
The Study of the Aorta Metallomics in the Context of Atherosclerosis




Abstract
1. Introduction
2. Materials and Methods
2.1. Biological Material
2.2. ICP-OES Coupled Plasma Optical Emmision Spectrometer
2.3. Immunohistochemistry
2.4. Von Kossa Silver Test for Calcium
2.5. Statistics
3. Results
3.1. Preliminary Analysis
3.1.1. Average Analyte Contents
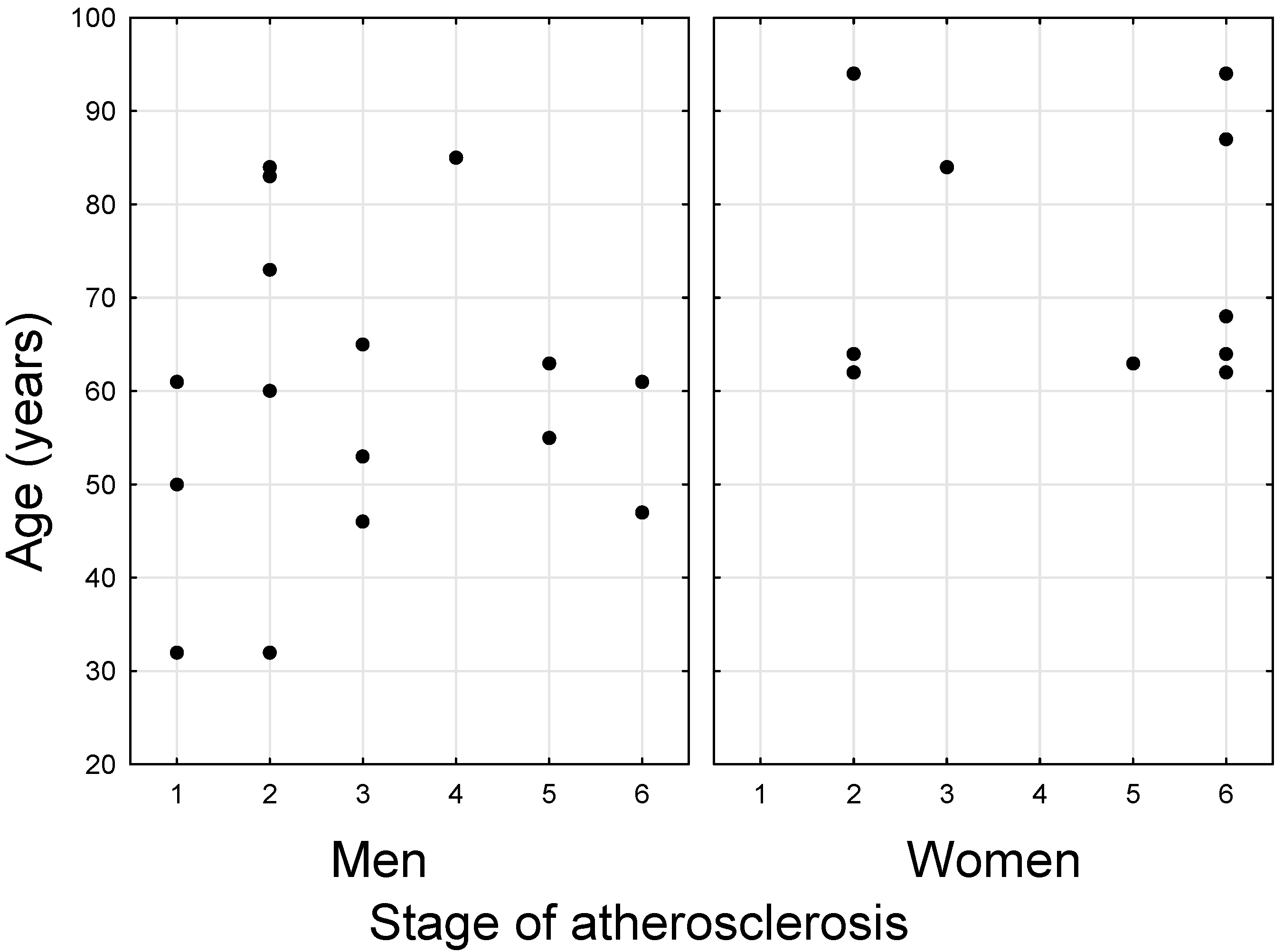
3.1.2. Differences in the Values of Variables between the Sexes
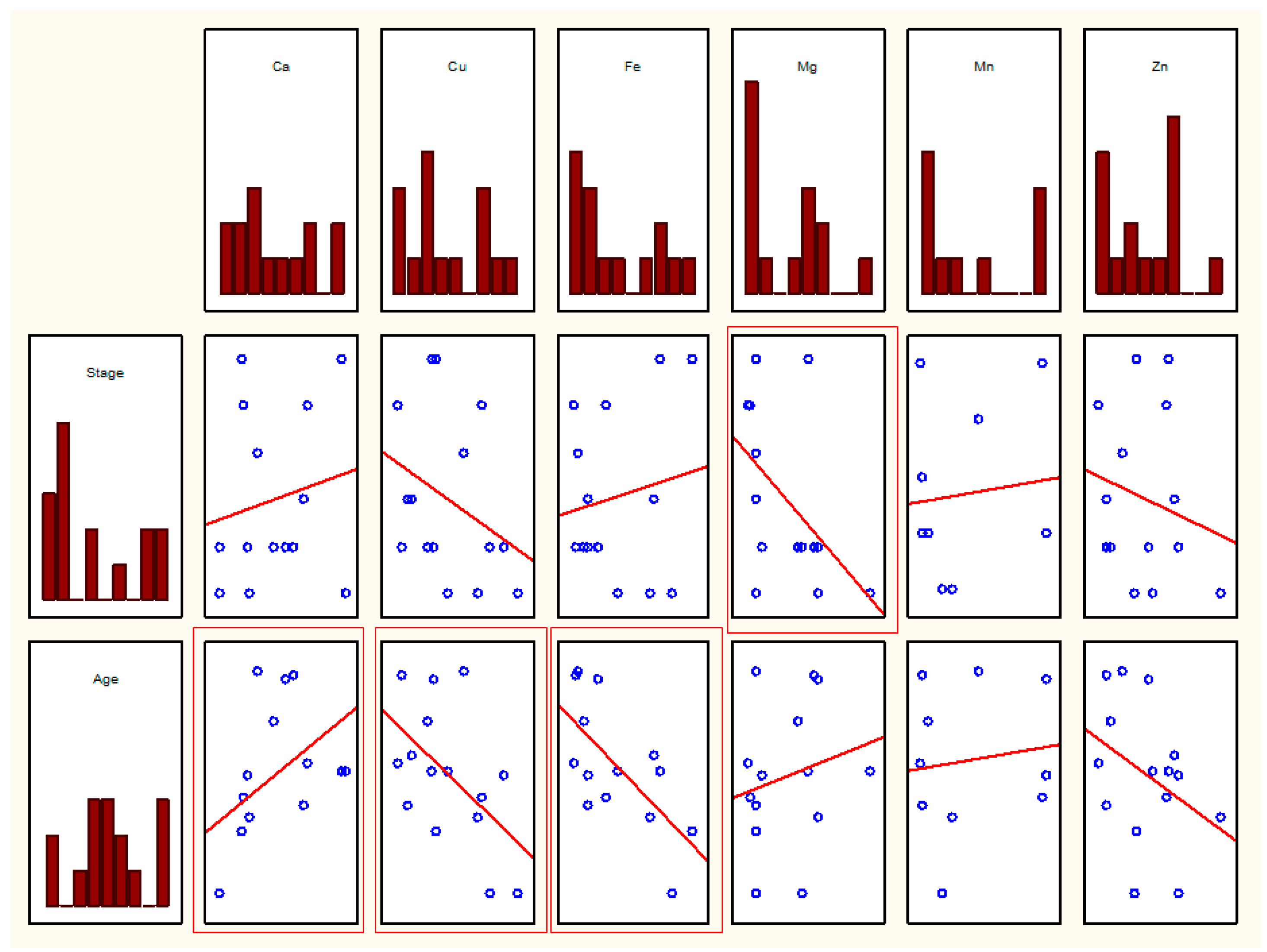
3.2. Statistical Analysis of the Relationship between Parameters
3.2.1. Correlation Matrix Including Ca, Cu, Fe, Mg, Mn, and Zn
3.2.2. Analysis of Cd, Pb, and Cr Content
Correlations
Comparison of N vs. T
- −
- Cd: no difference of any kind between n and y;
- −
- Cr: significantly higher values of Cu (p = 0.010) and Fe (p = 0.014) for n (i.e., below the Cr threshold);
- −
- Pb: significantly higher Cu values (p = 0.032) and almost significantly (p = 0.070) higher Fe for n (i.e., below the threshold Pb values).
