

Acute Kidney Injury in Very Low Birth Weight Infants: A Major Morbidity and Mortality Risk Factor

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Acute Kidney Injury
2.4. Outcomes
2.5. Statistical Analysis
3. Results
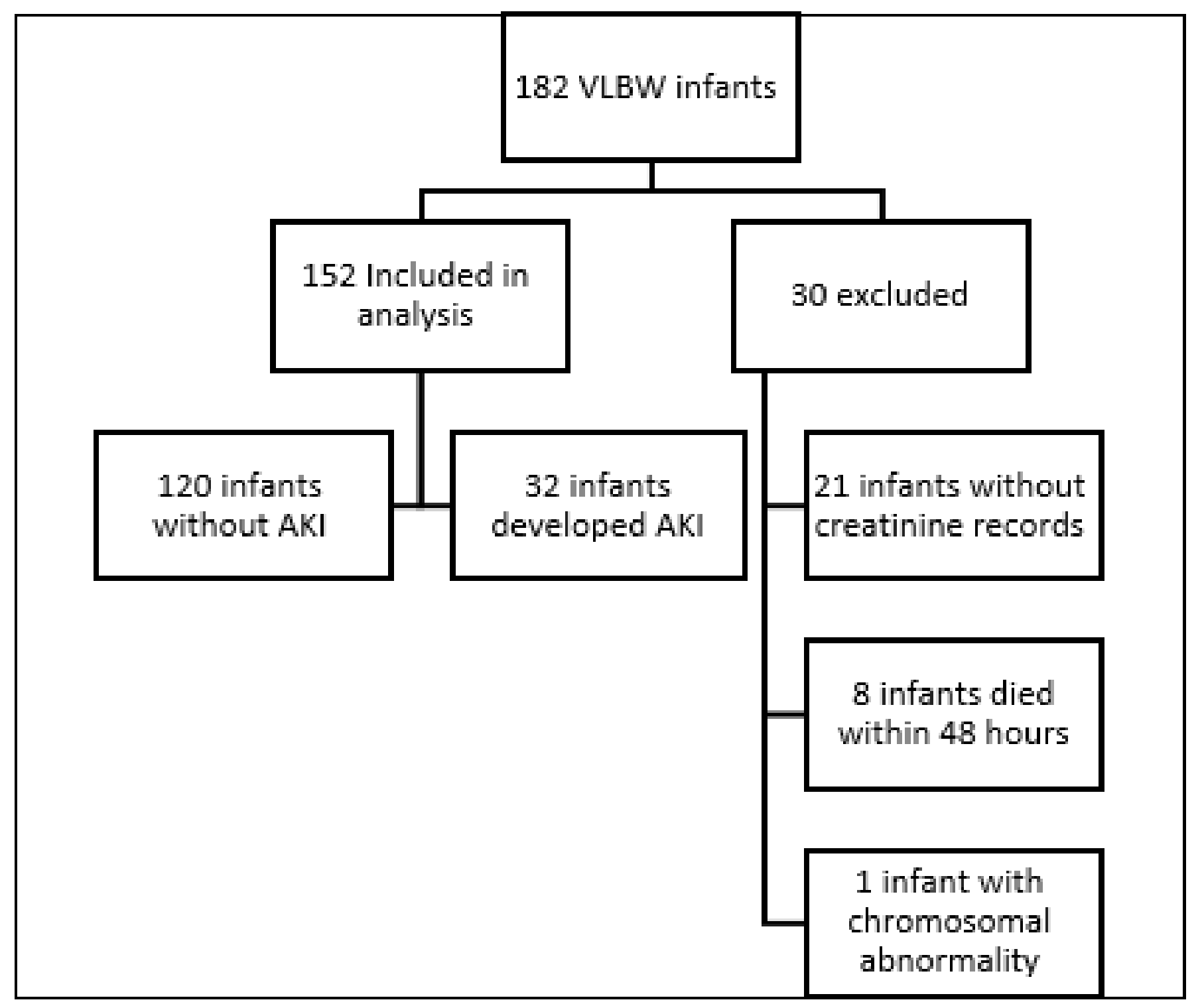
3.1. Study Group
3.2. Characteristics of AKI Patients
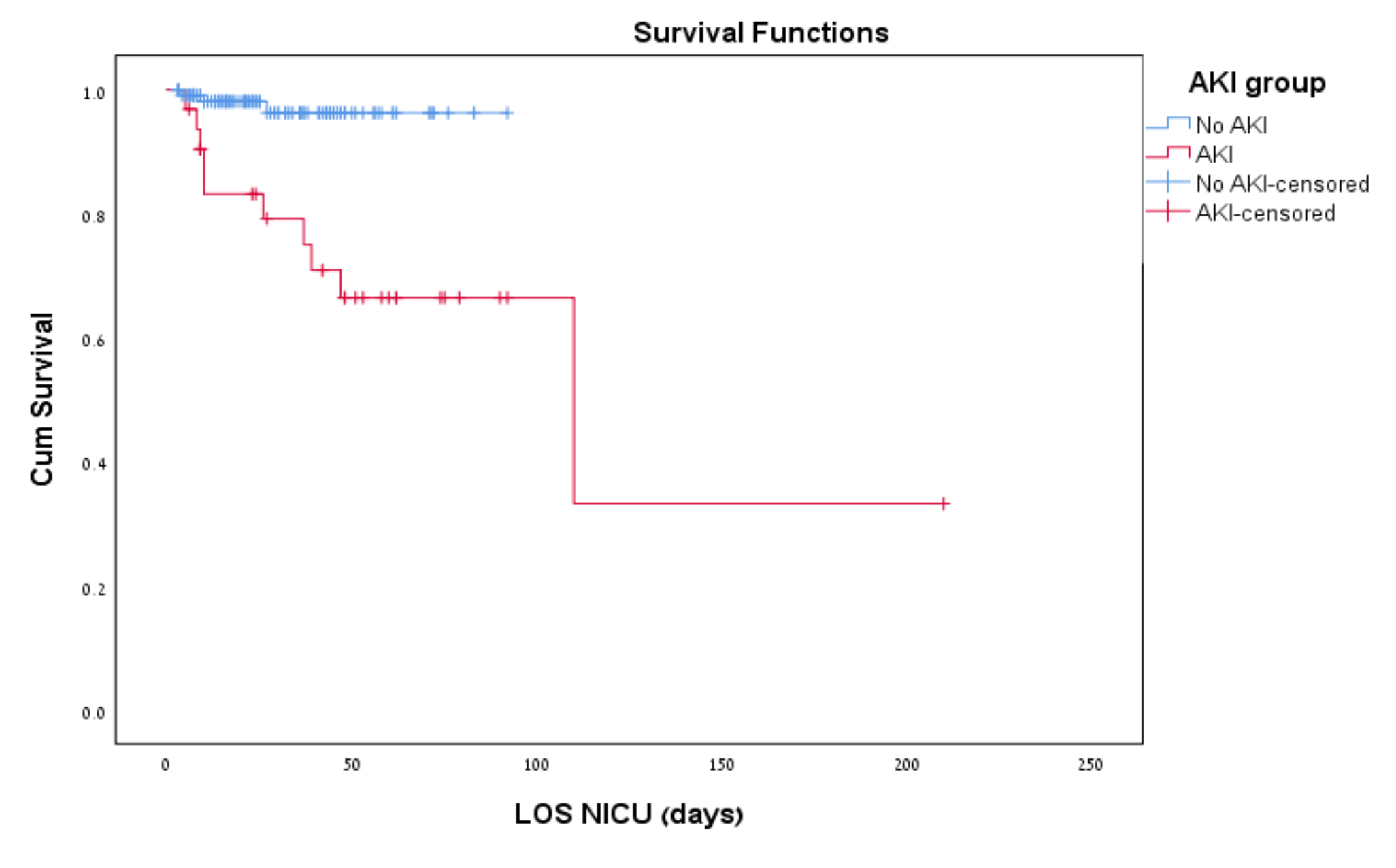
3.3. Outcome
3.3.1. Risk Factors Associated with AKI—Univariate Analysis
3.3.2. Risk Factors Associated with AKI—Multivariate Analysis
3.3.3. Multivariate Analysis—Risk Factors for Mortality in VLBW
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, S.; Schmicker, R.H.; Brophy, P.D.; Heagerty, P.J.; Juul, S.E.; Goldstein, S.L.; Askenazi, D. Severe acute kidney injury and mortality in extremely low gestational age neonates. CJASN 2021, 16, 862–869. [Google Scholar] [CrossRef] [PubMed]
- Starr, M.C.; Charlton, J.R.; Guillet, R.; Reidy, K.; Tipple, T.E.; Jetton, J.G.; Kent, A.L.; Abitbol, C.L.; Ambalavanan, N.; Mhanna, M.J.; et al. Advances in neonatal acute kidney injury. Pediatrics 2021, 148, e2021051220. [Google Scholar] [CrossRef] [PubMed]
- Jetton, J.G.; Guillet, R.; Askenazi, D.J.; Dill, L.; Jacobs, J.; Kent, A.L.; Selewski, D.T.; Abitbol, C.L.; Kaskel, F.J.; Mhanna, M.J.; et al. Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates: Design of a Retrospective Cohort Study. Front. Pediatr. 2016, 4, 68. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef]
- Bruel, A.; Rozé, J.-C.; Flamant, C.; Simeoni, U.; Roussey-Kesler, G.; Allain-Launay, E. Critical serum creatinine values in very preterm newborns. PLoS ONE 2013, 8, e84892. [Google Scholar] [CrossRef]
- Askenazi, D.; Abitbol, C.; Boohaker, L.; Griffin, R.; Raina, R.; Dower, J.; Davis, T.K.; Ray, P.E.; Perazzo, S.; DeFreitas, M.; et al. Optimizing the AKI Definition during First Postnatal Week Using Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates (AWAKEN) Cohort. Pediatr. Res. 2019, 85, 329–338. [Google Scholar] [CrossRef]
- Abitbol, C.L.; DeFreitas, M.J.; Strauss, J. Assessment of kidney function in preterm infants: Lifelong implications. Pediatr. Nephrol. 2016, 31, 2213–2222. [Google Scholar] [CrossRef]
- Filler, G.; Bhayana, V.; Schott, C.; Díaz-González de Ferris, M.E. How should we assess renal function in neonates and infants? Acta Paediatr. 2021, 110, 773–780. [Google Scholar] [CrossRef]
