
Exploring Biosignals for Quantitative Pain Assessment in Cancer Patients: A Proof of Concept

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
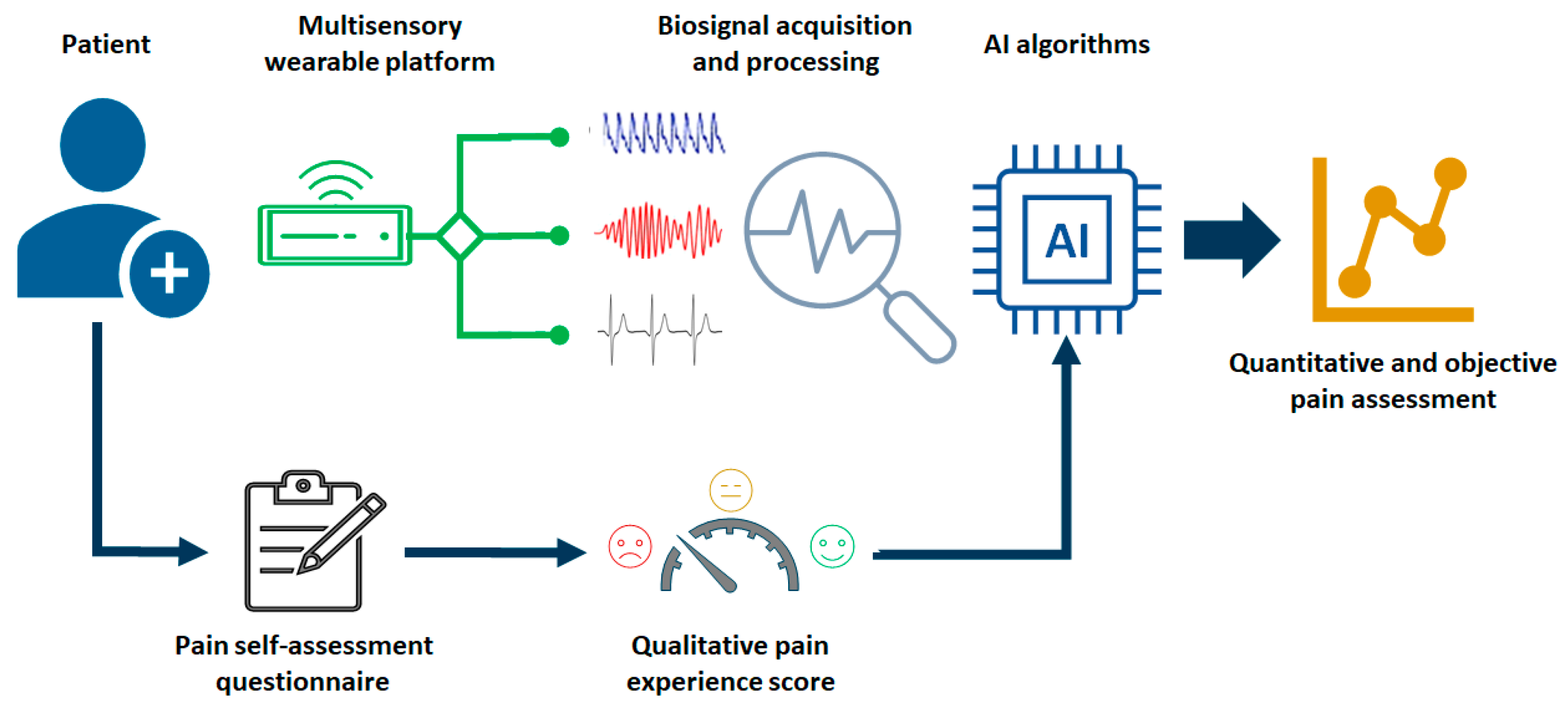
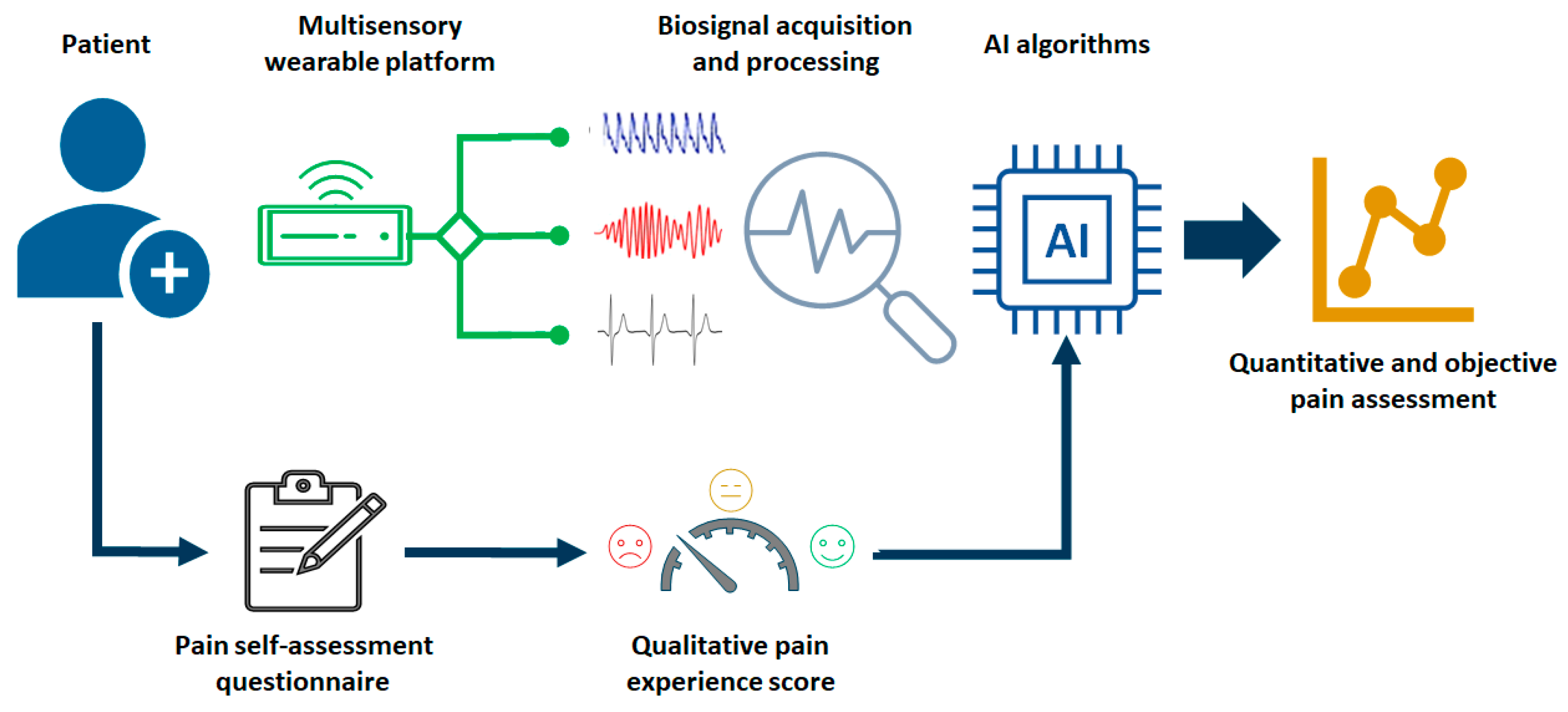
2.1. Framework for Quantitative Cancer Pain Assessment
2.2. Context and Data Collection
2.3. Approach for Qualitative Pain Assessment
2.4. Approach for Quantitative Pain Assessment
- -
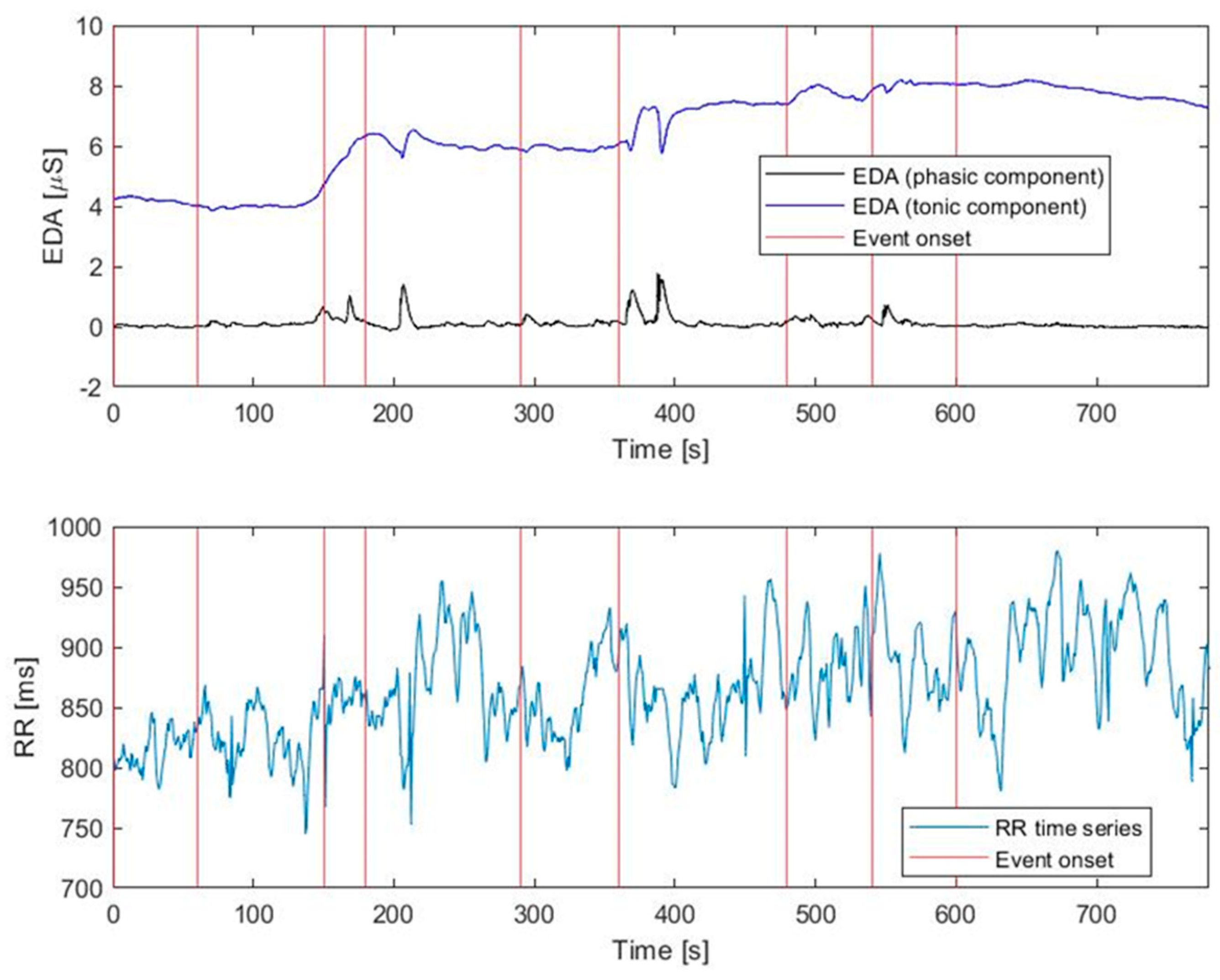
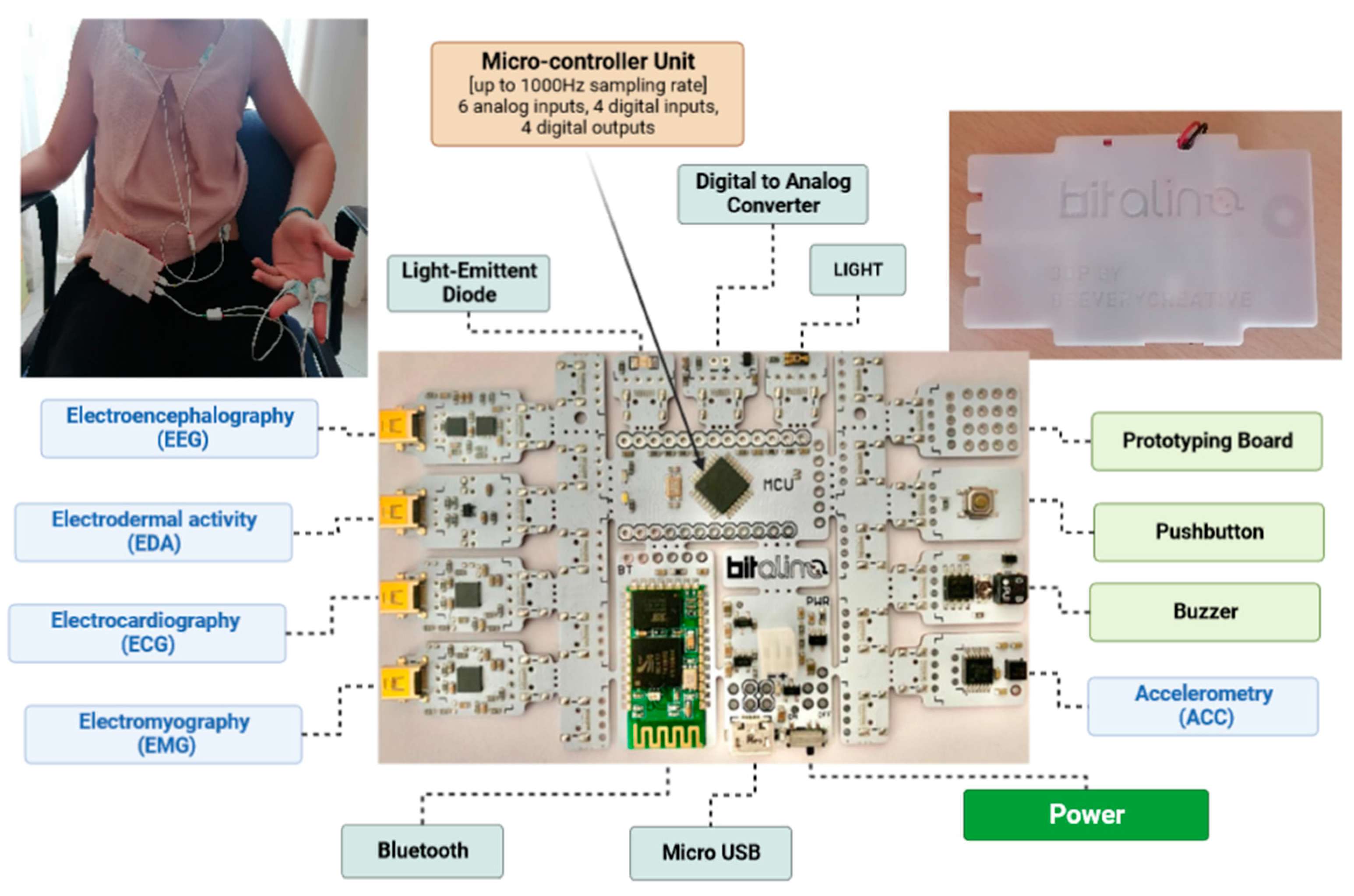
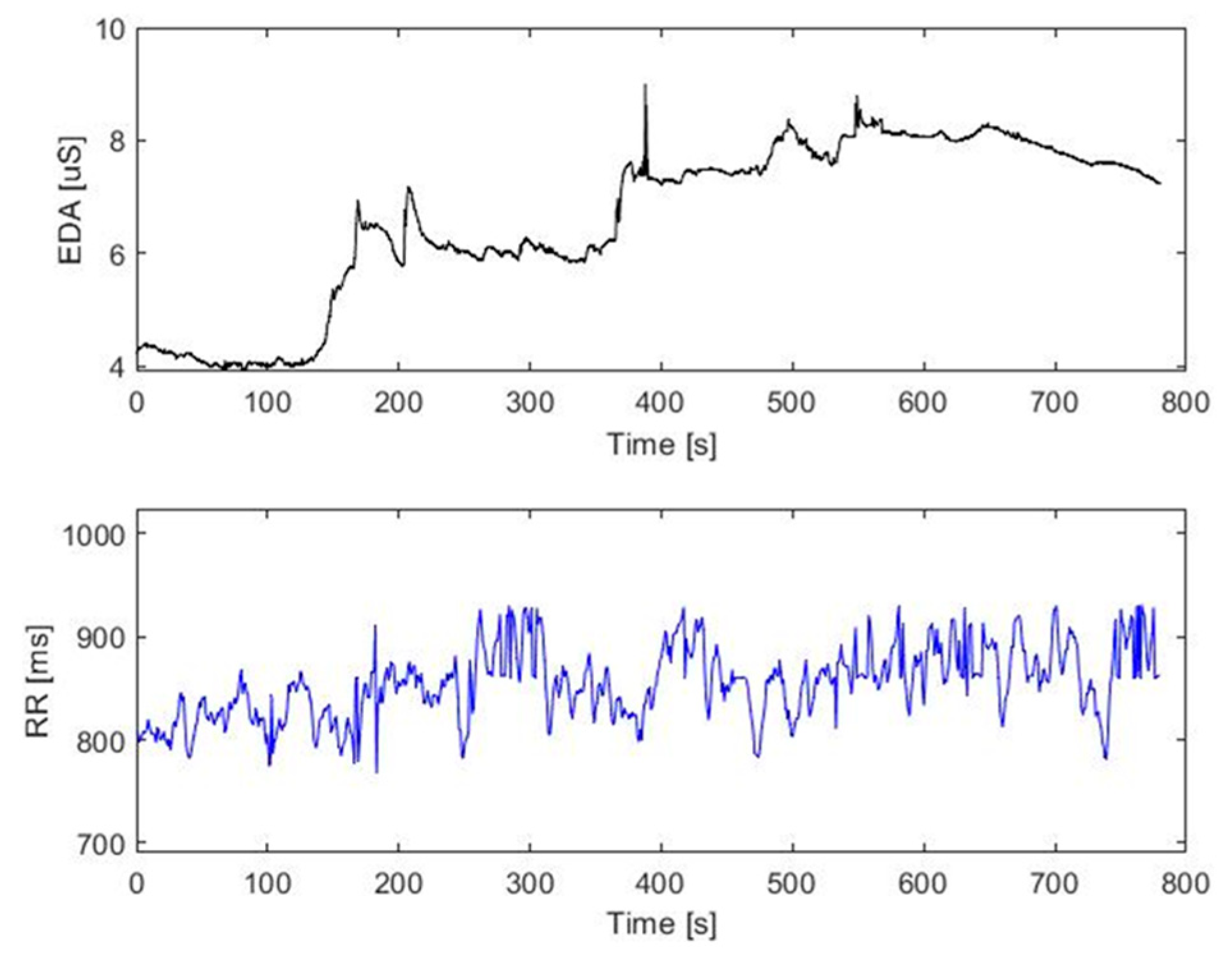
