
Long-Term Effects on the Lipidome of Acute Coronary Syndrome Patients

 , , , ,
, , , , 
Abstract
:
1. Introduction
2. Results
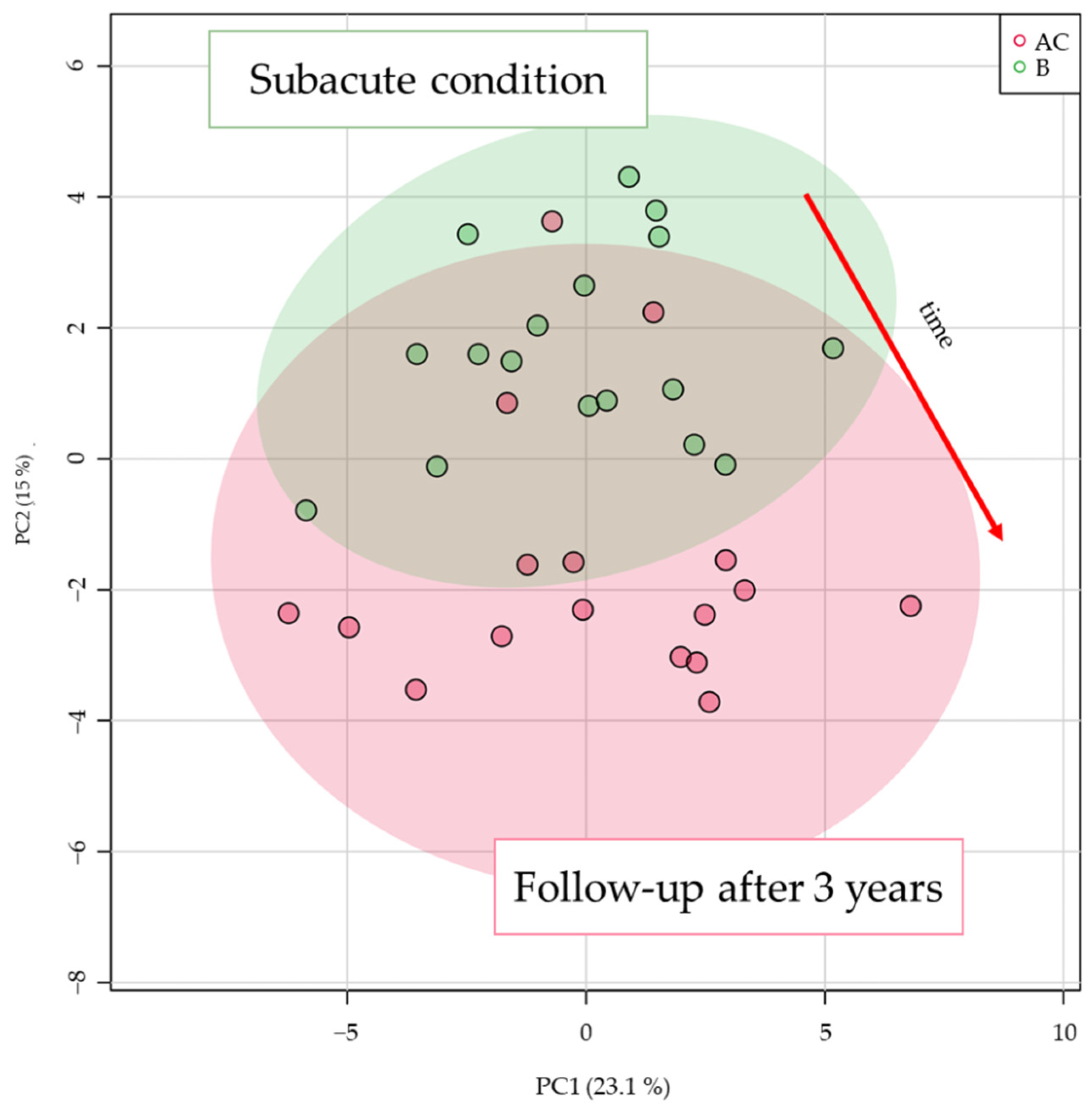
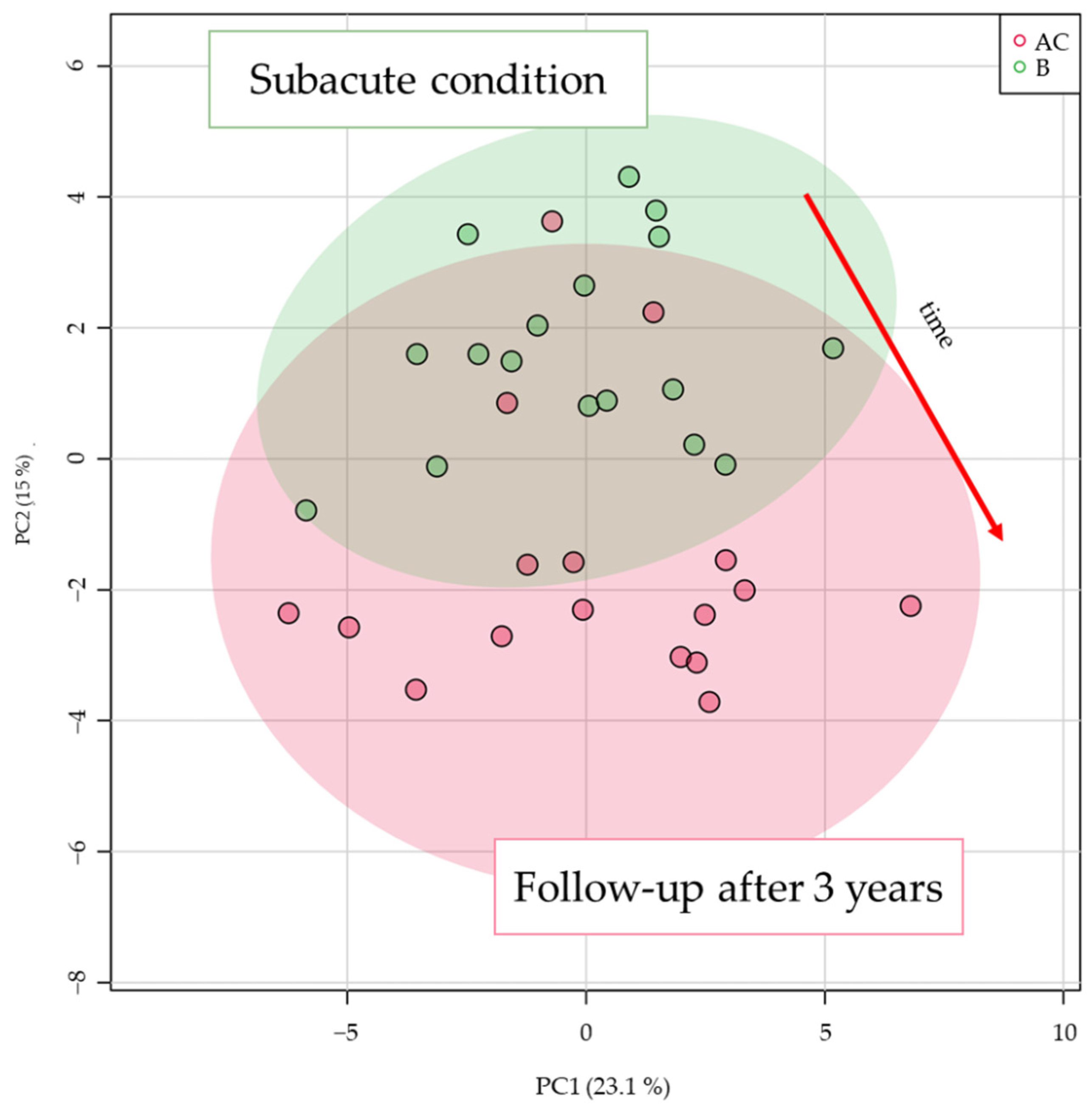
