

Staphylococcus aureus Genomic Analysis and Outcomes in Patients with Bone and Joint Infections: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Searched
2.2. Data Extraction
2.3. Data Synthesis and Analysis
3. Results and Discussion
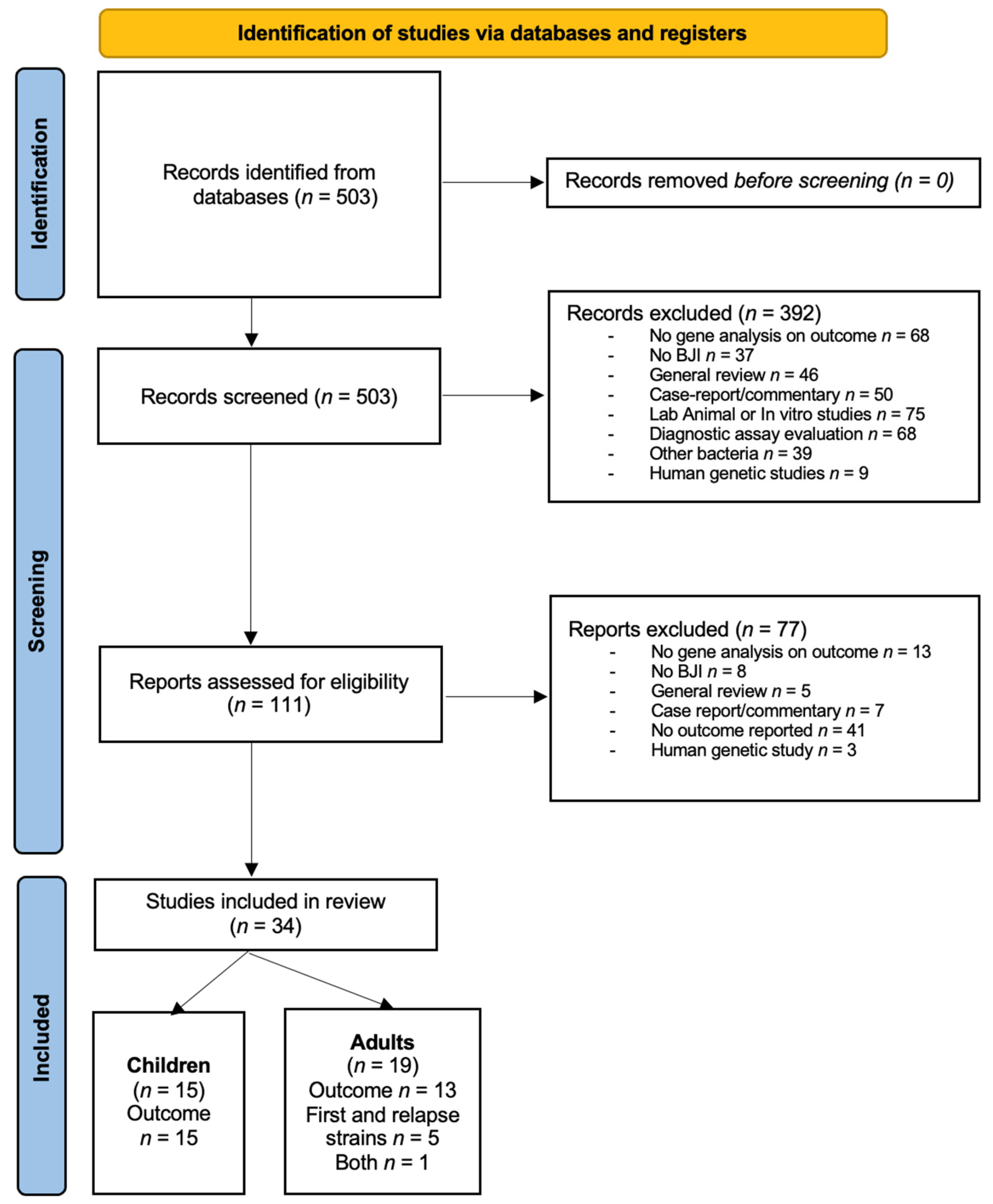
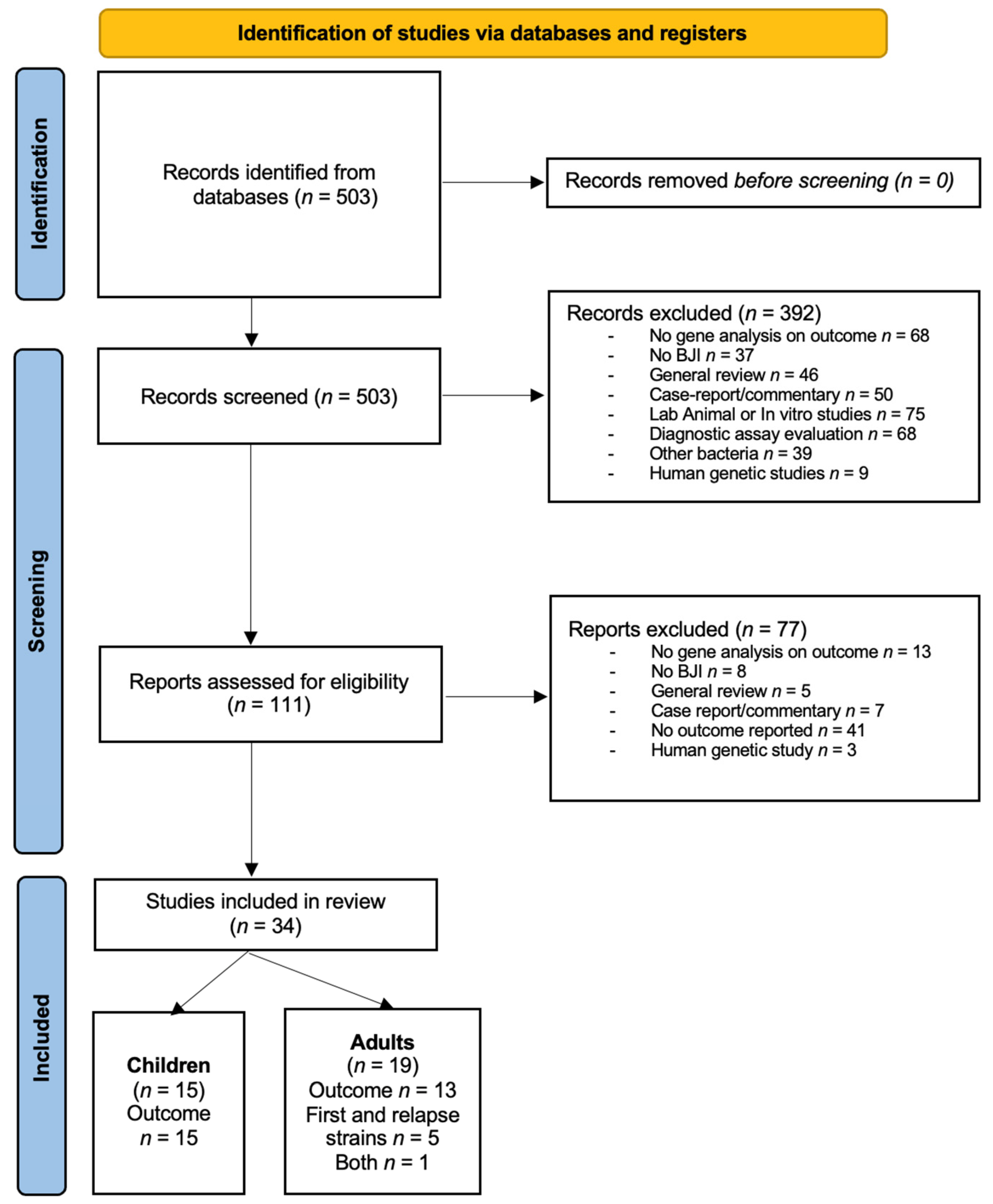
3.1. Studies Included
3.2. BJI in Children
3.2.1. Studies Included
3.2.2. PVL
3.2.3. Sequence Type/Clonal Complex
3.2.4. Other Genes
3.2.5. Quality of Studies
3.3. BJI in Adults
3.3.1. Studies Included
3.3.2. PVL
3.3.3. Sequence Type/Clonal Complex
3.3.4. Other Virulence Genes

{kind=link}
| Reference | Study Design | Country | Years of Study | Number of Patients/Strains | MRSA n, (%) | Type of BJI | Genomic Analysis | Comparison | Follow-Up | Genotype and Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Banerjee et al., 2020 [34] | Prospective single-center | India | 2018–2019 | 60/60 | 40/60 (67) | OM, arthritis, spondylodiscitis Presence of foreign bodies (n = 30) | PCR lukS-PV, lukF-PV, lukD and lukE | Recovered (n = 46) vs. not recovered (n = 14) | All patients were followed up for six months after the end of treatment for the initial infection | In BJI with foreign body (n = 30), factors associated with unresolved infection (univariate analysis): Age: OR (95% CI) = 0.94 (0.88–1.0), p = 0.049 Number of surgical interventions: OR (95% CI) = 10.68 (1.37–83.52), p = 0.024 Duration of antibiotics: OR (95% CI) = 1.07 (1.01–1.13), p = 0.029 Presence of luk genes was not associated with unresolved infection: OR (95% CI) = 2.0 (0.38–10.51), p = 0.413 In BJI without foreign body (n = 30), no factor significantly differed Presence of any luk genes: OR (95% CI) = 0.44 (0.22-23.27), p = 0.413 |
| Bouiller et al., 2020 [25] | Retrospective single-center | France | 2010–2017 | 244/244 | 37/244 (15) | DFI with OM | PCR CC398-lineage specific | CC398 (n = 37) vs. non-CC398 (n = 207) | ND | In multivariate analysis, a patient with S. aureus CC398 DFI had more severe infection (IWGDF-IDSA grade 4): 23/37, 62% vs. 33/207, 16%, OR (95% CI) = 8.5 (3.5–20.7), p < 0.001 |
| Chen et al., 2022 [27] | Retrospective single-center | Taiwan | 2016–2019 | 36/36 | 0 | Acute PJI | PCR lukS-PV, lukF-PV, MLST | ST239 (n = 11) vs. ST8 (n = 10) vs. ST59 (n = 8) vs. other ST (n = 7) | ND | Number of surgical debridements ST239 vs. ST8: n = 10/11, 91% vs. n = 4/10, 40%, p < 0.05 ST239 vs. ST59: n = 10/11, 91% vs. n = 6/8, 75%, p > 0.05 ST239 vs. other ST: n = 10/11, 91% vs. n = 7/7, 100%, p > 0.05 Number of hospital admissions ST239 vs. ST8: n = 7/11, 64% vs. n = 5/10 50%, p > 0.05 ST239 vs. ST59: n = 7/11, 64% vs. n = 5/8 63%, p > 0.05 ST239 vs. other ST: n = 7/11, 64% vs. n = 6/7, 86%, p > 0.05 Pre-operative CRP (mg/L, mean ± SD): ST239 vs. ST8: 279.16 ± 109.53 vs. 66.8 ± 57.56, p < 0.05 ST239 vs. ST59: 279.16 ± 109.53 vs. 184.29 ± 90.60, p < 0.05 ST239 vs. other ST: 279.16 ± 109.53 vs. 118.19 ± 100, p < 0.05 Fever (no p-value provided) ST239 vs. ST8: n = 7/11, 64% vs. n = 1/10, 10% ST239 vs. ST59: n = 7/11, 64% vs. n = 0/8 ST239 vs. other ST: n = 7/11, 64% vs. n = 1/7, 14% Prevalence of PVL was higher in ST8 than other STs: ST8: n = 9/10 (90%) ST59: n = 6/8 (75%) ST239: n = 5/11 (46%) |
| Jiang et al., 2017 [24] | Retrospective, single-center | China | 2013–2015 | 60/60 | 9/60 (15) | OM | Multiplex PCR 1 | PVL+ (n = 17) vs. PVL− (n = 43) Duration time of OM < 24 months or >24 months and <20 years or >20 years | ND | OM duration was significantly longer in PVL-positive patients (mean ± SD): 192.1 ± 150 mo versus 50.0 ± 150 mo, p = 0.00060 PVL gene presence was positively associated both with OM duration of greater than 24 months (p = 0.00030) and greater than 20 years (p = 0.00030) Presence of bbp (p = 0.016) and sei (p = 0.041) genes were associated with OM duration of longer than 20 years |
| Kalinka et al., 2014 [31] | Retrospective multicenter | Argentina | ND | 21/21 | 7/21 (33) | OM | PCR and/or RT-PCR 2 | Acute OM (<2 months) (n = 11) vs. chronic OM (>2 months) (n = 10) | ND | Little difference between the presence or absence of genes and acute or chronic OM, but no statistical analysis was performed to compare the 2 groups bbp: 9% vs. 0% cna: 27% vs. 10% fnbB: 82% vs. 100% sdrD: 100% vs. 100% sdrE: 82% vs. 100% |
| Muñoz-Gallego et al., 2017 [32] | Retrospective, single-center | Spain | 2005–2015 | 18/18 | 18/18 (100) | PJI | DNA microarrays 3 PFGE, MLST | Failure 4 vs. cure | 688 days (median) | No significant differences but a trend towards a higher frequency in failure group of: sak: 80.0% vs. 37.5% (p = 0.145) chp: 80.0% vs. 25.0% (p = 0.054) scn: 80.0% vs. 37.5% (p = 0.145) |
| Muñoz-Gallego et al., 2020 [28] | Prospective multicenter | Spain | 2016–2017 | 88/88 | 20/88 (22.7) | PJI | DNA microarrays 3 | Failure 5 vs. cure | 1 year | No genotypic or phenotypic characteristics predicted failure, except vancomycin MIC ≥ 1.5 mg/L (23.1% failure vs. 3.4% cure, p = 0.044). Clonal complex (p = 0.574), and strains with different agr type (p = 0.434) were not predictive of failure Trend toward greater presence of S. aureus belonging to CC5 (30.8% vs. 13.8%, p = 0.192) and agr type II (46.2% vs. 24.1%, p = 0.099) among the failures |
| Muñoz-Gallego et al., 2022 [33] | Prospective multicenter | Spain | 2016–2107 | 14/20 | 2/18 6 (11) | PJI with DAIR (symptoms < 21 days) | WGS | Relapse/persistent (n = 6) vs. Cured (n = 8) | 1 year | No association between the presence or absence of genes and persistent or relapsing PJI versus resolved PJI No significant difference between strains causing persistent or relapsing PJI and those with a favorable outcome |