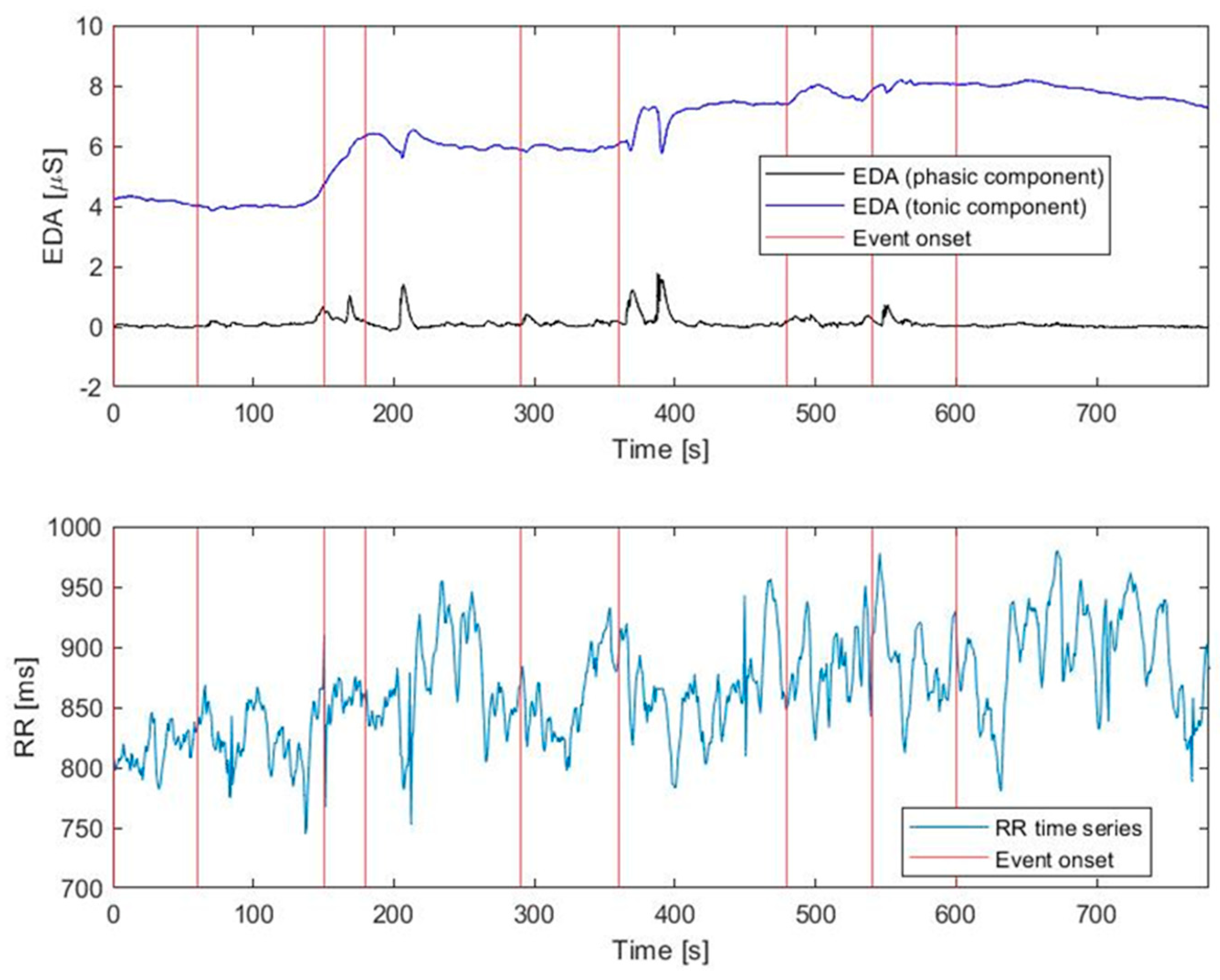
- EDA signal. This reflects the sympathetic nervous system activity and has already been used in pain recognition tasks [23]. This approach serves as a valuable indicator for assessing pain-induced neurocognitive stress by detecting changes in the electrical properties of the skin with the activation of sweat glands and ultimately an increase in skin conductance. The continuous changes in skin conductance are referred to as the skin conductance level (SCL), whereas the transient responses that occur within seconds are known as the galvanic skin response (GSR). Both the SCL and GSR contribute to the tonic and phasic components. The former represents a basic level of conductance (i.e., the SCL) and exhibits slow variations. On the other hand, the phasic component reflects the short-duration changes in the EDA signal (i.e., the skin conductance responses, SCRs) aroused by the presentation of a stimulus. Usually, the EDA signal is quantified in microsiemens (µS). Notably, this component can be used for providing insights into the overall automatic pain response [18].