3.2.3. Analysis Elements vs. Degree of Development of Atherosclerosis
3.2.4. Correlation Analysis among Samples in Advanced Disease Stages and in Early Atheroma Development Stages
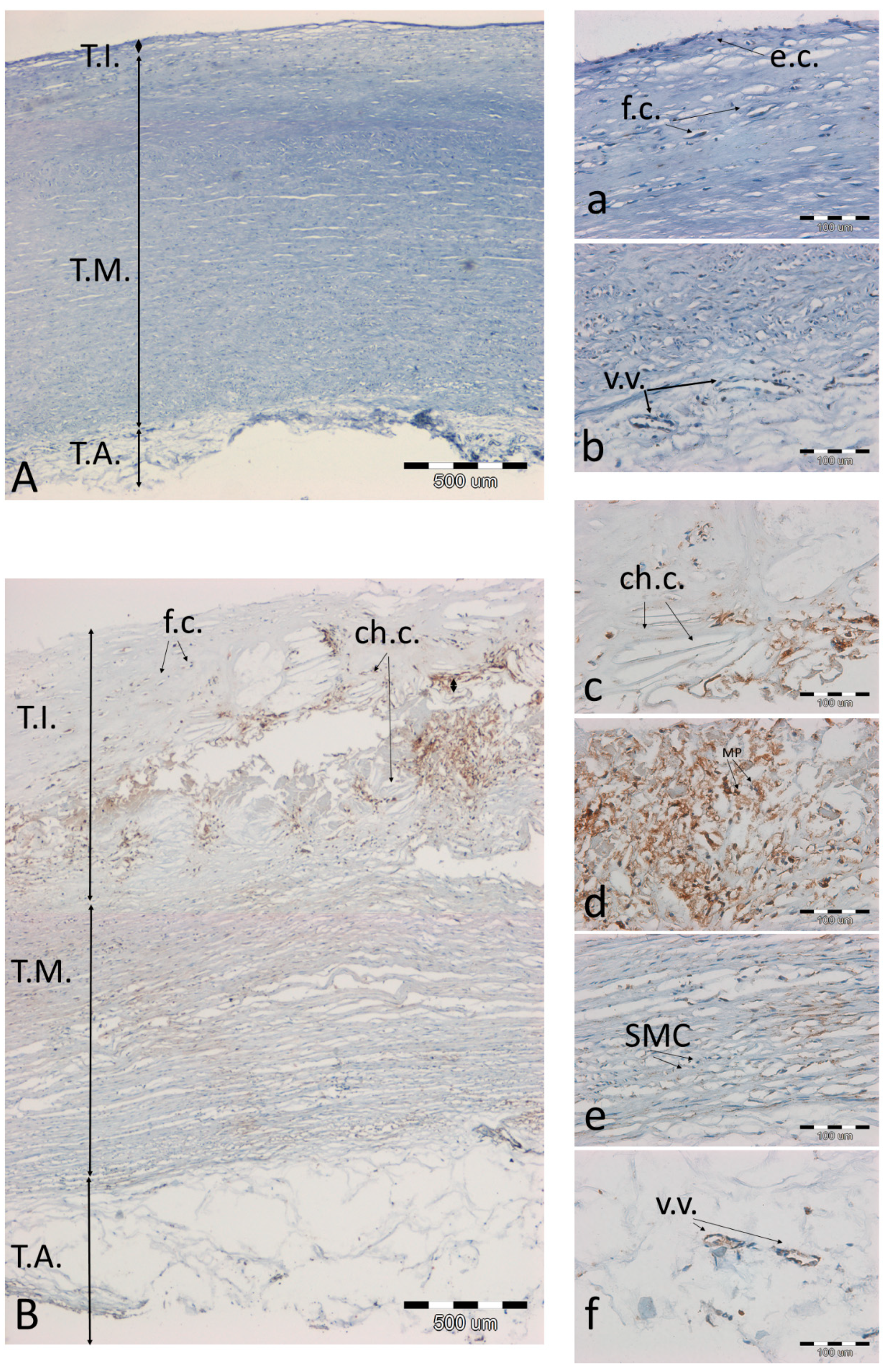
3.3. Analysis of Preparations with Immunohistochemical Detection of SOD2, MMP9, and NOS3 and Staining of Calcium Salts by the Von Kossa Method
4. Discussion
4.1. Sex-Related Differences
4.2. Iron
4.3. Calcium and Magnesium
4.4. Manganese
4.5. Copper
4.6. Zinc
4.7. Cadmium
4.8. Chrome and Lead
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wan, H.; Zhao, S.; Zeng, Q.; Tan, Y.; Zhang, C.; Liu, L.; Qu, S. CircRNAs in Diabetic Cardiomyopathy. Clin. Chim. Acta 2021, 517, 127–132. [Google Scholar] [CrossRef]
- Kansara, T.; Kumar, A.; Majmundar, M.; Basman, C. Mitral regurgitation following PASCAL mitral valve repair system: A single arm meta-analysis. Indian Heart J. 2020, 73, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Wang, Z.; Hong, J.; Che, Y.; Chen, R.; Hu, Z.; Hu, X.; Wu, Q.; Hu, J.; Zhang, M. Iron deficiency promotes aortic medial degeneration via destructing cytoskeleton of vascular smooth muscle cells. Clin. Transl. Med. 2021, 11, e276. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, A.; Shah, M.H. Multivariate statistical evaluation of trace metal levels in the blood of atherosclerosis patients in comparison with healthy subjects. Heliyon 2016, 2, e00054. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Edvinsson, M.; Ilbäck, N.G.; Frisk, P.; Thelin, S.; Nyström-Rosander, C. Trace Element Changes in Thoracic Aortic Dissection. Biol. Trace Elem. Res. 2016, 169, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Tasic, N.M.; Tasic, D.; Veselinovic, M.; Jakovljevic, V.; Djuric, D.; Radak, D. Iron concentrations in atherosclerotic plaque and serum in patients with carotid atherosclerosis. Acta Physiol. Hung. 2015, 102, 143–150. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Doehner, W.; Comin-Colet, J.; Cappellini, M.D.; Camaschella, C.; Francisco, A.; de Dignass, A.; Kadir, R.; Macdougall, I.C.; Spahn, D.R.; et al. Iron deficiency in chronic heart failure: Case-based practical guidance. ESC Heart Fail. 2018, 5, 764–771. [Google Scholar] [CrossRef]
- Ari, E.; Kaya, Y.; Demir, H.; Asicioglu, E.; Keskin, S. The correlation of serum trace elements and heavy metals with carotid artery atherosclerosis in maintenance hemodialysis patients. Biol. Trace Elem. Res. 2011, 144, 351–359. [Google Scholar] [CrossRef]
- Dinicolantonio, J.J.; Mangan, D.; O’Keefe, J.H. Copper deficiency may be a leading cause of ischaemic heart disease. Open Heart 2018, 5, 784. [Google Scholar] [CrossRef]
- Villa-Bellosta, R. Impact of magnesium:calcium ratio on calcification of the aortic wall. PLoS ONE 2017, 12, e0178872. [Google Scholar] [CrossRef]