| Peyrani et al., 2012 [35] | Retrospective, single-center | USA | 2007–2008 | 50/50 | 50/50 (100) | OM | PFGE, PCR PVL gene (unspecified) | Success 7 (n = 37) vs. failure (n = 13) | >1 year | No correlation with USA300 pulsotype, PVL, SCCmec or agr type USA300: n = 21/37, 56.8% vs. N = 6/13, 46.2% (p = 0.537) PVL: n = 10/37, 27% vs. N = 2/13, 15.4% (p > 0.05) SCCmec type II: n = 16/37, 43.2% vs. N = 7/13, 53.9% (p > 0.05) agr type II: n = 12/37, 40% vs. N = 5/13, 55.6% (p > 0.05) The PVL gene was identified in 44% of USA300 isolates and in none of the non–USA300 isolates |
| Trobos et al., 2022 [29] | Retrospective, single-center | Sweden | 2012–2015 | 38/45 | 3/45 (6.7) | PJI | WGS | Resolved 8 (n = 22) vs. unresolved infection (n = 23) | 3.5–5 years | None of the CC types were associated with the outcome: CC15: n = 4/5, 80% vs. n = 1/5, 20% (p = 0.1399) CC30: n = 2/7, 28.6% vs. N = 5/7, 71.4% (p = 0.2163) CC45: n = 7/12, 58.3% vs. N = 5/12, 41.7% (p = 0.4447) CC8: n = ¼, 25% vs. n = ¾, 75% (p = 0.3167) agr type II strains were significantly associated with a resolved outcome agr type II: n = 8/10, 80% vs. n = 2/10, 20% (p = 0.0256) Only the serine protease gene splE and blaZ were significantly less frequent in S. aureus from resolved than unresolved infections: splE: n = 9/22, 40% vs. n = 16/23, 70% (p ≤ 0.05) blaZ: n = 11/22, 50% vs. n = 21/23, 90% (p ≤ 0.01) |
| Valour et al., 2014 [26] | Retrospective single-center | France | 2011–2012 | 75/75 | 0 | Native septic arthritis, n = 10 (13%) PJI, n = 16 (21.3%) OM, n = 38 (50.7%) Vertebral OM, n = 11 (14.7%) | PCR CC398-specific | CC398 (n = 8) vs. Other clones (n = 67) | ND | Less severe biological inflammatory syndrome 9 with CC398: n = 5/8, 62.5% vs. n = 62/67, 92.5% (p = 0.035) Lower treatment failure 10 rates with CC398: n = 0/8 vs. n = 25/67, 37.3% (p = 0.032) |
| Valour et al., 2015 [36] | Retrospective single-center | France | 2001–2011 | 95/95 | 0 | Arthritis, n = 12 (13%) Non-vertebral OM, n = 12 (13%) Vertebral OM, n = 7 (7%) Foreign body infection, n = 64 (67%) (PJI, n = 29, OM, n = 32, others, n = 3) | DNA microarray 3 | Acute 11 (n = 64) vs. Chronic BJI (n = 31) | No significant difference in distribution of clonal complexes comparing acute and chronic BJI (p = 0.408) No identification of virulence genes associated with BJI chronicity: Multivariate analysis results sdrD: OR (95% CI) = 0.365 (0.128–1.038), p = 0.059 Internalization rate: OR (95% CI) = 1.000 (1.000–1.000), p = 0.244 Delta-toxin negative: OR (95% CI) = 0.397 (0.708–8.112), p = 0.160 | |
| Viquez-Molina 2018 [37] | Prospective single-center | Costa Rica | 2004–2016 | 58 | 35/58 (60.3) | DFI (58/58) OM (41/58) | PCR mecA, lukS-PV, lukF-PV, tsst, etA, etB | Lower extremity amputation vs. no lower extremity amputation | ND | In patients with DFI, the only predictive factor associated with the outcome of lower extremity amputation was the presence of necrosis: OR (95% CI) = 6.6 (1.5–28.4), p = 0.01 mecA+ vs. mecA− n = 13/35, 37% vs. n = 4/23, 17% (p = 0.10) PVL+ vs. PVL− n = 0/4 vs. n = 17/54, 31.5% (p = 0.23) tsst+ vs. tsst− n = 2/3, 67% vs. n = 15/55, 27% (p = 0.20) In 41 patients with OM associated DFI, presence of mecA was not associated with amputation: n = 4/14, 28.6% vs. n = 12/27, 44.4% (p = 0.32) Patient with mecA+ had longer time to wound healing: mecA+ vs. mecA− (days, median [Q1, Q3]): 104 (52, 132) vs. 74 (45, 80) (p = 0.04) |
| Wildeman et al., 2020 [30] | Retrospective multicenter | Sweden | 2004–2016 2012–2016 | 100 | 1/100 (1) | PJI | WGS | Treatment failure 12 49/99 (49%) or no microbiological eradication 13 40/99 (40%) | 26 months (median) | Genes associated with treatment failure (success vs. failure): cap5H: n = 7/50, 14% vs. n = 17/49, 34%, p = 0.02, OR (95% CI) = 2.83 (1.06–7.60) cap5J: n = 7/50, 14% vs. n = 16/49, 32%, p = 0.03, OR (95% CI) = 2.55 (0.95–6.87) cap5K: n = 7/50, 14% vs. n = 16/49, 32%, p = 0.03, OR (95% CI) = 2.55 (0.95–6.87) Genes associated with treatment success: cap8H: n = 23/49, 46% vs. n = 36/50, 72% p = 0.01, OR (95% CI) = 0.38 (0.17–0.87) cap8I: n = 31/49, 62% vs. n = 41/50, 82%, p = 0.02, OR (95% CI) = 0.38 (0.15–0.97) cap8J: n = 32/49, 64% vs. n = 42/50, 84%, p = 0.02, OR (95% CI) = 0.35 (0.13–0.95) cap8K: n = 32/49, 64% vs. n = 42/50, 84%, p = 0.02, OR (95% CI) = 0.32 (0.13–0.81) sspP: n = 44/49, 88% vs. n = 50/50, 100%, p = 0.03 (odds ratio not provided) Genes associated with eradication: cap8H: n = 40/59, 68% vs. n = 18/40, 45%, p = 0.02, OR (95% CI) = 0.39 (0.17–0.90) cap8K: n = 46/59, 78% vs. n = 24/40, 60%, p = 0.05, OR (95% CI) = 0.44 (0.18–1.08) 14 |
3.3.5. Quality of Studies
3.4. Comparison of Initial and Relapse Strains in BJI with Treatment Failure
3.4.1. Studies Included
3.4.2. Analysis of Genetic Differences between First and Recurrent/Relapse Isolates
3.4.3. Quality of Studies
3.5. Discussion
3.5.1. Role of S. aureus Lineage
3.5.2. Role of the agr System
3.5.3. Role of PVL Genes
3.5.4. Role of Other Virulence Genes
3.5.5. Strengths and Weaknesses of the Literature and Perspectives for the Future
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACME | arginine catabolic mobile element |
| AHO | acute hematogenous osteomyelitis |
| BJI | bone and joint infections |
| CC | clonal complex |
| CI | confidence interval |
| CRP | C-reactive protein |
| DAIR | debridement, antibiotics, and implant retention |
| DFI | diabetic foot infection |
| ESR | erythrocyte sedimentation rate |
| ICU | intensive care unit |
| MSCRAMM | microbial surface components recognizing adhesive matrix molecules |
| MSSA | methicillin-susceptible Staphylococcus aureus |
| MRSA | methicillin-resistant Staphylococcus aureus |
| OM | osteomyelitis |
| OR | odds ratio |
| PCR | polymerase chain reaction |
| PFGE | pulsed-field gel electrophoresis |
| PJI | prosthetic joint infection |
| PRISMA | Preferred Reporting Items for Systematic Review and Meta-Analyses |