- Askenazi, D.J.; Heagerty, P.J.; Schmicker, R.H.; Griffin, R.; Brophy, P.; Juul, S.E.; Mayock, D.E.; Goldstein, S.L.; Hingorani, S.; PENUT Trial Consortium. Prevalence of acute kidney injury (AKI) in Extremely Low Gestational Age Neonates (ELGAN). Pediatr. Nephrol. 2020, 35, 1737–1748. [Google Scholar] [CrossRef]
- Carmody, J.B.; Swanson, J.R.; Rhone, E.T.; Charlton, J.R. Recognition and reporting of AKI in very low birth weight infants. Clin. J. Am. Soc. Nephrol. 2014, 9, 2036–2043. [Google Scholar] [CrossRef]
- Osathanondh, V.; Potter, E.L. Development of human kidney as shown by microdissection. III. Formation and interrelationship of collecting tubules and nephrons. Arch. Pathol. 1963, 76, 290–302. [Google Scholar]
- Rodríguez, M.M.; Gómez, A.H.; Abitbol, C.L.; Chandar, J.J.; Duara, S.; Zilleruelo, G.E. Histomorphometric analysis of postnatal glomerulogenesis in extremely preterm infants. Pediatr. Dev. Pathol. 2004, 7, 17–25. [Google Scholar] [CrossRef]
- Zohdi, V.; Sutherland, M.R.; Lim, K.; Gubhaju, L.; Zimanyi, M.A.; Black, M.J. Low birth weight due to intrauterine growth restriction and/or preterm birth: Effects on nephron number and long-term renal health. Int. J. Nephrol. 2012, 2012, 136942. [Google Scholar] [CrossRef]
- Black, M.J.; Sutherland, M.R.; Gubhaju, L.; Kent, A.L.; Dahlstrom, J.E.; Moore, L. When birth comes early: Effects on Nephrogenesis. Nephrology 2013, 18, 180–182. [Google Scholar] [CrossRef]
- Brennan, S.; Watson, D.L.; Rudd, D.M.; Kandasamy, Y. Kidney growth following preterm birth: Evaluation with renal parenchyma ultrasonography. Pediatr. Res. 2022. ahead of print. [Google Scholar] [CrossRef]
- Charlton, J.R.; Baldelomar, E.J.; Hyatt, D.M.; Bennett, K.M. Nephron number and its determinants: A 2020 update. Pediatr. Nephrol. 2021, 36, 797–807. [Google Scholar] [CrossRef]
- Charlton, J.R.; Baldelomar, E.J.; de Ronde, K.A.; Cathro, H.P.; Charlton, N.P.; Criswell, S.J.; Hyatt, D.M.; Nam, S.; Pearl, V.; Bennett, K.M. Nephron loss detected by MRI following neonatal acute kidney injury in rabbits. Pediatr. Res. 2020, 87, 1185–1192. [Google Scholar] [CrossRef]
- Makayes, Y.; Resnick, E.; Hinden, L.; Aizenshtein, E.; Shlomi, T.; Kopan, R.; Nechama, M.; Volovelsky, O. Increasing MTORC1 pathway activity or methionine supplementation during pregnancy reverses the negative effect of maternal malnutrition on the developing kidney. J. Am. Soc. Nephrol. 2021, 32, 1898–1912. [Google Scholar] [CrossRef]
- Su, S.W.; Stonestreet, B.S. Core concepts: Neonatal glomerular filtration rate. NeoReviews 2010, 11, e714–e721. [Google Scholar] [CrossRef]