- -
- ECG signal. This is the superficial recording of the heart’s electrical activity. Temporal fluctuations in inter-beat intervals can provide a measure of heart rate variability (HRV). This variability is closely linked to the activity of the autonomic nervous system (ANS) [24]. Indeed, HRV is influenced by the dynamic interplay between the sympathetic and parasympathetic branches of ANS (sympathovagal balance). These branches work in opposite directions, regulating heart rate to accommodate the body’s changing demands. Shifts in this equilibrium, reflected in HRV changes, are due to physiological factors (such as circadian rhythm) and pathological conditions (like diabetes and post-infarction situations) [25]. These variations can also indicate physiological responses to stressful and painful circumstances [16]. The RR series of interbeat intervals (i.e., the time between successive R waves of the QRS complex on the ECG waveform) has been computed to extract time-domain parameters of the HRV.
- -
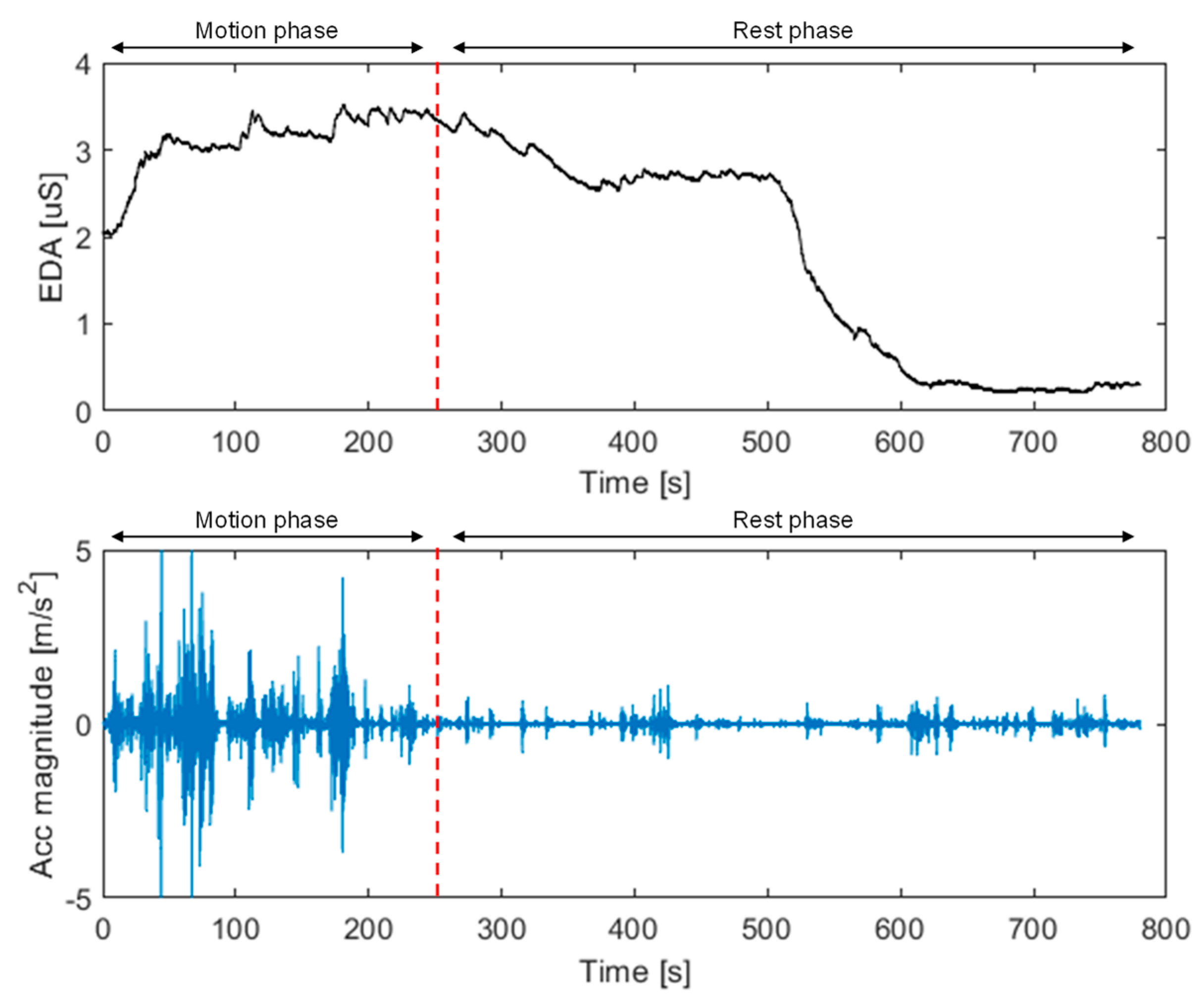
