
Analysis of Spatial and Driving Factors of National Sanitary Resources in China Using GIS

Abstract
1. Introduction
2. Theoretical Derivation and Significance of NSCC Policy
2.1. Original NSCC Policy
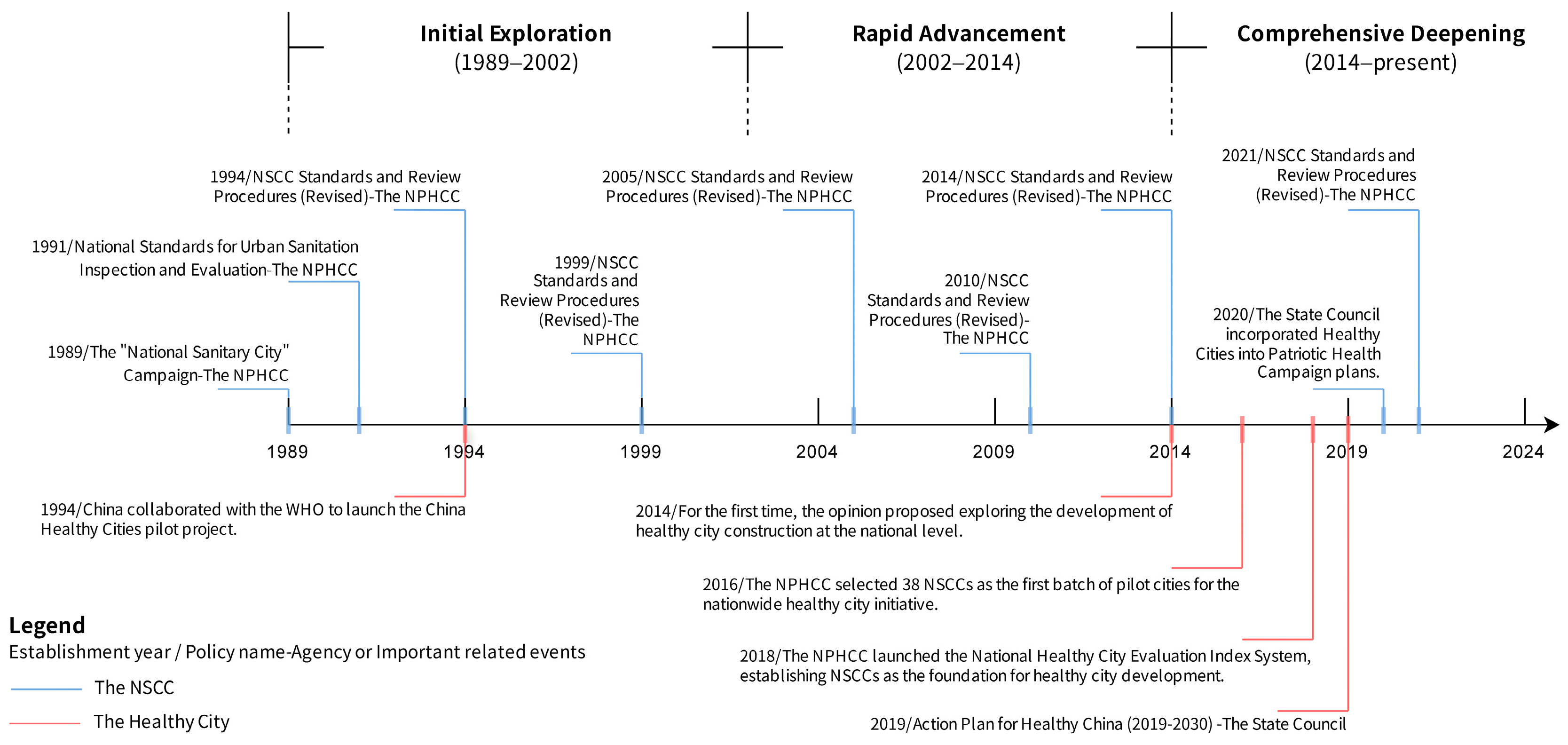
2.2. Evolution Process of NSCC Policy
2.3. Evolution of Selection Criteria and Mechanisms of NSCCs
2.4. Significance and Benefits
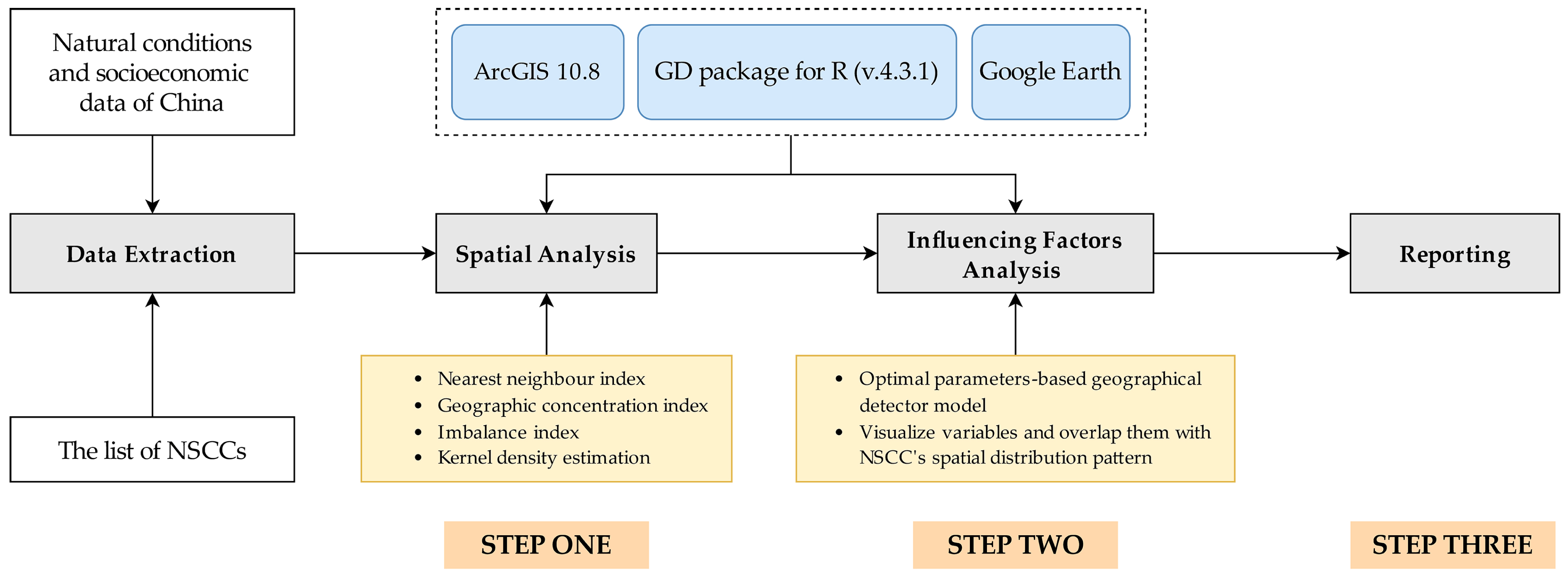
3. Data Sources and Research Methodology
3.1. Data Sources
3.2. Research Methodology