- Abitbol, C.L.; Seeherunvong, W.; Galarza, M.G.; Katsoufis, C.; Francoeur, D.; Defreitas, M.; Edwards-Richards, A.; Master Sankar Raj, V.; Chandar, J.; Duara, S.; et al. Neonatal Kidney Size and Function in Preterm Infants: What Is a True Estimate of Glomerular Filtration Rate? J. Pediatr. 2014, 164, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Hyink, D.P.; Abrahamson, D.R. Origin of the glomerular vasculature in the developing kidney. Semin. Nephrol. 1995, 15, 300–314. [Google Scholar]
- Iacobelli, S.; Guignard, J.-P. Maturation of glomerular filtration rate in neonates and infants: An overview. Pediatr. Nephrol. 2021, 36, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Nada, A.; Bonachea, E.M.; Askenazi, D.J. Acute kidney injury in the fetus and neonate. Semin. Fetal Neonatal Med. 2017, 22, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Koralkar, R.; Ambalavanan, N.; Levitan, E.B.; Mcgwin, G.; Goldstein, S.; Askenazi, D. Acute kidney injury reduces survival in very low birth weight infants. Pediatr Res. 2011, 69, 354–358. [Google Scholar] [CrossRef]
- Jetton, J.G.; Boohaker, L.J.; Sethi, S.K.; Wazir, S.; Rohatgi, S.; Soranno, D.E.; Chishti, A.S.; Woroniecki, R.; Mammen, C.; Swanson, J.R.; et al. Incidence and outcomes of neonatal acute kidney injury (AWAKEN): A multicentre, multinational, observational cohort study. Lancet Child Adolesc. Health 2017, 1, 184–194. [Google Scholar] [CrossRef]
- Üstün, N.; Arslanoglu, S.; Ovali, F. Antenatal steroids and acute kidney injury in preterm infants. Am. J. Perinatol. 2022, 39, 1334–1340. [Google Scholar] [CrossRef]
- Bonsante, F.; Ramful, D.; Binquet, C.; Samperiz, S.; Daniel, S.; Gouyon, J.-B.; Iacobelli, S. Low renal oxygen saturation at near-infrared spectroscopy on the first day of life is associated with developing acute kidney injury in very preterm infants. Neonatology 2019, 115, 198–204. [Google Scholar] [CrossRef]
- Gist, K.M.; Selewski, D.T.; Brinton, J.; Menon, S.; Goldstein, S.L.; Basu, R.K. Assessment of the independent and synergistic effects of fluid overload and acute kidney injury on outcomes of critically Ill children. Pediatr. Crit. Care Med. 2020, 21, 170–177. [Google Scholar] [CrossRef]
- Flori, H.R.; Church, G.; Liu, K.D.; Gildengorin, G.; Matthay, M.A. Positive fluid balance is associated with higher mortality and prolonged mechanical ventilation in pediatric patients with acute lung injury. Crit. Care Res. Pract. 2011, 2011, 854142. [Google Scholar] [CrossRef]