- Kostov, K.; Halacheva, L. Role of magnesium deficiency in promoting atherosclerosis, endothelial dysfunction, and arterial stiffening as risk factors for hypertension. Int. J. Mol. Sci. 2018, 19, 1724. [Google Scholar] [CrossRef]
- Tangvoraphonkchai, K.; Davenport, A. Magnesium and Cardiovascular Disease. Adv. Chronic Kidney Dis. 2018, 25, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Avarebeel, S.; Choudhary, N.S.; Goudar, M.; Tejaswini, C.J. Correlation of trace elements in patients of chronic liver disease with respect to child—turcotte-pugh scoring system. J. Clin. Diagn. Res. 2017, 11, OC25–OC28. [Google Scholar] [CrossRef]
- Tomat, A.L.; de los Ángeles Costa, M.; Arranz, C.T. Zinc restriction during different periods of life: Influence in renal and cardiovascular diseases. Nutrition 2011, 27, 392–398. [Google Scholar] [CrossRef]
- Provenzano, M.; Andreucci, M.; Garofalo, C.; Faga, T.; Michael, A.; Ielapi, N.; Grande, R.; Sapienza, P.; de Franciscis, S.; Mastroroberto, P.; et al. The association of matrix metalloproteinases with chronic kidney disease and peripheral vascular disease: A light at the end of the tunnel? Biomolecules 2020, 10, 154. [Google Scholar] [CrossRef]
- Choi, S.; Liu, X.; Pan, Z. Zinc deficiency and cellular oxidative stress: Prognostic implications in cardiovascular diseases review-article. Acta Pharmacol. Sin. 2018, 39, 1120–1132. [Google Scholar] [CrossRef]
- Li, L.; Yang, X. The essential element manganese, oxidative stress, and metabolic diseases: Links and interactions. Oxid. Med. Cell. Longev. 2018, 2018, 7580707. [Google Scholar] [CrossRef] [PubMed]
- Fukai, T.; Ushio-Fukai, M. Superoxide dismutases: Role in redox signaling, vascular function, and diseases. Antioxid. Redox Signal. 2011, 15, 1583–1606. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Liu, P.; Pattar, G.R.; Tackett, L.; Bhonagiri, P.; Strawbridge, A.B.; Elmendorf, J.S. Chromium activates glucose transporter 4 trafficking and enhances insulin-stimulated glucose transport in 3T3-L1 adipocytes via a cholesterol-dependent mechanism. Mol. Endocrinol. 2006, 20, 857–870. [Google Scholar] [CrossRef] [PubMed]
- Nigra, A.E.; Ruiz-Hernandez, A.; Redon, J.; Navas-Acien, A.; Tellez-Plaza, M. Environmental Metals and Cardiovascular Disease in Adults: A Systematic Review beyond Lead and Cadmium. Curr. Environ. Health Rep. 2016, 3, 416–433. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, Y.; Zheng, L. Disease ionomics: Understanding the role of ions in complex disease. Int. J. Mol. Sci. 2020, 21, 8646. [Google Scholar] [CrossRef] [PubMed]
- Subrahmanyam, G.; Pathapati, R.M.; Ramalingam, K.; Indira, S.A.; Kantha, K.; Soren, B. Arterial stiffness and trace elements in apparently healthy population- A cross-sectional study. J. Clin. Diagn. Res. 2016, 10, LC12–LC15. [Google Scholar] [CrossRef] [PubMed]