| PVL | Panton Valentine leucocidin |
| S. aureus | Staphylococcus aureus |
| SCV | small colony variant |
| SSTI | skin and soft tissue infection |
| ST | sequence type |
| VISA | vancomycin-intermediate S. aureus |
| WGS | whole genome sequencing |
References
- Urish, K.L.; Cassat, J.E. Staphylococcus aureus Osteomyelitis: Bone, Bugs, and Surgery. Infect. Immun. 2020, 88, e00932-19. [Google Scholar] [CrossRef] [PubMed]
- Patel, R. Periprosthetic Joint Infection. New Engl. J. Med. 2023, 388, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.A.; Sharma-Kuinkel, B.K.; Maskarinec, S.A.; Eichenberger, E.M.; Shah, P.P.; Carugati, M.; Holland, T.L.; Fowler, V.G. Methicillin-Resistant Staphylococcus aureus: An Overview of Basic and Clinical Research. Nat. Rev. Microbiol. 2019, 17, 203–218. [Google Scholar] [CrossRef]
- Bouiller, K.; Gbaguidi-Haore, H.; Hocquet, D.; Cholley, P.; Bertrand, X.; Chirouze, C. Clonal Complex 398 Methicillin-Susceptible Staphylococcus aureus Bloodstream Infections Are Associated with High Mortality. Clin. Microbiol. Infect. 2016, 22, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Souli, M.; Ruffin, F.; Choi, S.-H.; Park, L.P.; Gao, S.; Lent, N.C.; Sharma-Kuinkel, B.K.; Thaden, J.T.; Maskarinec, S.A.; Wanda, L.; et al. Changing Characteristics of Staphylococcus aureus Bacteremia: Results From a 21-Year, Prospective, Longitudinal Study. Clin. Infect. Dis. 2019, 69, 1868–1877. [Google Scholar] [CrossRef] [PubMed]
- Recker, M.; Laabei, M.; Toleman, M.S.; Reuter, S.; Saunderson, R.B.; Blane, B.; Török, M.E.; Ouadi, K.; Stevens, E.; Yokoyama, M.; et al. Clonal Differences in Staphylococcus aureus Bacteraemia-Associated Mortality. Nat. Microbiol. 2017, 2, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Pimentel de Araujo, F.; Monaco, M.; Del Grosso, M.; Pirolo, M.; Visca, P.; Pantosti, A. Staphylococcus aureus Clones Causing Osteomyelitis: A Literature Review (2000-2020). J. Glob. Antimicrob. Resist. 2021, 26, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Gallego, I.; Mancheño, M.; Pérez-Montarelo, D.; Viedma, E.; Chaves, F.; Lora-Tamayo, J. Staphylococcus aureus Native Arthritis over 10 Years. Médecine Et. Mal. Infect. 2020, 50, 257–262. [Google Scholar] [CrossRef]
- Kok, E.Y.; Vallejo, J.G.; Sommer, L.M.; Rosas, L.; Kaplan, S.L.; Hulten, K.G.; McNeil, J.C. Association of Vancomycin MIC and Molecular Characteristics with Clinical Outcomes in Methicillin-Susceptible Staphylococcus aureus Acute Hematogenous Osteoarticular Infections in Children. Antimicrob Agents Chemother 2018, 62, e00084-18. [Google Scholar] [CrossRef]
- McCaskill, M.L.; Mason, E.O.J.; Kaplan, S.L.; Hammerman, W.; Lamberth, L.B.; Hultén, K.G. Increase of the USA300 Clone Among Community-Acquired Methicillin-Susceptible Staphylococcus aureus Causing Invasive Infections. Pediatr. Infect. Dis. J. 2007, 26, 1122–1127. [Google Scholar] [CrossRef]
- McNeil, J.C.; Sommer, L.M.; Boyle, M.; Hogan, P.; Vallejo, J.G.; Hultén, K.G.; Flores, A.R.; Kaplan, S.L.; Fritz, S. Cefazolin Inoculum Effect and Methicillin-Susceptible Staphylococcus aureus Osteoarticular Infections in Children. Antimicrob Agents Chemother 2020, 64, e00703-20. [Google Scholar] [CrossRef] [PubMed]
- Gaviria-Agudelo, C.; Aroh, C.; Tareen, N.; Wakeland, E.K.; Kim, M.; Copley, L.A. Genomic Heterogeneity of Methicillin Resistant Staphylococcus aureus Associated with Variation in Severity of Illness among Children with Acute Hematogenous Osteomyelitis. PLoS ONE 2015, 10, e0130415. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.; Wakeland, E.K.; Raj, P.; Kim, M.S.; Kim, J.; Tareen, N.G.; Copley, L.A.B. The Impact of Staphylococcus aureus Genomic Variation on Clinical Phenotype of Children with Acute Hematogenous Osteomyelitis. Heliyon 2018, 4, e00674. [Google Scholar] [CrossRef] [PubMed]
- Belthur, M.V.; Birchansky, S.B.; Verdugo, A.A.; Mason, E.O.; Hulten, K.G.; Kaplan, S.L.; Smith, E.O.; Phillips, W.A.; Weinberg, J. Pathologic Fractures in Children with Acute Staphylococcus aureus Osteomyelitis. J. Bone Jt. Surg. Am. 2012, 94, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Bocchini, C.E.; Hulten, K.G.; Mason, E.O.; Gonzalez, B.E.; Hammerman, W.A.; Kaplan, S.L. Panton-Valentine Leukocidin Genes Are Associated with Enhanced Inflammatory Response and Local Disease in Acute Hematogenous Staphylococcus aureus Osteomyelitis in Children. Pediatrics 2006, 117, 433–440. [Google Scholar] [CrossRef]
- Bouras, D.; Doudoulakakis, A.; Tsolia, M.; Vaki, I.; Giormezis, N.; Petropoulou, N.; Lebessi, E.; Gennimata, V.; Tsakris, A.; Spiliopoulou, I.; et al. Staphylococcus aureus Osteoarticular Infections in Children: An 8-Year Review of Molecular Microbiology, Antibiotic Resistance and Clinical Characteristics. J. Med. Microbiol. 2018, 67, 1753–1760. [Google Scholar] [CrossRef]
- Carrillo-Marquez, M.A.; Hulten, K.G.; Hammerman, W.; Mason, E.O.; Kaplan, S.L. USA300 Is the Predominant Genotype Causing Staphylococcus aureus Septic Arthritis in Children. Pediatr. Infect. Dis. J. 2009, 28, 1076–1080. [Google Scholar] [CrossRef]
- Dohin, B.; Gillet, Y.; Kohler, R.; Lina, G.; Vandenesch, F.; Vanhems, P.; Floret, D.; Etienne, J. Pediatric Bone and Joint Infections Caused by Panton-Valentine Leukocidin-Positive Staphylococcus aureus. Pediatr. Infect. Dis. J. 2007, 26, 1042–1048. [Google Scholar] [CrossRef]
- Gijón, M.; Bellusci, M.; Petraitiene, B.; Noguera-Julian, A.; Glikman, D.; Saavedra-Lozano, J.; Neth, O.; Daskalaki, M.; Zilinskaite, V.; Kaiser-Labusch, P.; et al. Pediatric Community-Acquired Bone and Joint Staphylococcus aureus Infections In Europe: Severe Infections Are Associated to Panton-Valentine Leucocidin Presence. Pediatr. Infect. Dis. J. 2020, 39, e73–e76. [Google Scholar] [CrossRef]
