anatomy (Figure 1, Table 1) [41]. In addition, ultrasound as a dynamic examination provides important information in real time on the dynamics of intestinal activity in terms of peristalsis and lumen width. In addition, color Doppler enables the visualization of increased perfusion in inflamed segments of the intestine.
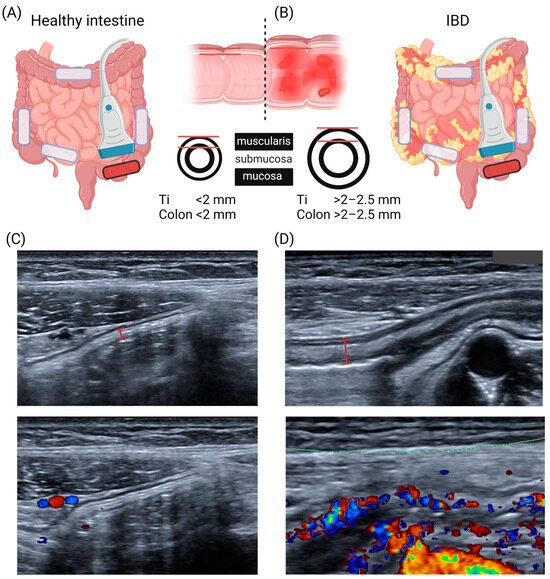
Figure 1.
Ultrasound for assessment of inflammatory bowel diseases (A,B) Schematic cartoon of standard imaging locations for disease activity assessment in inflammatory bowel diseases as follows: terminal ileum and ascending, transverse, descending, and sigmoid colon. In healthy subjects, the intestinal wall of the terminal ileum/colon is thinner than 2 mm and it exceeds 2–2.5 mm in inflamed segments in IBD patients. (C,D) Exemplary B-mode and color Doppler images of healthy and inflamed segments of the sigmoid colon with exemplary bowel wall measurements. Displayed is a healthy child and one pediatric patient with UC. B-mode images show enlarged submucosa in the UC patient with increased blood flow measured by color Doppler. IBD = inflammatory bowel disease, Ti = terminal ileum. Created with https://www.biorender.com/ (accessed on 22 January 2024).

Table 1.
Ultrasound anatomy of the intestinal wall (from inside to outside layers), modified from Strobel, Goertz, and Bernatik [41].
Knowledge of regular US anatomy serves as the baseline for physicians in order to use such technologies in IBD diagnostics.
3.2. Current US Information Used in IBD Diagnostics
While endoscopic procedures are generally restricted to the evaluation of the mucosal surface, and histological assessments inevitably take days, abdominal US is more than an adjunct tool in order to assess the inflammation of the intestinal wall [42]. US examinations can immediately provide information on concomitant mesenterial lymphadenopathy and bowel wall thickness (BWT), while Doppler signals are used as surrogates of intestinal blood flow changes and the detection of mesenteric inflammatory fat. Together, these alterations can help in interpreting the extent of severity and in the prediction of disease activity in IBD. The ultrasonographic appearance of Crohn’s disease is characterized by segmental inflammation, asymmetric thickening of the intestinal wall, and transmural inflammation, as depicted by increased perfusion [34].
In cases of long-standing disease, IUS is able to provide additional information, as untreated or insufficiently treated IBD can result in an extensive and circumferential loss of the characteristic tissue layers of the intestinal wall, appearing sonographically as a hypoechoic rim with abrogated stratification. As a result of the fibrofatty alteration of the mesenteric tissue, affected segments tend to be contrasted and fixed without peristalsis with the impression of an abnormal angulation [41]. In cases of chronic inflammatory, active disease, these features may be additionally associated with luminal stenosis, rigid and immobile bowel segments, or even loss of the haustra, e.g., in the colon [41]. Further complications are the development of abscess and/or fistula formations or a mechanical ileus due to pronounced luminal stenosis.
In general, studies using the conventional B-mode US in Crohn’s disease to detect inflammatory lesions at the terminal ileum demonstrated an overall sensitivity of 74–88%, and an overall specificity of 78–93% [43]. For instance, when Canani et al. assessed the effectiveness of ultrasonographic bowel wall measurement in the diagnostic work-up of children with suspected IBD by combining it with established and, to some extent, distinctive laboratory markers, such as the determination of fecal calprotectin, anti-Saccharomyces cerevisiae antibodies, and perinuclear staining antineutrophil antibodies [44], they found that UC-directed bowel wall measurement proved to be an accurate, non-invasive, and reproducible technique for the detection of inflammation localized in the ileum. Their results even led to the interpretation that abdominal US may be used as a primary imaging procedure in children with suspected IBD [34].
However, with respect to the above-described characteristic, but mainly qualitative assessments of alterations of the intestinal bowel and its surrounding anatomical structures, there is a great need for a standardization of the use of US in pediatric IBD patients. To achieve a standardized examination procedure in children, we must defined which criteria in quality and quantity should be taken into account to define an abnormal US in the first place. This poses an important unmet prerequisite, since a recent systematic review on the diagnostic accuracy of IUS showed that to date, no common criteria to define an IUS as abnormal are in use [45]. More interestingly, in adults, there is a so-called expert consensus on the optimal acquisition and development of the International Bowel Ultrasound Segmental Activity Score (IBUS-SAS), identifying four major parameters: bowel wall thickness (BWT); bowel wall stratification; hyperemia of the wall (color Doppler imaging), and inflammatory mesenteric fat [46].
3.3. Bowel Wall Thickness (BWT)
A meta-analysis reported bowel wall thickness values ranging from 0.8 to 1.9 mm in the small bowel and from 1.0 to 1.9 mm in the colon with increasing with age (Table 2) [47].
Table 2.
Pooled mean bowel wall thickness modified from van Wassenaer et al. [47].
This means that BWT assessed via US is mostly reported to be 1.2 mm on average and does not reach values above 2 mm [48,49,50]. In the last twenty years, only a few studies have dealt with the differences in BWT between different categories of disease severity [45]. In contrast to normal measures, the mean value for BWT was 1.7 ± 0.4 mm in remission, 2.4 ± 0.4 in mild, 3.5 ± 0.5 in moderate, and 4.8 ± 0.7 in severe endoscopic disease activity, respectively. In adults, transmural remission in both CD and UC was defined by bowel thickness ≤ 3 mm, and to assess treatment response, a reduction in BWT of over 25% or over 2.0 mm or over 1.0 mm and one color Doppler signal reduction were defined [31]. With regard to such data, the optimal cut-off may be defined as 2–2.5 mm. The findings of another study from Chioran and co-workers demonstrated that children with Crohn’s disease exhibited an increased thickness of the ileocecal intestinal wall (>3 mm) when compared to healthy age-matched subjects (less than 2 mm) [51].
Increased BWT in the presence of hyperemia is frequently seen in both subtypes of IBD. It is thus not always possible to clearly distinguish UC from CD using the B-mode alone [30]. Voogd et al. reported BWT to be an accurate parameter for monitoring treatment response in adult patients receiving tofacitinib treatment [52]. Whether or not this is applicable in younger patients remains to be determined. However, these data require confirmation in future prospective multicenter studies with respect to subtypes, treatment strategies, and individual courses of the disease. Additionally, there is still a requirement to define the exact methodology for measuring BWT, for example, on longitudinal or cross-sectional images (see Figure 1).
3.4. US Doppler Signals
Besides BWT, the very first approaches using ultrasound to diagnose and monitor inflammatory activity in IBD also assessed Doppler signals in the bowel wall. Limberg et al. used a qualitative, descriptive approach to grade scores from I to IV (Table 3) [53].
Table 3.
Ultrasound (doppler) scoring of inflammatory activity according to Limberg [53].
For example, such measurements of vessel density were able to reflect disease activity in patients with CD [54]. In 2004, Scholbach et al. reported flow velocities inside intestinal walls derived from recorded Doppler ultrasounds in 34 healthy children and 14 pediatric patients with CD [55]. In the small intestine, the flow velocity was 0.025 cm/s in healthy participants and elevated to 0.095 cm/s in those with CD, and in the large intestine, these values were 0.012 cm/s vs. 0.082 cm/s, without a strong correlation of clinical activity indices [55]. On a microscopic scale, preclinical studies have found that despite an increase in volumetric flow during inflammation, the actual velocity in the smallest intestinal capillaries decreased to create conditions suitable for leucocyte adhesion and transmigration [56]. With new technological developments, such as ultrasensitive Doppler, these criteria will also be adapted for children.