2.1. Multivariate Analysis for Data Overview
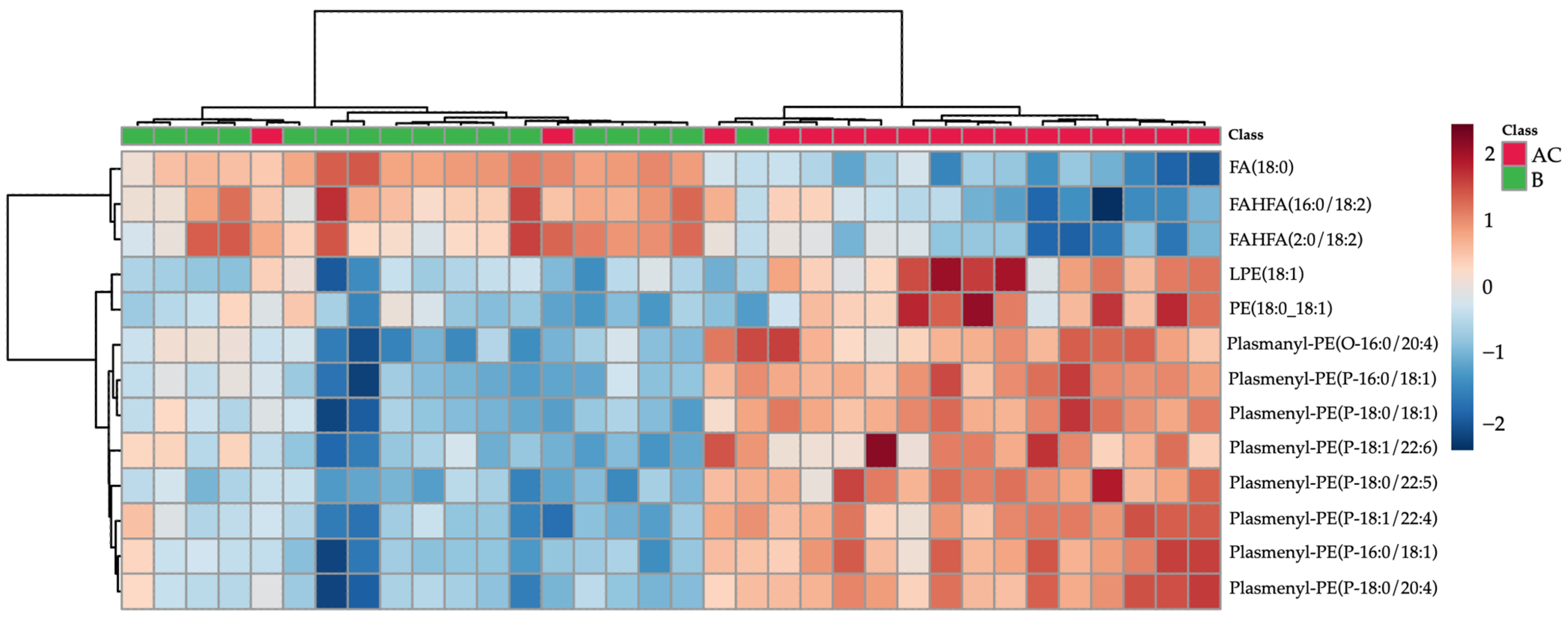
2.2. Time Effect for ACS Patient Lipidome
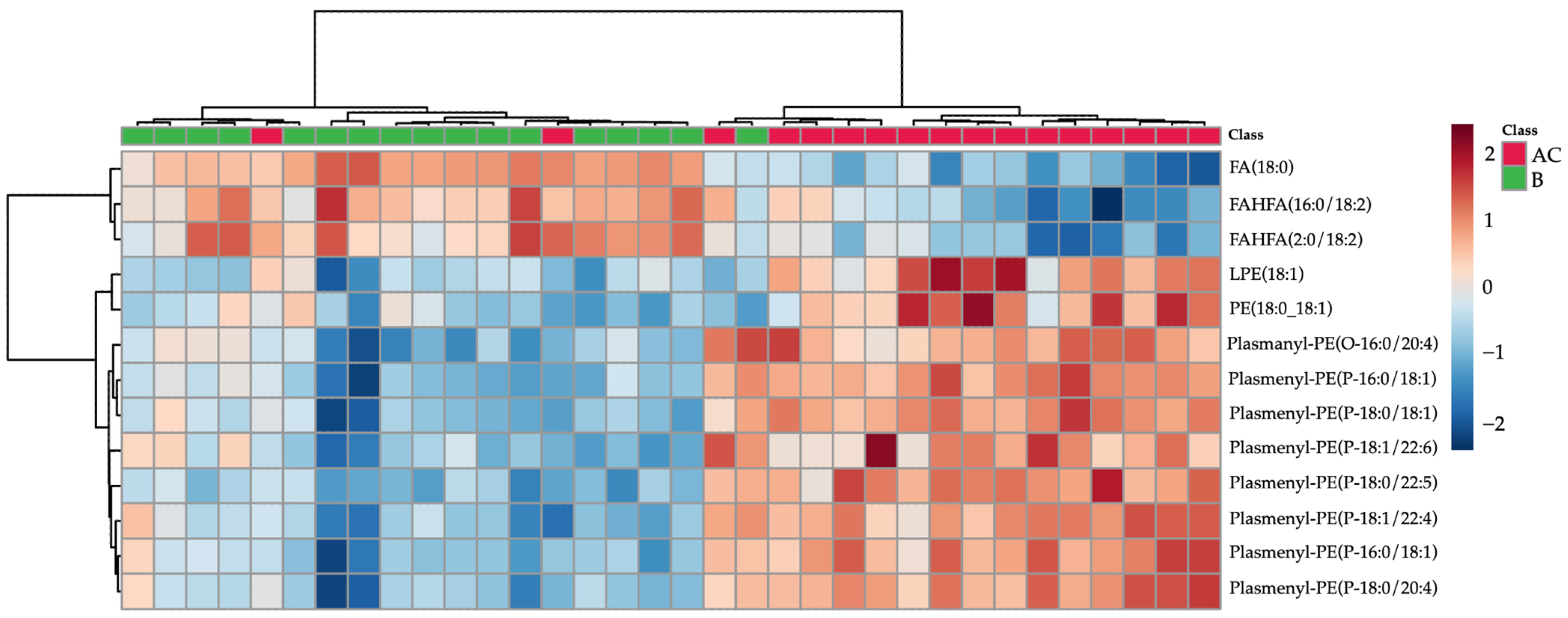
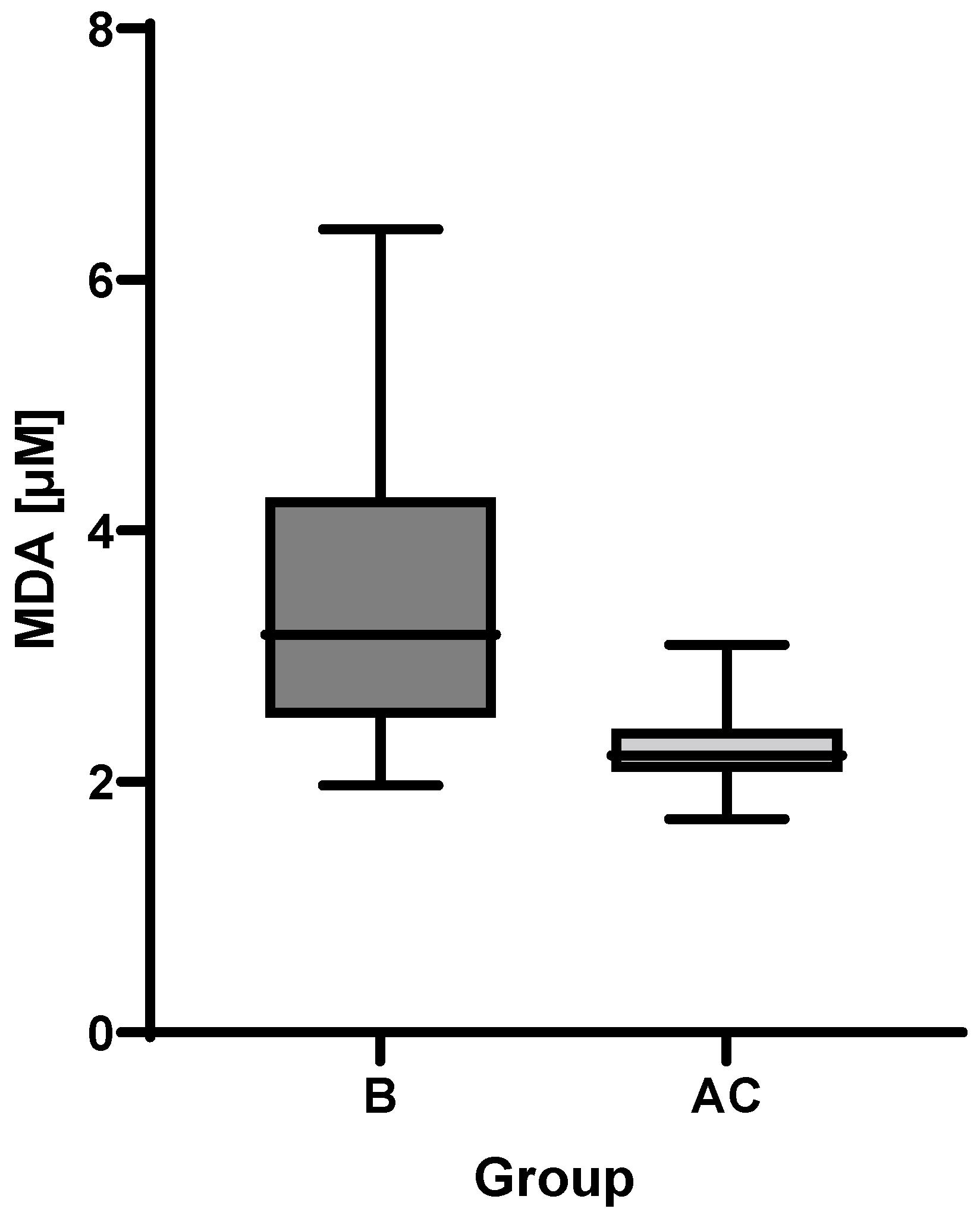
