Abstract
The European Commission has highlighted the development of entrepreneurship competence in lifelong learning skills. In this way, the present study aims to contribute towards fostering the intrapreneurial mindset in healthcare settings. The focus of attention is on the relationship between organizational structures and processes (work-related content and content, specifically psychosocial risk factors), as well as individual wellbeing factors (distress and resilient coping) that could be relevant not only for the promotion of organizational wellbeing, but also to ensure an intrapreneurship-friendly environment (through the promotion of self-efficacy). An empirical study was conducted involving 333 formal caregivers of healthcare services. Portuguese versions of the instruments Kessler Psychological Distress Scale (K10), Brief Resilient Coping Scale (BRCS), and Copenhagen Psychosocial Questionnaire (COPSOQ III, medium version) were employed. Results show that resilience and distress (at the individual level), as well as role clarity, control over working time, and job insecurity (at the organizational level) are predisposing factors for self-efficacy, which are highlighted as essential to ensure an enabling environment for intrapreneurship and wellbeing. For practical consideration, we present an entrepreneurial mindset development strategy through the implementation of cause-related marketing as a pedagogical tool for entrepreneurship within the organization, which allows for experimentation and the necessary creative flexibility.
1. Introduction
The “New Skills Agenda for Europe: Working Together to Strengthen Human Capital, Employability, and Competitiveness” [1], proposed by The European Commission (EC), intends to address the need to take action to promote employability and prosperity through the skills developed in its citizens. The EC recognises that it is not enough just to increase the level of qualifications held by citizens, but that it is also necessary to promote the acquisition of skills (through formal or informal means) with quality. In this sense, the European Union (EU) has been creating key competences frameworks in order to increase the literacy of Europeans in those same areas, creating self-assessment models and establishing lifelong learning objectives [1,2]. Under this competences framework, assessment and learning models have been created, of which we highlight the EntreComp (entrepreneurial competencies). It is grounded on three axes of an entrepreneurial process, which reflect the main temporal and spatial variables of business action, namely, “in-action”, “ideas and opportunities”, and “resources” [3,4]. It is worth pointing out that, usually, entrepreneurial competencies are often related to skills and innovation processes needed by independent owner–managers to develop a new product and/or independent business venture [5]. Thus, entrepreneurship can be interpreted in its broader meaning as the ability and willingness to conceive, develop, and manage a business. However, nowadays, this concept goes beyond its economic dimension; this process should consider economic, ecological, and social development as a triad of added value to generate a positive impact on sustainable economic growth corresponding to an extension of entrepreneurship that incorporates these three aspects, namely, sustainable entrepreneurship [6,7].
On the other hand, entrepreneurial behaviour is also found among employees within organisations (where it is known as intrapreneurship) as a mechanism for economic and social adjustment [5,8,9,10,11]. It should be noted that in the present article, intrapreneurship is understood in its broad definition, corresponding to entrepreneurship within an existing organization (not only for the creation of new ventures) and corresponding to the process by which organizations renew themselves, and referring to processes related to innovative activities and orientations going on inside an existing firm (regardless of its size) [8,10]. Thus, (such as in sustainable entrepreneurship), also at the intrapreneurial level, the strategic objectives of achieving positive economic, environmental, and social results can be pursued in a dynamic that can be intertwined with corporate social responsibility (CSR) [12,13].
Intrapreneurship Concept
There are several explanatory models for intrapreneurship [10], being that the most used correspond to the explanatory theory based on the social learning theory of Bandura. According to this author, learning new behaviours is a cognitive process inserted into a social context and that occurs through observation and imitation of others and suggests that cognition, behaviour, and the external environment act reciprocally [14]. The conviction/belief that an individual has, to successfully perform the desired behaviour to produce a certain result, arrives from a process in which self-efficacy is central. It is therefore an indicator that the behaviours, cognitions, and contingencies of the environment influence each other, allowing individuals to form beliefs about their ability to perform certain tasks [10,14] Thus, self-efficacy is not only the outcome of performance, but is also the deterrent factor for further and revised performance [10,14]. As such, various articles examined the effect of self-efficacy of employees as key role in forming intrapreneurial intentions [5,10,15]. On the other hand, as social learning theory suggests that cognition, behaviour, and environment are linked in a reciprocal way [10,14], there is a research stream based on the assumption that individual-level initiatives, as well as organizational level approaches (such as corporate entrepreneurship (CE)), are necessary to enable intrapreneurial behaviour [10]. It has been pointed out that intrapreneurship and CE are highly related terms, but they are not the same. Both concern entrepreneurship within an organisation; however, while CE can be seen as a top-down process (advantage-seeking at the strategic level), intrapreneurship can be seen as a bottom-up approach—it differs from the first because it focuses attention on individual employees’ intrapreneurial behaviours or initiatives that facilitates/contribute to organizations’ innovation and/or renewal [10]. As stated by Blanka [10] “the intrapreneurship concept is based on the idea that valuable human capital resides in entrepreneurial employees within existing organizations”. Thus, organizational empowerment is a key factor for human capital empowerment due to its direct effect on self-empowerment [10,16,17,18]. In fact, several studies focus their attention on the importance of intrapreneurship as a fundamental competence that allows organizations to “develop and sustain internal competencies, identify and construct