3.2.1. Nearest Neighbour Index
3.2.2. Geographic Concentration Index
3.2.3. Imbalance Index
3.2.4. Kernel Density Estimation
3.2.5. Optimal Parameter-Based Geographical Detector Model
4. Results
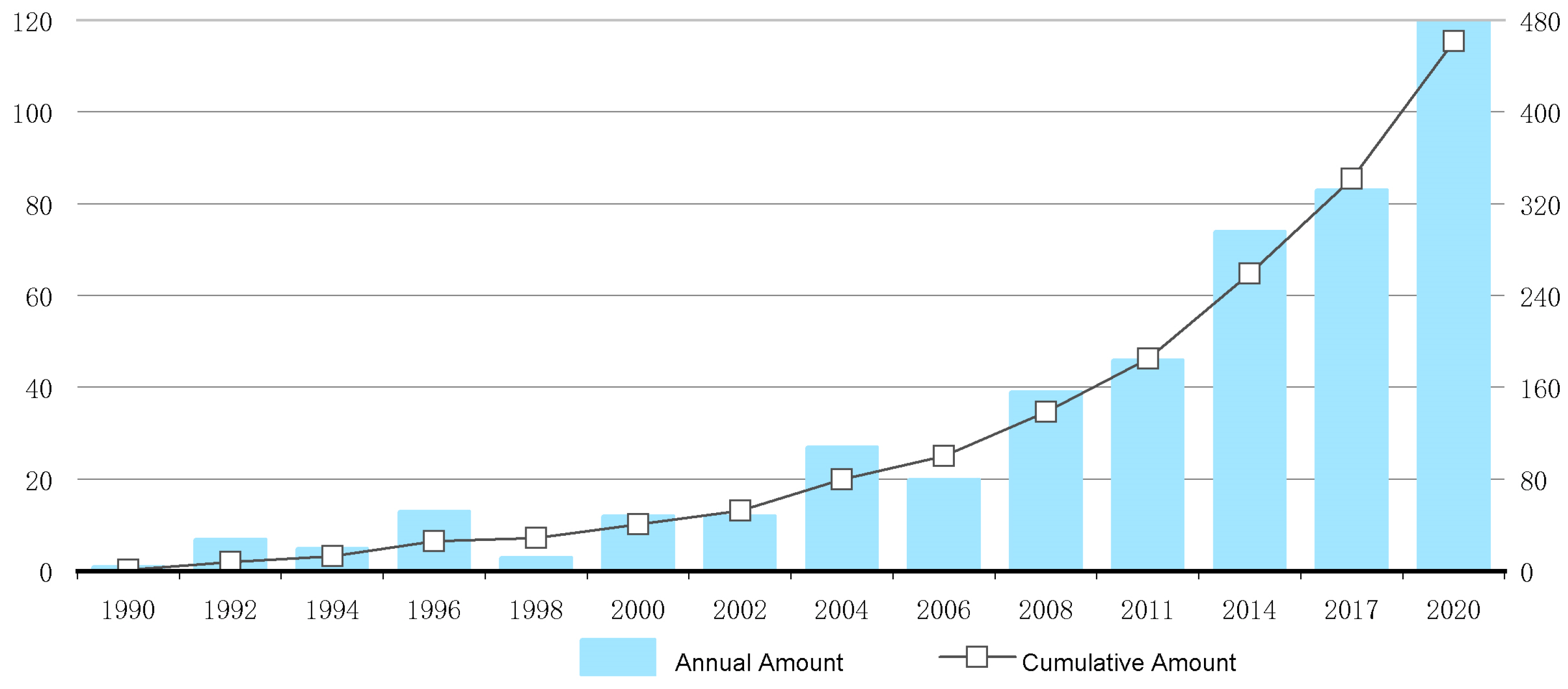
4.1. Overview of the Study Subject
4.2. Spatial Characteristics and Structural Analysis
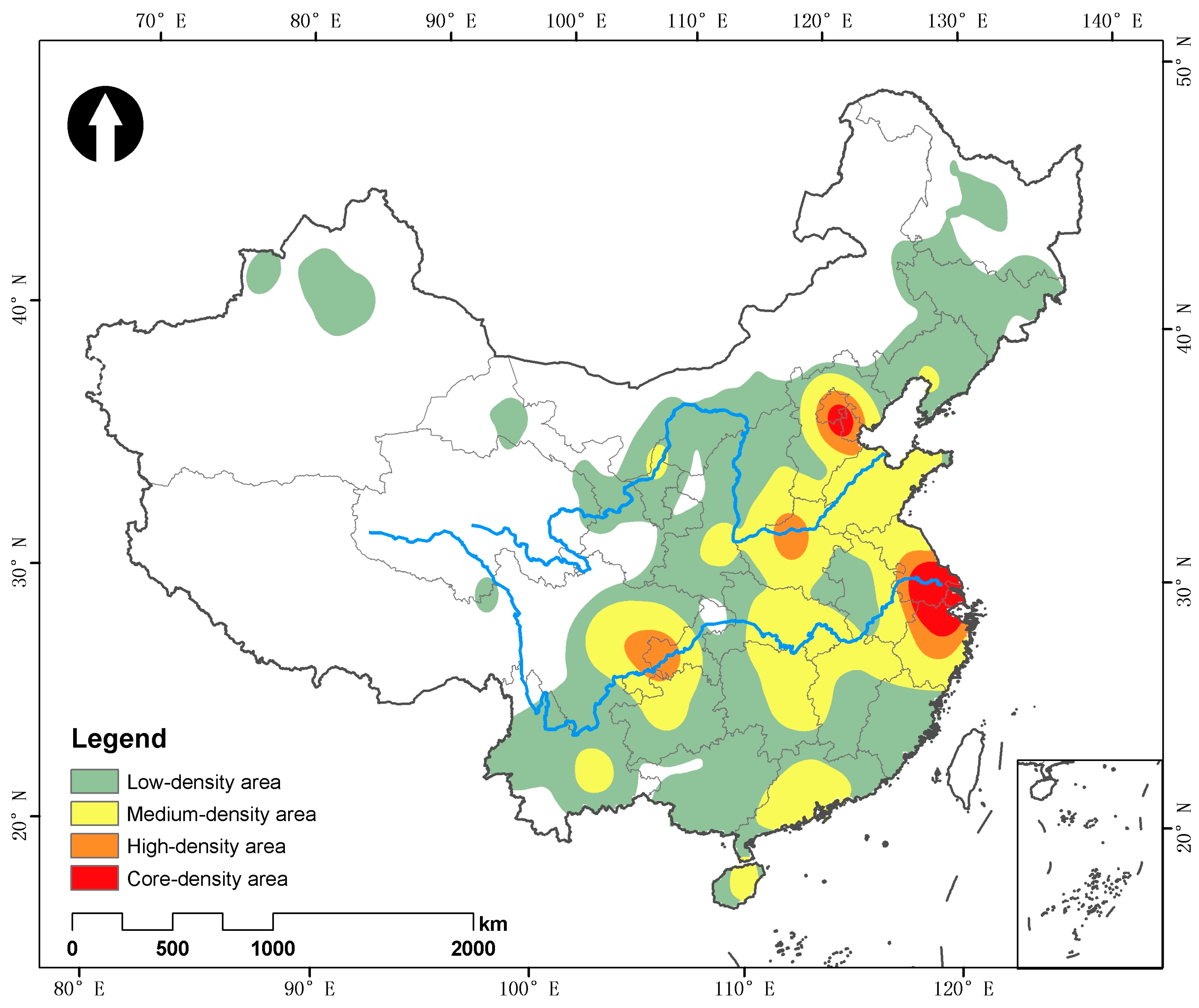
4.2.1. Spatial Distribution Pattern
4.2.2. Balanced Spatial Distribution
- 1.
- Concentration analysis of spatial distribution
- 2.