3.5. Mesenterial or “Creeping Fat”
A feature of CD is the extra-intestinal appearance and expansion of so called “creeping fat”, which may prevent (together with fibrosis) the systemic translocation of gut bacteria [57]. Interestingly, this “organ” is not a passive bystander in intestinal inflammation and might harbor two—harmful and beneficial—sites in this regard; while it might develop as a reaction to intestinal injury, leading to limited bacterial dissemination, it does not show a switch-off in CD [57,58,59]. It is now well understood that adipose tissue is associated with major alterations in the secretion of cytokines and adipokines, which mediate the immune-metabolic crosstalk of immune, lymphatic, neuroendocrine, and intestinal epithelial systems in IBD [60]. Calculating the slope of the Hounsfield unit (HU) curve of “creeping fat” on energy spectral computed tomography (CT) images, it could be shown that this correlated with endoscopic (SES-CD, r = 0.66, p < 0.01) and clinical disease activity (Harvey-Bradshaw index, r = 0.414, p < 0.01) [61]. A novel mesenteric creeping fat index (MCFI) has been shown to accurately characterize the extent of mesenteric fat wrapping in surgical specimens [62]. This might be particularly important in planning surgery for CD, because the inclusion of the mesentery in ileocolic resections may alter the course of CD [63,64], reducing the risk for recurrence requiring reoperation [65]. “Creeping fat” can be assessed in US and may also correlate with inflammatory activity [66]. So far, it has been used far less as a single characteristic for measuring clinical outcomes in IBD but more frequently in multiparametric intestinal US scoring systems. Furthermore, more specific studies in children and adolescents are missing.
3.6. Fibrostenosis and Intestinal Strictures
Fibrostenosis is the permanent and abnormal deposition of extracellular matrix (ECM, primarily collagens) to the intestinal wall, leading to a narrowed lumen with proximal dilation [67]. This process is still often regarded as irreversible following long-term inflammation in patients with less favorable responses to therapy [68]. The most important predilection site for such complications in patients with CD is the terminal ileum [69]. Although it appears to be more common in CD, similar complications can also occur in UC. It can already occur at the time of diagnosis, with rates of up to 21% in patients with CD and 1–11% in patients with UC [70]. However, an optimal anti-inflammatory regime including early anti-TNFα therapy did reduce the risk of penetrating but not fibrostenoic complications in children [71]. This, in turn, calls into question the effectiveness of current anti-inflammatory therapies in preventing such complications.
Various signaling pathways, growth factors, and cytokines, including IL-13, platelet-derived growth factor (PDGF), connective tissue growth factor, basic fibroblast growth factor, insulin-like growth factor, bone morphogenetic proteins (BMPs), and transforming growth factor-β (TGFβ), have been associated with its development [67,72]. According to Kugathasan et al., there might be an ECM gene signature that can predict the development of stricturing complications [71]. For this reason, it would be highly desirable to be able to reliably detect these processes at an early stage using non-invasive US, and also to identify patients at risk for unfavorable outcomes. More specifically, given the high frequency of intestinal strictures, the differentiation between fibrotic and inflammatory strictures might be crucial for clinical decision making [73].
A systematic review including 14 studies (511 adult subjects) found that US can currently not differentiate between fibrotic and inflammatory stenosis in CD patients [74]. Given the idea that these intestinal sections were subject to remodeling over a longer period of time, the main parameters used were B-mode US, strain elastography, shear wave elastography, and contrast-enhanced ultrasound (CEUS) [75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92]. These are primarily intended to demonstrate the altered intestinal wall structure or stratification with abnormal deposition of ECM, vascular changes, and an increase in stiffness. A first study with CEUS in pediatric IBD containing a small number of patients (n = 25) shows encouraging results [93], but these protocols are far from standardization or routine use. In the future, such techniques could become more sophisticated may be able to better capture changes in flow behavior in the tissues of smaller children [94,95,96] or even depict and quantify small microstructures [97].
3.7. US Scoring Systems
In addition to the aforementioned imaging features, ultrasonographic activity indices or scores would definitely be desirable and represent an unmet need. Concerning the latter, the field is moving forward as there have been a couple of promising approaches (Table 4).
Table 4.
Overview of pediatric sonographic US indices.
Civitelli et al. introduced a prospectively studied score for children with UC combining five US items [98]. These included bowel wall thickness (>3 mm), bowel wall stratification, vascularity, the presence of haustra coli, and enlarged mesenteric lymph nodes (51). Similarly, Wassenaer et al. investigated pediatric UC, reporting the so-called ulcerative colitis intestinal ultrasound (UC-IUS) index [99]. UC-IUS performed better than the Civitelli score with respect to the endoscopic subscore [102]. The pediatric CD intestinal US (PCD-US) index was developed to assess disease activity more specifically in CD [100]. The PCD-US index was evaluated in a prospective study, wherein the assessment was validated with the simple endoscopic score for CD (SES-CD) [103]. Kellar et al. developed their Simple Pediatric Activity Ultrasound Score (SPAUSS) for both IBD subtypes in a small retrospective study, dealing with four US parameters, including bowel wall thickness (BWT), mesenteric inflammatory fat, lymphadenopathy, and hyperemia [101]. Here, more emphasis was put on the presence or absence of mesenteric inflammatory fat to predict disease severity. A major limitation lies in the fact that SPAUSS has unfortunately not been validated against an endoscopic score.
Recently, a blinded, cross-sectional cohort study in young CD patients demonstrated the high sensitivity and specificity of IUS scores and BWT compared with the endoscopic SES-CD score [29]. Such scores or indices may correctly reflect endoscopic disease activity [104], but further external validation in prospective multicenter approaches is recommended to accelerate integration into clinical guidelines and clinical practice.
4. Novel US-Based Imaging Technologies: Optoacoustic Imaging (OAI)
While conventional US is based on the piezoelectric effect, discovered by the Curie brothers in 1880 [105], optoacoustic imaging is a further development of the photoacoustic effect, discovered by Alexander Graham Bell in the same year [106]. In contrast to US, OAI was applied in humans much later, with first descriptions in the early 1990s [107,108]. In OAI, light is used to induce the movement of molecules in deep tissue, and the scattered ultrasound waves are then detected [109,110]. By applying several wavelengths, specific optoacoustic spectra of different endogenous (oxygenated and deoxygenated hemoglobin, lipids, collagens, and melanin) and exogenous chromophores (dyes like indocyanine green) can be detected and quantified [111,112,113]. Hemoglobin is especially predestined for OAI, as it is one of the main absorbers in the used Near-infrared field of light and a surrogate OAI biomarker for various inflammatory [114] and cardiovascular diseases [115,116,117]. Furthermore, OAI allows scalability of the imaging device and resolution from cells and animal models to humans [110].
In murine models of colitis, disease severity can be measured by means of increased signal intensities for hemoglobin transabdominally in vivo [118,119], and by using transrectal guidance, changes in the intestinal wall thickness and vessel architecture can even be detected [120]. Furthermore, OAI technologies have the potential to identify intestinal inflammation and fibrosis to characterize intestinal strictures in mice [121,122]. The first pilot studies in adult patients with Crohn’s disease used a handheld OAI system to carry out so-called multispectral optoacoustic tomography (MSOT) to assess disease activity in comparison to clinical, laboratory, endoscopic, and conventional ultrasound [123,124]. The MSOT signal levels for hemoglobin correlated well with disease phenotype with minimal effort from the patient, and with high accuracy in the detection of remission and active disease [124]. In addition, studies on the precision of MSOT for imaging the human intestine showed resilient data [125], and the option of imaging luminal contrast agents throughout the intestinal tract opens the door to further translational applications and functional assessment of the gastrointestinal tract [126,127,128]. Such approaches might help to delineate complications likes fistulae, which are common manifestations in CD patients [129,130]. Early pilot studies in other pediatric conditions (neuromuscular disorders) were promising [131,132,133], and the first study in pediatric patients with UC and CD confirmed previous findings in adults [134] (Figure 2).
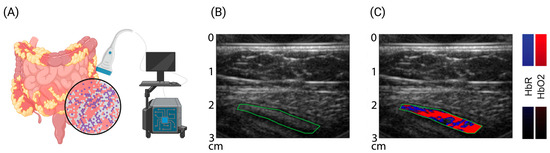
Figure 2.