- Martínez-Aguilar, G.; Avalos-Mishaan, A.; Hulten, K.; Hammerman, W.; Mason, E.O.J.; Kaplan, S.L. Community-Acquired, Methicillin-Resistant and Methicillin-Susceptible Staphylococcus aureus Musculoskeletal Infections in Children. Pediatr. Infect. Dis. J. 2004, 23, 701–706. [Google Scholar] [CrossRef]
- McNeil, J.C.; Vallejo, J.G.; Kok, E.Y.; Sommer, L.M.; Hultén, K.G.; Kaplan, S.L. Clinical and Microbiologic Variables Predictive of Orthopedic Complications Following Staphylococcus aureus Acute Hematogenous Osteoarticular Infections in Children. Clin. Infect. Dis. 2019, 69, 1955–1961. [Google Scholar] [CrossRef] [PubMed]
- Moutaouakkil, K.; Abdellaoui, H.; Arhoune, B.; Atarraf, K.; El Fakir, S.; Yahyaoui, G.; Mahmoud, M.; Afifi, M.A.; Oumokhtar, B. Paediatric Osteoarticular Infections Caused by Staphylococcus aureus Producing Panton-Valentine Leucocidin in Morocco: Risk Factors and Clinical Features. Afr. J. Paediatr. Surg. 2022, 19, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Sdougkos, G.; Chini, V.; Papanastasiou, D.A.; Christodoulou, G.; Tagaris, G.; Dimitracopoulos, G.; Spiliopoulou, I. Methicillin-Resistant Staphylococcus aureus Producing Panton-Valentine Leukocidin as a Cause of Acute Osteomyelitis in Children. Clin. Microbiol. Infect. 2007, 13, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Wang, Y.; Feng, Z.; Xu, L.; Tan, L.; Zhao, S.; Gong, Y.; Zhang, C.; Luo, X.; Li, S.; et al. Panton-Valentine Leucocidin (PVL) as a Potential Indicator for Prevalence, Duration, and Severity of Staphylococcus aureus Osteomyelitis. Front. Microbiol. 2017, 8, 2355. [Google Scholar] [CrossRef]
- Bouiller, K.; Hocquet, D.; Sauget, M.; Bertrand, X.; Chirouze, C. Epidemiology and Risk Factors of Staphylococcus aureus CC398 Bone and Joint Infections. BMC Infect. Dis. 2020, 20, 384. [Google Scholar] [CrossRef]
- Valour, F.; Tasse, J.; Trouillet-Assant, S.; Rasigade, J.-P.; Lamy, B.; Chanard, E.; Verhoeven, P.; Decousser, J.-W.; Marchandin, H.; Bès, M.; et al. Methicillin-Susceptible Staphylococcus aureus Clonal Complex 398: High Prevalence and Geographical Heterogeneity in Bone and Joint Infection and Nasal Carriage. Clin. Microbiol. Infect. 2014, 20, O772–O775. [Google Scholar] [CrossRef]
- Chen, J.-L.; Huang, T.-Y.; Hsu, W.-B.; Lee, C.-W.; Chiang, Y.-C.; Chang, P.-J.; Peng, K.-T. Characterization of Methicillin-Resistant Staphylococcus aureus Isolates from Periprosthetic Joint Infections. Pathogens 2022, 11, 719. [Google Scholar] [CrossRef]
- Muñoz-Gallego, I.; Viedma, E.; Esteban, J.; Mancheño-Losa, M.; García-Cañete, J.; Blanco-García, A.; Rico, A.; García-Perea, A.; Ruiz Garbajosa, P.; Escudero-Sánchez, R.; et al. Genotypic and Phenotypic Characteristics of Staphylococcus aureus Prosthetic Joint Infections: Insight on the Pathogenesis and Prognosis of a Multicenter Prospective Cohort. Open Forum. Infect. Dis. 2020, 7, ofaa344. [Google Scholar] [CrossRef]
- Trobos, M.; Firdaus, R.; Svensson Malchau, K.; Tillander, J.; Arnellos, D.; Rolfson, O.; Thomsen, P.; Lasa, I. Genomics of Staphylococcus aureus and Staphylococcus epidermidis from Periprosthetic Joint Infections and Correlation to Clinical Outcome. Microbiol. Spectr. 2022, 10, e02181-21. [Google Scholar] [CrossRef]
- Wildeman, P.; Tevell, S.; Eriksson, C.; Lagos, A.C.; Söderquist, B.; Stenmark, B. Genomic Characterization and Outcome of Prosthetic Joint Infections Caused by Staphylococcus aureus. Sci. Rep. 2020, 10, 5938. [Google Scholar] [CrossRef]
- Kalinka, J.; Hachmeister, M.; Geraci, J.; Sordelli, D.; Hansen, U.; Niemann, S.; Oetermann, S.; Peters, G.; Löffler, B.; Tuchscherr, L. Staphylococcus aureus Isolates from Chronic Osteomyelitis Are Characterized by High Host Cell Invasion and Intracellular Adaptation, but Still Induce Inflammation. Int. J. Med. Microbiol. 2014, 304, 1038–1049. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Gallego, I.; Lora-Tamayo, J.; Pérez-Montarelo, D.; Brañas, P.; Viedma, E.; Chaves, F. Influence of Molecular Characteristics in the Prognosis of Methicillin-Resistant Staphylococcus aureus Prosthetic Joint Infections: Beyond the Species and the Antibiogram. Infection 2017, 45, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Gallego, I.; Meléndez-Carmona, M.Á.; Lora-Tamayo, J.; Garrido-Allepuz, C.; Chaves, F.; Sebastián, V.; Viedma, E. Microbiological and Molecular Features Associated with Persistent and Relapsing Staphylococcus aureus Prosthetic Joint Infection. Antibiotics 2022, 11, 1119. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, B.; Shaw, T.; Mukhopadhyay, C.; Bhat, N.S.; Singh, B.M.K. Epidemiology, Resistance Characteristics, Virulence Determinants, and Treatment Outcomes of Staphylococcus aureus Bone and Joint Infections: A One-Year Prospective Study at a Tertiary Care Hospital in India. Pathog. Glob. Health 2020, 114, 482–486. [Google Scholar] [CrossRef]
- Peyrani, P.; Allen, M.; Seligson, D.; Roberts, C.; Chen, A.; Haque, N.; Zervos, M.; Wiemken, T.; Harting, J.; Christensen, D.; et al. Clinical Outcomes of Osteomyelitis Patients Infected with Methicillin-Resistant Staphylococcus aureus USA-300 Strains. Am. J. Orthop. (Belle Mead NJ) 2012, 41, 117–122. [Google Scholar]
- Valour, F.; Rasigade, J.-P.; Trouillet-Assant, S.; Gagnaire, J.; Bouaziz, A.; Karsenty, J.; Lacour, C.; Bes, M.; Lustig, S.; Bénet, T.; et al. Delta-Toxin Production Deficiency in Staphylococcus aureus: A Diagnostic Marker of Bone and Joint Infection Chronicity Linked with Osteoblast Invasion and Biofilm Formation. Clin. Microbiol. Infect. 2015, 21, 568.e1-11. [Google Scholar] [CrossRef]