creative and innovative practices, and implement beneficial changes” [18], which will confer innovation, competitive advantage, and subsequent success [18,19]. On the other hand, if this organizational predisposition was already highly relevant for organizational survival in the quickly changing business world (rising resource cost, climate change, public awareness, and changing lifestyles), it became particularly relevant in the face of the global pandemic crisis caused by COVID-19, in various contexts [9,20,21,22]. Of the various contexts, the health sector stands out as the one that was at the front line of response and, consequently, under the pressures suffered to face the necessary adaptations [23]. In this complex and volatile context, health systems and their professionals need to be able to deal with the constant changes in internal and external circumstances, which goes far beyond the need for economic and/or financial survival; according to Marimuthu and Paulose [24], “it has become imperative for healthcare organizations to have a multi directional focus in terms of the services it provides for the surrounding environment, customer, employee and community”. This highlights the need for the adoption of innovative behaviours by health professionals that are essential for access to new resources and competencies, as well as for the strategic renewal of health systems as a response to the emerging challenge [23,24,25]. However, this may also constitute a heavy ideological burden, to be placed on the already overloaded health system, with exhausted professionals [23,26]. Thus, a key issue to be addressed is to clarify how to align the factors of work content and context (from an ecological perspective) for the development of sustainable intrapreneurship and wellbeing of these professionals [27]. This is not a new perspective, since several studies have addressed the influence of organizational factors on intrapreneurship in different professional contexts, e.g., the influence of formal and informal structures, as well as leadership and management styles [10,11], including the health context [23,28]. Alternatively, the model developed by Kuratko emphasizes the processes and antecedent factors, both organizational (e.g., work discretion, management support, rewards) and individual (internal locus of control, desire for autonomy), which act as precipitating factors for intrapreneurial behaviour; however, the impact of this dynamic is measured in terms of organizational performance [20]. Additionally, there is a greater tendency to focus on the process of shaping individual entrepreneurial behaviour, leaving out a whole panoply of relevant conditions in this process, such as the wellbeing of professionals [11].
Thus, the present study aims to originally contribute towards fostering the intrapreneurial mindset in a personal, humanistic, and ecological framework in healthcare setting. We start from the assumption that the intrapreneurship spirit of internal innovative performance of an organization results from its capabilities to facilitate the global empowerment of the human capital that integrates them [17,18]. More specifically, this paper focuses its attention on the relationship between organizational structures and processes (work-related content and specifically psychosocial risk factors), as well as individual wellbeing factors (distress and resilient coping) that could be relevant not only for the promotion of organizational wellbeing but also to ensure an intrapreneurship-friendly environment (through the promotion of self-efficacy). We aim to contribute with an exploratory approach that aims at a practical indication based on theory (processes and factors precipitating intrapreneurship), combining the deductive identification of clusters (with common factors between wellbeing at work, individual competencies and factors, and intrapreneurship) aiming at the development of inductive models in an aligned way, in which entrepreneurship education “fits” or can be adjusted to meet these expectations in an aligned way.
2. Materials and Methods
2.1. Study Design
The present work is part of an observational study that was conducted between April and August 2021. The aim was to characterize the work context of healthcare settings in terms of exposure to PRFs as well as to collect the levels of resilience and distress of the staff in this professional context during the COVID-19 pandemic. A quantitative methodology was used through an online questionnaire survey. This paper presents for the first-time data on the levels of distress and resilience, as well as the exposure to descriptive analysis of PRFs of health professionals in the Portuguese healthcare context. Data on the respective health impact that exposure to PRFs represents, in Portuguese healthcare settings, have already been disclosed [26].
2.2. Participants
The present study relied on the participation of 333 formal caregivers of Portuguese healthcare services. The sample was constituted based on the total target population of 88,174 health professionals working in Portugal [29]. Considering the error of 5% and the confidence level of 95% (1.96), the representative sample should be the minimal of 383 participants. Nevertheless, the percentage of the sample by group following a distribution, in general, is similar to that found in the population percentage in terms of gender, region, or public/private sector.
The present study had a sample of 33 formal caregivers of public (n = 287, 86.2%) and private (n = 46, 13.8%) healthcare services. The sample comprised 252 females (75.7%) and 81 males (24.3%), aged between 22 and 67 years old (M = 43.52, SD = 10.121). Most of the participants were married or had a consensual union (62.5%) and had a bachelor’s degree or above (40.8%) (Table 1). Most of the participants had 16 to 25 years of work experience (M = 19.33, SD = 10.40) and had different roles relating to the healthcare provided, namely, Nurses (n = 211), Doctors (n = 47), Higher Technician in Diagnosis and Therapy (HTDT, n = 36), Technical Assistant (n = 19), Healthcare Assistant (n = 12), and other healthcare related professionals (n = 8). On the other hand, most participants had a permanent contractual arrangement (88.0%), a full-time work-schedule (96.7%), and a rotative work shift (which included nights, 42.6%). Regarding regional location, the sample worked in various geographical Portuguese regions, namely, the North (41.1%), Centre (44.7%), Lisbon Metropolitan Area (10.5%), Alentejo (0.6%), Algarve (0.6%), Madeira Autonomous Region (0.3%), and Açores Autonomous Region (0.6%); 1.2% of the sample worked in more than one region, and 0.3% did not provide region information. The details of the sample characteristics can be seen in Table 1.