Multispectral optoacoustic imaging—molecular sensitive ultrasound. (A) Cartoon of bedside multispectral optoacoustic tomography (MSOT) to assess molecular tissue composition. (B,C) Exemplary reflected-ultrasound computed tomography (RUCT) and MSOT images of a pediatric patient with ulcerative colitis. RUCT enables real-time guidance of the investigator. Spectral unmixing of MSOT data allows differentiation and quantification of oxygenated (red) and deoxygenated (blue) blood within the bowel wall (green, region of interest). Increased levels of hemoglobin correlate with disease activity and might serve as surrogate biomarkers. Created with https://www.biorender.com/ (accessed on 22 January 2024).
Currently, the multicenter approval study of MSOT in adult patients with Crohn’s disease is closed (https://euphoria2020.eu/, accessed on 22 January 2024), and further longitudinal studies in pediatric IBD are expected. For the manifestation of Crohn’s disease in the upper gastrointestinal tract, the integration of OAI in (capsule) endoscopic devices might allow the molecular assessment of the disease similarly to prior studies of the esophagus [135,136,137].
Therefore, OAI might aid in the bedside assessment of molecular disease activity and remission both in adult and pediatric IBD.
5. Conclusions
Intestinal US has undergone significant development in recent years. While technical progress and standardized examination methods have been introduced in the field of adult medicine in particular, some of these developments are still pending in pediatrics. The entire field still lacks prospective, multicenter studies that exploit the usability of IUS, particularly with regard to disease and therapy monitoring. However, from the perspective of a physician, the implementation of basic US categorization into the clinical routine follow-up procedure for IBD should rely on the quantitative assessment of the intestinal wall thickness. Hence, an intestinal wall that exceeds 2–3 mm in inflamed segments with increased blood flow should alert doctors to possible IBD lesions or a flare in already diagnosed patients.
This review is limited by its narrative character. Systematic reviews are necessary to determine standard examinations, cut-off values and scoring procedures. However, this review provides important information to perform pediatric IUS and integrate this into future clinical studies. Furthermore, emerging optoacoustic technologies are introduced to the readership to highlight new methods of non-invasive disease assessment in IBD. The molecular decryption and quantification of tissue composition, labeling of targeted therapies, and mapping of microvasculature will pave the way for the assessment and monitoring of individualized precision medicine.
The great advantages of IUS compared to other diagnostics in pediatric IBD are the non-invasiveness, the broad availability, the low infrastructure costs, and the easy-to-learn imaging modality with simple comprehensibility. For routine IUS diagnostics in clinical practice, at least the BWT and Limberg Score might be assessed. And, from our perspective, IUS should be implemented as a clinical endpoint in future clinical trials. However, more clinical studies [138] and robust scores with this methodology are needed to routinely implement IUS as a primary endpoint in clinical trials [139], like in the STARDUST study [140].
In the future, technological improvements and new technologies could provide a large number of other imaging biomarkers, making US-based imaging the first-line diagnostic method in pediatric IBD imaging.
Author Contributions
Conceptualization, A.H., J.J. and A.P.R.; Writing—Original Draft Preparation, A.H., J.J., G.S., F.K. and A.P.R.; Writing—Review and Editing, A.H., J.J., G.S., F.K. and A.P.R.; Visualization and Funding Acquisition, A.P.R. Literature search was performed via pubmed. All authors have read and agreed to the published version of the manuscript.
Funding
Funding was provided by Else Kröner-Fresenius Stiftung to A.P.R.
Data Availability Statement
Not applicable.
Conflicts of Interest
A.P.R. and F.K. are shared patent holders, together with iThera Medical GmbH (Munich, Germany), for the optoacoustic imaging system/software described in this study. F.K. is a member of the clinical advisory board of iThera Medical GmbH (Munich, Germany).
References
- Graham, D.B.; Xavier, R.J. Pathway paradigms revealed from the genetics of inflammatory bowel disease. Nature 2020, 578, 527–539. [Google Scholar] [CrossRef]
- Chang, J.T. Pathophysiology of Inflammatory Bowel Diseases. N. Engl. J. Med. 2020, 383, 2652–2664. [Google Scholar] [CrossRef]
- Khor, B.; Gardet, A.; Xavier, R.J. Genetics and pathogenesis of inflammatory bowel disease. Nature 2011, 474, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Schaffler, H.; Kaschitzki, A.; Alberts, C.; Bodammer, P.; Bannert, K.; Koller, T.; Warnke, P.; Kreikemeyer, B.; Lamprecht, G. Alterations in the mucosa-associated bacterial composition in Crohn’s disease: A pilot study. Int. J. Color. Dis. 2016, 31, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Neurath, M.F. Host-microbiota interactions in inflammatory bowel disease. Nat. Reviews. Gastroenterol. Hepatol. 2020, 17, 76–77. [Google Scholar] [CrossRef]
- Ruel, J.; Ruane, D.; Mehandru, S.; Gower-Rousseau, C.; Colombel, J.F. IBD across the age spectrum: Is it the same disease? Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Podolsky, D.K. Inflammatory bowel disease. N. Engl. J. Med. 2002, 347, 417–429. [Google Scholar] [CrossRef]
- Van Limbergen, J.; Russell, R.K.; Drummond, H.E.; Aldhous, M.C.; Round, N.K.; Nimmo, E.R.; Smith, L.; Gillett, P.M.; McGrogan, P.; Weaver, L.T.; et al. Definition of phenotypic characteristics of childhood-onset inflammatory bowel disease. Gastroenterology 2008, 135, 1114–1122. [Google Scholar] [CrossRef]
- Le Berre, C.; Honap, S.; Peyrin-Biroulet, L. Ulcerative colitis. Lancet 2023, 402, 571–584. [Google Scholar] [CrossRef]
- Ko, C.W.; Singh, S.; Feuerstein, J.D.; Falck-Ytter, C.; Falck-Ytter, Y.; Cross, R.K.; American Gastroenterological Association Institute Clinical Guidelines Committee. AGA Clinical Practice Guidelines on the Management of Mild-to-Moderate Ulcerative Colitis. Gastroenterology 2019, 156, 748–764. [Google Scholar] [CrossRef]
- Buderus, S.; Scholz, D.; Behrens, R.; Classen, M.; De Laffolie, J.; Keller, K.M.; Zimmer, K.P.; Koletzko, S.; Group, C.-G.S. Inflammatory bowel disease in pediatric patients: Characteristics of newly diagnosed patients from the CEDATA-GPGE Registry. Dtsch. Arztebl. Int. 2015, 112, 121–127. [Google Scholar] [CrossRef][Green Version]
- Rogler, G.; Singh, A.; Kavanaugh, A.; Rubin, D.T. Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management. Gastroenterology 2021, 161, 1118–1132. [Google Scholar] [CrossRef]
- Neurath, M.F. Targeting cytokines in inflammatory bowel disease. Sci. Transl. Med. 2022, 14, eabq4473. [Google Scholar] [CrossRef] [PubMed]