- Víquez-Molina, G.; Aragón-Sánchez, J.; Pérez-Corrales, C.; Murillo-Vargas, C.; López-Valverde, M.E.; Lipsky, B.A. Virulence Factor Genes in Staphylococcus aureus Isolated From Diabetic Foot Soft Tissue and Bone Infections. Int. J. Low Extrem. Wounds 2018, 17, 36–41. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Tsai, J.-C.; Yamamoto, T.; Chen, H.-J.; Hung, W.-C.; Hsueh, P.-R.; Teng, L.-J. Emergence of a Small Colony Variant of Vancomycin-Intermediate Staphylococcus aureus in a Patient with Septic Arthritis during Long-Term Treatment with Daptomycin. J. Antimicrob. Chemother. 2016, 71, 1807–1814. [Google Scholar] [CrossRef]
- Cafiso, V.; Lo Verde, F.; Zega, A.; Pigola, G.; Rostagno, R.; Borrè, S.; Stefani, S. Genomic Characterization of a New Biofilm-Forming and Adhesive ST398 Human-Adapted MSSA Lineage Causing Septic Knee Arthritis Following Surgical Reconstruction. Microorganisms 2021, 9, 305. [Google Scholar] [CrossRef]
- Loss, G.; Simões, P.M.; Valour, F.; Cortês, M.F.; Gonzaga, L.; Bergot, M.; Trouillet-Assant, S.; Josse, J.; Diot, A.; Ricci, E.; et al. Staphylococcus aureus Small Colony Variants (SCVs): News From a Chronic Prosthetic Joint Infection. Front. Cell Infect. Microbiol. 2019, 9, 363. [Google Scholar] [CrossRef]
- Ma, D.; Brothers, K.M.; Maher, P.L.; Phillips, N.J.; Simonetti, D.; William Pasculle, A.; Richardson, A.R.; Cooper, V.S.; Urish, K.L. Staphylococcus aureus Genotype Variation among and within Periprosthetic Joint Infections. J. Orthop. Res. 2022, 40, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Trouillet-Assant, S.; Lelièvre, L.; Martins-Simões, P.; Gonzaga, L.; Tasse, J.; Valour, F.; Rasigade, J.-P.; Vandenesch, F.; Muniz Guedes, R.L.; Ribeiro de Vasconcelos, A.T.; et al. Adaptive Processes of Staphylococcus aureus Isolates during the Progression from Acute to Chronic Bone and Joint Infections in Patients. Cell Microbiol. 2016, 18, 1405–1414. [Google Scholar] [CrossRef] [PubMed]
- David, M.Z.; Daum, R.S. Community-Associated Methicillin-Resistant Staphylococcus aureus: Epidemiology and Clinical Consequences of an Emerging Epidemic. Clin. Microbiol. Rev. 2010, 23, 616–687. [Google Scholar] [CrossRef] [PubMed]
- Gustave, C.-A.; Tristan, A.; Martins-Simões, P.; Stegger, M.; Benito, Y.; Andersen, P.S.; Bes, M.; Le Hir, T.; Diep, B.A.; Uhlemann, A.-C.; et al. Demographic Fluctuation of Community-Acquired Antibiotic-Resistant Staphylococcus aureus Lineages: Potential Role of Flimsy Antibiotic Exposure. ISME J. 2018, 12, 1879–1894. [Google Scholar] [CrossRef] [PubMed]
- Eichenberger, E.M.; Ruffin, F.; Sharma-Kuinkel, B.; Dagher, M.; Park, L.; Kohler, C.; Sinclair, M.R.; Maskarinec, S.A.; Fowler Jr, V.G. Bacterial Genotype and Clinical Outcomes in Solid Organ Transplant Recipients with Staphylococcus aureus Bacteremia. Transplant. Infect. Dis. 2021, 23, e13730. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Hamid, M.I.; Sewid, A.H.; Samir, M.; Hegazy, W.A.H.; Bahnass, M.M.; Mosbah, R.A.; Ghaith, D.M.; Khalifa, E.; Ramadan, H.; Alshareef, W.A.; et al. Clonal Diversity and Epidemiological Characteristics of ST239-MRSA Strains. Front. Cell Infect. Microbiol. 2022, 12, 782045. [Google Scholar] [CrossRef] [PubMed]
- Le, K.Y.; Otto, M. Quorum-Sensing Regulation in Staphylococci—An Overview. Front. Microbiol. 2015, 6, 1174. [Google Scholar] [CrossRef] [PubMed]
- Painter, K.L.; Krishna, A.; Wigneshweraraj, S.; Edwards, A.M. What Role Does the Quorum-Sensing Accessory Gene Regulator System Play during Staphylococcus aureus Bacteremia? Trends Microbiol. 2014, 22, 676–685. [Google Scholar] [CrossRef]
- Lee, S.O.; Lee, S.; Lee, J.E.; Song, K.-H.; Kang, C.K.; Wi, Y.M.; San-Juan, R.; López-Cortés, L.E.; Lacoma, A.; Prat, C.; et al. Dysfunctional Accessory Gene Regulator (Agr) as a Prognostic Factor in Invasive Staphylococcus aureus Infection: A Systematic Review and Meta-Analysis. Sci. Rep. 2020, 10, 20697. [Google Scholar] [CrossRef]
- Sakoulas, G.; Eliopoulos, G.M.; Moellering, R.C.; Wennersten, C.; Venkataraman, L.; Novick, R.P.; Gold, H.S. Accessory Gene Regulator (Agr) Locus in Geographically Diverse Staphylococcus aureus Isolates with Reduced Susceptibility to Vancomycin. Antimicrob Agents Chemother 2002, 46, 1492–1502. [Google Scholar] [CrossRef]
- Gagnaire, J.; Dauwalder, O.; Boisset, S.; Khau, D.; Freydière, A.-M.; Ader, F.; Bes, M.; Lina, G.; Tristan, A.; Reverdy, M.-E.; et al. Detection of Staphylococcus aureus Delta-Toxin Production by Whole-Cell MALDI-TOF Mass Spectrometry. PLoS ONE 2012, 7, e40660. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, J.; Kamio, Y. Bacterial Two-Component and Hetero-Heptameric Pore-Forming Cytolytic Toxins: Structures, Pore-Forming Mechanism, and Organization of the Genes. Biosci. Biotechnol. Biochem. 2004, 68, 981–1003. [Google Scholar] [CrossRef] [PubMed]
- Shallcross, L.J.; Fragaszy, E.; Johnson, A.M.; Hayward, A.C. The Role of the Panton-Valentine Leucocidin Toxin in Staphylococcal Disease: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2013, 13, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Lina, G.; Piémont, Y.; Godail-Gamot, F.; Bes, M.; Peter, M.O.; Gauduchon, V.; Vandenesch, F.; Etienne, J. Involvement of Panton-Valentine Leukocidin-Producing Staphylococcus aureus in Primary Skin Infections and Pneumonia. Clin. Infect. Dis. 1999, 29, 1128–1132. [Google Scholar] [CrossRef]
- Petraitiene, B.; Conejo, P.R.; Jankauskaite, L.; Kevalas, R.; Trumpulyte, G.; Snipaitiene, A.; Vitkauskiene, A.; Gurskis, V. Prevalence, Clinical Expression, Invasiveness and Outcome of Staphylococcus aureus Containing Panton-Valentine Leukocidin in Children Treated in a University Hospital of Lithuania. Infect. Dis. (Lond) 2020, 52, 464–472. [Google Scholar] [CrossRef]
- Gillet, Y.; Tristan, A.; Rasigade, J.-P.; Saadatian-Elahi, M.; Bouchiat, C.; Bes, M.; Dumitrescu, O.; Leloire, M.; Dupieux, C.; Laurent, F.; et al. Prognostic Factors of Severe Community-Acquired Staphylococcal Pneumonia in France. Eur. Respir. J. 2021, 58, 2004445. [Google Scholar] [CrossRef]