- Goldstein, S.L.; Currier, H.; Graf Cd Cosio, C.C.; Brewer, E.D.; Sachdeva, R. Outcome in Children receiving continuous venovenous hemofiltration. Pediatrics 2001, 107, 1309–1312. [Google Scholar] [CrossRef]
- Sanderson, K.R.; Harshman, L.A. Renal replacement therapies for infants and children in the ICU. Curr. Opin. Pediatr. 2020, 32, 360–366. [Google Scholar] [CrossRef]
- Ye, Z.; Wang, Y.; Ge, L.; Guyatt, G.H.; Collister, D.; Alhazzani, W.; Bagshaw, S.M.; Belley-Cote, E.P.; Fang, F.; Hou, L.; et al. Comparing renal replacement therapy modalities in critically Ill patients with acute kidney injury: A systematic review and network meta-analysis. Crit. Care Explor. 2021, 3, e0399. [Google Scholar] [CrossRef]
- Harshman, L.A.; Muff-Luett, M.; Neuberger, M.L.; Dagle, J.M.; Shilyansky, J.; Nester, C.M.; Brophy, P.D.; Jetton, J.G. Peritoneal dialysis in an extremely low-birth-weight infant with acute kidney injury. Clin. Kidney J. 2014, 7, 582–585. [Google Scholar] [CrossRef]
- Kaddourah, A.; Goldstein, S.L. Renal replacement therapy in neonates. Clin. Perinatol. 2014, 41, 517–527. [Google Scholar] [CrossRef]
- Starr, M.C.; Boohaker, L.; Eldredge, L.C.; Menon, S.; Griffin, R.; Mayock, D.E.; Li, L.; Askenazi, D.; Hingorani, S.; Neonatal Kidney Collaborative. Acute kidney injury and bronchopulmonary dysplasia in premature neonates born less than 32 weeks’ gestation. Am. J. Perinatol. 2020, 37, 341–348. [Google Scholar] [CrossRef]
- Stoops, C.; Sims, B.; Griffin, R.; Askenazi, D.J. Neonatal Acute kidney injury and the risk of intraventricular hemorrhage in the very low birth weight infant. Neonatology 2016, 110, 307–312. [Google Scholar] [CrossRef]
- Majed, B.; Bateman, D.A.; Uy, N.; Lin, F. Patent ductus arteriosus is associated with acute kidney injury in the preterm infant. Pediatr. Nephrol. 2019, 34, 1129–1139. [Google Scholar] [CrossRef]
- Stoops, C.; Stone, S.; Evans, E.; Dill, L.; Henderson, T.; Griffin, R.; Goldstein, S.L.; Coghill, C.; Askenazi, D.J. Baby NINJA (Nephrotoxic Injury Negated by Just-in-Time Action): Reduction in nephrotoxic medication-associated acute kidney injury in the neonatal intensive care unit. J. Pediatr. 2019, 215, 223–228. [Google Scholar] [CrossRef]
- Bancalari, E.; Claure, N. Definitions and Diagnostic Criteria for Bronchopulmonary Dysplasia. Semin. Perinatol. 2006, 30, 164–170. [Google Scholar] [CrossRef]