- Rogler, G. Resolution of inflammation in inflammatory bowel disease. Lancet Gastroenterol. Hepatol. 2017, 2, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Present, D.H.; Rutgeerts, P.; Targan, S.; Hanauer, S.B.; Mayer, L.; van Hogezand, R.A.; Podolsky, D.K.; Sands, B.E.; Braakman, T.; DeWoody, K.L.; et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N. Engl. J. Med. 1999, 340, 1398–1405. [Google Scholar] [CrossRef]
- Feagan, B.G.; Greenberg, G.R.; Wild, G.; Fedorak, R.N.; Pare, P.; McDonald, J.W.; Dube, R.; Cohen, A.; Steinhart, A.H.; Landau, S.; et al. Treatment of ulcerative colitis with a humanized antibody to the alpha4beta7 integrin. N. Engl. J. Med. 2005, 352, 2499–2507. [Google Scholar] [CrossRef] [PubMed]
- Loftus, E.V., Jr.; Panes, J.; Lacerda, A.P.; Peyrin-Biroulet, L.; D’Haens, G.; Panaccione, R.; Reinisch, W.; Louis, E.; Chen, M.; Nakase, H.; et al. Upadacitinib Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2023, 388, 1966–1980. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, E.I.; Fortinsky, K.J.; Gozdyra, P.; Van den Heuvel, M.; Van Limbergen, J.; Griffiths, A.M. Epidemiology of pediatric inflammatory bowel disease: A systematic review of international trends. Inflamm. Bowel Dis. 2011, 17, 423–439. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Bernstein, C.N.; Bitton, A.; Carroll, M.W.; Singh, H.; Otley, A.R.; Vutcovici, M.; El-Matary, W.; Nguyen, G.C.; Griffiths, A.M.; et al. Trends in Epidemiology of Pediatric Inflammatory Bowel Disease in Canada: Distributed Network Analysis of Multiple Population-Based Provincial Health Administrative Databases. Am. J. Gastroenterol. 2017, 112, 1120–1134. [Google Scholar] [CrossRef]
- Kaplan, G.G.; Ng, S.C. Understanding and Preventing the Global Increase of Inflammatory Bowel Disease. Gastroenterology 2017, 152, 313–321.e312. [Google Scholar] [CrossRef]
- Ruemmele, F.M. Pediatric inflammatory bowel diseases: Coming of age. Curr. Opin. Gastroenterol. 2010, 26, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Dabritz, J.; Gerner, P.; Enninger, A.; Classen, M.; Radke, M. Inflammatory Bowel Disease in Childhood and Adolescence. Dtsch. Arztebl. Int. 2017, 114, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohns Colitis 2020, 15, 171–194. [Google Scholar] [CrossRef]
- Turner, D.; Ruemmele, F.M.; Orlanski-Meyer, E.; Griffiths, A.M.; de Carpi, J.M.; Bronsky, J.; Veres, G.; Aloi, M.; Strisciuglio, C.; Braegger, C.P.; et al. Management of Paediatric Ulcerative Colitis, Part 1: Ambulatory Care-An Evidence-based Guideline From European Crohn’s and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 257–291. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ruemmele, F.M.; Orlanski-Meyer, E.; Griffiths, A.M.; de Carpi, J.M.; Bronsky, J.; Veres, G.; Aloi, M.; Strisciuglio, C.; Braegger, C.P.; et al. Management of Paediatric Ulcerative Colitis, Part 2: Acute Severe Colitis-An Evidence-based Consensus Guideline From the European Crohn’s and Colitis Organization and the European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 292–310. [Google Scholar] [CrossRef] [PubMed]
- De Bie, C.I.; Buderus, S.; Sandhu, B.K.; de Ridder, L.; Paerregaard, A.; Veres, G.; Dias, J.A.; Escher, J.C.; ESPGHAN, E.P.I.W.G.o. Diagnostic workup of paediatric patients with inflammatory bowel disease in Europe: Results of a 5-year audit of the EUROKIDS registry. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Dolinger, M.T.; Kayal, M. Intestinal ultrasound as a non-invasive tool to monitor inflammatory bowel disease activity and guide clinical decision making. World J. Gastroenterol. WJG 2023, 29, 2272–2282. [Google Scholar] [CrossRef] [PubMed]
- Dolinger, M.T.; Aronskyy, I.; Kellar, A.; Spencer, E.; Pittman, N.; Dubinsky, M.C. Early Intestinal Ultrasound Response to Biologic Therapy Predicts Endoscopic Remission in Children with Ileal Crohn’s Disease: Results from the Prospective Super Sonic Study. J. Crohns Colitis 2023, 2023, jjad216. [Google Scholar] [CrossRef]
- Dolinger, M.T.; Aronskyy, I.; Kellar, A.; Gao, M.; Spencer, E.A.; Pittman, N.; Dubinsky, M.C. Determining the accuracy of intestinal ultrasound scores as a pre-screening tool in Crohn’s disease clinical trials. Am. J. Gastroenterol. 2023, 2023, 2632. [Google Scholar] [CrossRef]
- Van Wassenaer, E.A.; Benninga, M.A.; van Limbergen, J.L.; D’Haens, G.R.; Griffiths, A.M.; Koot, B.G.P. Intestinal Ultrasound in Pediatric Inflammatory Bowel Disease: Promising, but Work in Progress. Inflamm. Bowel Dis. 2022, 28, 783–787. [Google Scholar] [CrossRef]
- Ilvemark, J.; Hansen, T.; Goodsall, T.M.; Seidelin, J.B.; Al-Farhan, H.; Allocca, M.; Begun, J.; Bryant, R.V.; Carter, D.; Christensen, B.; et al. Defining Transabdominal Intestinal Ultrasound Treatment Response and Remission in Inflammatory Bowel Disease: Systematic Review and Expert Consensus Statement. J. Crohns Colitis 2022, 16, 554–580. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.H.; Yoon, H.M.; Jung, A.Y.; Lee, J.S.; Cho, Y.A. Diagnostic Performance of Diffusion-weighted Imaging for Evaluation of Bowel Inflammation in Paediatric Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. J. Crohns Colitis 2022, 16, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.M.; Suh, C.H.; Kim, J.R.; Lee, J.S.; Jung, A.Y.; Kim, K.M.; Cho, Y.A. Diagnostic Performance of Magnetic Resonance Enterography for Detection of Active Inflammation in Children and Adolescents With Inflammatory Bowel Disease: A Systematic Review and Diagnostic Meta-analysis. JAMA Pediatr. 2017, 171, 1208–1216. [Google Scholar] [CrossRef]
- Schreiber-Dietrich, D.; Chiorean, L.; Cui, X.W.; Braden, B.; Kucharzik, T.; Jungert, J.; Kosiak, W.; Stenzel, M.; Dietrich, C.F. Particularities of Crohn’s disease in pediatric patients: Current status and perspectives regarding imaging modalities. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 1313–1325. [Google Scholar] [CrossRef] [PubMed]
- Watson, T.A.; Petit, P.; Augdal, T.A.; Avni, E.F.; Bruno, C.; Damasio, M.B.; Darge, K.; Kjucevsek, D.; Franchi-Abella, S.; Ibe, D.; et al. European Society of Paediatric Radiology abdominal imaging task force: Statement on imaging in very early onset inflammatory bowel disease. Pediatr. Radiol. 2019, 49, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Panes, J.; Bouhnik, Y.; Reinisch, W.; Stoker, J.; Taylor, S.A.; Baumgart, D.C.; Danese, S.; Halligan, S.; Marincek, B.; Matos, C.; et al. Imaging techniques for assessment of inflammatory bowel disease: Joint ECCO and ESGAR evidence-based consensus guidelines. J. Crohns Colitis 2013, 7, 556–585. [Google Scholar] [CrossRef]
- Van Wassenaer, E.A.; van Rijn, R.R.; de Voogd, F.A.E.; Noels, F.L.; Deurloo, E.E.; van Schuppen, J.; Verbeke, J.; Gecse, K.B.; D’Haens, G.R.; Benninga, M.A.; et al. A Healthcare Physician Can Be Trained to Perform Intestinal Ultrasound in Children With Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2022, 74, e143–e147. [Google Scholar] [CrossRef]
