

Full-Thickness Rectal Biopsy in Children Suspected of Having Hirschsprung’s Disease: The Inconclusive Biopsy
 ,
,
Abstract
:1. Introduction
2. Material and Methods
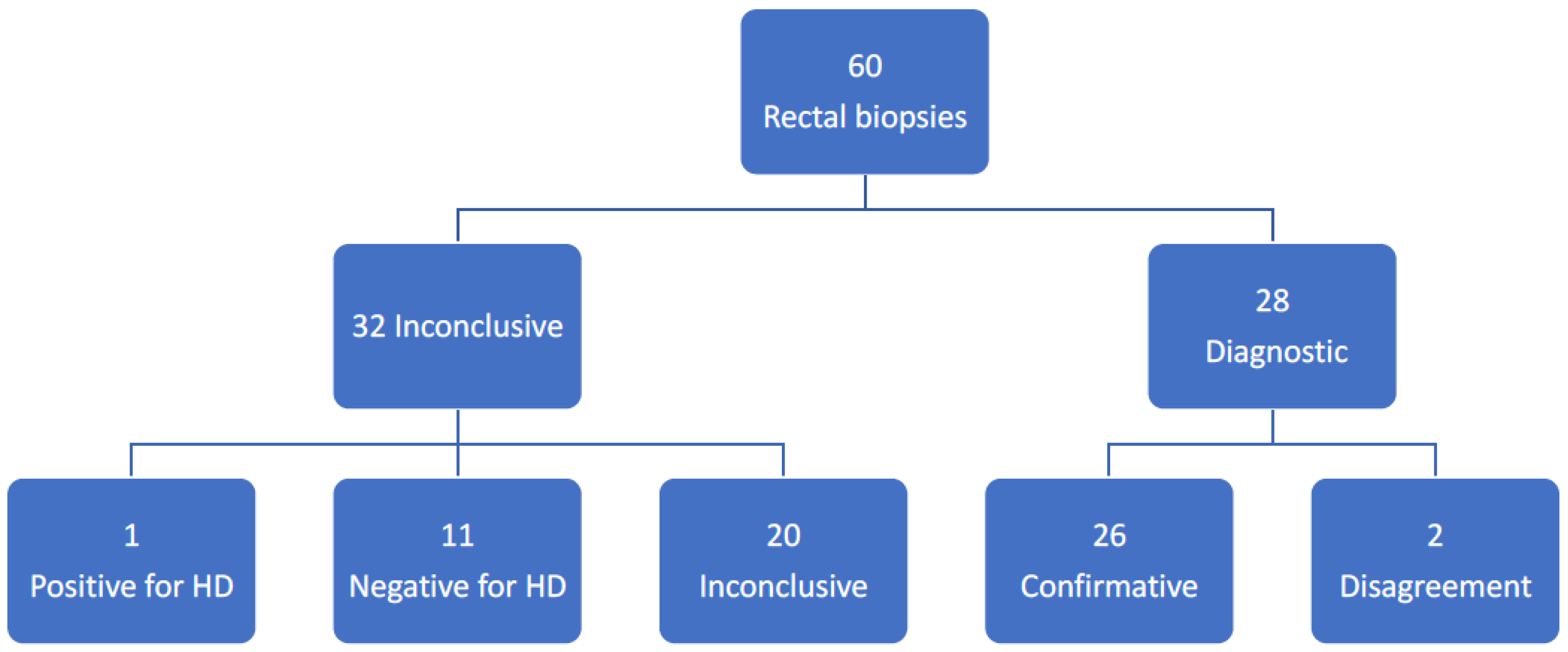
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muise, E.D.; Hardee, S.; Morotti, R.A.; Cowles, R.A. A comparison of suction and full-thickness rectal biopsy in children. J. Surg. Res. 2016, 201, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Imaizumi, T.; Murakami, H.; Nakamura, H.; Seo, S.; Koga, H.; Miyano, G.; Okawada, M.; Doi, T.; Lane, G.J.; Okazaki, T.; et al. Rectal mucosal/submucosal biopsy under general anesthesia ensures optimum diagnosis of bowel motility disorders. Pediatr. Surg. Int. 2016, 32, 1173–1176. [Google Scholar] [CrossRef] [PubMed]
- Takawira, C.; D’Agostini, S.; Shenouda, S.; Persad, R.; Sergi, C. Laboratory procedures update on Hirschsprung disease. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Meier-Ruge, W.A.; Bruder, E. Current consepts of immune histochemistry in modern pathology. Pathobiology 2008, 75, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Holland, S.K.; Hessler, R.B.; Reid-Nicholson, M.D.; Ramalingam, P.; Lee, J.R. Utilization of peripherin and S100 immunohistochemistry in the diagnosis of Hirschsprung disease. Mod. Pathol. 2010, 23, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, B.; Mukhopadhyay, M.; Mondal, K.C.; Sengupta, M.; Paul, A. Hirschsprung’s disease in neonates with special reference to calretinin I immunohistochemistry. J. Clin. Diagn. Res. 2015, 9, EC06-9. [Google Scholar] [CrossRef] [PubMed]
- Musa, Z.A.; Qaim, B.J.; Ghazi, H.F.; Shaikhly, W. Diagnostic roles of calretinin in Hirschsprung disease: A comparison to neuron-specific enolase. Saudi. J. Gastroenterol. 2017, 23, 60–66. [Google Scholar] [PubMed]
- Gonzalo, D.H.; Plesec, T. Hirschsprung disease and use of calretinin in inadequate rectal suction biopsies. Arch. Pathol. Lab. Med. 2013, 137, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Ambartsumyan, L.; Smith, C.; Kapur, R.P. Diagnosis of Hirschsprung disease. Pediatr. Dev. Pathol. 2020, 23, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Matsukuma, K.; Gui, D.; Saadai, P. Hirschsprung disease for the practicing surgical pathologist. Am. J. Clin. Pathol. 2023, 159, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, A.M.; Barbosa, A.J.; Carvalho, A.A.; Pinheiro, F.C.; Coelho, M.; Cabral, M.M.; Andrade, I.E. Usefulness of immunocytochemical demonstration of neuron-specific enolase in the diagnosis of Hirschsprung’s disease. J. Pediatr. Gastroenterol. Nutr. 1990, 11, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, L.; Besendörfer, M.; Carbon, R.; Lux, P.; Agaimy, A.; Hartmann, L.; Rau, T.T. Immunohistochemical panel for the diagnosis of Hirschsprung’s disease using antibodies to MAP2, calretinin, GLUT1 and S100. Histopathology 2015, 66, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Li, K.; Li, S.; Yang, D.; Zhang, X.; Fang, M.; Cao, G.; Wang, Y.; Chen, W.; Tang, C. Calretinin, S100 and protein gene product 9.5 immunostaining of rectal suction biopsies in the diagnosis of Hirschsprung’s disease. Am. J. Transl. Res. 2016, 8, 3159–3168. [Google Scholar] [PubMed]