- Tubsakul, A.; Sangartit, W.; Pakdeechote, P.; Kukongviriyapan, V.; Apaijit, K.; Kukongviriyapan, U. Curcumin mitigates hypertension, endothelial dysfunction and oxidative stress in rats with chronic exposure to lead and cadmium. Tohoku J. Exp. Med. 2021, 253, 69–76. [Google Scholar] [CrossRef]
- Ilmiawati, C.; Reza, M.; Yanni, M.; Rusjdi, D.A. Blood Cd levels and carotid intima-media thickness in young adults living in Padang, Indonesia. BMC Res. Notes 2020, 13. [Google Scholar] [CrossRef]
- Stary, H.C.; Chandler, A.B.; Dinsmore, R.E.; Fuster, V.; Glagov, S.; Insull, W.; Rosenfeld, M.E.; Schwartz, C.J.; Wagner, W.D.; Wissler, R.W. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. In A Report from the Committee on Vascular Lesions of the Council on Arteriosclerosis; American Heart Association: Dallas, TX, USA, 1995. [Google Scholar]
- Stary, H.C.; Chandler, A.B.; Glagov, S.; Guyton, J.R.; Insull, W.; Rosenfeld, M.E.; Schaffer, S.A.; Schwartz, C.J.; Wagner, W.D.; Wissler, R.W. A definition of initial, fatty streak, and intermediate lesions of atherosclerosis. In A Report from the Committee on Vascular Lesions of the Council on Arteriosclerosis; American Heart Association: Dallas, TX, USA, 1994. [Google Scholar]
- Rambousková, J.; Krsková, A.; Slavíková, M.; Čejchanová, M.; Wranová, K.; Procházka, B.; Černá, M. Trace elements in the blood of institutionalized elderly in the Czech Republic. Arch. Gerontol. Geriatr. 2013, 56, 389–394. [Google Scholar] [CrossRef]
- Thijs, L.; Staessen, J.; Amery, A.; Bruaux, P.; Buchet, J.P.; Claeys, F.; De Plaen, P.; Ducoffre, G.; Lauwerys, R.; Lijnen, P.; et al. Determinants of serum zinc in a random population sample of four Belgian towns with different degrees of environmental exposure to cadmium. Environ. Health Perspect. 1992, 98, 251–258. [Google Scholar] [CrossRef]
- Tasić, N.M.; Popović, A.D.; Tasić, D.; Otašević, P.; Veselinović, M.; Jakovljević, V.; Djurić, D.; Radak, D. Copper and zinc concentrations in atherosclerotic plaque and serum in relation to lipid metabolism in patients with carotid atherosclerosis. Vojn. Pregl. 2015, 72, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Bang, E.S.; Lee, J.H.; Lee, J.D.; Kang, D.R.; Hong, J.; Lee, J.M. Serum Concentrations of Trace Elements Zinc, Copper, Selenium, and Manganese in Critically Ill Patients. Biol. Trace Elem. Res. 2019, 188, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Dubick, M.A.; Hunter, G.C.; Carl, L.K. Trace Element and Mineral Concentrations in Serum and Aorta from Patients with Abdominal Aneurysmal or Occlusive Disease—UC Davis. Available online: https://ucdavis.pure.elsevier.com/en/publications/trace-element-and-mineral-concentrations-in-serum-and-aorta-from- (accessed on 22 June 2021).