- Hudson, A.S.; Huynh, H.Q.; Novak, K.L.; Ma, H.; Kuc, A.; Kim, J.; Almeida, P.; Carroll, M.W.; Wine, E.; Isaac, D.M. Pediatric Patient and Caregiver Satisfaction With the Use of Transabdominal Bowel Ultrasound in the Assessment of Inflammatory Bowel Diseases. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 33–37. [Google Scholar] [CrossRef]
- Van Wassenaer, E.A.; van der Klift, R.R.; Staphorst, M.S.; van der Lee, J.H.; Benninga, M.A.; Koot, B.G.P. The child’s perception on monitoring inflammatory bowel disease activity. Eur. J. Pediatr. 2022, 181, 1143–1149. [Google Scholar] [CrossRef]
- Elliott, C.L.; Maclachlan, J.; Beal, I. Paediatric bowel ultrasound in inflammatory bowel disease. Eur. J. Radiol. 2018, 108, 21–27. [Google Scholar] [CrossRef]
- Strobel, D.; Goertz, R.S.; Bernatik, T. Diagnostics in inflammatory bowel disease: Ultrasound. World J. Gastroenterol. WJG 2011, 17, 3192–3197. [Google Scholar]
- Hirche, T.O.; Russler, J.; Schroder, O.; Schuessler, G.; Kappeser, P.; Caspary, W.F.; Dietrich, C.F. The value of routinely performed ultrasonography in patients with Crohn disease. Scand. J. Gastroenterol. 2002, 37, 1178–1183. [Google Scholar] [CrossRef]
- Bremner, A.R.; Griffiths, M.; Argent, J.D.; Fairhurst, J.J.; Beattie, R.M. Sonographic evaluation of inflammatory bowel disease: A prospective, blinded, comparative study. Pediatr. Radiol. 2006, 36, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Canani, R.B.; de Horatio, L.T.; Terrin, G.; Romano, M.T.; Miele, E.; Staiano, A.; Rapacciuolo, L.; Polito, G.; Bisesti, V.; Manguso, F.; et al. Combined use of noninvasive tests is useful in the initial diagnostic approach to a child with suspected inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Van Wassenaer, E.A.; de Voogd, F.A.E.; van Rijn, R.R.; van Der Lee, J.H.; Tabbers, M.M.; van Etten-Jamaludin, F.S.; Gecse, K.B.; Kindermann, A.; De Meij, T.G.J.; D’Haens, G.R.; et al. Diagnostic Accuracy of Transabdominal Ultrasound in Detecting Intestinal Inflammation in Paediatric IBD Patients-a Systematic Review. J. Crohns Colitis 2019, 13, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Novak, K.L.; Nylund, K.; Maaser, C.; Petersen, F.; Kucharzik, T.; Lu, C.; Allocca, M.; Maconi, G.; de Voogd, F.; Christensen, B.; et al. Expert Consensus on Optimal Acquisition and Development of the International Bowel Ultrasound Segmental Activity Score [IBUS-SAS]: A Reliability and Inter-rater Variability Study on Intestinal Ultrasonography in Crohn’s Disease. J. Crohns Colitis 2021, 15, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Van Wassenaer, E.A.; de Voogd, F.A.E.; van Rijn, R.R.; van der Lee, J.H.; Tabbers, M.M.; van Etten-Jamaludin, F.S.; Kindermann, A.; de Meij, T.G.J.; Gecse, K.B.; D’Haens, G.R.; et al. Bowel ultrasound measurements in healthy children—Systematic review and meta-analysis. Pediatr. Radiol. 2020, 50, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Haber, H.P.; Stern, M. Intestinal ultrasonography in children and young adults: Bowel wall thickness is age dependent. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2000, 19, 315–321. [Google Scholar] [CrossRef]
- Ramsden, W.H.; Moya, E.F.; Littlewood, J.M. Colonic wall thickness, pancreatic enzyme dose and type of preparation in cystic fibrosis. Arch. Dis. Child. 1998, 79, 339–343. [Google Scholar] [CrossRef]
- Pohl, M.; Krackhardt, B.; Posselt, H.G.; Lembcke, B. Ultrasound studies of the intestinal wall in patients with cystic fibrosis. J. Pediatr. Gastroenterol. Nutr. 1997, 25, 317–320. [Google Scholar] [CrossRef]
- Chiorean, L.; Schreiber-Dietrich, D.; Braden, B.; Cui, X.; Dietrich, C.F. Transabdominal ultrasound for standardized measurement of bowel wall thickness in normal children and those with Crohn’s disease. Med. Ultrason. 2014, 16, 319–324. [Google Scholar] [CrossRef][Green Version]
- De Voogd, F.; van Wassenaer, E.A.; Mookhoek, A.; Bots, S.; van Gennep, S.; Lowenberg, M.; D’Haens, G.R.; Gecse, K.B. Intestinal Ultrasound Is Accurate to Determine Endoscopic Response and Remission in Patients With Moderate to Severe Ulcerative Colitis: A Longitudinal Prospective Cohort Study. Gastroenterology 2022, 163, 1569–1581. [Google Scholar] [CrossRef] [PubMed]
- Limberg, B. Diagnosis of chronic inflammatory bowel disease by ultrasonography. Z. Fur Gastroenterol. 1999, 37, 495–508. [Google Scholar]
- Spalinger, J.; Patriquin, H.; Miron, M.C.; Marx, G.; Herzog, D.; Dubois, J.; Dubinsky, M.; Seidman, E.G. Doppler US in patients with crohn disease: Vessel density in the diseased bowel reflects disease activity. Radiology 2000, 217, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Scholbach, T.; Herrero, I.; Scholbach, J. Dynamic color Doppler sonography of intestinal wall in patients with Crohn disease compared with healthy subjects. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 524–528. [Google Scholar] [CrossRef]
- Ravnic, D.J.; Konerding, M.A.; Tsuda, A.; Huss, H.T.; Wolloscheck, T.; Pratt, J.P.; Mentzer, S.J. Structural adaptations in the murine colon microcirculation associated with hapten-induced inflammation. Gut 2007, 56, 518–523. [Google Scholar] [CrossRef]
- Ha, C.W.Y.; Martin, A.; Sepich-Poore, G.D.; Shi, B.; Wang, Y.; Gouin, K.; Humphrey, G.; Sanders, K.; Ratnayake, Y.; Chan, K.S.L.; et al. Translocation of Viable Gut Microbiota to Mesenteric Adipose Drives Formation of Creeping Fat in Humans. Cell 2020, 183, 666–683.e617. [Google Scholar] [CrossRef] [PubMed]
- Eder, P.; Adler, M.; Dobrowolska, A.; Kamhieh-Milz, J.; Witowski, J. The Role of Adipose Tissue in the Pathogenesis and Therapeutic Outcomes of Inflammatory Bowel Disease. Cells 2019, 8, 628. [Google Scholar] [CrossRef]
- Rivera, E.D.; Coffey, J.C.; Walsh, D.; Ehrenpreis, E.D. The Mesentery, Systemic Inflammation, and Crohn’s Disease. Inflamm. Bowel Dis. 2019, 25, 226–234. [Google Scholar] [CrossRef]
- Goncalves, P.; Magro, F.; Martel, F. Metabolic inflammation in inflammatory bowel disease: Crosstalk between adipose tissue and bowel. Inflamm. Bowel Dis. 2015, 21, 453–467. [Google Scholar] [CrossRef]
- Feng, Q.; Xu, X.T.; Zhou, Y.; Yan, Y.Q.; Ran, Z.H.; Zhu, J. Creeping fat in patients with ileo-colonic Crohn’s disease correlates with disease activity and severity of inflammation: A preliminary study using energy spectral computed tomography. J. Dig. Dis. 2018, 19, 475–484. [Google Scholar] [CrossRef]
- Li, X.H.; Feng, S.T.; Cao, Q.H.; Coffey, J.C.; Baker, M.E.; Huang, L.; Fang, Z.N.; Qiu, Y.; Lu, B.L.; Chen, Z.H.; et al. Degree of Creeping Fat Assessed by Computed Tomography Enterography is Associated with Intestinal Fibrotic Stricture in Patients with Crohn’s Disease: A Potentially Novel Mesenteric Creeping Fat Index. J. Crohns Colitis 2021, 15, 1161–1173. [Google Scholar] [CrossRef] [PubMed]
- Coffey, J.C.; O’Leary, D.P. The mesentery: Structure, function, and role in disease. Lancet Gastroenterol. Hepatol. 2016, 1, 238–247. [Google Scholar] [CrossRef]