- Neu, J. Necrotizing enterocolitis: The search for a unifying pathogenic theory leading to prevention. Pediatr. Clin. N. Am. 1996, 43, 409–432. [Google Scholar] [CrossRef] [PubMed]
- Zappitelli, M.; Ambalavanan, N.; Askenazi, D.J.; Moxey-Mims, M.; Kimmel, P.L.; Star, R.A.; Abitbol, C.L.; Brophy, P.D.; Hidalgo, G.; Hanna, M.; et al. Developing a neonatal acute kidney injury research definition: A report from the NIDDK neonatal AKI workshop. Pediatr. Res. 2017, 82, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Elmas, A.T.; Tabel, Y.; Özdemir, R. Risk factors and mortality rate in premature babies with acute kidney injury. J. Clin. Lab. Anal. 2018, 32, e22441. [Google Scholar] [CrossRef] [PubMed]
- Ting, J.Y.; McDougal, K.; De Mello, A.; Kwan, E.; Mammen, C. Acute Kidney injury among preterm infants receiving nonsteroidal anti-inflammatory drugs: A pilot study. Pediatr. Neonatol. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Branagan, A.; Costigan, C.S.; Stack, M.; Slagle, C.; Molloy, E.J. Management of acute kidney injury in extremely low birth weight infants. Front. Pediatr. 2022, 10, 867715. [Google Scholar] [CrossRef]
- Hanna, M.; Brophy, P.D.; Giannone, P.J.; Joshi, M.S.; Bauer, J.A.; RamachandraRao, S. Early urinary biomarkers of acute kidney injury in preterm infants. Pediatr. Res. 2016, 80, 218–223. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, H.; Pei, J.; Jiang, X.; Tang, J. Acute kidney injury in premature and low birth weight neonates: A systematic review and meta-analysis. Pediatr. Nephrol. 2022, 37, 275–287. [Google Scholar] [CrossRef]
- Aziz, K.B.; Schles, E.M.; Makker, K.; Wynn, J.L. Frequency of acute kidney injury and association with mortality among extremely preterm infants. JAMA Netw. Open 2022, 5, e2246327. [Google Scholar] [CrossRef]
- Elgendy, M.M.; Othman, H.F.; Younis, M.; Puthuraya, S.; Matar, R.B.; Aly, H. Trends and racial disparities for acute kidney injury in premature infants: The US national database. Pediatr. Nephrol. 2021, 36, 2789–2795. [Google Scholar] [CrossRef]
- Masumoto, K.; Kusuda, S. Hemodynamic support of the micropreemie: Should hydrocortisone never be left out? Semin. Fetal Neonatal Med. 2021, 26, 101222. [Google Scholar] [CrossRef]