- Tubek, S.; Tubek, S.; Szyguła, R. Gender differences in correlations between the content of elements in rain water and the frequency of hospitalization for arterial hypertension, chronic obstructive pulmonary disease, and psoriasis in opole voivodship, Poland, during 2000–2002. Biol. Trace Elem. Res. 2008, 126, 98–105. [Google Scholar] [CrossRef]
- Nawrot, T.; Geusens, P.; Nulens, T.S.; Nemery, B. Occupational cadmium exposure and calcium excretion, bone density, and osteoporosis in men. J. Bone Miner. Res. 2010, 25, 1441–1445. [Google Scholar] [CrossRef]
- Fairweather-Tait, S.J.; Wawer, A.A.; Gillings, R.; Jennings, A.; Myint, P.K. Iron status in the elderly. Mech. Ageing Dev. 2014, 136–137, 22–28. [Google Scholar] [CrossRef]
- Kali, A.; Yayar, O.; Erdogan, B.; Eser, B.; Buyukbakkal, M.; Ercan, Z.; Merhametsiz, O.; Haspulat, A.; Gök Oğuz, E.; Canbakan, B.; et al. Is hepcidin-25 a predictor of atherosclerosis in hemodialysis patients? Hemodial. Int. 2016, 20, 191–197. [Google Scholar] [CrossRef]
- Ebner, N.; von Haehling, S. Why is Iron Deficiency Recognised as an Important Comorbidity in Heart Failure? Card. Fail. Rev. 2019, 5, 173–175. [Google Scholar] [CrossRef] [PubMed]
- Lakhal-Littleton, S. Iron deficiency as a therapeutic target in cardiovascular disease. Pharmaceuticals 2019, 12, 125. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Tighiouart, H.; Manjunath, G.; MacLeod, B.; Griffith, J.; Salem, D.; Levey, A.S. Anemia as a risk factor for cardiovascular disease in the Atherosclerosis Risk in Communities (ARIC) study. J. Am. Coll. Cardiol. 2002, 40, 27–33. [Google Scholar] [CrossRef]
- Stadler, N.; Stanley, N.; Heeneman, S.; Vacata, V.; Daemen, M.J.A.P.; Bannon, P.G.; Waltenberger, J.; Davies, M.J. Accumulation of zinc in human atherosclerotic lesions correlates with calcium levels but does not protect against protein oxidation. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Husain, K.; Vazquez-Ortiz, M.; Lalla, J. Down regulation of aortic nitric oxide and antioxidant systems in chronic alcohol-induced hypertension in rats. Hum. Exp. Toxicol. 2007, 26, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Li, C.J.; Hou, M.F.; Chu, P.Y. New insights into the role of inflammation in the pathogenesis of atherosclerosis. Int. J. Mol. Sci. 2017, 18, 2034. [Google Scholar] [CrossRef] [PubMed]
- Joh, J.H.; Kim, D.I. Quantitative analysis of vascular calcification. Exp. Ther. Med. 2013, 7, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Florea, A.; Morgenroth, A.; Bucerius, J.; Schurgers, L.J.; Mottaghy, F.M. Locking and loading the bullet against micro-calcification. Eur. J. Prev. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wróbel, A.; Goncerz, G.; Kunz, J.; Podolec, P.; Rokita, E. Determination of the elemental composition of aortic valve cusps by EDXRF. X-Ray Spectrom. An Int. J. 2004, 33, 50–54. [Google Scholar] [CrossRef]
- Tzanakis, I.; Virvidakis, K.; Tsomi, A.; Mantakas, E.; Girousis, N.; Karefyllakis, N.; Papadaki, A.; Kallivretakis, N.; Mountokalakis, T. Intra- and extracellular magnesium levels and atheromatosis in haemodialysis patients. Magnes. Res. 2004, 17, 102–108. [Google Scholar]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia is a significant predictor of cardiovascular and non-cardiovascular mortality in patients undergoing hemodialysis. Kidney Int. 2014, 85, 174–181. [Google Scholar] [CrossRef]