2.3. MDA Analysis
3. Discussion
4. Materials and Methods
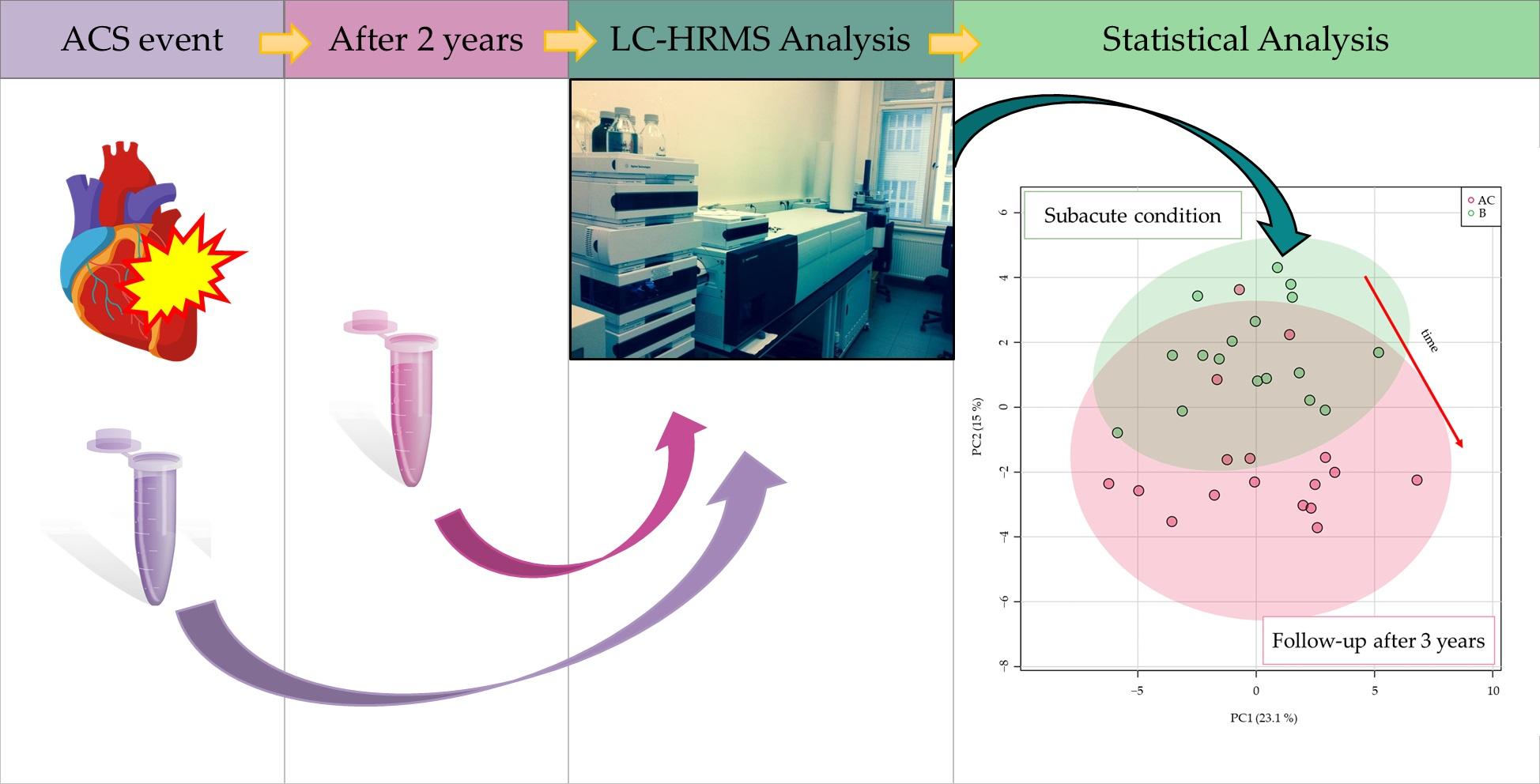
4.1. Study Design
4.2. Chemicals and Materials
4.3. Sample Collection
4.4. Sample Preparation
4.5. Instrumental Conditions
4.6. Data Processing for Fingerprinting Experiment
5. Limitations of the Study
6. Conclusions
- The concentration of MDA, an oxidative stress marker, decreased, and plasma antioxidant capacity, as indicated by higher levels of plasmalogens, increased.
- The observed increase in FAHFA class lipids in samples of subacute patients may be indicative of the inflammation that accompanies ACS; a subsequent decrease of these lipids in follow-up samples was observed.
- Further investigation of lipidome changes in a larger cohort over a longer period of time might confirm the above observations, and possibly complement existing knowledge.