- Equilibrium analysis of spatial distribution
4.2.3. Spatial Distribution Density Characteristics
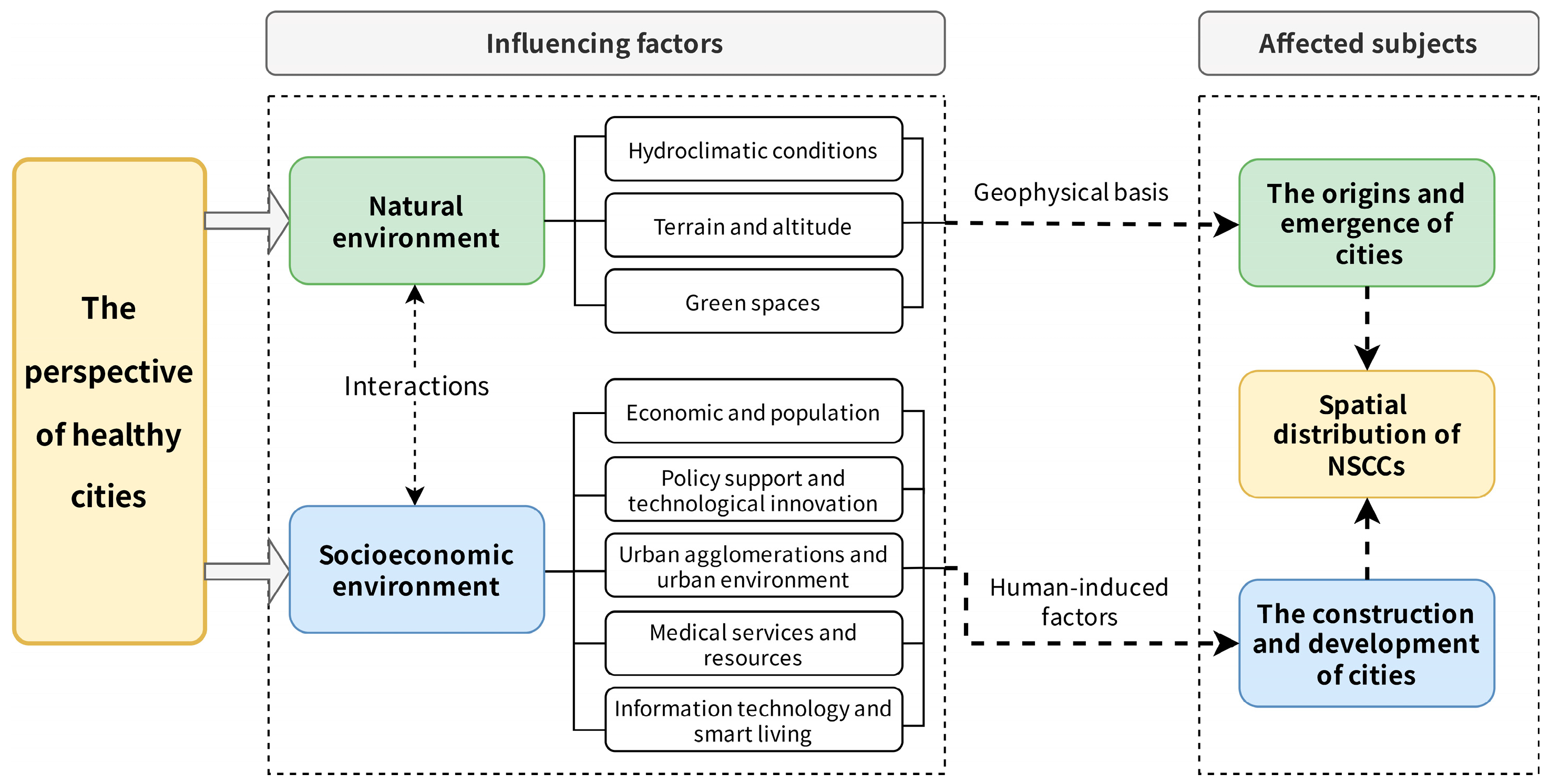
5. Driving and Influencing Factors of the Spatial Distribution of NSCCs
5.1. Natural Environmental Factors
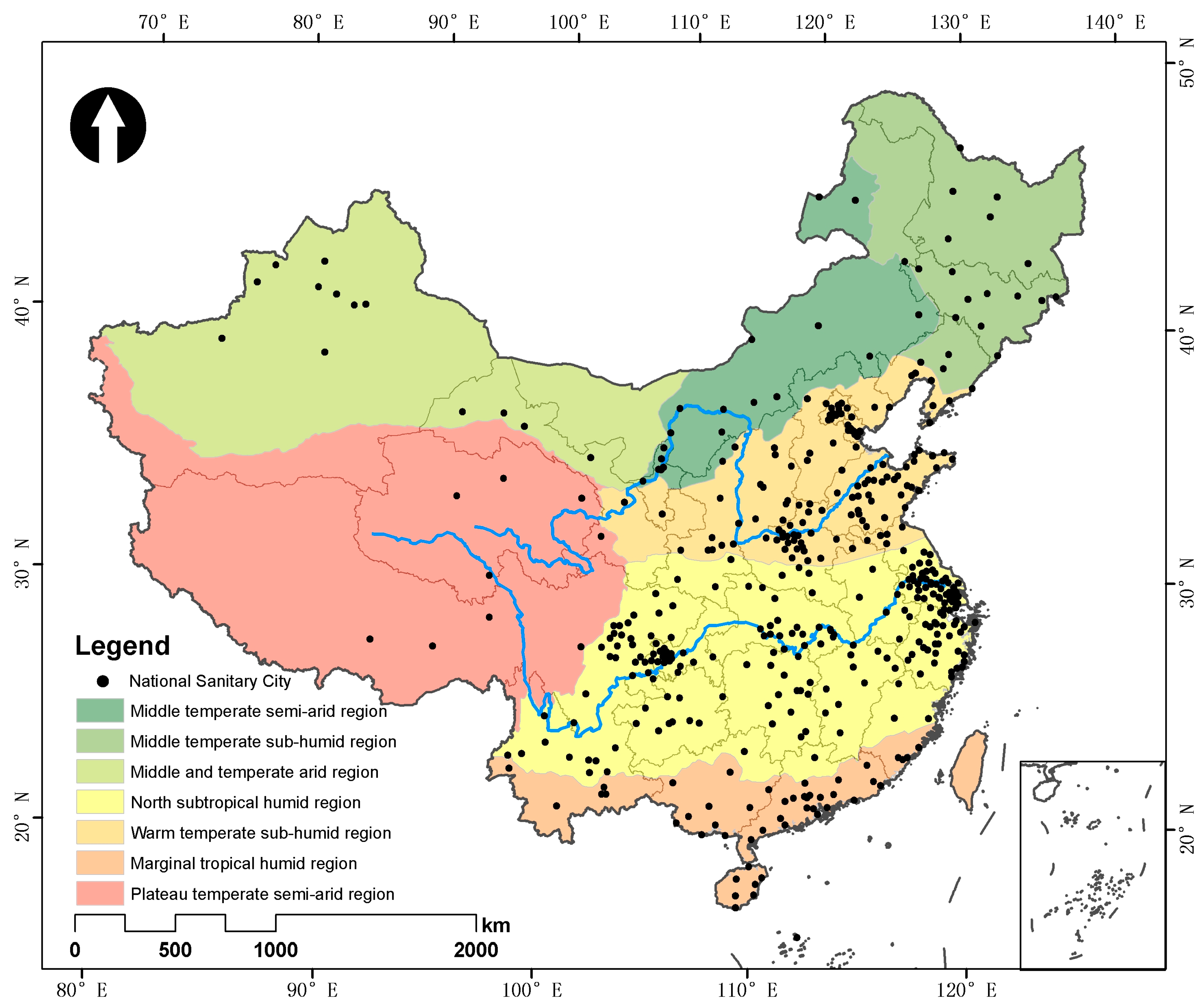
5.1.1. Hydroclimatic Conditions
5.1.2. Terrain and Altitude
5.1.3. Urban Green Spaces
5.2. Socioeconomic Factors
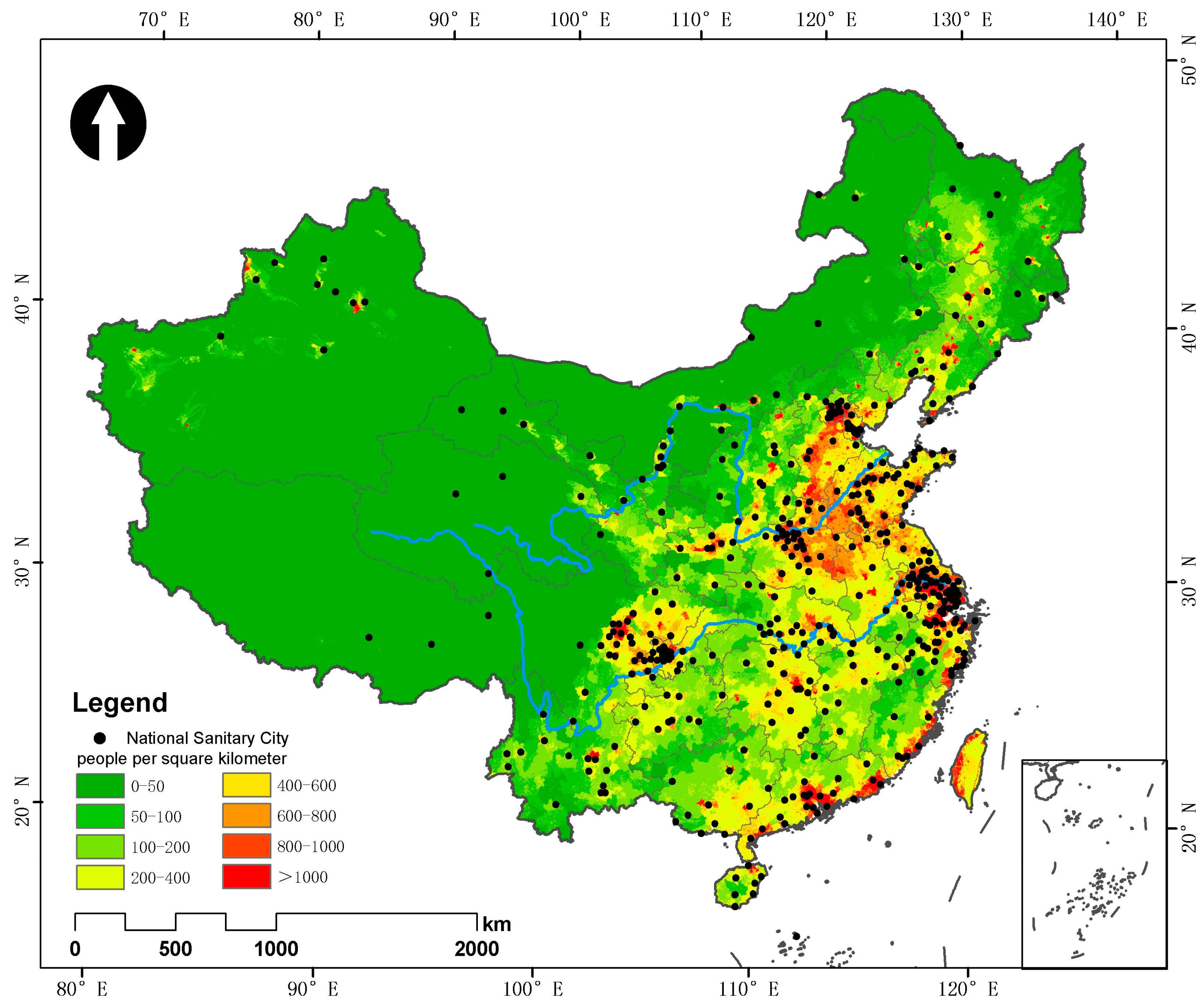
5.2.1. Economic and Population
5.2.2. Policy Support and Technological Innovation
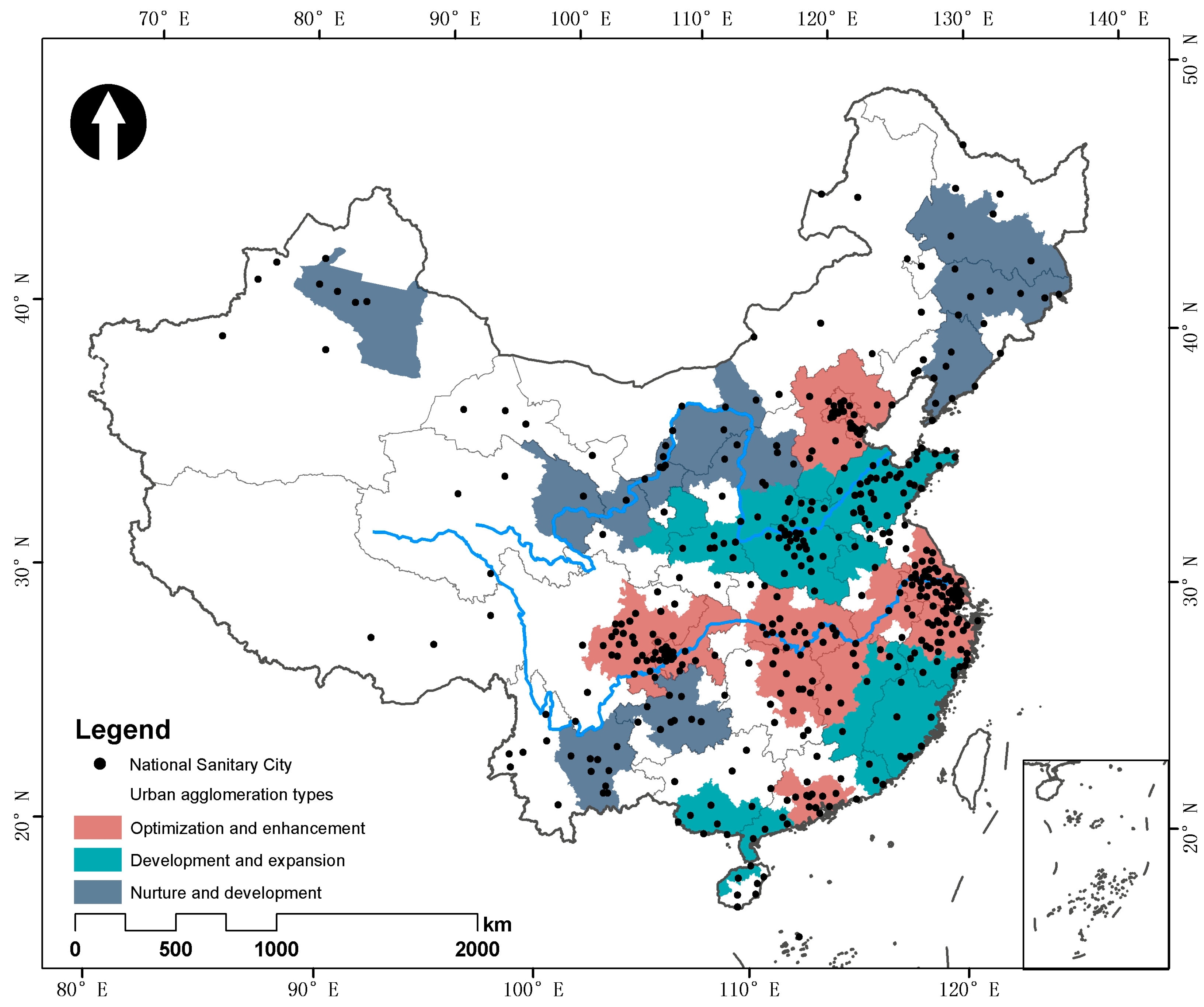
5.2.3. Urban Agglomerations and Urban Environment
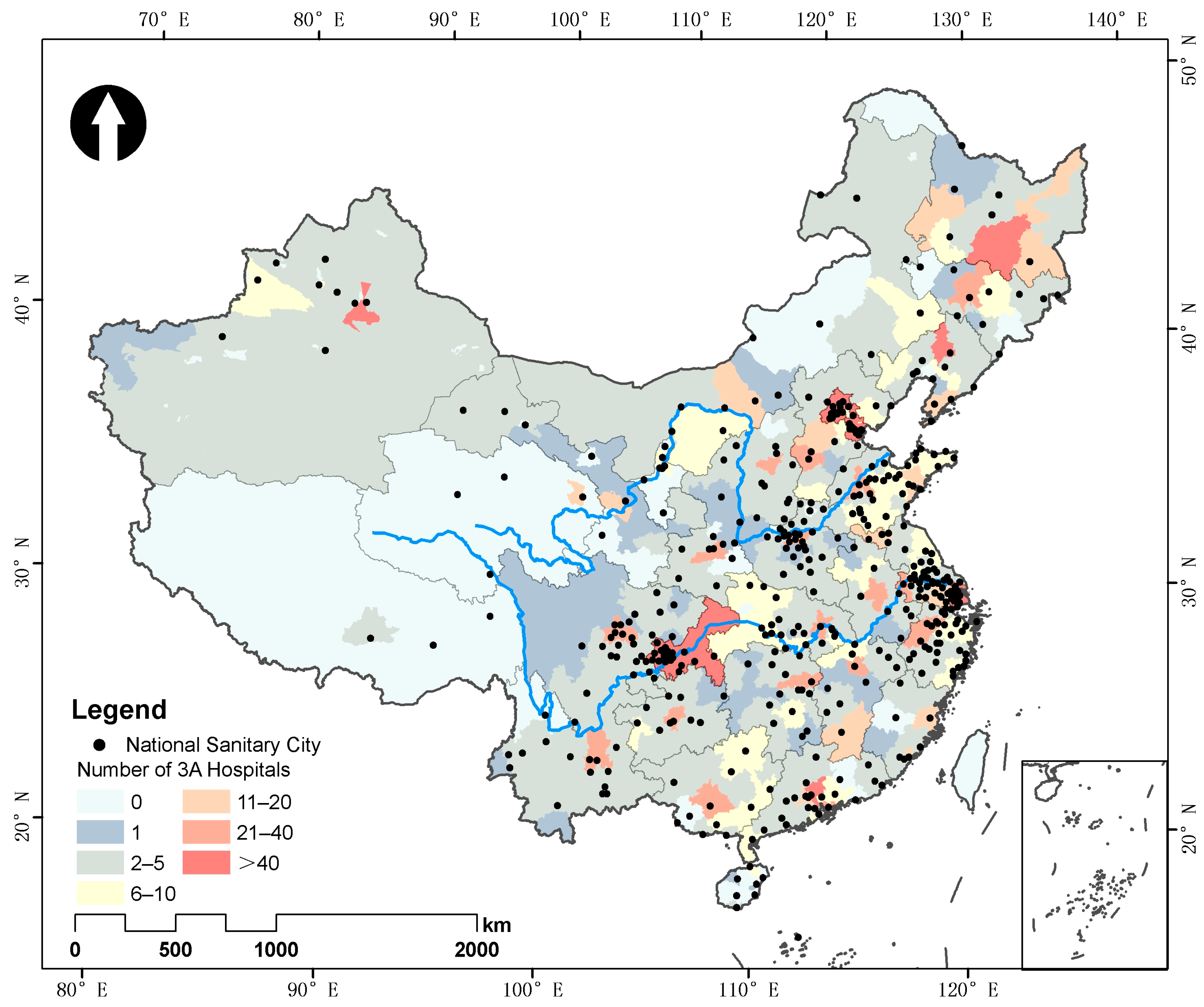
5.2.4. Medical Services and Resources
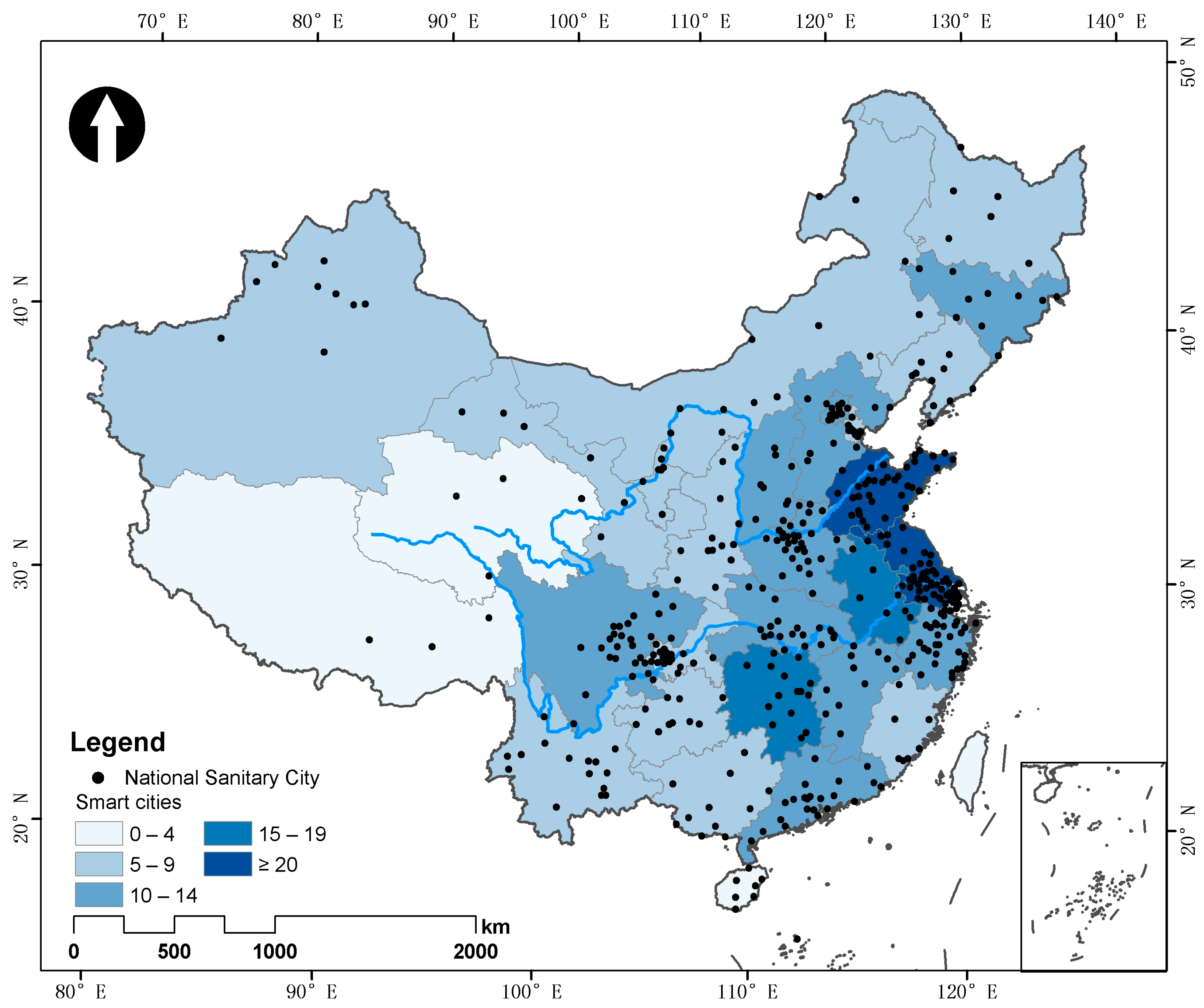
5.2.5. Information Technology and Smart Living
6. Discussion
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kundu, D.; Pandey, A.K. World Urbanisation: Trends and Patterns. In Developing National Urban Policies: Ways Forward to Green and Smart Cities; Kundu, D., Sietchiping, R., Kinyanjui, M., Eds.; Springer Nature: Singapore, 2020; pp. 13–49. ISBN 978-981-15-3738-7. [Google Scholar]
- Singh, N.; Singh, S.; Mall, R.K. Chapter 17–Urban Ecology and Human Health: Implications of Urban Heat Island, Air Pollution and Climate Change Nexus. In Urban Ecology; Verma, P., Singh, P., Singh, R., Raghubanshi, A.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 317–334. ISBN 978-0-12-820730-7. [Google Scholar]
- Chaudhry, D. Climate Change and Health of the Urban Poor: The Role of Environmental Justice. J. Clim. Change Health 2024, 15, 100277. [Google Scholar] [CrossRef]
- Mouratidis, K. Urban Planning and Quality of Life: A Review of Pathways Linking the Built Environment to Subjective Well-Being. Cities 2021, 115, 103229. [Google Scholar] [CrossRef]
- McGreevy, M.; Harris, P.; Delaney-Crowe, T.; Fisher, M.; Sainsbury, P.; Riley, E.; Baum, F. How Well Do Australian Government Urban Planning Policies Respond to the Social Determinants of Health and Health Equity? Land Use Policy 2020, 99, 105053. [Google Scholar] [CrossRef]