Table 1.
Demographic and work characteristics of participants.
2.3. Instruments
In addition to the collection of demographic and work characteristics of participants, the Portuguese versions of the instruments Kessler Psychological Distress Scale (K10), Brief Resilient Coping Scale (BRCS), and Copenhagen Psychosocial Questionnaire (COPSOQ III, medium version) were employed.
The K10 [31] is a brief, highly reliable scale for assessing non-specific psychological distress. It is a 10-item scale based on the self-reporting of psychological distress symptoms during the last 30 days. Symptoms are estimated according to a 5-step Likert scale ranging from 1 to 5 (“no day”, “few days”, “some days” “most days”, “every day”). It results in a total score between 10 and 50, wherein values equal to or above the 22-point cut-off represents a risk of developing a mental disorder. Furthermore, values between 10 and 15 represent absence of or low distress, 16 to 21 means moderate distress, 22 to 29 portrays high distress, and 30 to 50 very high distress. The Portuguese version showed good internal consistency with Cronbach’s alpha (α) of 0.910.
The BRCS [32] is a brief instrument used to access the capacity to deal with stress in an adaptive way (resilience capacity). Is a one-dimensional scale consisting of four self-report items whose answer is given in five levels in a Likert format ranging between 1 and 5 (almost never, occasionally, often, very often, almost always). The magnitude of the results varies between 4 and 20, with those values below 13 being indicative of low resilience, and scores above 17 corresponding to strong resilience. The original scale had an internal consistency of 0.68, and in the Portuguese version it presents as α = 0.53. In the present work it was verified as α = 0.77.
The COPSOQ is a highly reliable scale for assessing breadth PRFs that are potential generators of stress at work by applying a multidimensional approach with a very broad spectrum of aspects checked [33,34,35,36], including individual factors/personality (as self-efficacy). An updated COPSOQ was released in 2019, the COPSOQ III [35], whose middle version has a Portuguese preliminary validation [37]. This revised instrument is composed of 85 items distributed in 31 PRFs, grouped into 7 main dimensions. The present work considered (1) self-efficacy, which corresponds to the personality dimension, as well as PRFs related to work content or context; (2) quantitative demands, work pace, cognitive demands, and emotional demands, which are grouped into the dimension of demands at work; (3) influence on work, development possibilities, control over working time, and meaning of work, which are grouped in the work organization and content dimension; (4) commitment to workplace, job insecurity, insecurity over working conditions, quality of work, work–life conflict, and job satisfaction, which are grouped in the dimension of work–individual interface; (5) predictability, recognition, role clarity, role conflicts, quality of leadership, social support from colleagues, social support from supervisors, and sense of community at work, which are grouped in the dimension of interpersonal relations and leadership; and (6) horizontal trust, vertical trust, and organizational justice, which are grouped in the dimension of social capital. The Portuguese COPSOQ III (middle version) shows good internal consistency. In the present study, it also showed good internal consistency with a range between α = 0.665 and α = 0.939 for the subscales.
2.4. Procedures
To recruit participants, the research protocol was disseminated by email through the communication services of the target entities (healthcare services), and it was also disseminated through social networks. Participants were invited to complete the online questionnaires on a voluntary, anonymous, and confidential basis, adopting a natural random selection of the sample. Several dissemination reinforcements were made in an attempt to obtain sample representativeness based on target population data and proportional criteria.
All data collection, registration, and communication procedures were in accordance with the guidelines of the National Commission for Data Protection and the General Data Protection Regulation. This implied the observance of prior informed consent, given voluntarily and in an informed manner, based on adequate and sufficient information, namely, the objective, purpose, and procedures in data processing. All information was treated with the highest degree of confidentiality. The present work also considered the Code of Responsible Conduct in Scientific Research, subscribing to the principles, rules, and procedures of the European Code of Conduct for Scientific Integrity, namely, reliability, honesty, respect, and accountability [38].
2.5. Data Analysis
All analyses were done using IBM SPSS Statistics® (version 26). At an early stage, in addition to descriptive statistics and internal consistency of the scales, Pearson’s correlation analyses were conducted to assess the relation between self-efficacy and distress, and resiliency and the PRFs. Next, given the interest in defining which dimensions best predicted self-efficacy, stepwise multiple regressions were employed.
3. Results
3.1. Individual Factors (Self-Efficacy, Distress, and Resilient Coping)
Considering the results of self-efficacy, the results ranged from a minimum of 1.5 to a maximum of 5 (M = 3.55, SD = 0.61) (Figure 1).

Figure 1.
Self-efficacy measured with COPSOQ.
Considering the results of distress (K10), the sum values of total responders was mostly above of the 22-point cut-off (M = 24.07; SD = 9.49). It should be noted that according to the level of distress outcomes of the total responders, 53.76% of participants presented significant psychological distress symptoms (Figure 2).
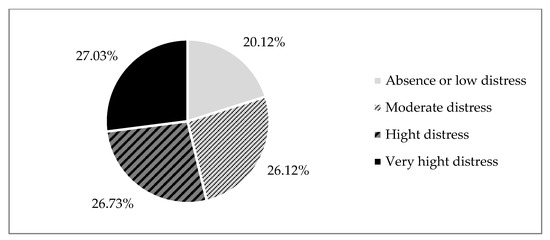
Figure 2.