- Coffey, J.C.; Byrnes, K.G.; Walsh, D.J.; Cunningham, R.M. Update on the mesentery: Structure, function, and role in disease. Lancet Gastroenterol. Hepatol. 2022, 7, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Coffey, C.J.; Kiernan, M.G.; Sahebally, S.M.; Jarrar, A.; Burke, J.P.; Kiely, P.A.; Shen, B.; Waldron, D.; Peirce, C.; Moloney, M.; et al. Inclusion of the Mesentery in Ileocolic Resection for Crohn’s Disease is Associated With Reduced Surgical Recurrence. J. Crohns Colitis 2018, 12, 1139–1150. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, G.; Rodriguez-Justo, M.; Higginson, A.; Bassett, P.; Windsor, A.; Cohen, R.; Halligan, S.; Taylor, S.A. Inflammation and fibrosis in Crohn’s disease: Location-matched histological correlation of small bowel ultrasound features. Abdom. Radiol. 2021, 46, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Stenke, E.; Bourke, B.; Knaus, U. Crohn’s Strictures—Moving Away from the Knife. Front. Pediatr. 2017, 5, 141. [Google Scholar] [CrossRef] [PubMed]
- Rieder, F.; Fiocchi, C.; Rogler, G. Mechanisms, Management, and Treatment of Fibrosis in Patients With Inflammatory Bowel Diseases. Gastroenterology 2017, 152, 340–350.e346. [Google Scholar] [CrossRef]
- Freeman, H.J. Natural history and long-term clinical course of Crohn’s disease. World J. Gastroenterol. 2014, 20, 31–36. [Google Scholar] [CrossRef]
- Mak, J.W.Y.; Ng, S.C. Epidemiology of fibrostenosing inflammatory bowel disease. J. Dig. Dis. 2020, 21, 332–335. [Google Scholar] [CrossRef]
- Kugathasan, S.; Denson, L.A.; Walters, T.D.; Kim, M.O.; Marigorta, U.M.; Schirmer, M.; Mondal, K.; Liu, C.; Griffiths, A.; Noe, J.D.; et al. Prediction of complicated disease course for children newly diagnosed with Crohn’s disease: A multicentre inception cohort study. Lancet 2017, 389, 1710–1718. [Google Scholar] [CrossRef] [PubMed]
- Bettenworth, D.; Rieder, F. Medical therapy of stricturing Crohn’s disease: What the gut can learn from other organs—A systematic review. Fibrogenesis Tissue Repair 2014, 7, 5. [Google Scholar] [CrossRef] [PubMed]
- Coelho, R.; Ribeiro, H.; Maconi, G. Bowel Thickening in Crohn’s Disease: Fibrosis or Inflammation? Diagnostic Ultrasound Imaging Tools. Inflamm. Bowel Dis. 2017, 23, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Jiang, W.; Wang, L.; Mao, X.; Ye, Z.; Zhang, H. Intestinal Ultrasound for Differentiating Fibrotic or Inflammatory Stenosis in Crohn’s Disease: A Systematic Review and Meta-analysis. J. Crohns Colitis 2022, 16, 1493–1504. [Google Scholar] [CrossRef] [PubMed]
- Dillman, J.R.; Stidham, R.W.; Higgins, P.D.; Moons, D.S.; Johnson, L.A.; Keshavarzi, N.R.; Rubin, J.M. Ultrasound shear wave elastography helps discriminate low-grade from high-grade bowel wall fibrosis in ex vivo human intestinal specimens. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2014, 33, 2115–2123. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Muller, H.P.; Grittner, U.; Metzke, D.; Fischer, A.; Guckelberger, O.; Pascher, A.; Sack, I.; Vieth, M.; Rudolph, B. US-based Real-time Elastography for the Detection of Fibrotic Gut Tissue in Patients with Stricturing Crohn Disease. Radiology 2015, 275, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.S.; Fang, Y.; Wan, J.; Zhao, C.K.; Xiang, L.H.; Liu, H.; Pu, H.; Xu, G.; Zhang, K.; Xu, X.R.; et al. Usefulness of Strain Elastography, ARFI Imaging, and Point Shear Wave Elastography for the Assessment of Crohn Disease Strictures. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2019, 38, 2861–2870. [Google Scholar] [CrossRef]
- Kratzer, W.; von Tirpitz, C.; Mason, R.; Reinshagen, M.; Adler, G.; Moller, P.; Rieber, A.; Kachele, V. Contrast-enhanced power Doppler sonography of the intestinal wall in the differentiation of hypervascularized and hypovascularized intestinal obstructions in patients with Crohn’s disease. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2002, 21, 149–157, quiz 158–149. [Google Scholar] [CrossRef]
- Lenze, F.; Wessling, J.; Bremer, J.; Ullerich, H.; Spieker, T.; Weckesser, M.; Gonschorrek, S.; Kannengiesser, K.; Rijcken, E.; Heidemann, J.; et al. Detection and differentiation of inflammatory versus fibromatous Crohn’s disease strictures: Prospective comparison of 18F-FDG-PET/CT, MR-enteroclysis, and transabdominal ultrasound versus endoscopic/histologic evaluation. Inflamm. Bowel Dis. 2012, 18, 2252–2260. [Google Scholar] [CrossRef]
- Lu, C.; Gui, X.; Chen, W.; Fung, T.; Novak, K.; Wilson, S.R. Ultrasound Shear Wave Elastography and Contrast Enhancement: Effective Biomarkers in Crohn’s Disease Strictures. Inflamm. Bowel Dis. 2017, 23, 421–430. [Google Scholar] [CrossRef]
- Maconi, G.; Carsana, L.; Fociani, P.; Sampietro, G.M.; Ardizzone, S.; Cristaldi, M.; Parente, F.; Vago, G.L.; Taschieri, A.M.; Bianchi Porro, G. Small bowel stenosis in Crohn’s disease: Clinical, biochemical and ultrasonographic evaluation of histological features. Aliment. Pharmacol. Ther. 2003, 18, 749–756. [Google Scholar] [CrossRef]
- Nylund, K.; Jirik, R.; Mezl, M.; Leh, S.; Hausken, T.; Pfeffer, F.; Odegaard, S.; Taxt, T.; Gilja, O.H. Quantitative contrast-enhanced ultrasound comparison between inflammatory and fibrotic lesions in patients with Crohn’s disease. Ultrasound Med. Biol. 2013, 39, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Orlando, S.; Fraquelli, M.; Coletta, M.; Branchi, F.; Magarotto, A.; Conti, C.B.; Mazza, S.; Conte, D.; Basilisco, G.; Caprioli, F. Ultrasound Elasticity Imaging Predicts Therapeutic Outcomes of Patients With Crohn’s Disease Treated With Anti-Tumour Necrosis Factor Antibodies. J. Crohns Colitis 2018, 12, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Quaia, E.; Gennari, A.G.; Cova, M.A.; van Beek, E.J.R. Differentiation of Inflammatory From Fibrotic Ileal Strictures among Patients with Crohn’s Disease Based on Visual Analysis: Feasibility Study Combining Conventional B-Mode Ultrasound, Contrast-Enhanced Ultrasound and Strain Elastography. Ultrasound Med. Biol. 2018, 44, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Quaia, E.; De Paoli, L.; Stocca, T.; Cabibbo, B.; Casagrande, F.; Cova, M.A. The value of small bowel wall contrast enhancement after sulfur hexafluoride-filled microbubble injection to differentiate inflammatory from fibrotic strictures in patients with Crohn’s disease. Ultrasound Med. Biol. 2012, 38, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Orlova, L.; Samsonova, T.; Khalif, I. P1018 Strain elastography and differential diagnosis of inflammatory and fibrotic strictures in Crohn’s disease. United Eur. Gastroenterol. J. 2017, 5, A518. [Google Scholar]
- Schirin-Sokhan, R.; Winograd, R.; Tischendorf, S.; Wasmuth, H.E.; Streetz, K.; Tacke, F.; Trautwein, C.; Tischendorf, J.J. Assessment of inflammatory and fibrotic stenoses in patients with Crohn’s disease using contrast-enhanced ultrasound and computerized algorithm: A pilot study. Digestion 2011, 83, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Serra, C.; Rizzello, F.; Pratico, C.; Felicani, C.; Fiorini, E.; Brugnera, R.; Mazzotta, E.; Giunchi, F.; Fiorentino, M.; D’Errico, A.; et al. Real-time elastography for the detection of fibrotic and inflammatory tissue in patients with stricturing Crohn’s disease. J. Ultrasound 2017, 20, 273–284. [Google Scholar] [CrossRef]