- Li, X.; Song, J.; Lin, T.; Dixon, J.; Zhang, G.; Ye, H. Urbanization and Health in China, Thinking at the National, Local and Individual Levels. Environ. Health 2016, 15, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Du, P.; Sun, B.; Pan, L.J.; Cheng, Y.B.; Li, T.T.; Wang, X.L.; Shi, L.W.; Yao, X.Y.; Shi, X.M. Achievements and Prospects on Environmental Health and Sanitary Engineering in China. Zhonghua Yu Fang Yi Xue Za Zhi Chin. J. Prev. Med. 2019, 53, 865–870. [Google Scholar] [CrossRef]
- Li, Y.; Yang, H. The Incentive Effect of Creating a National Health City on the Ecological Welfare Performance: Based on the Evidence of Yangtze River Delta in China. Environ. Sci. Pollut. Res. 2023, 30, 83735–83759. [Google Scholar] [CrossRef]
- Yin, S.; Chen, W.Y.; Liu, C. Urban Forests as a Strategy for Transforming towards Healthy Cities. Urban. For. Urban. Green. 2023, 81, 127871. [Google Scholar] [CrossRef]
- Palutturi, S.; Saleh, L.M.; Rachmat, M.; Malek, J.A.; Nam, E.W. Principles and Strategies for Aisles Communities Empowerment in Creating Makassar Healthy City, Indonesia. Gac. Sanit. 2021, 35, S46–S48. [Google Scholar] [CrossRef]
- Bafarasat, A.; Cheshmehzangi, A.; Ankowska, A. A Set of 99 Healthy City Indicators for Application in Urban Planning and Design. Sustain. Dev. 2023, 31, 1978–1989. [Google Scholar] [CrossRef]
- Zhao, M.; Qin, W.; Zhang, S.; Qi, F.; Li, X.; Lan, X. Assessing the Construction of a Healthy City in China: A Conceptual Framework and Evaluation Index System. Public Health 2023, 220, 88–95. [Google Scholar] [CrossRef]
- Ali, M.; Rahaman, M.; Hossain, S. Urban Green Spaces for Elderly Human Health: A Planning Model for Healthy City Living. Land Use Policy 2022, 114, 105970. [Google Scholar] [CrossRef]