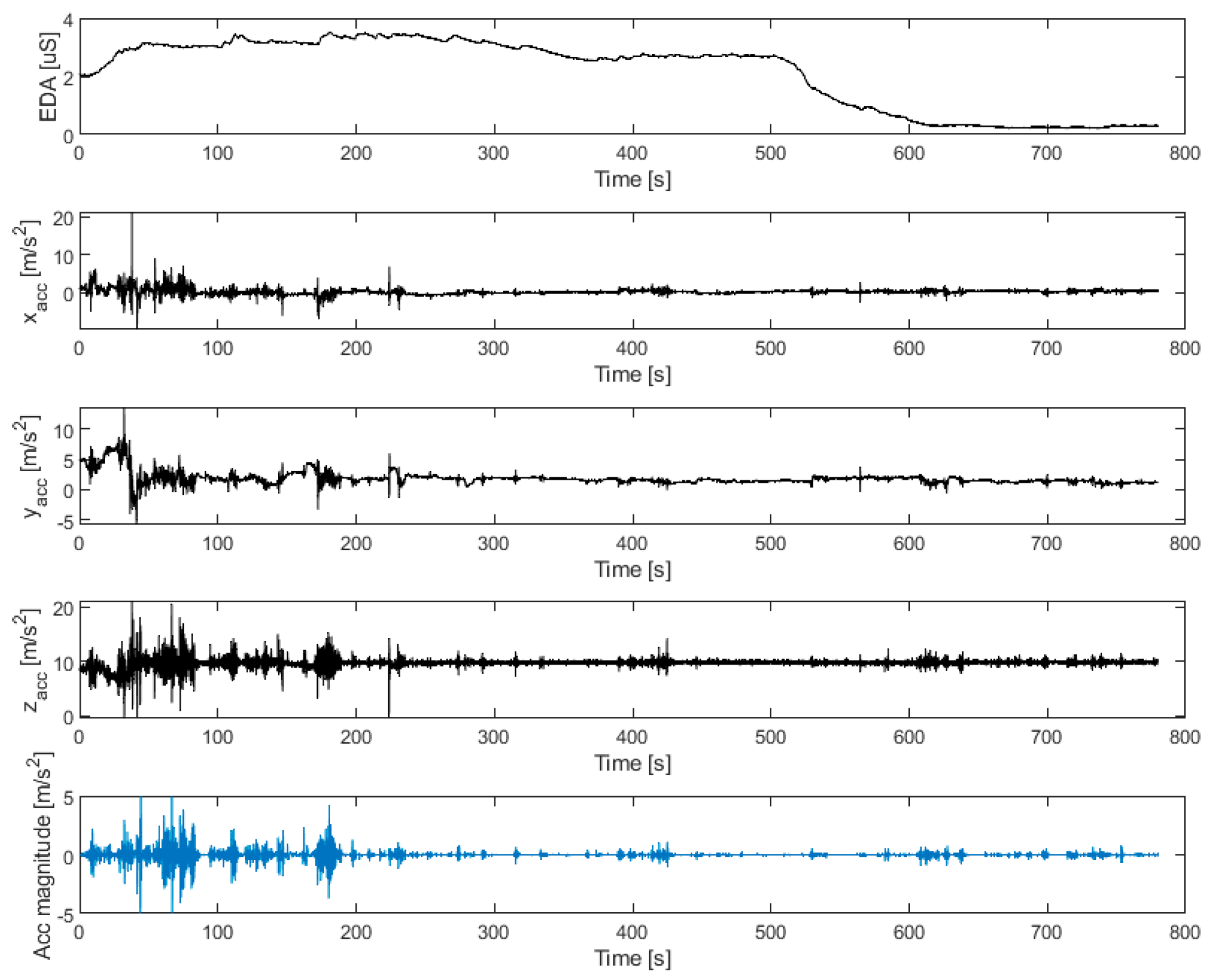
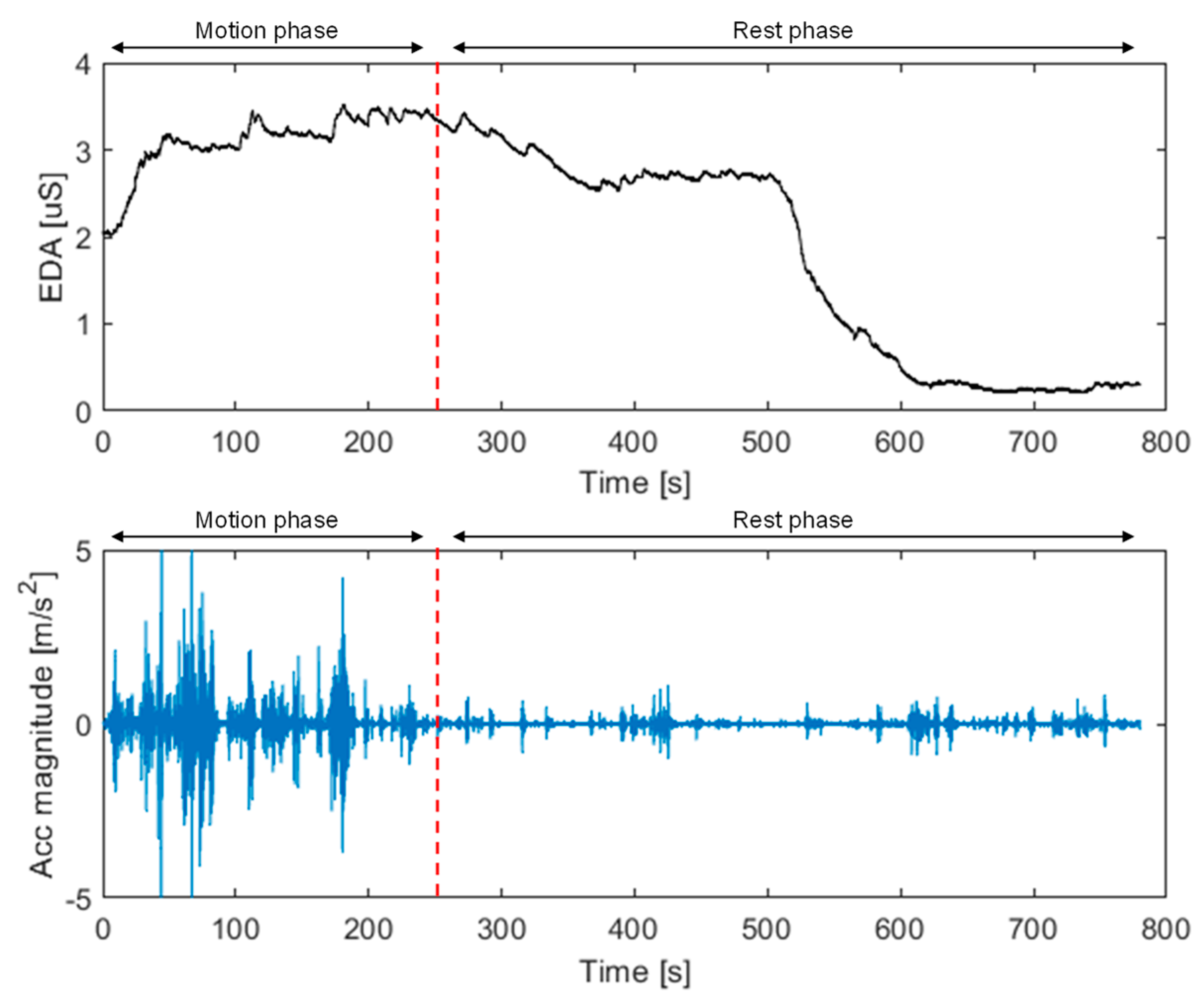
- Accelerometer signals. These can provide measurements of the motor activity along the three main directions of an orthogonal cartesian plane. Chen et al. [26] demonstrated that accelerometer signals correlate to the patient’s stress-induced pain. Within the proposed framework, they are used for obtaining a quantitative measure of motion-associated pain.
2.5. Biosignal Processing and Statistical Analysis
2.6. Case Studies
3. Results
3.1. Case Study No. 1: Clinical Presentation
3.2. Case Study No. 1: Pain Assessment by Means of EDA Signal
3.3. Case Study No. 2: Clinical Presentation
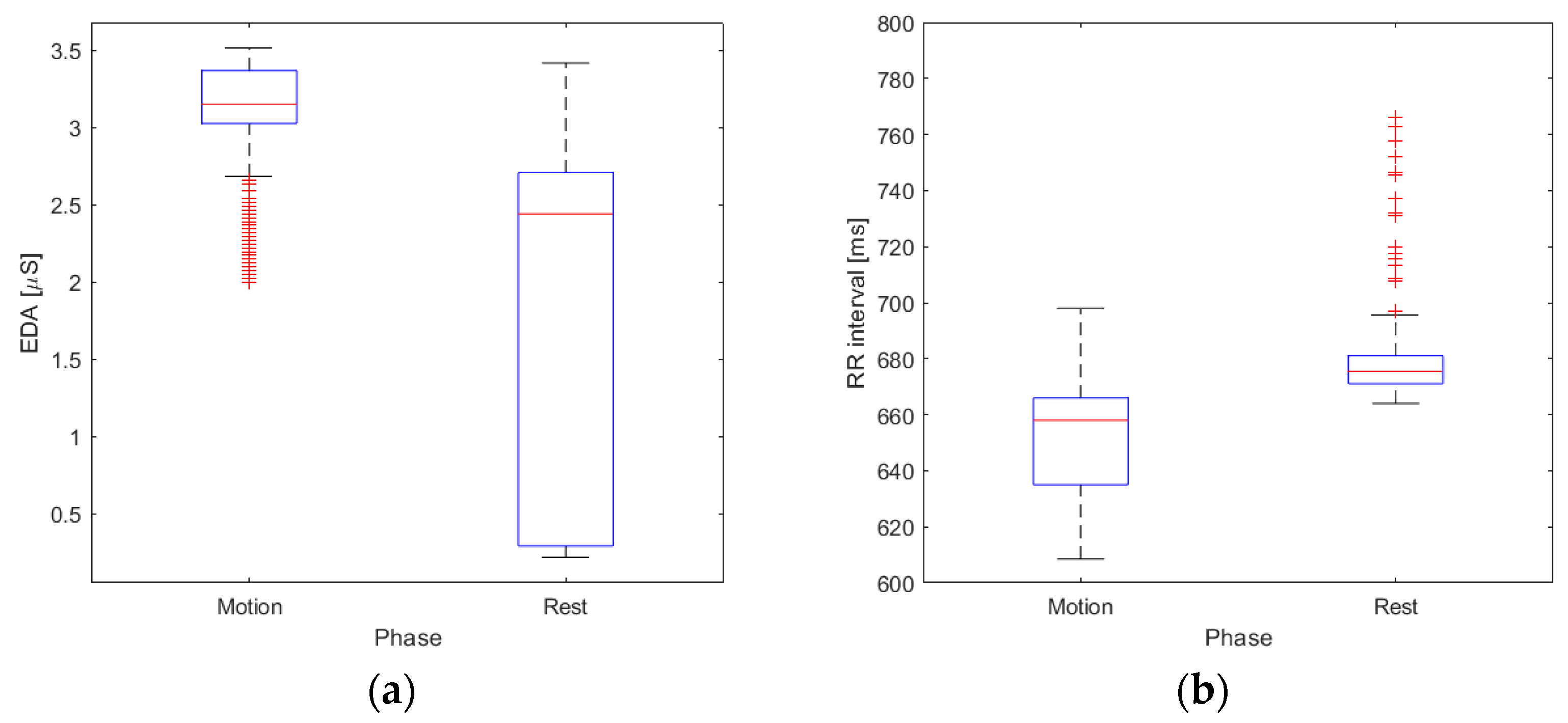
3.4. Case Study No. 2: Motion-Associated Pain Assessment by Means of EDA Signal and Accelerometer Data
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WCRF International. Global Cancer Data by Country; World Cancer Research Fund International: London, UK. Available online: https://www.wcrf.org/cancer-trends/global-cancer-data-by-country (accessed on 23 August 2023).