- Campo, M.; Hachem, R.; Jiang, Y.; Dvorak, T.; Carrillo-Marquez, M.; Hulten, K.; Chemaly, R.F.; Raad, I. Panton Valentine Leukocidin Exotoxin Has No Effect on the Outcome of Cancer Patients with Methicillin-Resistant Staphylococcus aureus (MRSA) Infections. Med. (Baltim) 2011, 90, 312–318. [Google Scholar] [CrossRef]
- Aamot, H.V.; Blomfeldt, A.; Eskesen, A.N. Genotyping of 353 Staphylococcus aureus Bloodstream Isolates Collected between 2004 and 2009 at a Norwegian University Hospital and Potential Associations with Clinical Parameters. J. Clin. Microbiol. 2012, 50, 3111–3114. [Google Scholar] [CrossRef]
- Wang, J.-L.; Wang, J.-T.; Chen, S.-Y.; Hsueh, P.-R.; Kung, H.-C.; Chen, Y.-C.; Chang, S.-C. Adult Methicillin-Resistant Staphylococcus aureus Bacteremia in Taiwan: Clinical Significance of Non-Multi-Resistant Antibiogram and Panton-Valentine Leukocidin Gene. Diagn Microbiol. Infect. Dis 2007, 59, 365–371. [Google Scholar] [CrossRef]
- Qu, M.D.; Kausar, H.; Smith, S.; Lazar, P.G.; Kroll-Desrosiers, A.R.; Iii, C.H.; Barton, B.A.; Ward, D.V.; Iii, R.T.E. Epidemiological and Clinical Features of Panton-Valentine Leukocidin Positive Staphylococcus aureus Bacteremia: A Case-Control Study. PLoS ONE 2022, 17, e0265476. [Google Scholar] [CrossRef]
- Campbell, A.J.; Mowlaboccus, S.; Coombs, G.W.; Daley, D.A.; Al Yazidi, L.S.; Phuong, L.K.; Leung, C.; Best, E.J.; Webb, R.H.; Voss, L.; et al. Whole Genome Sequencing and Molecular Epidemiology of Paediatric Staphylococcus aureus Bacteraemia. J. Glob. Antimicrob. Resist. 2022, 29, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Nero, T.; Mukherjee, S.; Olson, R.; Yan, J. Searching for the Secret of Stickiness: How Biofilms Adhere to Surfaces. Front. Microbiol. 2021, 12, 686793. [Google Scholar] [CrossRef] [PubMed]
- Lattar, S.M.; Tuchscherr, L.P.N.; Centrón, D.; Becker, K.; Predari, S.C.; Buzzola, F.R.; Robinson, D.A.; Sordelli, D.O. Molecular Fingerprinting of Staphylococcus aureus Isolated from Patients with Osteomyelitis in Argentina and Clonal Distribution of the Cap5(8) Genes and of Other Selected Virulence Genes. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 2559–2566. [Google Scholar] [CrossRef] [PubMed]
- Lattar, S.M.; Tuchscherr, L.P.N.; Caccuri, R.L.; Centrón, D.; Becker, K.; Alonso, C.A.; Barberis, C.; Miranda, G.; Buzzola, F.R.; von Eiff, C.; et al. Capsule Expression and Genotypic Differences among Staphylococcus aureus Isolates from Patients with Chronic or Acute Osteomyelitis. Infect. Immun. 2009, 77, 1968–1975. [Google Scholar] [CrossRef]
- Boyle-Vavra, S.; Li, X.; Alam, M.T.; Read, T.D.; Sieth, J.; Cywes-Bentley, C.; Dobbins, G.; David, M.Z.; Kumar, N.; Eells, S.J.; et al. USA300 and USA500 Clonal Lineages of Staphylococcus aureus Do Not Produce a Capsular Polysaccharide Due to Conserved Mutations in the Cap5 Locus. mBio 2015, 6, e02585-14. [Google Scholar] [CrossRef]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success after Treatment of Periprosthetic Joint Infection: A Delphi-Based International Multidisciplinary Consensus. Clin. Orthop. Relat. Res. 2013, 471, 2374–2382. [Google Scholar] [CrossRef]
| Reference | Study Design | Country | Years of Study | Number of Patients/Strains | MRSA n, (%) | Type of BJI | Genomic Analysis | Groups Compared | Genotype and Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Belthur et al., 2012 [14] | Retrospective, single-center | USA | 2001–2009 | 66/66 | 58/66 (88) | AHO | PFGE, PCR PVL gene (unspecified) | Bone fracture (n = 17) vs. no bone fracture (n = 49) | Prevalence of PVL and USA300 clone did not differ significantly PVL: n = 17/17, 100% vs. n = 45/49, 92% (p = 0.565) USA300 pulsotype: n = 16/17, 94% vs. n = 43/49, 88% (p = 0.667) The USA300-0114 clone was more frequent with a fracture: n = 14/17, 82% vs. n = 27/49, 55% (p = 0.034) |
| Bocchini et al., 2006 [15] | Retrospective, single-center | USA | 2001–2004 | 89/89 | 56/89 (85) | AHO | PCR luk-S-PV, luk-F-PV, fnbB | PVL+ (n = 59) vs. PVL- (n = 26) fnbB+ (n = 66) vs. fnbB- (n = 10) | PVL+/PVL- Severe infection that required care in the ICU: n = 11/59, 18.6% vs. n = 1/26, 3.8% (p = 0.01) Higher CRP levels (mg/L, mean ± SD): 23.1 ± 18.1 vs. 7.1 ± 7.1 (p = 0.000002) Higher WBC count (cells x 103/mm3, mean ± SD): 15.1 ± 6.6 vs. 11.6 ± 6.4 (p = 0.03) Positive blood culture: n = 39/58, 67.2% vs. n = 5/26, 19.2% (p = 0.0001) Surrounding myositis/pyomyositis on MRI: n = 28/45, 62.2% vs. n = 6/19, 31.6% (p = 0.05) Subperiosteal/intraosseal abscess on MRI: n = 34/45, 75.6% vs. n = 9/19, 47.4% (p = 0.06) fnbB+/fnbB− No significant differences |
| Bouras et al., 2018 [16] | Retrospective, two centers | Greece | 2007–2015 | 125/68 | 26/68 (38.2) | OM (n = 72) septic arthritis (n = 45) Both (n = 6) | PCR luk-S-PV, luk-F-PV, cna, fib, clfA, clfB, fnBPA, fnBPB, bbp, eno and ebpS PCR agr and SCCmec | Presence of virulence genes or not | No differences except for a correlation of PVL positivity with greater number of days of hospitalization (mean ± SD) (PVL+ vs. PVL−: 19.94 ± 7.61 vs. 14.47 ± 5.11 days [p = 0.002]) |
| Carrillo-Marquez et al., 2009 [17] | Retrospective, single-center | USA | 2001–2008 | 44/44 | 17/44 (38) | Septic arthritis | PCR lukS-PV and lukFPV | PVL+ (n = 27) vs. PVL− (n = 17) | More associated cellulitis/abscess with PVL+: n = 8/27, 30% vs. 0% (p = 0.02) Initial CRP > 10 mg/L: n = 8/22, 36% vs. n = 1/16, 7% (p = 0.05) |
| Collins et al., 2018 [13] | Retrospective, single-center | USA | 2009–2014 | 70/70 | 43/70 (61) | AHO | WGS (201 virulence genes tested) | Severe 1 (n = 36) vs. non-severe (n = 33) | 40 genes were significantly associated with increased severity of illness of the affected children (p < 0.01) Enterotoxins: seg, sek, sei, seq, sem, sen, seo Exotoxins: set13, set11, ssl11nm, set7, set14, ssl6nm, set15, set12 Adhesin: cna Hemolysin: hla Toxins: lukS-PV, lukF-PV, lukE Proteases: splA, splB Others: capE, sarU, ccra, lpl1, agrC, epiC, ear, lpl4, hsdM, sarH2, pls, cadA, spa, bbp, speG, lpl11, fhuD, epiB MRSA isolates encoded a significantly greater number of virulence genes (p < 0.0001) than did MSSA isolates |