- Hundscheid, T.; Onland, W.; Kooi, E.M.W.; Vijlbrief, D.C.; de Vries, W.B.; Dijkman, K.P.; van Kaam, A.H.; Villamor, E.; Kroon, A.A.; Visser, R.; et al. Expectant Management or Early Ibuprofen for Patent Ductus Arteriosus. N. Engl. J. Med. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Velazquez, D.M.; Reidy, K.J.; Sharma, M.; Kim, M.; Vega, M.; Havranek, T. The effect of hemodynamically significant patent ductus arteriosus on acute kidney injury and systemic hypertension in extremely low gestational age newborns. J. Matern Fetal Neonatal Med 2019, 32, 3209–3214. [Google Scholar] [CrossRef]
- Coggins, S.A.; Laskin, B.; Harris, M.C.; Grundmeier, R.W.; Passarella, M.; McKenna, K.J.; Srinivasan, L. Acute kidney injury associated with late-onset neonatal sepsis: A matched cohort study. J. Pediatr. 2021, 231, 185–192.e4. [Google Scholar] [CrossRef]
- Barbosa, J.D.S.; Silva Júnior, G.B.D.; Meneses, G.C.; Martins, A.M.C.; Daher, E.F.; Machado, R.P.G.; Lemes, R.P.G. Use of non-conventional biomarkers in the early diagnosis of acute kidney injury in preterm newborns with sepsis. J. Bras. Nefrol. 2022, 44, 97–108. [Google Scholar] [CrossRef]
- Bowen, J.R.; Callander, I.; Richards, R.; Lindrea, K.B.; Sepsis Prevention in NICUs Group. Decreasing Infection in Neonatal Intensive Care Units through Quality Improvement. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F51–F57. [Google Scholar] [CrossRef]
- Neill, S.; Haithcock, S.; Smith, P.B.; Goldberg, R.; Bidegain, M.; Tanaka, D.; Carriker, C.; Ericson, J.E. Sustained Reduction in Bloodstream Infections in Infants at a Large Tertiary Care Neonatal Intensive Care Unit. Adv. Neonatal Care 2016, 16, 52–59. [Google Scholar] [CrossRef]
- Cleper, R.; Shavit, I.; Blumenthal, D.; Reisman, L.; Pomeranz, G.; Haham, A.; Friedman, S.; Goldiner, I.; Mandel, D. Neonatal Acute Kidney Injury: Recording Rate, Course, and Outcome: One Center Experience. J. Matern Fetal Neonatal Med. 2019, 32, 3379–3385. [Google Scholar] [CrossRef]
- Simmons, E.M.; Himmelfarb, J.; Sezer, M.T.; Chertow, G.M.; Mehta, R.L.; Paganini, E.P.; Soroko, S.; Freedman, S.; Becker, K.; Spratt, D.; et al. Plasma cytokine levels predict mortality in patients with acute renal failure. Kidney Int. 2004, 65, 1357–1365. [Google Scholar] [CrossRef]
- Jefferies, J.L.; Goldstein, S.L. Cardorenal syndrome: An emerging problem in pediatric critical care. Pediatr. Nephrol. 2013, 28, 855–862. [Google Scholar] [CrossRef]
- Arcinue, R.; Kantak, A.; Elkhwad, M. Acute kidney injury in ELBW Infants (< 750 Grams) and its associated risk factors. J. Neonatal Perinatal Med. 2015, 8, 349–357. [Google Scholar] [CrossRef]