- World Health Organization (WHO). WHO Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents. Available online: https://www.who.int/publications-detail-redirect/9789241550390 (accessed on 16 June 2023).
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C.I. Management of Cancer Pain in Adult Patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv166–iv191. [Google Scholar] [CrossRef]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic Pain as a Symptom or a Disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic Pain: An Update on Burden, Best Practices, and New Advances. Lancet Lond. Engl. 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Cuomo, A.; Bimonte, S.; Forte, C.A.; Botti, G.; Cascella, M. Multimodal Approaches and Tailored Therapies for Pain Management: The Trolley Analgesic Model. J. Pain Res. 2019, 12, 711–714. [Google Scholar] [CrossRef]
- Brunelli, C.; Borreani, C.; Caraceni, A.; Roli, A.; Bellazzi, M.; Lombi, L.; Zito, E.; Pellegrini, C.; Spada, P.; Kaasa, S.; et al. PATIENT VOICES, a Project for the Integration of the Systematic Assessment of Patient Reported Outcomes and Experiences within a Comprehensive Cancer Center: A Protocol for a Mixed Method Feasibility Study. Health Qual. Life Outcomes 2020, 18, 252. [Google Scholar] [CrossRef]
- Caraceni, A.; Shkodra, M. Cancer Pain Assessment and Classification. Cancers 2019, 11, 510. [Google Scholar] [CrossRef]
- Kristiansen, F.L.; Olesen, A.E.; Brock, C.; Gazerani, P.; Petrini, L.; Mogil, J.S.; Drewes, A.M. The Role of Pain Catastrophizing in Experimental Pain Perception. Pain Pract. Off. J. World Inst. Pain 2014, 14, E136–E145. [Google Scholar] [CrossRef]
- Cascella, M.; Muzio, M.R.; Monaco, F.; Nocerino, D.; Ottaiano, A.; Perri, F.; Innamorato, M.A. Pathophysiology of Nociception and Rare Genetic Disorders with Increased Pain Threshold or Pain Insensitivity. Pathophysiol. Off. J. Int. Soc. Pathophysiol. 2022, 29, 435–452. [Google Scholar] [CrossRef] [PubMed]
- Yessick, L.R.; Tanguay, J.; Gandhi, W.; Harrison, R.; Dinu, R.; Chakrabarti, B.; Borg, E.; Salomons, T.V. Investigating the Relationship between Pain Indicators and Observers’ Judgements of Pain. Eur. J. Pain Lond. Engl. 2023, 27, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Bimonte, S.; Saettini, F.; Muzio, M.R. The Challenge of Pain Assessment in Children with Cognitive Disabilities: Features and Clinical Applicability of Different Observational Tools. J. Paediatr. Child Health 2019, 55, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Deldar, K.; Froutan, R.; Ebadi, A. Challenges Faced by Nurses in Using Pain Assessment Scale in Patients Unable to Communicate: A Qualitative Study. BMC Nurs. 2018, 17, 11. [Google Scholar] [CrossRef]
- Moscato, S.; Orlandi, S.; Giannelli, A.; Ostan, R.; Chiari, L. Automatic Pain Assessment on Cancer Patients Using Physiological Signals Recorded in Real-World Contexts. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022; pp. 1931–1934. [Google Scholar] [CrossRef]
- Wang, J.; Cheng, Z.; Kim, Y.; Yu, F.; Heffner, K.L.; Quiñones-Cordero, M.M.; Li, Y. Pain and the Alzheimer’s Disease and Related Dementia Spectrum in Community-Dwelling Older Americans: A Nationally Representative Study. J. Pain Symptom Manag. 2022, 63, 654–664. [Google Scholar] [CrossRef]
- Misra, G.; Wang, W.-E.; Archer, D.B.; Roy, A.; Coombes, S.A. Automated Classification of Pain Perception Using High-Density Electroencephalography Data. J. Neurophysiol. 2017, 117, 786–795. [Google Scholar] [CrossRef]
- Pouromran, F.; Radhakrishnan, S.; Kamarthi, S. Exploration of Physiological Sensors, Features, and Machine Learning Models for Pain Intensity Estimation. PLoS ONE 2021, 16, e0254108. [Google Scholar] [CrossRef]
- Posada-Quintero, H.F.; Chon, K.H. Innovations in Electrodermal Activity Data Collection and Signal Processing: A Systematic Review. Sensors 2020, 20, 479. [Google Scholar] [CrossRef]
- Forte, G.; Troisi, G.; Pazzaglia, M.; Pascalis, V.D.; Casagrande, M. Heart Rate Variability and Pain: A Systematic Review. Brain Sci. 2022, 12, 153. [Google Scholar] [CrossRef]
- Kim, Y.; Yoon, H.Y.; Kwon, I.K.; Youn, I.; Han, S. Heart Rate Variability as a Potential Indicator of Cancer Pain in a Mouse Model of Peritoneal Metastasis. Sensors 2022, 22, 2152. [Google Scholar] [CrossRef]
- Li, G.; Wu, S.; Zhao, H.; Guan, W.; Zhou, Y.; Shi, B. Non-Invasive Prognostic Biomarker of Lung Cancer Patients with Brain Metastases: Recurrence Quantification Analysis of Heart Rate Variability. Front. Physiol. 2022, 13, 987835. [Google Scholar] [CrossRef]
- Cuomo, A.; Cascella, M.; Forte, C.A.; Bimonte, S.; Esposito, G.; De Santis, S.; Cavanna, L.; Fusco, F.; Dauri, M.; Natoli, S.; et al. Careful Breakthrough Cancer Pain Treatment through Rapid-Onset Transmucosal Fentanyl Improves the Quality of Life in Cancer Patients: Results from the BEST Multicenter Study. J. Clin. Med. 2020, 9, 1003. [Google Scholar] [CrossRef]
- Moscato, S.; Cortelli, P.; Chiari, L. Physiological Responses to Pain in Cancer Patients: A Systematic Review. Comput. Methods Programs Biomed. 2022, 217, 106682. [Google Scholar] [CrossRef]