- Capolongo, S.; Rebecchi, A.; Dettori, M.; Appolloni, L.; Azara, A.; Buffoli, M.; Capasso, L.; Casuccio, A.; Conti, G.; D’Amico, A.; et al. Healthy Design and Urban Planning Strategies, Actions, and Policy to Achieve Salutogenic Cities. Int. J. Environ. Res. Public Health 2018, 15, 2698. [Google Scholar] [CrossRef]
- Xie, Y.; Meng, X.; Cenci, J.; Zhang, J. Spatial Pattern and Formation Mechanism of Rural Tourism Resources in China: Evidence from 1470 National Leisure Villages. ISPRS Int. J. Geo-Inf. 2022, 11, 455. [Google Scholar] [CrossRef]
- Zhang, Z.; Cenci, J.; Zhang, J. Policies for Equity in Access to Urban Green Space: A Spatial Perspective of the Chinese National Forest City Policy. Forests 2024, 15, 608. [Google Scholar] [CrossRef]
- Tao, W.; Zeng, Z.; Dang, H.; Li, P.; Chuong, L.; Yue, D.; Wen, J.; Zhao, R.; Li, W.; Kominski, G. Towards Universal Health Coverage: Achievements and Challenges of 10 Years of Healthcare Reform in China. BMJ Glob. Health 2020, 5, e002087. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lin, Z.; Li, L.; Li, J.; Wang, Y.; Pan, Y.; Yang, J.; Xu, C.; Zeng, X.; Xie, X.; et al. Ten Years of China’s New Healthcare Reform: A Longitudinal Study on Changes in Health Resources. BMC Public Health 2021, 21, 2272. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Dai, J.; Gao, J.; Jia, Y.; Zheng, P. Healthy City Construction in China: Accomplishments and Prospects. Chin. J. Public Health 2019, 35, 1285–1288. [Google Scholar] [CrossRef]
- Liu, S.R.; Wang, H.; Xi, T.Y. Administrative Bidding, Performance, and Political Incentives——Evidence from National Health Cities. J. Public Manag. 2020, 17, 10–20. [Google Scholar] [CrossRef]
- Bai, Y.; Zhang, Y.; Zotova, O.; Pineo, H.; Siri, J.; Liang, L.; Luo, X.; Kwan, M.-P.; Ji, J.; Jiang, X.; et al. Healthy Cities Initiative in China: Progress, Challenges, and the Way Forward. Lancet Reg. Health West. Pac. 2022, 27, 100539. [Google Scholar] [CrossRef]
- Announcement of the 2021 National Sanitary City and Town Reassessment Results by the National Patriotic Health Campaign Committee. Available online: http://www.nhc.gov.cn/guihuaxxs/gongwen1/202202/253a2c03dbee4cf9a952238236fda163.shtml (accessed on 7 August 2024).