- Leenders, N.H.J.; Vermeulen, E.A.; van Ballegooijen, A.J.; Hoekstra, T.; de Vries, R.; Beulens, J.W.; Vervloet, M.G. The association between circulating magnesium and clinically relevant outcomes in patients with chronic kidney disease: A systematic review and meta-analysis. Clin. Nutr. 2021, 40, 3133–3147. [Google Scholar] [CrossRef] [PubMed]
- Mendis, S. Magnesium, zinc, and manganese in atherosclerosis of the aorta. Biol. Trace Elem. Res. 1989, 22, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Absi, M.; Eid, B.G.; Ashton, N.; Hart, G.; Gurney, A.M. Simvastatin causes pulmonary artery relaxation by blocking smooth muscle ROCK and calcium channels: Evidence for an endothelium-independent mechanism. PLoS ONE 2019, 14, e0220473. [Google Scholar] [CrossRef]
- Agostoni, C.; Berni Canani, R.; Fairweather-Tait, S.; Heinonen, M.; Korhonen, H.; La Vieille, S.; Marchelli, R.; Martin, A.; Naska, A.; Neuhäuser-Berthold, M.; et al. Scientific Opinion on Dietary Reference Values for manganese. EFSA J. 2013, 11, 3419–3421. [Google Scholar] [CrossRef]
- Mehra, R.; Thakur, A.S. Relationship between lead, cadmium, zinc, manganese and iron in hair of environmentally exposed subjects. Arab. J. Chem. 2016, 9, S1214–S1217. [Google Scholar] [CrossRef]
- Hamilton, I.M.J.; Gilmore, W.S.; Strain, J.J. Marginal copper deficiency and atherosclerosis. Biol. Trace Elem. Res. 2000, 78, 179–189. [Google Scholar] [CrossRef]
- Malavolta, M.; Piacenza, F.; Basso, A.; Giacconi, R.; Costarelli, L.; Mocchegiani, E. Serum copper to zinc ratio: Relationship with aging and health status. Mech. Ageing Dev. 2015, 151, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Iskra, M.; Patelski, J.; Majewski, W. Relationship of calcium, magnesium, zinc and copper concentrations in the arterial wall and serum in atherosclerosis obliterans and aneurysm. J. Trace Elem. Med. Biol. 1997, 11, 248–252. [Google Scholar] [CrossRef]
- Kopriva, D.; Kisheev, A.; Meena, D.; Pelle, S.; Karnitsky, M.; Lavoie, A.; Buttigieg, J. The Nature of Iron Deposits Differs between Symptomatic and Asymptomatic Carotid Atherosclerotic Plaques. PLoS ONE 2015, 10, e0143138. [Google Scholar] [CrossRef]
- Pinheiro Júnior, J.E.G.; Moraes, P.Z.; Rodriguez, M.D.; Simões, M.R.; Cibin, F.; Pinton, S.; Barbosa Junior, F.; Peçanha, F.M.; Vassallo, D.V.; Miguel, M.; et al. Cadmium exposure activates NADPH oxidase, renin–angiotensin system and cyclooxygenase 2 pathways in arteries, inducing hypertension and vascular damage. Toxicol. Lett. 2020, 333, 80–89. [Google Scholar] [CrossRef]
- Meijer, G.W.; Beems, R.B.; Janssen, G.B.; Vaessen, H.A.M.G.; Speijers, G.J.A. Cadmium and atherosclerosis in the rabbit: Reduced atherogenesis by superseding of iron? Food Chem. Toxicol. 1996, 34, 611–621. [Google Scholar] [CrossRef]
- Szlacheta, Z.; Wasik, M.; Machon-Grecka, A.; Kasperczyk, A.; Dobrakowski, M.; Bellanti, F.; Szlacheta, P.; Kasperczyk, S. Potential Antioxidant Activity of Calcium and Selected Oxidative Stress Markers in Lead- And Cadmium-Exposed Workers. Oxid. Med. Cell. Longev. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Aaseth, J.; Skalny, A.V.; Suliburska, J.; Skalnaya, M.G.; Nikonorov, A.A.; Tinkov, A.A. Interactions of iron with manganese, zinc, chromium, and selenium as related to prophylaxis and treatment of iron deficiency. J. Trace Elem. Med. Biol. 2017, 41, 41–53. [Google Scholar] [CrossRef]