- Csaicsich, D.; Russo-Schlaff, N.; Messerschmidt, A.; Weninger, M.; Pollak, A.; Aufricht, C. Renal failure, comorbidity and mortality in preterm infants. Wien Klin Wochenschr 2008, 120, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Adegboyega, O.O.; Singh, Y.; Bhutada, A.; Kupferman, J.C.; Rastogi, S. Recurrent acute kidney injury in preterm neonates is common and associated with worse outcomes and higher mortality. Pediatr. Res. 2022, 92, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Askenazi, D.; Patil, N.R.; Ambalavanan, N.; Balena-Borneman, J.; Lozano, D.J.; Ramani, M.; Collins, M.; Griffin, R.L. Acute kidney injury is associated with bronchopulmonary dysplasia/mortality in premature infants. Pediatr. Nephrol. 2015, 30, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Askenazi, D.J.; Morgan, C.; Goldstein, S.L.; Selewski, D.T.; Moxey-Mims, M.M.; Kimmel, P.L.; Star, R.A.; Higgins, R.; Laughon, M. Strategies to improve the understanding of long-term renal consequences after neonatal acute kidney injury. Pediatr. Res. 2016, 79, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, V.A. Preterm birth and its impact on renal health. Semin. Nephrol. 2017, 37, 311–319. [Google Scholar] [CrossRef]
- Vikse, B.E.; Irgens, L.M.; Leivestad, T.; Hallan, S.; Iversen, B.M. Low birth weight increases risk for end-stage renal disease. J. Am. Soc. Nephrol. 2008, 19, 151–157. [Google Scholar] [CrossRef]
- Kumar, V.H.S. Cardiovascular morbidities in adults born preterm: Getting to the heart of the matter! Children 2022, 9, 1843. [Google Scholar] [CrossRef]
- Sutherland, M.R.; Gubhaju, L.; Moore, L.; Kent, A.L.; Dahlstrom, J.E.; Horne, R.S.C.; Hoy, W.E.; Bertram, J.F.; Black, M.J. Accelerated maturation and abnormal morphology in the preterm neonatal kidney. J. Am. Soc. Nephrol. 2011, 22, 1365–1374. [Google Scholar] [CrossRef]
- Singhal, A.; Cole, T.J.; Lucas, A. Early nutrition in preterm infants and later blood pressure: Two cohorts after randomised trials. Lancet 2001, 357, 413–419. [Google Scholar] [CrossRef]
- Fanos, V.; Castagnola, M.; Faa, G. Prolonging nephrogenesis in preterm infants: A new approach for prevention of kidney disease in adulthood? Iran J. Kidney Dis. 2015, 9, 180–185. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| No AKI (n = 120) | AKI (n = 32) | p-Value | |
|---|---|---|---|
| Male gender | 68 (57%) | 15 (47%) | 0.323 |
| GA (mean week ± SD) | 29.12 ± 2.6 | 26.4 ± 2.7 | p < 0.001 |