- Zheng, W.; Yao, H.; Yu, S.; Liu, J.; Hu, Y.; Wang, J. Residents’ Sense of Acquisition and Influencing Factors in China’s Sanitary City Initiative. Chin. J. Epidemiol. 2023, 44, 457–462. [Google Scholar] [CrossRef]
- Wang, Y.; Pei, R.; Gu, X.; Liu, B.; Liu, L. Has the Healthy City Pilot Policy Improved Urban Health Development Performance in China? Evidence from a Quasi-Natural Experiment. Sustain. Cities Soc. 2023, 88, 104268. [Google Scholar] [CrossRef]
- Tang, G.; Lin, M.; Xu, Y.; Li, J.; Chen, L. Impact of Rating and Praise Campaigns on Local Government Environmental Governance Efficiency: Evidence from the Campaign of Establishment of National Sanitary Cities in China. PLoS ONE 2021, 16, e0253703. [Google Scholar] [CrossRef]
- Yue, D.; Ruan, S.; Xu, J.; Zhu, W.; Zhang, L.; Cheng, G.; Meng, Q. Impact of the China Healthy Cities Initiative on Urban Environment. J. Urban Health 2017, 94, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.; Zhang, C.; Shen, R.; Li, B. Can the Establishment of National Sanitary Cities Better Resist the Impact of COVID-19? Front. Public Health 2023, 11, 1041355. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, Morbidity, and Risk Factors in China and Its Provinces, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 394, 1145–1158. [Google Scholar] [CrossRef] [PubMed]
- Barber, R.M.; Fullman, N.; Sorensen, R.J.D.; Bollyky, T.; McKee, M.; Nolte, E.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; et al. Healthcare Access and Quality Index Based on Mortality from Causes Amenable to Personal Health Care in 195 Countries and Territories, 1990–2015: A Novel Analysis from the Global Burden of Disease Study 2015. Lancet 2017, 390, 231–266. [Google Scholar] [CrossRef]
- The 2023 Statistical Bulletin on the Development of China’s Health Sector. Available online: https://www.gov.cn/lianbo/bumen/202408/content_6971241.htm (accessed on 4 September 2024).