- Stidham, R.; Dillman, J.; Rubin, J.; Higgins, P. P-111 Using Stiffness Imaging of the Intestine to Predict Response to Medical Therapy in Obstructive Crohn’s Disease. Inflamm. Bowel Dis. 2016, 22, S44–S45. [Google Scholar] [CrossRef]
- Wilkens, R.; Hagemann-Madsen, R.H.; Peters, D.A.; Nielsen, A.H.; Norager, C.B.; Glerup, H.; Krogh, K. Validity of Contrast-enhanced Ultrasonography and Dynamic Contrast-enhanced MR Enterography in the Assessment of Transmural Activity and Fibrosis in Crohn’s Disease. J. Crohns Colitis 2018, 12, 48–56. [Google Scholar] [CrossRef]
- Zhao, J.; Liao, D.; Wilkens, R.; Krogh, K.; Glerup, H.; Gregersen, H. Bowel stiffness associated with histopathologic scoring of stenosis in patients with Crohn’s disease. Acta Biomater. 2021, 130, 332–342. [Google Scholar] [CrossRef]
- Nylund, K.; Leh, S.; Immervoll, H.; Matre, K.; Skarstein, A.; Hausken, T.; Gilja, O.H.; Birger Nesje, L.; Odegaard, S. Crohn’s disease: Comparison of in vitro ultrasonographic images and histology. Scand. J. Gastroenterol. 2008, 43, 719–726. [Google Scholar] [CrossRef]
- Sidhu, S.D.; Joseph, S.; Dunn, E.; Cuffari, C. The Utility of Contrast Enhanced Ultrasound and Elastography in the Early Detection of Fibro-Stenotic Ileal Strictures in Children with Crohn’s Disease. Pediatr. Gastroenterol. Hepatol. Nutr. 2023, 26, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Knieling, F.; Cesnjevar, R.; Regensburger, A.P.; Wagner, A.L.; Purbojo, A.; Dittrich, S.; Münch, F.; Neubert, A.; Woelfle, J.; Jüngert, J.; et al. Transfontanellar Contrast-enhanced US for Intraoperative Imaging of Cerebral Perfusion during Neonatal Arterial Switch Operation. Radiology 2022, 304, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Rüffer, A.; Knieling, F.; Cesnjevar, R.; Regensburger, A.; Purbojo, A.; Dittrich, S.; Münch, F.; Wölfle, J.; Jüngert, J. Equal cerebral perfusion during extended aortic coarctation repair. Eur. J. Cardiothorac. Surg. 2022, 61, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Knieling, F.; Rüffer, A.; Cesnjevar, R.; Regensburger, A.P.; Purbojo, A.; Dittrich, S.; Münch, F.; Neubert, A.; Meyer, S.; Strobel, D.; et al. Transfontanellar Contrast-Enhanced Ultrasound for Monitoring Brain Perfusion During Neonatal Heart Surgery. Circ. Cardiovasc. Imaging 2020, 13, e010073. [Google Scholar] [CrossRef] [PubMed]
- Knieling, F.; Schmarz, S.; Denis, L.; Nedoschill, E.; Buehler, A.; Danko, V.; Mandelbaum, H.; Nuñez, F.B.; Dürr, N.; Schlunz-Hendann, M. Ultrasound super-resolution imaging of neonatal cerebral vascular reorganization during neurovascular interventions. Tech. Rep. 2023. preprint. [Google Scholar]
- Civitelli, F.; Di Nardo, G.; Oliva, S.; Nuti, F.; Ferrari, F.; Dilillo, A.; Viola, F.; Pallotta, N.; Cucchiara, S.; Aloi, M. Ultrasonography of the colon in pediatric ulcerative colitis: A prospective, blind, comparative study with colonoscopy. J. Pediatr. 2014, 165, 78–84.e72. [Google Scholar] [CrossRef] [PubMed]
- Van Wassenaer, E.A.; van Rijn, R.R.; Zwetsloot, S.L.M.; de Voogd, F.A.E.; van Schuppen, J.; Kindermann, A.; de Meij, T.G.J.; van Limbergen, J.E.; Gecse, K.B.; D’Haens, G.R.; et al. Intestinal Ultrasound to Assess Ulcerative Colitis Disease Activity in Children: External Validation and Comparison of 2 Intestinal Ultrasound Activity Indices. Inflamm. Bowel Dis. 2023, 29, 1217–1222. [Google Scholar] [CrossRef]
- Van Wassenaer, E.A.; van Rijn, R.R.; de Voogd, F.A.E.; van Schuppen, J.; Kindermann, A.; de Meij, T.G.J.; van Limbergen, J.E.; Gecse, K.B.; D’Haens, G.R.; Benninga, M.A.; et al. Assessing Disease Activity in Pediatric Crohn’s Disease Using Ultrasound: The Pediatric Crohn Disease Intestinal Ultrasound Score. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 582–589. [Google Scholar] [CrossRef]
- Kellar, A.; Wilson, S.; Kaplan, G.; DeBruyn, J.; Tanyingoh, D.; Novak, K.L. The Simple Pediatric Activity Ultrasound Score (SPAUSS) for the Accurate Detection of Pediatric Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 69, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N. Engl. J. Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef]
- Daperno, M.; D’Haens, G.; Van Assche, G.; Baert, F.; Bulois, P.; Maunoury, V.; Sostegni, R.; Rocca, R.; Pera, A.; Gevers, A.; et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: The SES-CD. Gastrointest. Endosc. 2004, 60, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Fodor, I.; Serban, O.; Serban, D.E.; Farcau, D.; Fufezan, O.; Asavoaie, C.; Man, S.C.; Dumitrascu, D.L. The value of abdominal ultrasonography compared to colonoscopy and faecal calprotectin in following up paediatric patients with ulcerative colitis. Med. Ultrason. 2021, 23, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Curie, P.; Curie, J. Développement par compression de l’électricité polaire dans les cristaux hémièdres à faces inclinées. Bull. Minéralogie 1880, 3, 90–93. [Google Scholar] [CrossRef]
- Bell, A.G. On the production and reproduction of sound by light. Am. J. Sci. 1880, s3–s20, 305–324. [Google Scholar] [CrossRef]
- Chen, Q.X.; Dewhurst, R.J.; Payne, P.A.; Davies, A. Photo-acoustic probe for intra-arterial imaging and therapy. Electron. Lett. 1993, 29, 1632–1633. [Google Scholar] [CrossRef]
- Oraevsky, A.J.; Jacques, A.J.; Esenaliev, R.; Tittel, F. Laser-based optoacoustic imaging in biological tissues. In Proceedings of the SPIE, OE/LASE ‘94, 1994, Los Angeles, CA, USA, 23 January 1994. [Google Scholar]
- Razansky, D.; Distel, M.; Vinegoni, C.; Ma, R.; Perrimon, N.; Köster, R.W.; Ntziachristos, V. Multispectral opto-acoustic tomography of deep-seated fluorescent proteins in vivo. Nat. Photon. 2009, 3, 412–417. [Google Scholar] [CrossRef]
- Wang, L.V.; Hu, S. Photoacoustic tomography: In vivo imaging from organelles to organs. Science 2012, 335, 1458–1462. [Google Scholar] [CrossRef]
- Tzoumas, S.; Deliolanis, N.; Morscher, S.; Ntziachristos, V. Unmixing Molecular Agents From Absorbing Tissue in Multispectral Optoacoustic Tomography. IEEE Trans. Med. Imaging 2014, 33, 48–60. [Google Scholar] [CrossRef]
- Cao, Q.; Zhegalova, N.G.; Wang, S.T.; Akers, W.J.; Berezin, M.Y. Multispectral imaging in the extended near-infrared window based on endogenous chromophores. J. Biomed. Opt. 2013, 18, 101318. [Google Scholar] [CrossRef]
- Wang, L.V.; Yao, J. A practical guide to photoacoustic tomography in the life sciences. Nat. Methods 2016, 13, 627–638. [Google Scholar] [CrossRef]
- Regensburger, A.P.; Brown, E.; Kronke, G.; Waldner, M.J.; Knieling, F. Optoacoustic Imaging in Inflammation. Biomedicines 2021, 9, 483. [Google Scholar] [CrossRef]
- Karlas, A.; Fasoula, N.A.; Paul-Yuan, K.; Reber, J.; Kallmayer, M.; Bozhko, D.; Seeger, M.; Eckstein, H.H.; Wildgruber, M.; Ntziachristos, V. Cardiovascular optoacoustics: From mice to men—A review. Photoacoustics 2019, 14, 19–30. [Google Scholar] [CrossRef]