Distress levels, measured with K10.
Considering the results of resilient coping (BCRS), the sum values of total responders was within range of the 13–17 cut-off points (M = 14.01, SD = 2.83), corresponding to moderate resilient coping capacity. The results showed some differences in the percentage according to the level of resilient coping capacity outcomes of the total responders, namely, 41.7% scored low in resilient coping capacity, 42.62% scored moderate in resilient coping capacity, and 15.626% scored strong in resilient coping capacity (Figure 3).
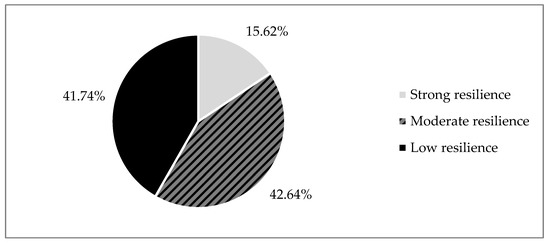
Figure 3.
Resilient coping levels, measured with BRCS.
3.2. Organizational Factors (PRFs)
Considering PRF results (COPSOQ), in the interpretation of the average results by factor and dimension (Figure 4), it should be noted that the highest values were found in the dimension of demands at work (emotional, cognitive, and quantitative demands, as well as work pace).

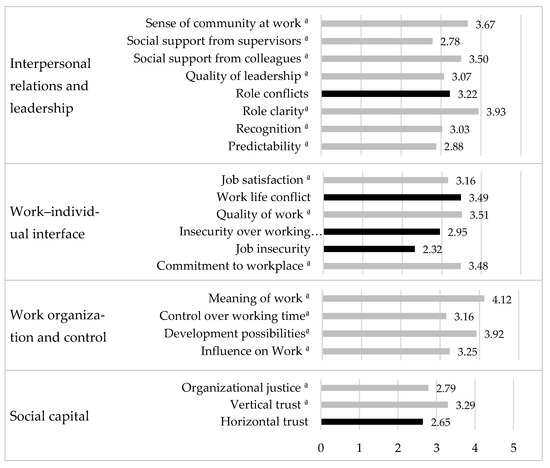
Figure 4.
Present study COPSOQ means. a. Positive subscales, high values represent low risk (represented by grey).
3.3. Organizational Factors (PRFs)
Positive and negative significant correlations were found between self-efficacy and distress (r = −0.440, ρ ≤ 0.001), resilient coping capacity (r = 0.461, ρ ≤ 0.001), as well as PRFs; positive correlations found between self-efficacy and role clarity (r = 0.327, ρ ≤ 0.001) and job satisfaction (r = 0.321, ρ ≤ 0.001) stood out as the highest. On the other hand, negative correlations were found between self-efficacy and control over working time ª (r = −0.208, ρ ≤ 0.001) and job insecurity (r = −0.180, ρ ≤ 0.001). In the PRFs of quantitative demands, cognitive demands, and emotional demands, no significant correlations were found.
Stepwise multiple regressions were employed to test if distress, resilient coping, and PRFs predicted participants’ ratings of distress and state-trait anxiety. The analysis resulted in a statistically significant model, indicating that five predictors explained 36.4% of the variance (F (5, 327) = 37.360, p < 0.001, R2 = 0.364). Specifically, distress, resilient coping, role clarity, control over working time, and job insecurity predicted self-efficacy levels (Table 2).
Table 2.
Predictive models for self-efficacy considering organizational factors (PRFs) and individual factors (distress and resilient coping).
4. Discussion
In the present work we start from the assumption that the intrapreneurship spirit of internal innovative performance of an organization results from its capabilities to facilitate the global empowerment of human capital [17,18]. Here we adapt the Kuratko model, placing particular emphasis on the antecedent factors and processes, both organizational and individual, that act as precipitating factors for intrapreneurship behaviour [11], However, the impact of this dynamic is measured in terms of self-efficacy and organizational wellbeing together. We focused our attention on the relationship between the work environment (through PRFs) and individual factors (distress and resilient coping) in the work context of health professionals, trying to find clusters of predisposing factors for self-efficacy as essential factors to ensure an environment friendly to intrapreneurship and wellbeing.
Through stepwise multiple regressions, considering the individual factors, it was verified that perceived resilience levels can act as predictors for self-efficacy, while perceived distress presents a significant inverse relationship. Regarding PRFs, role clarity, control over working time, and job insecurity are highlighted as factors that predict self-efficacy levels. Thus, it is possible to identify, in addition to resilience, two organizational dimensions that act as a positive predictor of self-efficacy (and as such ensure an intrapreneurship-friendly environment). In turn, the levels of exposure to distress and job insecurity act in reverse and may act as an impairment of this dynamic (Figure 5).
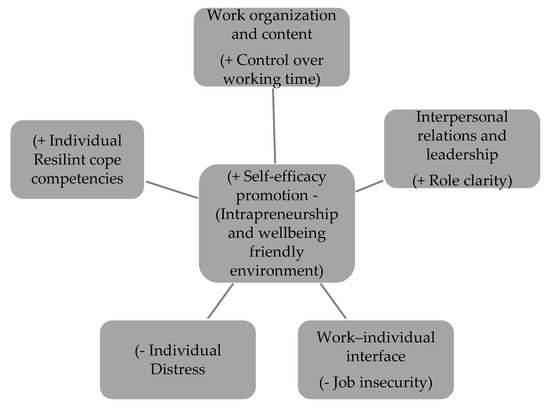
Figure 5.