- Yang, G. What Is Historical Political Science? Chin. Political Sci. Rev. 2022, 7, 1–28. [Google Scholar] [CrossRef]
- Feng, D.; Bao, W.; Yang, Y.; Fu, M. How Do Government Policies Promote Greening? Evidence from China. Land Use Policy 2021, 104, 105389. [Google Scholar] [CrossRef]
- Ding, A.; Cenci, J.; Zhang, J. Links between the Pandemic and Urban Green Spaces, a Perspective on Spatial Indices of Landscape Garden Cities in China. Sustain. Cities Soc. 2022, 85, 104046. [Google Scholar] [CrossRef]
- Dumais, G.; Ellison, G.; Glaeser, E.L. Geographic Concentration as a Dynamic Process. Rev. Econ. Stat. 2002, 84, 193–204. [Google Scholar] [CrossRef]
- Zhang, J.; Cenci, J.; Becue, V.; Koutra, S. Research of the Industrial Heritage Category and Spatial Density Distribution in Walloon Region and Northeast China. WIT Trans. Built Environ. 2021, 203, 285. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, J.; Cenci, J.; Becue, V. Spatial Distribution Characteristics and Influencing Factors of the World Architectural Heritage. Heritage 2021, 4, 2942–2959. [Google Scholar] [CrossRef]
- Song, Y.; Wang, J.; Ge, Y.; Xu, C. An Optimal Parameters-Based Geographical Detector Model Enhances Geographic Characteristics of Explanatory Variables for Spatial Heterogeneity Analysis: Cases with Different Types of Spatial Data. GI Sci. Remote Sens. 2020, 57, 593–610. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, L.; Zhang, X.; Yang, M.; Zou, W. Efficiency Measurement and Spatial Spillover Effect of Provincial Health Systems in China: Based on the Two-Stage Network DEA Model. Front. Public Health 2022, 10, 952975. [Google Scholar] [CrossRef]
- Wang, K.; Zhang, Q.; Zhang, J. Analysis on Spatial Differences and Changes of Health Level in China. Adv. Appl. Math. 2022, 11, 7524–7532. [Google Scholar] [CrossRef]
- Ziafati Bafarasat, A.; Sharifi, A. How to Achieve a Healthy City: A Scoping Review with Ten City Examples. J. Urban Health 2024, 101, 120–140. [Google Scholar] [CrossRef]
- Xie, S.; Yin, G.; Wei, W.; Sun, Q.; Zhang, Z. Spatial–Temporal Change in Paddy Field and Dryland in Different Topographic Gradients: A Case Study of China during 1990–2020. Land 2022, 11, 1851. [Google Scholar] [CrossRef]
- Wang, X.-C.; Klemeš, J.J.; Dong, X.; Fan, W.; Xu, Z.; Wang, Y.; Varbanov, P.S. Air Pollution Terrain Nexus: A Review Considering Energy Generation and Consumption. Renew. Sustain. Energy Rev. 2019, 105, 71–85. [Google Scholar] [CrossRef]
- Xi, C.; Qian, T.; Chi, Y.; Chen, J.; Wang, J. Relationship between Settlements and Topographical Factors: An Example from Sichuan Province, China. J. Mt. Sci. 2018, 15, 2043–2054. [Google Scholar] [CrossRef]
- Chen, R.; Yin, P.; Wang, L.; Liu, C.; Niu, Y.; Wang, W.; Jiang, Y.; Liu, Y.; Liu, J.; Qi, J.; et al. Association between Ambient Temperature and Mortality Risk and Burden: Time Series Study in 272 Main Chinese Cities. BMJ 2018, 363, k4306. [Google Scholar] [CrossRef]
- Yao, N.; Li, Y.; Lei, T.; Peng, L. Drought Evolution, Severity and Trends in Mainland China over 1961–2013. Sci. Total Environ. 2018, 616–617, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, T.; Burkart, K.G.; Wang, H.; He, G.; Hu, J.; Xiao, J.; Yin, P.; Wang, L.; Liang, X.; et al. Mortality Burden Attributable to High and Low Ambient Temperatures in China and Its Provinces: Results from the Global Burden of Disease Study 2019. Lancet Reg. Health West. Pac. 2022, 24, 100493. [Google Scholar] [CrossRef] [PubMed]
- Gao, W. A Case Study of the Relationship Between Vegetation Coverage and Urban Heat Island in a Coastal City by Applying Digital Twins. Front. Plant Sci. 2022, 13, 861768. [Google Scholar]
- Zhou, M.; Huang, Y.; Li, G. Changes in the Concentration of Air Pollutants before and after the COVID-19 Blockade Period and Their Correlation with Vegetation Coverage. Environ. Sci. Pollut. Res. 2021, 28, 23405–23419. [Google Scholar] [CrossRef] [PubMed]
- Crane, M.; Lloyd, S.; Haines, A.; Ding, D.; Hutchinson, E.; Belesova, K.; Davies, M.; Osrin, D.; Zimmermann, N.; Capon, A.; et al. Transforming Cities for Sustainability: A Health Perspective. Environ. Int. 2021, 147, 106366. [Google Scholar] [CrossRef]
- Johnston, B.M.; Burke, S.; Kavanagh, P.M.; O’Sullivan, C.; Thomas, S.; Parker, S. Moving beyond Formulae: A Review of International Population-Based Resource Allocation Policy and Implications for Ireland in an Era of Healthcare Reform. HRB Open Res. 2021, 4, 121. [Google Scholar] [CrossRef]
- Marmot, M. Health Equity in England: The Marmot Review 10 Years On. BMJ 2020, 368, m693. [Google Scholar] [CrossRef]
- Bellini, P.; Nesi, P.; Pantaleo, G. IoT-Enabled Smart Cities: A Review of Concepts, Frameworks and Key Technologies. Appl. Sci. 2022, 12, 1607. [Google Scholar] [CrossRef]
- Wan, S.; Chen, Y.; Xiao, Y.; Zhao, Q.; Li, M.; Wu, S. Spatial Analysis and Evaluation of Medical Resource Allocation in China Based on Geographic Big Data. BMC Health Serv. Res. 2021, 21, 1084. [Google Scholar] [CrossRef]
- You, H.; Wu, X.; Guo, X. Distribution of COVID-19 Morbidity Rate in Association with Social and Economic Factors in Wuhan, China: Implications for Urban Development. Int. J. Environ. Res. Public Health 2020, 17, 3417. [Google Scholar] [CrossRef]
- Smith, S.A.; Mays, G.P.; Felix, H.C.; Tilford, J.M.; Curran, G.M.; Preston, M.A. Impact of Economic Constraints on Public Health Delivery Systems Structures. Am. J. Public Health 2015, 105, e48–e53. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Bai, Y.; Zhang, Z. Spatial Matching Analysis of Urban Health Resources and Population Distribution--A Case Study of the Central District of Lanzhou City. Resour. Dev. Mark. Chin. J. 2023, 39, 1619–1627. [Google Scholar] [CrossRef]
- Tan, X. Explaining Provincial Government Health Expenditures in China: Evidence from Panel Data 2007–2013. China Financ. Econ. Rev. 2017, 5, 9. [Google Scholar] [CrossRef]
- Zhang, D.; Rahman, K.M.A. Government Health Expenditure, OUT-OF-POCKET Payment and Social Inequality: A CROSS-NATIONAL Analysis of China and OECD Countries. Int. J. Health Plan. Manag. 2020, 35, 1111–1126. [Google Scholar] [CrossRef]
- Zhang, J.; Chang, Y.; Zhang, L.; Li, D. Do Technological Innovations Promote Urban Green Development?—A Spatial Econometric Analysis of 105 Cities in China. J. Clean. Prod. 2018, 182, 395–403. [Google Scholar] [CrossRef]
- Hu, F.; Qiu, L.; Xiang, Y.; Wei, S.; Sun, H.; Hu, H.; Weng, X.; Mao, L.; Zeng, M. Spatial Network and Driving Factors of Low-Carbon Patent Applications in China from a Public Health Perspective. Front. Public Health 2023, 11, 1121860. [Google Scholar] [CrossRef]
- 14th Five-Year Plan for the National Economic and Social Development of the People’s Republic of China and the Long-Range Objectives Through the Year 2035. Available online: http://www.gjbmj.gov.cn/n1/2021/0315/c409080-32051071.html (accessed on 15 August 2024).