- Cascella, M.; Schiavo, D.; Cuomo, A.; Ottaiano, A.; Perri, F.; Patrone, R.; Migliarelli, S.; Bignami, E.G.; Vittori, A.; Cutugno, F. Artificial Intelligence for Automatic Pain Assessment: Research Methods and Perspectives. Pain Res. Manag. 2023, 2023, e6018736. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, R.; Kumar, R.; Malik, S.; Raj, T.; Kumar, P. Analysis of Heart Rate Variability and Implication of Different Factors on Heart Rate Variability. Curr. Cardiol. Rev. 2021, 17, e160721189770. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Abbod, M.; Shieh, J.-S. Pain and Stress Detection Using Wearable Sensors and Devices-A Review. Sensors 2021, 21, 1030. [Google Scholar] [CrossRef] [PubMed]
- Batista, D.; Silva, H.; Fred, A. Experimental Characterization and Analysis of the BITalino Platforms against a Reference Device. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Republic of Korea, 11–15 July 2017; pp. 2418–2421. [Google Scholar]
- Clevenger, K.A.; Pfeiffer, K.A.; Mackintosh, K.A.; McNarry, M.A.; Brønd, J.; Arvidsson, D.; Montoye, A.H.K. Effect of Sampling Rate on Acceleration and Counts of Hip- and Wrist-Worn ActiGraph Accelerometers in Children. Physiol. Meas. 2019, 40, 095008. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Hammerla, N.; Mellor, S.; Plötz, T. Optimising Sampling Rates for Accelerometer-Based Human Activity Recognition. Pattern Recognit. Lett. 2016, 73, 33–40. [Google Scholar] [CrossRef]
- Taylor, S.; Jaques, N.; Chen, W.; Fedor, S.; Sano, A.; Picard, R. Automatic Identification of Artifacts in Electrodermal Activity Data. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 1934–1937. [Google Scholar] [CrossRef]
- Benedek, M.; Kaernbach, C. A Continuous Measure of Phasic Electrodermal Activity. J. Neurosci. Methods 2010, 190, 80–91. [Google Scholar] [CrossRef]
- Benedek, M.; Kaernbach, C. Decomposition of Skin Conductance Data by Means of Nonnegative Deconvolution. Psychophysiology 2010, 47, 647–658. [Google Scholar] [CrossRef]
- Daviaux, Y.; Bonhomme, E.; Ivers, H.; de Sevin, É.; Micoulaud-Franchi, J.-A.; Bioulac, S.; Morin, C.M.; Philip, P.; Altena, E. Event-Related Electrodermal Response to Stress: Results From a Realistic Driving Simulator Scenario. Hum. Factors 2020, 62, 138–151. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, BME-32, 230–236. [Google Scholar] [CrossRef]
- Moeyersons, J.; Amoni, M.; Van Huffel, S.; Willems, R.; Varon, C. R-DECO: An Open-Source Matlab Based Graphical User Interface for the Detection and Correction of R-Peaks. PeerJ Comput. Sci. 2019, 5, e226. [Google Scholar] [CrossRef]
- Armañac, P.; Hernando, D.; Lázaro, J.; De Haro, C.; Magrans, R.; Sarlabous, L.; López-Aguilar, J.; Laguna, P.; Gil, E.; Blanch, L.; et al. Baroreflex Sensitivity Evolution Before Weaning From Mechanical Ventilation. In Proceedings of the 2020 Computing in Cardiology, Rimini, Italy, 13–16 September 2020; pp. 1–4. [Google Scholar]
- Karlsson, M.; Hörnsten, R.; Rydberg, A.; Wiklund, U. Automatic Filtering of Outliers in RR Intervals before Analysis of Heart Rate Variability in Holter Recordings: A Comparison with Carefully Edited Data. Biomed. Eng. Online 2012, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Maczák, B.; Vadai, G.; Dér, A.; Szendi, I.; Gingl, Z. Detailed Analysis and Comparison of Different Activity Metrics. PLoS ONE 2021, 16, e0261718. [Google Scholar] [CrossRef]
- John, D.; Tyo, B.; Bassett, D.R. Comparison of Four Actigraph Accelerometers During Walking and Running. Med. Sci. Sports Exerc. 2010, 42, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Khamis, H. Measures of Association: How to Choose? J. Diagn. Med. Sonogr. 2008, 24, 155–162. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Malik, M. Heart Rate Variability. Ann. Noninvasive Electrocardiol. 1996, 1, 151–181. [Google Scholar] [CrossRef]
- Vaschillo, E.; Lehrer, P.; Rishe, N.; Konstantinov, M. Heart Rate Variability Biofeedback as a Method for Assessing Baroreflex Function: A Preliminary Study of Resonance in the Cardiovascular System. Appl. Psychophysiol. Biofeedback 2002, 27, 1–27. [Google Scholar] [CrossRef]
- Martin, C.B. Physiology and Clinical Use of Fetal Heart Rate Variability. Clin. Perinatol. 1982, 9, 339–352. [Google Scholar] [CrossRef]
- Meister, K.; Juckel, G. A Systematic Review of Mechanisms of Change in Body-Oriented Yoga in Major Depressive Disorders. Pharmacopsychiatry 2018, 51, 73–81. [Google Scholar] [CrossRef]
- Mathersul, D.C.; Dixit, K.; Avery, T.J.; Schulz-Heik, R.J.; Zeitzer, J.M.; Mahoney, L.A.; Cho, R.H.; Bayley, P.J. Heart Rate and Heart Rate Variability as Outcomes and Longitudinal Moderators of Treatment for Pain across Follow-up in Veterans with Gulf War Illness. Life Sci. 2021, 277, 119604. [Google Scholar] [CrossRef]
- Javorka, K.; Lehotska, Z.; Kozar, M.; Uhrikova, Z.; Kolarovszki, B.; Javorka, M.; Zibolen, M. Heart Rate Variability in Newborns. Physiol. Res. 2017, 66, S203–S214. [Google Scholar] [CrossRef]