Model of predisposing factors for self-efficacy as essential factors to ensure an environment friendly to intrapreneurship and wellbeing.
The results of this study build linkages between individual and organizational factors, central to promoting an environment that is friendly to wellbeing and intrapreneurship, by providing insights into how these relate to self-efficacy (as a central factor to intrapreneurship). Although it is difficult to establish definitive measures of success, we have started to extract some key considerations that can be used to guide the establishment and maintenance of an intrapreneurship- and wellbeing-friendly environment in the context of health professionals. These include strategy and leadership that see innovation as an organizational priority, establishing organizational cultures and structures that facilitate a healthy environment in terms of exposure and distress and fostering resilience, as well as work organization and content of greater self-control (particularly in working time), interpersonal relations, and leadership that promote greater clarity of roles (clarity), as well as promoting an individual work climate with the work–individual interface (job insecurity). As a whole, the proposed model answers the research question concerning the essential individual and organizational predictors of intrapreneurship, specifically how these factors can be incorporated into an organizational competency model in healthcare settings. It reflects the need for healthcare systems to support, shape, and manage intrapreneurship across ecosystem boundaries, combining multiple inbound factors within diverse and dynamic processes [10,11,39]. For practitioners, the following implications support the implementation, development, and management of intrapreneurship within the organizations. In the healthcare context, this is a relevant issue, particularly in the complex and volatile context of the global pandemic crisis caused by COVID-19. Healthcare professionals are at the frontline of the response to the changes required, and the adoption of innovative behaviours is essential for access to new resources and competencies, as well as for the strategic renewal of health systems, as a response to the emerging challenge [20].
On the other hand, as already mentioned, with regard to the particular health context, the focus on the process of modelling individual entrepreneurial behaviour (which is owing to other domains and organizational dynamics) may also constitute a heavy burden to put on these already-overloaded professionals [23,26]. Based on the results found, it is verified that there is a clear need to consider different types of organizational support structures in the sense of promoting both intrapreneurship- and wellbeing-friendly environments, including the establishment of hybrid approaches [11]. As such, the present study also aimed to develop inductive models in an aligned manner in which entrepreneurship education “fits”, or can be adjusted to meet strategies that organizations can adopt in fostering entrepreneurship as a mindset.
Kakouris [22] emphasizes entrepreneurship education in experimental and experiential perspectives. Furthermore, fostering entrepreneurship as a mindset can be thought of as a competency-based type of education, instructionally based on experiential learning [40]. Based on this construct, we present an entrepreneurial mindset development strategy through the implementation of “cause-related marketing”. We recognize that cause-related marketing has been a tool widely used for its impact on improving the organization’s image that enhances financial performance [41]. However, we stress that encouraging employees to engage and practical implementation of cause-related programs and projects in order to achieve a common positive impact can also be an innovative experiential basis of entrepreneurship pedagogy through practical learning. Practitioners learn through reflection and reframing in the context of organizational learning with critical reflection in practical learning, a strategy that has already been widely studied [27]. This can be central to experimentation and creative flexibility, designing environments that facilitate networking and relationship building that allow greater autonomy, greater clarity of roles, and more security in relation to the work. [10,11]. Additionally, a continuous learning environment may allow for development, internalization of feelings of autonomy, control, and success, and consequently on increased levels of employee self-efficacy [15], as well as result in learner empowerment and learner-driven change [40]. The creation of an environment that provides empowerment is an important organizational strategy that leads to positive workplaces, contributing to a healthy, productive, and innovative workforce with increased job satisfaction and retention [17,42] The building of an innovative organization also impacts the organization strategic value [18], being perfectly integrated into the CSR (as an investment in human capital, health, safety, and change management) [43]. It should be noted that CSR is understood as a shared responsibility that, starting from organizations, involves all stakeholders and society itself in general [13,44]. CRS is characterized in terms of its functionality by two perspectives, external and internal. While the first focuses on actions that include all stakeholders (from local communities to suppliers and consumers and relationships between them), the internal perspective is linked to employee-related issues through investment in human capital with key issues such as personnel policies, training, and health, and safety at work [43,45]. CSR can take several approaches, and cause-related marketing is also inherent to it [41]. It can be an interesting approach to introduce specific programs within the organization that allow (1) impacts to be made in the pursuit of the common good—the health and wellbeing of individuals (such as local prevention programs); and (2) contributions to the promotion of an entrepreneurial mindset, if used as a tool that boosts creativity and innovation. As an organization-wide participatory growth strategy, in a transdisciplinary problem-solving approach, it can also enhance the transition to sustainable healthcare delivery [12,39]. Indeed, sustainable healthcare education is an emerging theme that should already be included in university curricula, since education for sustainable healthcare delivery is recognized as part of the necessary response, as well as a professional and ethical requirement [39,40]. According to Schwerdtle et al. [39], it gives to all health professionals an “opportunity to influence the environmental footprint of the health sector and to work with colleagues in other disciplines to be part of the transition to sustainable healthcare delivery”. Additionally, it should be noted that in the healthcare context, sustainability also refers to the organization’s care to employees by creating a healthier workplace [24]. In other words, it is possible for a company to use cause marketing as a tool to achieve an innovative- and wellbeing-environment, and also education and promotion of sustainable and responsible behaviour (in a lifelong learning perspective).