| Birth weight (mean ± SD) | 1118 ± 235 | 906 ± 282 | p < 0.001 |
| Cord PH | 7.29 ± 0.08 | 7.32 ± 0.08 | 0.095 |
| Apgar score in 1st minute <7 | 50 (42%) | 16 (50%) | 0.43 |
| Apgar score in 5 min <7 | 9 (7.5%) | 8 (25%) | 0.01 |
| Temperature at 15 min from admission | 36.7 ± 0.53 | 36.3 ± 1.24 | 0.13 |
| RDS | 51 (42%) | 21 (65%) | 0.012 |
| TTN | 15 (12.5%) | 1 (3.2%) | 0.308 |
| PDA | 21 (17.5%) | 17 (53%) | p < 0.001 |
| Ibuprofen for PDA closure | 3 (14% of infants with PDA) | 2 (11% of infants with PDA) | 1 |
| Vasopressors medications | 6 (5%) | 12 (37.5%) | p < 0.001 |
| BSI | 5 (4%) | 9 (28%) | p < 0.001 |
| NEC | 12 (10%) | 13 (41%) | p < 0.001 |
| Surgical NEC | 1 (1%) | 9 (28%) | 0.01 |
| No AKI (n = 120) | AKI (n = 32) | p-Value | |
|---|---|---|---|
| BPD | 34 (28%) | 15 (47%) | 0.057 |
| Postnatal Steroids for BPD | 20 (17%) | 11 (34%) | 0.035 |
| Death | 3 (2.5%) | 10 (31%) | p < 0.001 |
| Significance | Adjusted OR | 95% Confidence Interval | |
|---|---|---|---|
| Vasopressors | 0.003 | 6.81 | (1.88, 24.6) |
| PDA | 0.012 | 3.62 | (1.32, 9.93) |
| BSI | 0.025 | 4.77 | (1.21, 18.78) |
| Significance | Adjusted OR | 95% Confidence Interval | |
|---|---|---|---|
| Vasopressors | 0.000 | 38.48 | (7.26, 204) |
| Acute kidney injury | 0.006 | 10.6 | (1.98, 56.99) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazarovits, G.; Ofek Shlomai, N.; Kheir, R.; Bdolah Abram, T.; Eventov Friedman, S.; Volovelsky, O. Acute Kidney Injury in Very Low Birth Weight Infants: A Major Morbidity and Mortality Risk Factor. Children 2023, 10, 242. https://doi.org/10.3390/children10020242
Lazarovits G, Ofek Shlomai N, Kheir R, Bdolah Abram T, Eventov Friedman S, Volovelsky O. Acute Kidney Injury in Very Low Birth Weight Infants: A Major Morbidity and Mortality Risk Factor. Children. 2023; 10(2):242. https://doi.org/10.3390/children10020242
Chicago/Turabian StyleLazarovits, Gilad, Noa Ofek Shlomai, Raed Kheir, Tali Bdolah Abram, Smadar Eventov Friedman, and Oded Volovelsky. 2023. "Acute Kidney Injury in Very Low Birth Weight Infants: A Major Morbidity and Mortality Risk Factor" Children 10, no. 2: 242. https://doi.org/10.3390/children10020242
APA StyleLazarovits, G., Ofek Shlomai, N., Kheir, R., Bdolah Abram, T., Eventov Friedman, S., & Volovelsky, O. (2023). Acute Kidney Injury in Very Low Birth Weight Infants: A Major Morbidity and Mortality Risk Factor. Children, 10(2), 242. https://doi.org/10.3390/children10020242