| Dohin et al., 2007 [18] | Retrospective, single-center | France | ND | 31/31 | 2/31 (6.5) | AHO (n = 18) Septic arthritis (n = 11) Both (n = 2) | PCR lukS-PV-lukF-PV | PVL+ (n = 14) vs. PVL− (n = 17) | More severe sepsis or septic shock with PVL+: n = 6/14, 43% vs. n = 0/17 (p = 0.004) More days of fever with PVL+ (mean ± SD): 28.6 ± 23.2 vs. 2.8 ± 2.2 (p < 0.001) More complications with PVL+: Muscle abscess: n = 3/14, 21% vs. 0/17 (p = 0.08) Pyomyositis: n = 5/14, 36% vs. 0/17 (p = 0.01) Subperiosteal abscess: n = 11/14, 79% vs. n = 1/17, 6% (p < 0.001) Visceral abscess: n = 11/14, 79% vs. 0/17 (p = 0.012) Deep venous thrombosis: n = 3/14, 21% vs. n = 0/17 (p = 0.08) |
| Gaviria-Agudelo et al., 2015 [12] | Prospective, single-center | USA | ND | 12/12 | 12/12 (100) | AHO | WGS (68 virulence genes tested) | Severe 1 (n = 8) vs. non-severe (n = 4) | Univariate analysis did not identify any virulence gene or SNP associated with severity sek + ear genes combination were more frequent in severe infection: n = 4/8, 50% vs. n = 0/4 (p = 0.208) |
| Gijon et al., 2020 [19] | Prospective, multicenter | Europe | 2012–2014 | 85/85 | 5/85 (6) | OM (n = 62) Septic arthritis (n = 21) Pyomyositis (n = 2) | PCR lukS-PV lukF-PV, mecA | Severe (ICU or death) (n = 11) vs. non-severe (n = 74) | The multivariate analysis identified PVL genes carriage as the only factor independently associated with severe outcomes aOR (95% CI): 12.5 (1.75–89) (p = 0.01) |
| Kok et al., 2018 [9] | Retrospective, single-center | USA | 2011–2016 | 183/183 | 0 | AHO and septic arthritis | PCR lukS-PV, lukF-PV and agr | ICU (n = 11) vs. Non-ICU (n = 172) | In univariate analysis, ICU admission was more often associated with: Bone abscesses: n = 7/11, 63.6% vs. n = 67/172, 39% (p = 0.1) USA300 pulsotype: n = 6/11, 54.5% vs. n = 42/172, 24.4% (p = 0.04) PVL-positive: n = 7/11, 63.6% vs. n = 36/172, 20.9% (p = 0.004) Vancomycin MIC ≥ 2 ug/mL: n = 2/11, 18.1% vs. n = 5/172, 2.9% (p = 0.059) In multivariable analysis, only vancomycin MIC was significantly associated with ICU admission (p = 0.049; OR [95% CI] = 7.85 [1.01–61.6]) |
| Martinez-Aguilar et al., 2004 [20] | Retrospective, single-center | USA | 2000–2002 | 59/59 | 31/59 (52.5) | OM (n = 48) Septic arthritis (n = 6) Pyomyositis (n = 5) | PCR clfA, cna, fnbB, mecA, lukS-PV, lukF-PV and tst | PVL+ (n = 33) vs. PVL− (n = 23) | More complicated infection 2: n = 10/33, 30% vs. n = 0/23 (p = 0.002) More febrile days (mean±SD): 4.2 ± 3.6 vs. 2.1 ± 2.5 (p = 0.017) No other virulence genes were associated with complications |
| McCaskill et al., 2007 [10] | Prospective, single-center | USA | 2001–2006 | 72/72 | 0 | OM | PFGE, PCR PVL genes (unspecified genes) | USA300 (n = 20) vs. Others (n = 52) PVL+ (n = 18) vs. PVL− (n = 54) | Patients with USA300 isolates infection had greater ESR values at presentation (p = 0.03), and maximum ESR values (p = 0.01) than the children with non-USA300 isolates Children infected with a PVL+ isolate had significantly increased values for ESR (p = 0.005) and absolute neutrophil count (p = 0.04) at presentation and maximum ESR (p = 0.002) and CRP (p = 0.04) compared to infection with a PVL− isolate |
| McNeil et al., 2019 [21] | Retrospective, single-center | USA | 2011–2017 | 286/286 | 79/286 (27.6) | AHO (n = 160) Septic arthritis (n = 96) Both (n = 30) | PCR lukS-PV, lukF-PV and agr | Orthopedic complications 3 (n = 27) vs. no orthopedic complications (n = 259) | Univariate analysis: PVL+: n = 14/27, 51.8% vs. n = 101/259, 38.9% (p = 0.21) and USA300 pulsotype: n = 13/27, 48.1% vs. n = 113/259, 43.6% (p = 0.69) were not significantly different and were not included in the multivariable analysis Multivariable logistic regression model for orthopedic complications: agr III: n = 6/27, 22.2% vs. n = 23/259, 8.8% (p = 0.007, OR [95% CI] = 5.05 [1.56–16.31]) Prolonged fever: n = 13/27, 48.1% vs. n = 58/259, 22.4% (p = 0.04, OR [95% CI] = 1.9 [1.79–5.51]) Delayed source control: n = 7/27, 25.9% vs. n = 21/259, 6.5% (p = 0.002, OR [95% CI] = 5.91 [1.95–17.88]) |
| McNeil et al., 2020 [11] | Retrospective, two centers | USA | 2011–2018 | 250/250 | 0 | Isolated AHO (n = 162) AHO and septic arthritis (n = 88) | PCR lukS-PV, lukF-PV and agr (n = 250) | Progression to chronic 4 OM (n = 13) vs. no progression to chronic OM (n = 237) | In multivariable analyses, associations between progression to chronic osteomyelitis and: Multiple surgical debridement n = 7/13, 53.8% vs. n = 38/237, 15.8% (p = 0.01, aOR [95% CI] = 6.99 [1.58–31.1]) Delayed source control n = 4/13, 30.7% vs. n = 22/237, 9.2% (p = 0.03, aOR [95% CI] = 2.59 [1.16–11.11]) agrIII n = 4/13, 30.7% vs. n = 36/237, 15.2% (p = 0.04, aOR [95% CI] = 1.71 [1.03–7.81]) CzIE n = 5/13, 38.5% vs. n = 31/237, 13.1% (p = 0.03, aOR [95% CI] = 13.4 [1.1–18.21]) When CzIE alone was substituted with CzIE and 1GC treatment, no association with chronic osteomyelitis (p = 0.3) PVL was not associated with chronic infection in univariate analysis n = 5/13, 38.5% vs. n = 47/237, 19.8% (p = 0.15) |
| Moutaouakkil et al., 2022 [22] | Prospective, single-center | Morocco | 2017–2018 | 37/37 | 1/37 (2.7) | septic arthritis (n = 14) OM (n = 16) Multifocal abscess (n = 7) | Multiplex PCR assay (luk-S/F-PV and mecA) | PVL+ (n = 17) vs. PVL- (n = 20) | No significant difference on laboratory data: CRP on admission (mg/L, mean ± SD): 170.2 ± 129.9 vs. 164.5 ± 112.8 (p = 0.749) Abnormal X-ray was significantly associated with PVL+ patients: n = 6/17, 35.3% vs. n = 1/20, 5% (p = 0.029) An abnormal ultrasound was not associated with PVL+: n = 14/17, 82.4% vs. n = 11/20, 57.9% (p = 0.219) Repeated surgical procedure was not associated with PVL+: n = 6/17, 35.3% vs. n = 3/20, 15.8% (p = 0.177) |