- Galazka, P.; Szyllberg, L.; Bodnar, M.; Styczykinski, J.; Marszalek, A. Diagnostic algorithm in Hirschsprung’s disease: Focus on immunochemistry markers. In Vivo 2020, 34, 1355–1359. [Google Scholar] [CrossRef] [PubMed]
- Aziz, Z.W.; Al Hajjar, B.K.; Al Hajjar, Z.A.A.; Almola, E.M.A.; Jawher, N.M.T.; Muhammad, R.K. Diagnostic accuracy of haematoxylin-eosin staining in comparison to calretinin and S100 for the assessment of ganglion cells in rectal biopsy. J. Pak. Med. Assoc. 2022, 72, 1123–1127. [Google Scholar] [PubMed]
- de Arruda Lourencao, P.L.T.; Takegawa, B.K.; Ortolan, E.V.; Terra, S.A.; Rodriques, M.A.M. Does calretinin immunohistochemistry reduce inconclusive diagnosis in rectal biopsies for Hirschsprung’s disease. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Guinard-Saumel, V.; Bonnard, A.; de Lagausie, P.; Philippe-Chromette, P.; Alberti, C.; El Ghoneimi, A.; Peuchmaur, M.; Berrebi-Binczak, D. Calretinin immunohistochemistry. A simple and efficient tool to diagnose Hirschsprung disease. Mod. Pathol. 2009, 22, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Meinds, R.J.; Kuiper, G.; Parry, K.; Timmer, A.; Groen, H.; Heineman, E.; Broens, P.M.A. Onfant’s age influences the accuracy of rectal suction biopsies for diagnosing of Hirschsprung’s disease. Clin. Gastroenterol. Hepatol. 2015, 13, 1801–18077. [Google Scholar] [CrossRef] [PubMed]
- Green, N.; Smith, C.A.; Bradford, M.C.; Ambartsumyan, L.; Kapur, R.P. Rectal suction biopsy versus incisional rectal biopsy in the diagnosis of Hirschsprung disease. Pediatr. Surg. Int. 2022, 38, 1989–1996. [Google Scholar] [CrossRef] [PubMed]
- De Lorijn, F.; Reitsma, J.B.; Voskuijl, W.P.; Aronson, D.C.; Kate, F.J.T.; Smets, A.M.J.B.; Taminiau, J.A.J.M.; Beninga, M.A. Diagnosis of Hirschsprung’s disease. A prospective, comparative accuracy study of common tests. J. Pediatr. 2005, 146, 787–792. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reason | Number of Biopsies |
|---|---|
| Lack of tunica mucularis | 23 |
| Biopsy taken too close to the dentate line. | 5 |
| The Biopsy is too small | 2 |
| Others | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korsager, L.E.H.; Bjørn, N.; Ellebæk, M.B.; Christensen, L.G.; Qvist, N. Full-Thickness Rectal Biopsy in Children Suspected of Having Hirschsprung’s Disease: The Inconclusive Biopsy. Children 2023, 10, 1619. https://doi.org/10.3390/children10101619
Korsager LEH, Bjørn N, Ellebæk MB, Christensen LG, Qvist N. Full-Thickness Rectal Biopsy in Children Suspected of Having Hirschsprung’s Disease: The Inconclusive Biopsy. Children. 2023; 10(10):1619. https://doi.org/10.3390/children10101619
Chicago/Turabian StyleKorsager, Leise Elisabeth Hviid, Niels Bjørn, Mark Bremholm Ellebæk, Lene Gaardsmand Christensen, and Niels Qvist. 2023. "Full-Thickness Rectal Biopsy in Children Suspected of Having Hirschsprung’s Disease: The Inconclusive Biopsy" Children 10, no. 10: 1619. https://doi.org/10.3390/children10101619
APA StyleKorsager, L. E. H., Bjørn, N., Ellebæk, M. B., Christensen, L. G., & Qvist, N. (2023). Full-Thickness Rectal Biopsy in Children Suspected of Having Hirschsprung’s Disease: The Inconclusive Biopsy. Children, 10(10), 1619. https://doi.org/10.3390/children10101619