- The lipidome changes attributable strictly to ACS seems to be very limited in long-term basis.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fan, A.; Wu, X.; Wu, H.; Li, L.; Huang, R.; Zhu, Y.; Qiu, Y.; Fu, J.; Ren, J.; Zhu, C. Atheroprotective Effect of Oleoylethanolamide (OEA) Targeting Oxidized LDL. PLoS ONE 2014, 9, e85337. [Google Scholar] [CrossRef] [PubMed]
- Maiolino, G.; Rossitto, G.; Caielli, P.; Bisogni, V.; Rossi, G.P.; Calò, L.A. The Role of Oxidized Low-Density Lipoproteins in Atherosclerosis: The Myths and the Facts. Mediat. Inflamm. 2013, 2013, 714653. [Google Scholar] [CrossRef] [Green Version]
- Giovanni, D.; Carlo, P. Platelet Activation and Atherothrombosis. N. Engl. J. Med. 2007, 357, 2482–2494. [Google Scholar]
- Malý, M.; Hajšl, M.; Bechyňská, K.; Kučerka, O.; Šrámek, M.; Suttnar, J.; Hlaváčková, A.; Hajšlová, J.; Kosek, V. Lipidomic Analysis to Assess Oxidative Stress in Acute Coronary Syndrome and Acute Stroke Patients. Metabolites 2021, 11, 412. [Google Scholar] [CrossRef]
- Mundra, P.; Barlow, C.K.; Nestel, P.J.; Barnes, E.H.; Kirby, A.; Thompson, P.; Sullivan, D.R.; Alshehry, Z.H.; Mellett, N.A.; Huynh, K.; et al. Large-scale plasma lipidomic profiling identifies lipids that predict cardiovascular events in secondary prevention. JCI Insight 2018, 3, e121326. [Google Scholar] [CrossRef]
- Park, J.Y.; Lee, S.-H.; Shin, M.-J.; Hwang, G.-S. Alteration in Metabolic Signature and Lipid Metabolism in Patients with Angina Pectoris and Myocardial Infarction. PLoS ONE 2015, 10, e0135228. [Google Scholar] [CrossRef] [Green Version]
- Toledo, E.; Wang, D.D.; Ruiz-Canela, M.; Clish, C.B.; Razquin, C.; Zheng, Y.; Guasch-Ferré, M.; Hruby, A.; Corella, D.; Gómez-Gracia, E.; et al. Plasma lipidomic profiles and cardiovascular events in a randomized intervention trial with the Mediterranean diet. Am. J. Clin. Nutr. 2017, 106, 973–983. [Google Scholar] [CrossRef]
- Koelmel, J.P.; Kroeger, N.M.; Ulmer, C.Z.; Bowden, J.A.; Patterson, R.E.; Cochran, J.A.; Beecher, C.W.W.; Garrett, T.J.; Yost, R.A. LipidMatch: An automated workflow for rule-based lipid identification using untargeted high-resolution tandem mass spectrometry data. BMC Bioinform. 2017, 18, 331. [Google Scholar] [CrossRef]
- Chen, H.; Wang, Z.X.; Qin, M.; Zhang, B.; Lin, L.; Ma, Q.L.; Liu, C.; Chen, X.P.; Li, H.P.; Lai, W.H.; et al. Comprehensive Metabolomics Identified the Prominent Role of Glycerophospholipid Metabolism in Coronary Artery Disease Progression. Front. Mol. Biosci. 2021, 8, 632950. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lipid Name | Detected Adduct | Retention Time [min] | m/z Value | t-Test FDR p-Value | PLS-DA VIP Score |