In summary, cause-related marketing as a pedagogical tool for entrepreneurship can be an interesting approach to introduce specific programs within the organization that allow experimentation and the necessary creative flexibility. It could also contribute to sustainable development and a more competitive economy, in line with the Europe 2020 objectives for smart, sustainable, and inclusive growth [41,43]. In this sense, it is recognized that in addition to systemic reforms in education and formal training systems, smart investments in human capital by public and private sources are also necessary in order to develop and update lifelong skills, including entrepreneurial skills [1,46].
Some limitations are inherent to this study, namely, in terms of sample size, when considering the representativeness of the target population. In addition, we highlight the auto-selection of the participants; as the survey was about the work environment (through PRFs) and individual factors (distress and resilient coping), it may attract responders who may feel more exposed at a time when these professionals are particularly vulnerable to it (changes and pressures arising from the COVID-19 pandemic). Furthermore, reflecting the reality and possible factors emerging from this phase is highly important; however, it does not consider the temporal context of changes and adaptations taking place. The present study presents cause-related marketing as an organization-wide possible approach for intrapreneurial mindset development in the healthcare context. However, this framework is based on an analytical literature review, which needs further research regarding its efficiency indicators as a widespread practice. It also requires interlinking with systems of monitoring and assessment to analyse the real impact of this strategy, in terms of sustainable development, incorporated into the core topics of CSR. For future studies, we propose focusing on a long-term investigation, preferably in the form of action-research, which may help to create a more integrated understanding of the proposed construct and underlying phenomena.
5. Conclusions
We seek to reconcile different theories to integrate the existing approaches to professional and entrepreneurship wellbeing in order to find factors that facilitate an intrapreneurship- and wellbeing-friendly environment in the healthcare work context. We start from the assumption that the promotion of self-efficacy emerges as a central element in this dynamic, which relies on individual and organizational factors simultaneously. Based on the results, it appears that the promotion of an entrepreneurship- and wellbeing-friendly environment may involve developing, facilitating, or enhancing greater resilience (at an individual level), as well as acting to reduce work-related stress factors (at an organizational level), in particular, role clarity, control over working time, and job insecurity. Still in the organizational domain, it should be recalled that these PRFs are integral factors in the organizational dimensions of interpersonal relations and leadership, organization and content and, finally, the individual–work interface. As such, the results indicate that organizational support structures in the sense of promoting an intrapreneurship- and wellbeing-friendly environment should include hybrid approaches, seeking to combine the deductively identified clusters in this exploratory approach.
For practical consideration, we present an entrepreneurial mindset development strategy through the implementation of cause-related marketing as a pedagogical tool for entrepreneurship within the organization that allows for experimentation and the necessary creative flexibility. Through environments that provide empowerment (as an organizational strategy) it is possible to achieve an innovative and wellbeing environment. This is a relevant issue in the complex and volatile context of the global pandemic crisis caused by COVID-19, particularly for health systems and their professionals that are at the frontline of the response to the changes required. The building of an innovative organization also impacts the organization strategic value, being perfectly integrated into corporate social responsibility (as an investment in human capital, health, safety, and change management) in line with the Europe 2020 objectives for smart, sustainable, and inclusive growth.
Author Contributions
A.P. and E.B. conceived the study. I.S. conducted the literature review, A.P. and E.B: methodology; I.S. data collection and formal analysis. I.S. drafted the paper, and A.P. and E.B., reviewed and edited the paper. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Funds through FCT—Fundação para a Ciência e a Tecnologia, I.P., (reference 2021.09377.BD); CIDTFF—Research Centre on Didactics and Technology in the Education of Trainers (reference UIDB/00194/2020 and UIDP/00194/2020).
Institutional Review Board Statement
All subjects gave their informed consent for inclusion before they participated in the study. All data were obtained in an anonymized form, and data are not externally accessible. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Aveiro University Ethics Committee (32-CED/2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Acknowledgments
The authors would like to thank all the employees that answered the questionnaires, and Bruno Alves, who have facilitated all the data collecting process within the healthcare settings.
Conflicts of Interest
The authors declare no conflict of interest.
References
- European Commission. A New Skills Agenda for Europe; European Commission: Brussels, Belgium, 2016.
- European Commission. Key Competences for LifeLong Learning; European Commission: Brussels, Belgium, 2018.