| Sdougkos et al., 2007 [23] | Retrospective, two centers | Greece | 2005–2006 | 19/19 | 5/19 (26) | AHO | PCR lukS-PV and lukF-PV | PVL+ (n = 7) vs. PVL− (n = 12) | Maximum ESR (mean ± SD): 108 ± 16 vs. 70 ± 15 (p = 0.0011) Days until ESR ormalization (mean ± SD): 27.0 ± 3.9 vs. 17.3±6.9 (p = 0.006) Maximal CRP, mg⁄dL (mean ± SD): 18.3 ± 8.0 vs. 7.9 ± 4.9 (p = 0.0023) Days until CRP normalization (mean ± SD): 17.1 ± 7.9 vs. 8.3 ± 3.7 (p = 0.0078) |
| Reference | Study Design | Country | Years of Study | Population | Number of Patients/Strains | MRSA n, (%) | Type of BJI | Genomic Analysis | Comparison | Interval between First and Second Strain | Genotype and Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lin et al., 2016 [38] | Case report | Taiwan | 2010 | Adult | 1/5 | 3/5 | Native septic arthritis | WGS | First and persistent (SCV) | 6, 10, 37, 41 days | 13 genetic differences: deletion of the entire SCCmecIII, three additional insertions of IS256, 8 point mutations (3 non-coding regions; fabF, fatty acid synthase; mprF, lysyl-phosphatidylglycerol synthase; clpX, ATP-dependent clp protease; and two different mutations of cls2, cardiolipin synthase); and a single nucleotide insertion (seq, enterotoxin). Mutation of the fabF gene (encodes a fatty acid synthase) was probably responsible for the SCV phenotype of recurrent strains |
| Cafiso et al., 2021 [39] | Case report | Italy | ND | Adult | 1/2 | 0 | Native knee septic arthritis and tibial osteomyelitis | WGS | First and persistent | 20 days | No difference in virulence genes No difference in resistance genotype or phenotype In WGS only one SNP differed between 2 strains |
| Loss et al., 2019 [40] | Case report | France | ND | Adults | 1/2 | 0 | PJI | WGS | First and relapse (SCV) | 2 years | A striking difference between the index and relapse-SCV isolates was the loss of a ∼42.5 kb prophage in the genome of the stable relapse-SCV strain (φSa2) Only 5 SNPs identified, of which 2 were intergenic and 3 were intragenic, with only 1 introducing a nonsynonymous mutation Small INDELs (1 bp) inducing truncated proteins, due to a frameshift change in sasA (encodes SasA protein, associated with binding of platelets) and in glpD (encodes aerobic glycerol-3-phosphate dehydrogenase protein) Deletions leading to the emergence of truncated protein forms for an alpha-beta hydrolase (9 bp INDEL) and a putative serine protease (6 bp INDEL) A 9 bp (3 aa, LysGlyPro488−490) non-truncating deletion within the rpoB gene |
| Ma et al., 2022 [41] | Prospective single-center | USA | ND | Adults | 3/13 | ND | PJI | WGS | First and relapse (n = 1), first and recurrent (n = 2) | ND | Mutations in genes coding for proteins involved in fibronectin binding (ebh, fnbA, clfA and clfB) systematically distinguished later PJI isolates from the first PJI isolate from each patient Pairwise differences between isolates from the same patient differed by 0–9 SNPs or small insertion-deletion mutations, whereas comparisons from isolates between patients differed by more than 100 mutations Patient 1: fnb x3, clfB Patient 2: ebh, lysostaphin, epimerase, pheromone binding Patient 3: clf x2, ebH x5, indole 3 pyruvate |
| Trouillet-Assant et al., 2016 [42] | Retrospective single-center | France | ND | Adults | 3/6 | 0 | Osteosynthesis material (n = 1) PJI (n = 2) | WGS | First (n = 3) vs. relapse (n = 3) | 82, 204, 134 days | The genome sizes with the pairs were nearly identical with the exception of one isolate, in which a plasmid was lost in the relapse isolate. Totals of nine, eight and six variants (SNPs and/or INDELs), respectively, were identified, differentiating the pairs obtained from three patients Only a small number of these variants occurred in coding DNA sequences. No effects on the major regulatory systems that are known to control the expression of virulence in S. aureus |
| Muñoz-Gallego et al., 2022 [33] | Prospective multicenter | Spain | 2016–2017 | Adults | 6/12 | 2/12 (17) | PJI with DAIR (symptoms < 21 days) | WGS | First (n = 3) vs. second samples (relapse [n = 3] or persistent [n = 3]) | 144, 78, 25 days for persistent strains, ND for relapse strains | In all cases except one different variants of virulence genes were reported differentiating strain pairs in relapsing and persistent PJIs: bbp, sdrD, clfA, fnbA and fnbB for 2 patients fmt (encodes methionyl-tRNA formyltransferase protein) for one patient Deletion in DNA-3-methyladenine glycosylase in one patient Other mutations in 2 patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bouiller, K.; David, M.Z. Staphylococcus aureus Genomic Analysis and Outcomes in Patients with Bone and Joint Infections: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 3234. https://doi.org/10.3390/ijms24043234
Bouiller K, David MZ. Staphylococcus aureus Genomic Analysis and Outcomes in Patients with Bone and Joint Infections: A Systematic Review. International Journal of Molecular Sciences. 2023; 24(4):3234. https://doi.org/10.3390/ijms24043234
Chicago/Turabian StyleBouiller, Kevin, and Michael Z. David. 2023. "Staphylococcus aureus Genomic Analysis and Outcomes in Patients with Bone and Joint Infections: A Systematic Review" International Journal of Molecular Sciences 24, no. 4: 3234. https://doi.org/10.3390/ijms24043234
APA StyleBouiller, K., & David, M. Z. (2023). Staphylococcus aureus Genomic Analysis and Outcomes in Patients with Bone and Joint Infections: A Systematic Review. International Journal of Molecular Sciences, 24(4), 3234. https://doi.org/10.3390/ijms24043234