|---|---|---|---|---|---|
| Plasmenyl-PE(P-18:0/22:5) | [M − H]− | 10.48 | 776.5602 | 3.94 × 10−5 | 1.31 |
| Plasmenyl-PE(P-18:0/20:4) | [M − H]− | 10.52 | 750.5422 | 7.51 × 10−5 | 1.28 |
| Plasmenyl-PE(P-18:0/18:1) | [M − H]− | 11.43 | 728.5593 | 1.54 × 10−4 | 1.24 |
| Plasmenyl-PE(P-16:0/20:4) | [M − H]− | 9.643 | 722.5105 | 7.51 × 10−5 | 1.24 |
| Plasmenyl-PE(P-16:0/18:1) | [M − H]− | 10.59 | 700.5269 | 1.54 × 10−4 | 1.23 |
| Plasmenyl-PE(P-18:1/20:4) | [M − H]− | 9.658 | 748.5265 | 8.33 × 10−4 | 1.20 |
| LPE(18:1) | [M − H]− | 3.013 | 478.2923 | 2.83 × 10−4 | 1.09 |
| Plasmenyl-PE(O-16:0/20:4) | [M − H]− | 9.982 | 724.5262 | 4.11 × 10−3 | 1.08 |
| FAHFA(16:0/18:2) | [M − H]− | 5.078 | 533.4528 | 5.55 × 10−3 | 1.07 |
| Plasmenyl-PE(P-18:1/22:6) | [M − H]− | 9.359 | 772.5261 | 2.52 × 10−3 | 1.05 |
| PE(18:0_18:1) | [M − H]− | 10.99 | 744.5526 | 1.62 × 10−4 | 1.03 |
| FAHFA(2:0/18:2) | [M − H]− | 5.078 | 337.2339 | 2.23 × 10−2 | 1.02 |
| FA(18:0) | [M − H]− | 6.535 | 283.2636 | 4.94 × 10−2 | 1.01 |
| Patient Characteristics | Group B (n = 17) |
|---|---|
| Age (y) | 61 |
| Sex (m/f) | 12/5 |
| Clinical characterization | |
| Arterial hypertension (n/%) | 11/65 |
| Diabetes mellitus (n/%) | 4/24 |
| Current smoker (n/%) | 9/53 |
| BMI | 29.2 |
| Medical history | |
| History of MI (n/%) | 1/6 |
| History of PCI (n/%) | 1/6 |
| Laboratory results | |
| CKD epi (mL/min) | 88.7 |
| Kreatinin (µmol/L) | 75 |
| Total cholesterol (mmol/L) | 4.5 |
| TAG (mmol/L) | 1.1 |
| LDL cholesterol (mmol/L) | 2.9 |
| HDL cholesterol (mmol/L) | 1.1 |
| Post-procedure hypolidimic treatment | |
| Statin (n/%) | 17/100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosek, V.; Hajšl, M.; Bechyňská, K.; Kučerka, O.; Suttnar, J.; Hlaváčková, A.; Hajšlová, J.; Malý, M. Long-Term Effects on the Lipidome of Acute Coronary Syndrome Patients. Metabolites 2022, 12, 124. https://doi.org/10.3390/metabo12020124
Kosek V, Hajšl M, Bechyňská K, Kučerka O, Suttnar J, Hlaváčková A, Hajšlová J, Malý M. Long-Term Effects on the Lipidome of Acute Coronary Syndrome Patients. Metabolites. 2022; 12(2):124. https://doi.org/10.3390/metabo12020124
Chicago/Turabian StyleKosek, Vít, Martin Hajšl, Kamila Bechyňská, Ondřej Kučerka, Jiří Suttnar, Alžběta Hlaváčková, Jana Hajšlová, and Martin Malý. 2022. "Long-Term Effects on the Lipidome of Acute Coronary Syndrome Patients" Metabolites 12, no. 2: 124. https://doi.org/10.3390/metabo12020124
APA StyleKosek, V., Hajšl, M., Bechyňská, K., Kučerka, O., Suttnar, J., Hlaváčková, A., Hajšlová, J., & Malý, M. (2022). Long-Term Effects on the Lipidome of Acute Coronary Syndrome Patients. Metabolites, 12(2), 124. https://doi.org/10.3390/metabo12020124