- Rother, M.; Zwiener, U.; Eiselt, M.; Witte, H.; Zwacka, G.; Frenzel, J. Differentiation of Healthy Newborns and Newborns-at-Risk by Spectral Analysis of Heart Rate Fluctuations and Respiratory Movements. Early Hum. Dev. 1987, 15, 349–363. [Google Scholar] [CrossRef] [PubMed]
- van den Beuken-van Everdingen, M.H.J.; de Rijke, J.M.; Kessels, A.G.; Schouten, H.C.; van Kleef, M.; Patijn, J. Prevalence of Pain in Patients with Cancer: A Systematic Review of the Past 40 Years. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2007, 18, 1437–1449. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Vittori, A.; Petrucci, E.; Marinangeli, F.; Giarratano, A.; Cacciagrano, C.; Tizi, E.S.; Miceli, L.; Natoli, S.; Cuomo, A. Strengths and Weaknesses of Cancer Pain Management in Italy: Findings from a Nationwide SIAARTI Survey. Healthcare 2022, 10, 441. [Google Scholar] [CrossRef] [PubMed]
- Gkikas, S.; Tsiknakis, M. Automatic Assessment of Pain Based on Deep Learning Methods: A Systematic Review. Comput. Methods Programs Biomed. 2023, 231, 107365. [Google Scholar] [CrossRef]
- Cascella, M.; Coluccia, S.; Grizzuti, M.; Romano, M.C.; Esposito, G.; Crispo, A.; Cuomo, A. Satisfaction with Telemedicine for Cancer Pain Management: A Model of Care and Cross-Sectional Patient Satisfaction Study. Curr. Oncol. 2022, 29, 5566–5578. [Google Scholar] [CrossRef]
- Lamotte, G.; Shouman, K.; Benarroch, E.E. Stress and Central Autonomic Network. Auton. Neurosci. Basic Clin. 2021, 235, 102870. [Google Scholar] [CrossRef]
- Hohenschurz-Schmidt, D.J.; Calcagnini, G.; Dipasquale, O.; Jackson, J.B.; Medina, S.; O’Daly, O.; O’Muircheartaigh, J.; de Lara Rubio, A.; Williams, S.C.R.; McMahon, S.B.; et al. Linking Pain Sensation to the Autonomic Nervous System: The Role of the Anterior Cingulate and Periaqueductal Gray Resting-State Networks. Front. Neurosci. 2020, 14, 147. [Google Scholar] [CrossRef]
- Arslan, D.; Ünal Çevik, I. Interactions between the Painful Disorders and the Autonomic Nervous System. Agri J. Turk. Soc. Algol. 2022, 34, 155–165. [Google Scholar] [CrossRef]
- Kyle, B.N.; McNeil, D.W. Autonomic Arousal and Experimentally Induced Pain: A Critical Review of the Literature. Pain Res. Manag. 2014, 19, 159–167. [Google Scholar] [CrossRef]
- Dormal, V.; Vermeulen, N.; Mejias, S. Is Heart Rate Variability Biofeedback Useful in Children and Adolescents? A Systematic Review. J. Child Psychol. Psychiatry 2021, 62, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Geovanini, G.R.; Vasques, E.R.; de Oliveira Alvim, R.; Mill, J.G.; Andreão, R.V.; Vasques, B.K.; Pereira, A.C.; Krieger, J.E. Age and Sex Differences in Heart Rate Variability and Vagal Specific Patterns—Baependi Heart Study. Glob. Heart 2020, 15, 71. [Google Scholar] [CrossRef] [PubMed]
- Pei, Z.; Shi, M.; Guo, J.; Shen, B. Heart Rate Variability Based Prediction of Personalized Drug Therapeutic Response: The Present Status and the Perspectives. Curr. Top. Med. Chem. 2020, 20, 1640–1650. [Google Scholar] [CrossRef]
- Wujtewicz, M.; Owczuk, R. Heart Rate Variability in Anaesthesiology—Narrative Review. Anaesthesiol. Intensive Ther. 2023, 55, 1–8. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
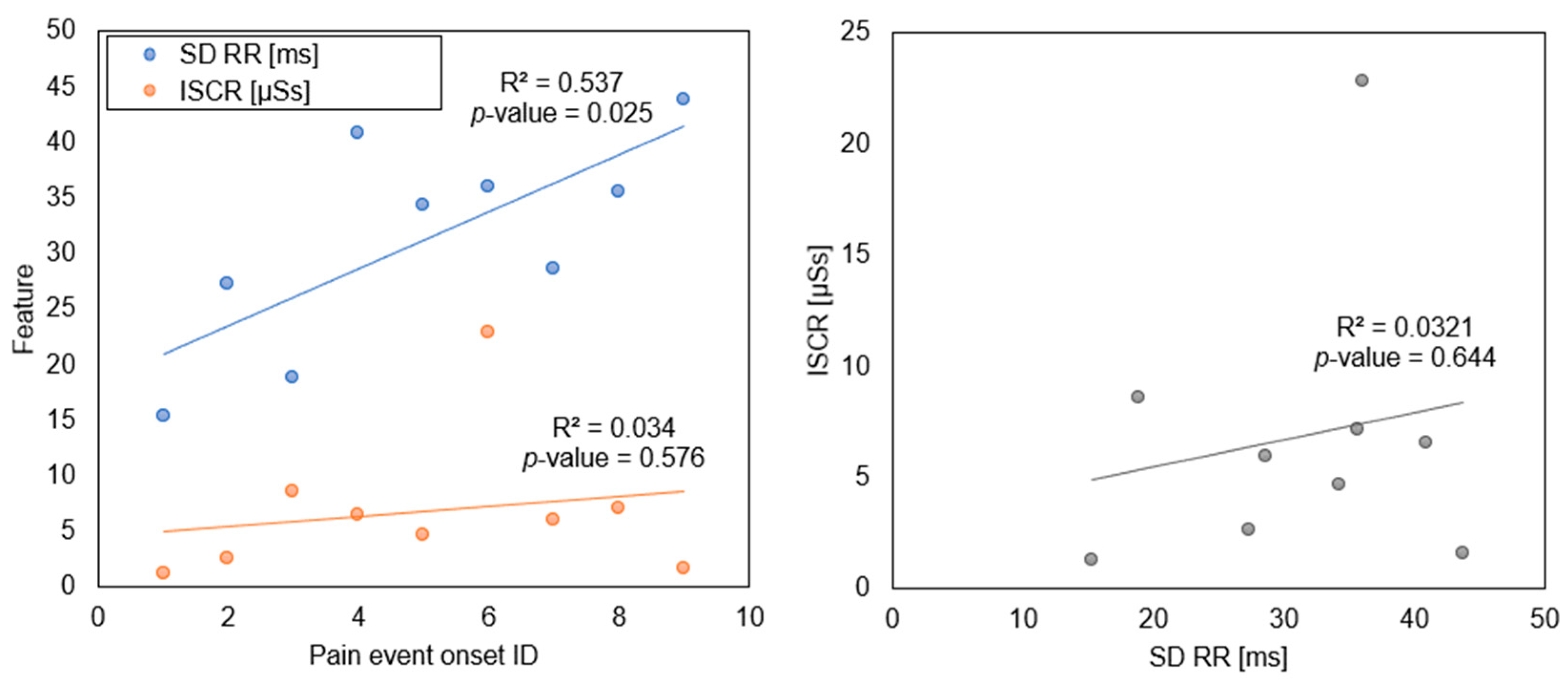
| Event ID * | SCR Latency (s) | SCR Sum (μS) | SCR Average (μS) | ISCR (μSs) | Mean RR (ms) | SD RR (ms) |
|---|---|---|---|---|---|---|
| 1 | 1.25 | 0.28 | 0.03 | 1.25 | 814.55 | 15.35 |
| 2 | 7.35 | 0.53 | 0.07 | 2.61 | 824.31 | 27.33 |
| 3 | 1.95 | 1.68 | 0.22 | 8.56 | 855.53 | 18.83 |
| 4 | 2.05 | 1.54 | 0.17 | 6.55 | 868.57 | 40.88 |
| 5 | 1.05 | 0.99 | 0.12 | 4.68 | 857.78 | 34.31 |
| 6 | 2.35 | 3.38 | 0.59 | 22.86 | 861.51 | 36.05 |
| 7 | 1.75 | 1.35 | 0.15 | 5.98 | 883.94 | 28.64 |
| 8 | 7.75 | 1.30 | 0.18 | 7.16 | 888.09 | 35.62 |
| 9 | 5.65 | 0.27 | 0.04 | 1.61 | 891.18 | 43.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cascella, M.; Vitale, V.N.; D’Antò, M.; Cuomo, A.; Amato, F.; Romano, M.; Ponsiglione, A.M. Exploring Biosignals for Quantitative Pain Assessment in Cancer Patients: A Proof of Concept. Electronics 2023, 12, 3716. https://doi.org/10.3390/electronics12173716
Cascella M, Vitale VN, D’Antò M, Cuomo A, Amato F, Romano M, Ponsiglione AM. Exploring Biosignals for Quantitative Pain Assessment in Cancer Patients: A Proof of Concept. Electronics. 2023; 12(17):3716. https://doi.org/10.3390/electronics12173716
Chicago/Turabian StyleCascella, Marco, Vincenzo Norman Vitale, Michela D’Antò, Arturo Cuomo, Francesco Amato, Maria Romano, and Alfonso Maria Ponsiglione. 2023. "Exploring Biosignals for Quantitative Pain Assessment in Cancer Patients: A Proof of Concept" Electronics 12, no. 17: 3716. https://doi.org/10.3390/electronics12173716
APA StyleCascella, M., Vitale, V. N., D’Antò, M., Cuomo, A., Amato, F., Romano, M., & Ponsiglione, A. M. (2023). Exploring Biosignals for Quantitative Pain Assessment in Cancer Patients: A Proof of Concept. Electronics, 12(17), 3716. https://doi.org/10.3390/electronics12173716