- Zhu, J.; Chertow, M.R. Greening Industrial Production through Waste Recovery: “Comprehensive Utilization of Resources” in China. Environ. Sci. Technol. 2016, 50, 2175–2182. [Google Scholar] [CrossRef] [PubMed]
- Shu, Z.; Wang, Z.; Chen, R.; Li, M.; Lou, J.; Huang, X.; Wu, J.; Jing, L. Allocation and Development of the General Practitioner Workforce in China from 2012 to 2015: A Literature Review. Lancet 2017, 390, S91. [Google Scholar] [CrossRef]
- Yu, Q.; Yin, W.; Huang, D.; Sun, K.; Chen, Z.; Guo, H.; Wu, D. Trend and Equity of General Practitioners’ Allocation in China Based on the Data from 2012–2017. Hum. Resour. Health 2021, 19, 20. [Google Scholar] [CrossRef]
- Liu, H.; Fang, C.; Fan, Y. Mapping the Inequalities of Medical Resource Provision in China. Reg. Stud. Reg. Sci. 2020, 7, 568–570. [Google Scholar] [CrossRef]
- Kim, H.; Mahmood, A.; Goldsmith, J.V.; Chang, H.; Kedia, S.; Chang, C.F. Access to Broadband Internet and Its Utilization for Health Information Seeking and Health Communication among Informal Caregivers in the United States. J. Med. Syst. 2021, 45, 24. [Google Scholar] [CrossRef] [PubMed]
- Milinovich, G.J.; Williams, G.M.; Clements, A.C.A.; Hu, W. Internet-Based Surveillance Systems for Monitoring Emerging Infectious Diseases. Lancet Infect. Dis. 2014, 14, 160–168. [Google Scholar] [CrossRef]
- Wu, W.; Zhu, D.; Liu, W.; Wu, C.-H. Empirical Research on Smart City Construction and Public Health under Information and Communications Technology. Socioecon. Plann. Sci. 2022, 80, 100994. [Google Scholar] [CrossRef]
- Wang, L.; Xie, Q.; Xue, F.; Li, Z. Does Smart City Construction Reduce Haze Pollution? Int. J. Environ. Res. Public Health 2022, 19, 16421. [Google Scholar] [CrossRef] [PubMed]
- Rocha, N.P.; Dias, A.; Santinha, G.; Rodrigues, M.; Queirós, A.; Rodrigues, C. Smart Cities and Public Health: A Systematic Review. Procedia Comput. Sci. 2019, 164, 516–523. [Google Scholar] [CrossRef]
- Zhao, W.; Zou, Y. Smart Urban Governance in Epidemic Control: Practices and Implications of Hangzhou. Chin. Public Adm. Rev. 2021, 12, 51–60. [Google Scholar] [CrossRef]
- Zhang, Z.; Huang, Q.; Lu, Y.; Li, M.; Chen, Z.; LI, F. Analysis of Life Expectancy and the Spatial Differences of Its Influencing Factors of Chinese Residents. J. Geo-Inf. Sci. 2021, 23, 1575–1585. [Google Scholar] [CrossRef]
- Jain-Chandra, M.S.; Khor, N.; Mano, R.; Schauer, J.; Wingender, M.P.; Zhuang, J. Inequality in China–Trends, Drivers and Policy Remedies; International Monetary Fund: Washington, DC, USA, 2018; ISBN 1-4843-5753-1. [Google Scholar]
- Zhong, D.; Lu, Q.; Zhang, Y.; Li, J.; Lei, T.; Liu, C. How a Poverty Alleviation Policy Affected Comprehensive Disaster Risk Reduction Capacity: Evidence from China’s Great Western Development Policy. Int. J. Disaster Risk Reduct. 2024, 111, 104656. [Google Scholar] [CrossRef]
- Yang, F.; Yang, M.; Xue, B.; Luo, Q. The Effects of China’s Western Development Strategy Implementation on Local Ecological Economic Performance. J. Clean. Prod. 2018, 202, 925–933. [Google Scholar] [CrossRef]
- Pan, J.; Shallcross, D. Geographic Distribution of Hospital Beds throughout China: A County-Level Econometric Analysis. Int. J. Equity Health 2016, 15, 179. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, L.; Cui, Z.; Wang, Y. Study on Equity and Efficiency of Health Resources and Services Based on Key Indicators in China. PLoS ONE 2015, 10, e0144809. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Rao, K.; Wu, J.; Gakidou, E. China’s Health System Performance. Lancet 2008, 372, 1914–1923. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Administrative Region | NSCC Amount | Proportion/% | Cumulative Proportion/% |
|---|---|---|---|---|
| 1 | Jiangsu | 41 | 8.87 | 8.87 |
| 2 | Shandong | 35 | 7.58 | 16.45 |
| 3 | Zhejiang | 34 | 7.36 | 23.81 |
| 4 | Henan | 31 | 6.71 | 30.52 |
| 5 | Sichuan | 26 | 5.63 | 36.15 |
| 6 | Guangdong | 22 | 4.76 | 40.91 |
| 7 | Hubei | 20 | 4.33 | 45.24 |
| 8 | Chongqing | 20 | 4.33 | 49.57 |
| 9 | Shanghai | 18 | 3.90 | 53.46 |
| 10 | Beijing | 18 | 3.90 | 57.36 |
| 11 | Hunan | 15 | 3.25 | 60.61 |
| 12 | Yunnan | 15 | 3.25 | 63.85 |
| 13 | Tianjin | 15 | 3.25 | 67.10 |
| 14 | Shaanxi | 13 | 2.81 | 69.91 |
| 15 | Inner Mongolia | 13 | 2.81 | 72.73 |
| 16 | Jiangxi | 11 | 2.38 | 75.11 |
| 17 | Guizhou | 11 | 2.38 | 77.49 |
| 18 | Guangxi | 11 | 2.38 | 79.87 |
| 19 | Liaoning | 10 | 2.16 | 82.03 |
| 20 | Jilin | 10 | 2.16 | 84.20 |
| 21 | Xinjiang | 9 | 1.95 | 86.15 |
| 22 | Shanxi | 9 | 1.95 | 88.10 |
| 23 | Hainan | 8 | 1.73 | 89.83 |
| 24 | Hebei | 7 | 1.52 | 91.34 |
| 25 | Anhui | 7 | 1.52 | 92.86 |
| 26 | Ningxia | 7 | 1.52 | 94.37 |
| 27 | Fujian | 7 | 1.52 | 95.89 |
| 28 | Heilongjiang | 6 | 1.30 | 97.19 |
| 29 | Gansu | 6 | 1.30 | 98.48 |
| 30 | Qinghai | 4 | 0.87 | 99.35 |
| 31 | Tibet | 3 | 0.65 | 100.00 |
| Region | 2000 | 2011 | 2020 | |||
|---|---|---|---|---|---|---|
| Amount | Proportion/% | Amount | Proportion/% | Amount | Proportion/% | |
| Eastern region | 33 | 80.48 | 119 | 64.32 | 215 | 46.54 |
| Central region | 4 | 9.76 | 32 | 17.30 | 109 | 23.59 |
| Western region | 4 | 9.76 | 34 | 18.38 | 138 | 29.87 |
| Nationwide | 41 | 100.00 | 185 | 100.00 | 462 | 100.00 |
| Dimensions | Factors | Units |
|---|---|---|
| Economic and Population | X1: Total value of secondary and tertiary industries | 100 million yuan (RMB) |
| X2: Urban population at year-end | persons | |
| Policy Support and Technological Innovation | X3: Proportion of government health expenditure in total health expenditure | % |
| X4: Number of patent applications | pcs | |
| Urban Agglomerations and Urban Environment | X5: Total number of cities in provincial-level administrative regions | cities |
| X6: Comprehensive utilization rate of general industrial solid waste (utilized amount/generated amount) | % | |
| Medical Services and Resources | X7: Number of general practitioners | persons per 10,000 population |
| X8: Number of beds in urban healthcare institutions | beds/1000 persons | |
| Information Technology and Smart Living | X9: Urban broadband internet subscribers | 10,000 households |
| X10: Smart cities in provincial-level administrative regions | cities |
| No. | Function | Index |
|---|---|---|
| 1 | Nearest neighbour index | 0.85 |
| 2 | Geographic concentration index | 21.35 |
| 3 | Imbalance index | 0.3525 |
| 4 | Kernel density estimation | 0.20–5.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the International Society for Photogrammetry and Remote Sensing. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, Y.; Feng, L.; Cenci, J.; Zhang, J.; Cai, J. Analysis of Spatial and Driving Factors of National Sanitary Resources in China Using GIS. ISPRS Int. J. Geo-Inf. 2025, 14, 186. https://doi.org/10.3390/ijgi14050186
Deng Y, Feng L, Cenci J, Zhang J, Cai J. Analysis of Spatial and Driving Factors of National Sanitary Resources in China Using GIS. ISPRS International Journal of Geo-Information. 2025; 14(5):186. https://doi.org/10.3390/ijgi14050186
Chicago/Turabian StyleDeng, Yujia, Lixia Feng, Jeremy Cenci, Jiazhen Zhang, and Jun Cai. 2025. "Analysis of Spatial and Driving Factors of National Sanitary Resources in China Using GIS" ISPRS International Journal of Geo-Information 14, no. 5: 186. https://doi.org/10.3390/ijgi14050186
APA StyleDeng, Y., Feng, L., Cenci, J., Zhang, J., & Cai, J. (2025). Analysis of Spatial and Driving Factors of National Sanitary Resources in China Using GIS. ISPRS International Journal of Geo-Information, 14(5), 186. https://doi.org/10.3390/ijgi14050186