- Bacigalupo, M.; Kampylis, P.; Punie, Y.; Van den Brande, G. EntreComp: The Entrepreneurship Competence Framework; Publications Office of the European Union: Luxembourg, 2016. [CrossRef]
- Bianchi, G.; Pisiotis, U.; Cabrera, M.; Punie, Y.; Bacigalupo, M. The European Sustainability Competence Framework. Publ. Off. Eur. Union 2022, 51, 13286. [Google Scholar] [CrossRef]
- Douglas, E.J.; Fitzsimmons, J.R. Intrapreneurial Intentions versus Entrepreneurial Intentions: Distinct Constructs with Different Antecedents. Small Bus. Econ. 2013, 41, 115–132. [Google Scholar] [CrossRef]
- Gu, W.; Wang, J. Research on Index Construction of Sustainable Entrepreneurship and Its Impact on Economic Growth. J. Bus. Res. 2022, 142, 266–276. [Google Scholar] [CrossRef]
- Biggeri, M.; Colucci, D.; Doni, N.; Valori, V. Sustainable Entrepreneurship: Good Deeds, Business, Social and Environmental Responsibility in a Market Experiment. Sustainabiliy 2022, 14, 3577. [Google Scholar] [CrossRef]
- Miller, D. The Correlates of Entrepreneurship in Three Types of Firms. Manag. Sci. 1983, 29, 770–791. [Google Scholar] [CrossRef]
- Alpkan, L.; Bulut, C.; Gunday, G.; Ulusoy, G.; Kilic, K. Organizational Support for Intrapreneurship and Its Interaction with Human Capital to Enhance Innovative Performance. Manag. Decis. 2010, 48, 25–1747. [Google Scholar] [CrossRef]
- Blanka, C. An Individual-Level Perspective on Intrapreneurship: A Review and Ways Forward. Rev. Manag. Sci. 2019, 13, 919–961. [Google Scholar] [CrossRef]
- Gardiner, E.; Debrulle, J. Intrapreneurship and Wellbeing in Organizations. In The SAGE Handbook of Organizational Wellbeing; Wall, T., Cooper, C.L., Brough, P., Eds.; SAGE Publications Ltd.: London, UK, 2021; pp. 184–198. [Google Scholar] [CrossRef]
- Moldovan, F.; Blaga, P.; Moldovan, L.; Bataga, T. An Innovative Framework for Sustainable Development in Healthcare: The Human Rights Assessment. Int. J. Environ. Res. Public Health 2022, 19, 2222. [Google Scholar] [CrossRef]
- International Organisation for Standardization. ISO 26000:2010-Guidance on Social Responsibility. Available online: https://www.iso.org/standard/42546.html (accessed on 30 April 2022).
- Bandura, A. Self-Efficacy: Toward a Unifying Theory of Behavioral Change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Wakkee, I.; Elfring, T.; Monaghan, S. Creating Entrepreneurial Employees in Traditional Service Sectors: The Role of Coaching and Self-Efficacy. Int. Entrep. Manag. J. 2010, 6, 21. [Google Scholar] [CrossRef]
- Moghaddas, S.Z.; Tajafari, M.; Nowkarizi, M. Organizational Empowerment: A Vital Step toward Intrapreneurship. J. Librariansh. Inf. Sci. 2020, 52, 529–540. [Google Scholar] [CrossRef]
- Wagner, J.I.J.; Cummings, G.; Smith, D.L.; Olson, J.; Anderson, L.; Warren, S. The Relationship between Structural Empowerment and Psychological Empowerment for Nurses: A Systematic Review. J. Nurs. Manag. 2010, 18, 448–462. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, J.N.; Krishna, A. Bottom-Up Building of an Innovative Organization: Motivating Employee Intrapreneurship and Scouting and Their Strategic Value. Manag. Commun. Q. 2014, 28, 531–560. [Google Scholar] [CrossRef]
- Widya Hastuti, A.; Talib, N.B.A.; Wong, K.Y.; Mardani, A. The Role of Intrapreneurship for Sustainable Innovation through Process Innovation in Small and Medium-Sized Enterprises: A Conceptual Framework. Int. J. Econ. Financ. Issues 2016, 6, 83–91. [Google Scholar]
- Cherrington, M.; Airehrour, D.; Cameron-Brown, D.; Lu, J.; Xu, Q.; Stokes, A. Intrapreneurship in the Time of Covid. In Unitec Research Symposium Proceedings 2020; Papoutsaki, E., Shannon, M., Eds.; ePress, Unitec New Zealand: Auckland, New Zealand, 2021; pp. 95–107. [Google Scholar]
- Kiziloglu, M.; Ray, S. Do We Need a Second Engine for Entrepreneurship? How Well Defined Is Intrapreneurship to Handle Challenges during COVID-19? SHS Web Conf. 2021, 120, 02022. [Google Scholar] [CrossRef]
- Noordiana, N.; Yulia, R.; Iriani, S.; Witjaksono, A.D.; Wulandari, S.S.; Universitas, P.; Surabaya, N. Improvement of Intrapreneurship Behavior in Higher Education. J. Pendidik. Edutama 2022, 9, 193–212. [Google Scholar] [CrossRef]
- Ferraz, P.; Marques, C.S.; Santos, G.; Cunha, A.M.; Vaz, S. The Influence of Cognitive Styles as Promoters of Entrepreneurial Orientation and Intrapreneurship as Drivers of Innovation: The Case of Nurses in Health Services in Portugal in Times of COVID-19. Adm. Sci. 2021, 11, 107. [Google Scholar] [CrossRef]
- Marimuthu, M.; Paulose, H. Emergence of Sustainability Based Approaches in Healthcare: Expanding Research and Practice. Procedia Soc. Behav. Sci. 2016, 224, 554–561. [Google Scholar] [CrossRef]
- Marques, C.S.; Lopes, C.; Braga, V.; Ratten, V.; Santos, G. Intuition and Rationality in Intrapreneurship and Innovation Outputs: The Case of Health Professionals in Primary Health Care. Int. Entrep. Manag. J. 2022, 18, 579–602. [Google Scholar] [CrossRef]
- Pereira, A.; Brito, E.; Souto, I.; Alves, B. Healthcare Services and Formal Caregiver’s Psychosocial Risk Factors: An Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 5009. [Google Scholar] [CrossRef]
- Kakouris, A. Entrepreneurship Pedagogies in Lifelong Learning: Emergence of Criticality? Learn. Cult. Soc. Interact. 2015, 6, 87–97. [Google Scholar] [CrossRef]
- Alsop, A. Continuing Professional Development in Health and Social Care, 2nd ed.; Wiley-Blackwell Publishing Ltd: Chinchester, UK, 2013. [Google Scholar] [CrossRef]
- Instituto Nacional de Estatística [INE]. Estatísticas Da Saúde; INE: Lisboa, Portugal, 2019. [Google Scholar]
- Lei Geral Do Trabalho Em Funções Públicas—Subsecção II, Diário da República n.o 117/2014, Série II. 2014.