- Xie, Z.; Yang, Y.; He, Y.; Shu, C.; Chen, D.; Zhang, J.; Chen, J.; Liu, C.; Sheng, Z.; Liu, H.; et al. In vivo assessment of inflammation in carotid atherosclerosis by noninvasive photoacoustic imaging. Theranostics 2020, 10, 4694–4704. [Google Scholar] [CrossRef] [PubMed]
- Günther, J.S.; Knieling, F.; Träger, A.P.; Lang, W.; Meyer, A.; Regensburger, A.P.; Wagner, A.L.; Trollmann, R.; Woelfle, J.; Klett, D.; et al. Targeting Muscular Hemoglobin Content for Classification of Peripheral Arterial Disease by Noninvasive Multispectral Optoacoustic Tomography. JACC Cardiovasc. Imaging 2023, 16, 719–721. [Google Scholar] [CrossRef] [PubMed]
- Knieling, F.; Gonzales Menezes, J.; Claussen, J.; Schwarz, M.; Neufert, C.; Fahlbusch, F.B.; Rath, T.; Thoma, O.M.; Kramer, V.; Menchicchi, B.; et al. Raster-Scanning Optoacoustic Mesoscopy for Gastrointestinal Imaging at High Resolution. Gastroenterology 2018, 154, 807–809.e803. [Google Scholar] [CrossRef] [PubMed]
- Bhutiani, N.; Grizzle, W.E.; Galandiuk, S.; Otali, D.; Dryden, G.W.; Egilmez, N.K.; McNally, L.R. Noninvasive Imaging of Colitis Using Multispectral Optoacoustic Tomography. J. Nucl. Med. 2017, 58, 1009–1012. [Google Scholar] [CrossRef]
- Buehler, A.; Brown, E.; Paulus, L.P.; Eckstein, M.; Thoma, O.M.; Oraiopoulou, M.E.; Rother, U.; Hoerning, A.; Hartmann, A.; Neurath, M.F.; et al. Transrectal Absorber Guide Raster-Scanning Optoacoustic Mesoscopy for Label-Free In Vivo Assessment of Colitis. Adv. Sci. 2023, 10, e2300564. [Google Scholar] [CrossRef]
- Lei, H.; Johnson, L.A.; Eaton, K.A.; Liu, S.; Ni, J.; Wang, X.; Higgins, P.D.R.; Xu, G. Characterizing intestinal strictures of Crohn’s disease. Biomed. Opt. Express 2019, 10, 2542–2555. [Google Scholar] [CrossRef]
- Lei, H.; Johnson, L.A.; Liu, S.; Moons, D.S.; Ma, T.; Zhou, Q.; Rice, M.D.; Ni, J.; Wang, X.; Higgins, P.D.; et al. Characterizing intestinal inflammation and fibrosis in Crohn’s disease by photoacoustic imaging: Feasibility study. Biomed. Opt. Express 2016, 7, 2837–2848. [Google Scholar] [CrossRef]
- Waldner, M.J.; Knieling, F.; Egger, C.; Morscher, S.; Claussen, J.; Vetter, M.; Kielisch, C.; Fischer, S.; Pfeifer, L.; Hagel, A.; et al. Multispectral Optoacoustic Tomography in Crohn’s Disease: Noninvasive Imaging of Disease Activity. Gastroenterology 2016, 151, 238–240. [Google Scholar] [CrossRef]
- Knieling, F.; Neufert, C.; Hartmann, A.; Claussen, J.; Urich, A.; Egger, C.; Vetter, M.; Fischer, S.; Pfeifer, L.; Hagel, A.; et al. Multispectral Optoacoustic Tomography for Assessment of Crohn’s Disease Activity. N. Engl. J. Med. 2017, 376, 1292–1294. [Google Scholar] [CrossRef] [PubMed]
- Paulus, L.P.; Wagner, A.L.; Buehler, A.; Raming, R.; Jungert, J.; Simon, D.; Tascilar, K.; Schnell, A.; Gunther, J.; Rother, U.; et al. Multispectral optoacoustic tomography of the human intestine—Temporal precision and the influence of postprandial gastrointestinal blood flow. Photoacoustics 2023, 30, 100457. [Google Scholar] [CrossRef] [PubMed]
- Paulus, L.P.; Buehler, A.; Wagner, A.L.; Raming, R.; Jüngert, J.; Simon, D.; Tascilar, K.; Schnell, A.; Rother, U.; Eckstein, M.; et al. Contrast-Enhanced Multispectral Optoacoustic Tomography for Functional Assessment of the Gastrointestinal Tract. Adv. Sci. 2023, 10, e2302562. [Google Scholar] [CrossRef]
- Bhutiani, N.; Samykutty, A.; McMasters, K.M.; Egilmez, N.K.; McNally, L.R. In vivo tracking of orally-administered particles within the gastrointestinal tract of murine models using multispectral optoacoustic tomography. Photoacoustics 2019, 13, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Morscher, S.; Driessen, W.H.; Claussen, J.; Burton, N.C. Semi-quantitative Multispectral Optoacoustic Tomography (MSOT) for volumetric PK imaging of gastric emptying. Photoacoustics 2014, 2, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Pogacnik, J.S.; Salgado, G. Perianal Crohn’s Disease. Clin. Colon. Rectal Surg. 2019, 32, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Panes, J.; Rimola, J. Perianal fistulizing Crohn’s disease: Pathogenesis, diagnosis and therapy. Nat. Reviews. Gastroenterol. Hepatol. 2017, 14, 652–664. [Google Scholar] [CrossRef]
- Regensburger, A.P.; Fonteyne, L.M.; Jungert, J.; Wagner, A.L.; Gerhalter, T.; Nagel, A.M.; Heiss, R.; Flenkenthaler, F.; Qurashi, M.; Neurath, M.F.; et al. Detection of collagens by multispectral optoacoustic tomography as an imaging biomarker for Duchenne muscular dystrophy. Nat. Med. 2019, 25, 1905–1915. [Google Scholar] [CrossRef]
- Regensburger, A.P.; Wagner, A.L.; Danko, V.; Jungert, J.; Federle, A.; Klett, D.; Schuessler, S.; Buehler, A.; Neurath, M.F.; Roos, A.; et al. Multispectral optoacoustic tomography for non-invasive disease phenotyping in pediatric spinal muscular atrophy patients. Photoacoustics 2022, 25, 100315. [Google Scholar] [CrossRef] [PubMed]
- Regensburger, A.P.; Wagner, A.L.; Claussen, J.; Waldner, M.J.; Knieling, F. Shedding light on pediatric diseases: Multispectral optoacoustic tomography at the doorway to clinical applications. Mol. Cell Pediatr. 2020, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Regensburger, A.P.; Eckstein, M.; Wetzl, M.; Raming, R.; Paulus, L.-P.; Buehler, A.; Nedoschill, E.; Danko, V.; Jüngert, J.; Wagner, A.L.; et al. Multispectral optoacoustic tomography enables assessment of disease activity in paediatric inflammatory bowel disease. Photoacoustics 2024, 35, 100578. [Google Scholar] [CrossRef] [PubMed]
- Waterhouse, D.J.; Bano, S.; Januszewicz, W.; Stoyanov, D.; Fitzgerald, R.C.; di Pietro, M.; Bohndiek, S.E. First-in-human pilot study of snapshot multispectral endoscopy for early detection of Barrett’s-related neoplasia. J. Biomed. Opt. 2021, 26, 106002. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.M.; Favazza, C.; Chen, R.; Yao, J.; Cai, X.; Maslov, K.; Zhou, Q.; Shung, K.K.; Wang, L.V. Simultaneous functional photoacoustic and ultrasonic endoscopy of internal organs in vivo. Nat. Med. 2012, 18, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Stylogiannis, A.; Afshari, P.; Wiedemann, T.; Steiger, K.; Buehler, A.; Zakian, C.; Ntziachristos, V. Capsule optoacoustic endoscopy for esophageal imaging. J. Biophotonics 2019, 12, e201800439. [Google Scholar] [CrossRef] [PubMed]
- Goodsall, T.M.; Jairath, V.; Feagan, B.G.; Parker, C.E.; Nguyen, T.M.; Guizzetti, L.; Asthana, A.K.; Begun, J.; Christensen, B.; Friedman, A.B.; et al. Standardisation of intestinal ultrasound scoring in clinical trials for luminal Crohn’s disease. Aliment. Pharmacol. Ther. 2021, 53, 873–886. [Google Scholar] [CrossRef]
- Maaser, C.; Kucharzik, T.; Gecse, K. Is Intestinal Ultrasound Ready to be Used as Standard Monitoring Tool in Daily Practice and as Endpoint in Clinical Trials? J. Crohn’s Colitis 2021, 15, 1–2. [Google Scholar] [CrossRef]
- Kucharzik, T.; Wilkens, R.; D’Agostino, M.A.; Maconi, G.; Le Bars, M.; Lahaye, M.; Bravatà, I.; Nazar, M.; Ni, L.; Ercole, E.; et al. Early Ultrasound Response and Progressive Transmural Remission After Treatment With Ustekinumab in Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2023, 21, 153–163.e112. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).