- Whitfield, P.; Parry-Strong, A.; Walsh, E.; Weatherall, M.; Krebs, J.D. The effect of a cinnamon-, chromium- and magnesium-formulated honey on glycaemic control, weight loss and lipid parameters in type 2 diabetes: An open-label cross-over randomised controlled trial. Eur. J. Nutr. 2016, 55, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Rondó, P.H.; Carvalho, M.D.F.H.; Souza, M.C.; Moraes, F. Lead, hemoglobin, zinc protoporphyrin and ferritin concentrations in children. Rev. Saude Publica 2006, 40, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Navas-Acien, A.; Selvin, E.; Sharrett, A.R.; Calderon-Aranda, E.; Silbergeld, E.; Guallar, E. Lead, cadmium, smoking, and increased risk of peripheral arterial disease. Circulation 2004, 109, 3196–3201. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cu | Fe | Mg | Mn | Zn | |
|---|---|---|---|---|---|
| Ca | −0.74 * | −0.39 | 0.36 | −0.65 * | −0.33 |
| Cu | 0.47 | −0.01 | 0.72 * | 0.61 * | |
| Fe | 0.09 | 0.52 | 0.60 * | ||
| Mg | 0.31 | 0.42 | |||
| Mn | 0.84 * |
| Cu | Fe | Mg | Mn | Zn | |
|---|---|---|---|---|---|
| Ca | −0.70 * | −0.6 | −0.38 | −0.82 * | −0.75 * |
| Cu | 0.90 * | 0.33 | 0.38 | 0.78 * | |
| Fe | 0.43 | 0.4 | 0.76 * | ||
| Mg | 0.29 | 0.31 | |||
| Mn | 0.37 |
| Ca | Cu | Fe | Mg | Mn | Zn | Stage of Atherosclerosis | Age | |
|---|---|---|---|---|---|---|---|---|
| Cd | −0.94 * | 0.83 * | 0.83 * | 0.70 | 0.70 | 0.83 * | −0.83 * | −0.68 |
| Cr | −0.40 | 1 | 1 | 0.80 | 0.50 | 0.20 | −0.26 | −0.33 |
| Pb | 0.20 | 0.50 | 0.60 | 0.40 | −0.50 | 1 | −0.63 |
| Ca | Cu | Fe | Mg | Mn | Zn | |
|---|---|---|---|---|---|---|
| Stage | 0.12 | −0.37 | 0.01 | −0.58 * | −0.17 | −0.23 |
| Age | 0.61 * | −0.55 * | −0.65 * | 0.23 | 0.07 | −0.36 |
| Cd | Cr | Cu | Fe | Mg | Mn | Pb | Zn | |
|---|---|---|---|---|---|---|---|---|
| Ca | −0.90 * | 0.3 | −0.44 | −0.37 | 0.11 | −0.37 | −0.4 | −0.4 |
| Cd | 1 | 0.90 * | 0.3 | 0.8 | 0.7 | |||
| Cr | 1 | 1 | 0.90 * | 0.8 | 0.5 | 0.6 | ||
| Cu | 0.73 * | 0.22 | 0.65 * | 0.6 | 0.75 * | |||
| Fe | 0.29 | 0.65 * | 0.8 | 0.77 * | ||||
| Mg | 0.27 | 0.6 | 0.31 | |||||
| Mn | −0.5 | 0.67 * | ||||||
| Pb | 1 |
| Cu | Fe | Mg | Mn | Zn | |
|---|---|---|---|---|---|
| Ca | −0.52 | −0.27 | 0.81 * | 0.33 | −0.21 |
| Cu | 0.52 | −0.32 | 0.59 | 0.71 * | |
| Fe | 0.17 | 0.61 | 0.59 | ||
| Mg | 0.44 | 0.18 | |||
| Mn | 0.78 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuzan, A.; Wujczyk, M.; Wiglusz, R.J. The Study of the Aorta Metallomics in the Context of Atherosclerosis. Biomolecules 2021, 11, 946. https://doi.org/10.3390/biom11070946
Kuzan A, Wujczyk M, Wiglusz RJ. The Study of the Aorta Metallomics in the Context of Atherosclerosis. Biomolecules. 2021; 11(7):946. https://doi.org/10.3390/biom11070946
Chicago/Turabian StyleKuzan, Aleksandra, Marta Wujczyk, and Rafal J. Wiglusz. 2021. "The Study of the Aorta Metallomics in the Context of Atherosclerosis" Biomolecules 11, no. 7: 946. https://doi.org/10.3390/biom11070946
APA StyleKuzan, A., Wujczyk, M., & Wiglusz, R. J. (2021). The Study of the Aorta Metallomics in the Context of Atherosclerosis. Biomolecules, 11(7), 946. https://doi.org/10.3390/biom11070946