- Pereira, A.; Oliveira, C.A.; Bártolo, A.; Monteiro, S.; Vagos, P.; Jardim, J. Reliability and Factor Structure of the 10-Item Kessler Psychological Distress Scale (K10) among Portuguese Adults. Cienc. Saude Coletiva 2019, 24, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.L.P.; Morais, R. Adaptação Portuguesa Da Escala Breve de Coping Resiliente. Psicol. Saúde Doenças 2010, 11, 5–13. [Google Scholar]
- Silva, C.; Amaral, V.; Pereira, A.; Bem-haja, P.; Pereira, A.; Rodrigues, V.; Cotrim, T.; Silvério, J.; Nossa, P. (1). Copenhagen Psychosocial Questionnaire II: Portugal e Países Africanos de Língua Oficial Portuguesa; Departamento de Educação e Psicologia, Universidade de Aveiro: Aveiro, Portugal, 2011. [Google Scholar]
- Fernandes, C.; Pereira, A. Exposure to Psychosocial Risk Factors in the Context of Work: A Systematic Review. Rev. Saude Publ. 2016, 50, 6129. [Google Scholar] [CrossRef] [PubMed]
- Burr, H.; Berthelsen, H.; Moncada, S.; Nübling, M.; Dupret, E.; Demiral, Y.; Oudyk, J.; Kristensen, T.S.; Llorens, C.; Navarro, A.; et al. The Third Version of the Copenhagen Psychosocial Questionnaire. Saf. Health Work 2019, 10, 482–503. [Google Scholar] [CrossRef]
- Berthelsen, H.; Westerlund, H.; Bergström, G.; Burr, H. Validation of the Copenhagen Psychosocial Questionnaire Version III and Establishment of Benchmarks for Psychosocial Risk Management in Sweden. Int. J. Environ. Res. Public Health 2020, 17, 3179. [Google Scholar] [CrossRef] [PubMed]
- Cotrim, T.P.; Bem-Haja, P.; Pereira, A.; Fernandes, C.; Azevedo, R.; Antunes, S.; Pinto, J.S.; Kanazawa, F.; Souto, I.; Brito, E.; et al. The Portuguese Third Version of the Copenhagen Psychosocial Questionnaire: Preliminary Validation Studies of the Middle Version among Municipal and Healthcare Workers. Int. J. Environ. Res. Public Health 2022, 19, 1167. [Google Scholar] [CrossRef]
- All European Academies [ALLEA]. The European Code of Conduct for Research Integrity, Revised ed.; ALLEA-All European Academies: Berlin, Germany, 2017. [Google Scholar]
- Schwerdtle, N.; Horton, G.; Kent, F.; Walker, L.; McLean, M. Education for Sustainable Healthcare: A Transdisciplinary Approach to Transversal Environmental Threats. Med. Teach. 2020, 42, 1102–1106. [Google Scholar] [CrossRef]
- Huss, N.; Ikiugu, M.N.; Hackett, F.; Sheffield, P.E.; Palipane, N.; Groome, J. Education for Sustainable Health Care: From Learning to Professional Practice. Med. Teach. 2020, 42, 1097–1101. [Google Scholar] [CrossRef]
- Brønn, P.S.; Vrioni, A.B. Corporate Social Responsibility and Cause-Related Marketing: An Overview. Int. J. Advert. 2015, 20, 207–222. [Google Scholar] [CrossRef]
- Zhou, H.; Chen, J. How Does Psychological Empowerment Prevent Emotional Exhaustion? Psychological Safety and Organizational Embeddedness as Mediators. Front. Psychol. 2021, 12, 2945. [Google Scholar] [CrossRef] [PubMed]
- European Commission. A Renewed EU Strategy 2011-14 for Corporate Social Responsibility; European Commission: Brussels, Belgium, 2011.
- Latapí Agudelo, M.A.; Jóhannsdóttir, L.; Davídsdóttir, B. A Literature Review of the History and Evolution of Corporate Social Responsibility. Int. J. Corp. Soc. Responsib. 2019, 4, 23. [Google Scholar] [CrossRef]
- Koskela, M. Occupational Health and Safety in Corporate Social Responsibility Reports. Saf. Sci. 2014, 68, 294–308. [Google Scholar] [CrossRef]
- European Commission. The European Pillar of Social Rights. ERA Forum 2017, 18, 149–153. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).