Advances of ECG Sensors from Hardware, Software and Format Interoperability Perspectives

 ,
,  ,
,  ,
,
Abstract
1. Introduction
1.1. Existing Survey Work
1.2. Motivation
2. Background
2.1. Cardiovascular Disease
2.1.1. Electrocardiogram Signals
2.1.2. Heart Attributes
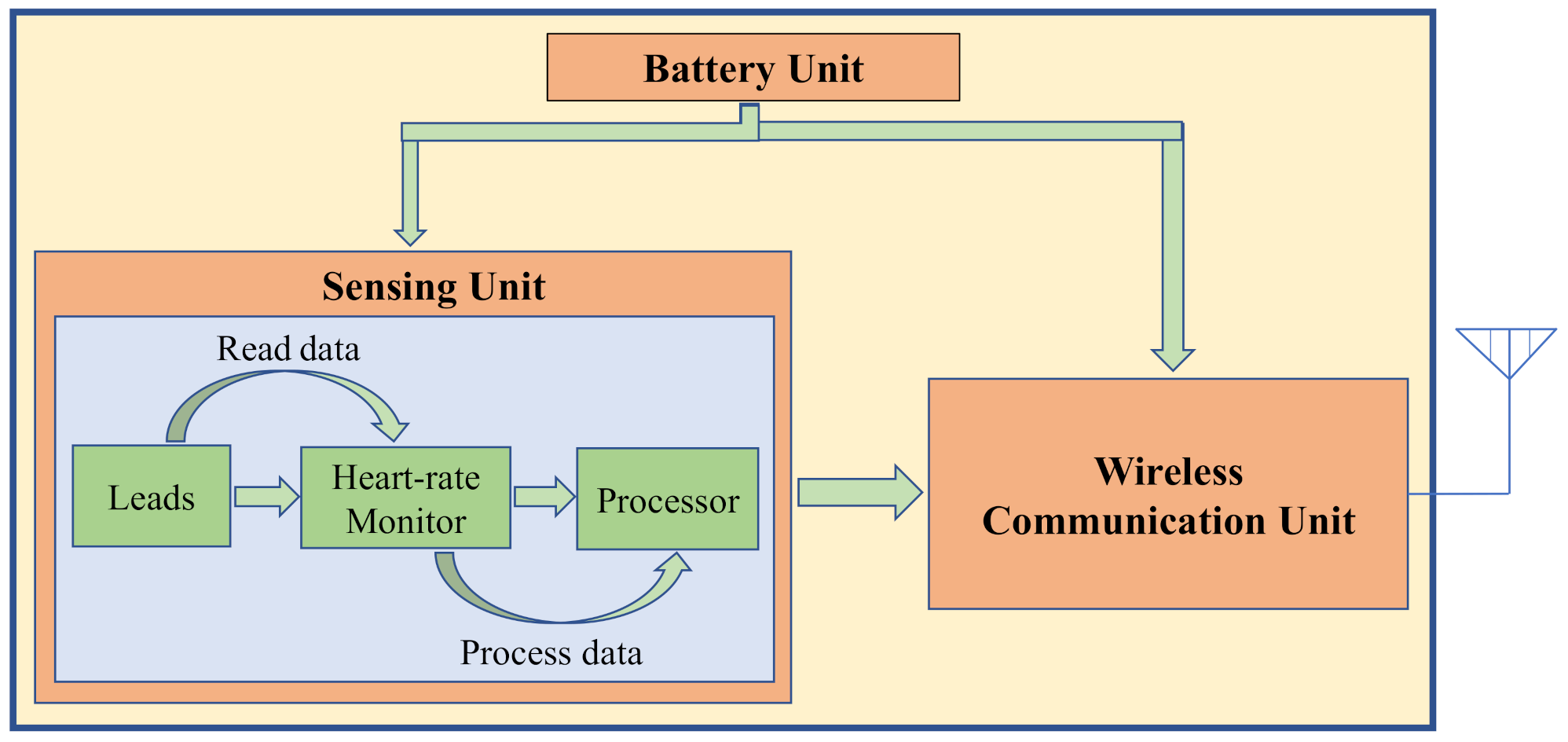
3. Hardware Perspective
3.1. Sensing Unit
3.1.1. Leads
3.1.2. Heart-Rate Monitor Board
AD8232:
AD8233:
MSP430FG439:
SEN0213:
3.1.3. Processing Board
Arduino UNO:
Arduino Pro Mini:
Arduino DUE:
Lilypad Arduino:
Raspberry Pi:
Raspberry Pi 2:
Raspberry Pi 3:
3.2. Communication Unit
3.2.1. ZigBee
3.2.2. Bluetooth
3.2.3. Infrared Data Association
3.2.4. Medical Implant Communication Service
3.2.5. IEEE 802.11g
3.3. Battery Unit
4. Software Perspective
4.1. Denoising
4.1.1. Discrete Wavelet Transform
- Hard thresholding
- Soft thresholding
4.1.2. Adaptive Filtering
Least Mean Squares (LMS) Algorithm:
Recursive Least-Squares (RLS):
4.1.3. Savitzky-Golay filtering
4.2. AI Techniques
4.2.1. Machine Learning
4.2.2. Deep Learning
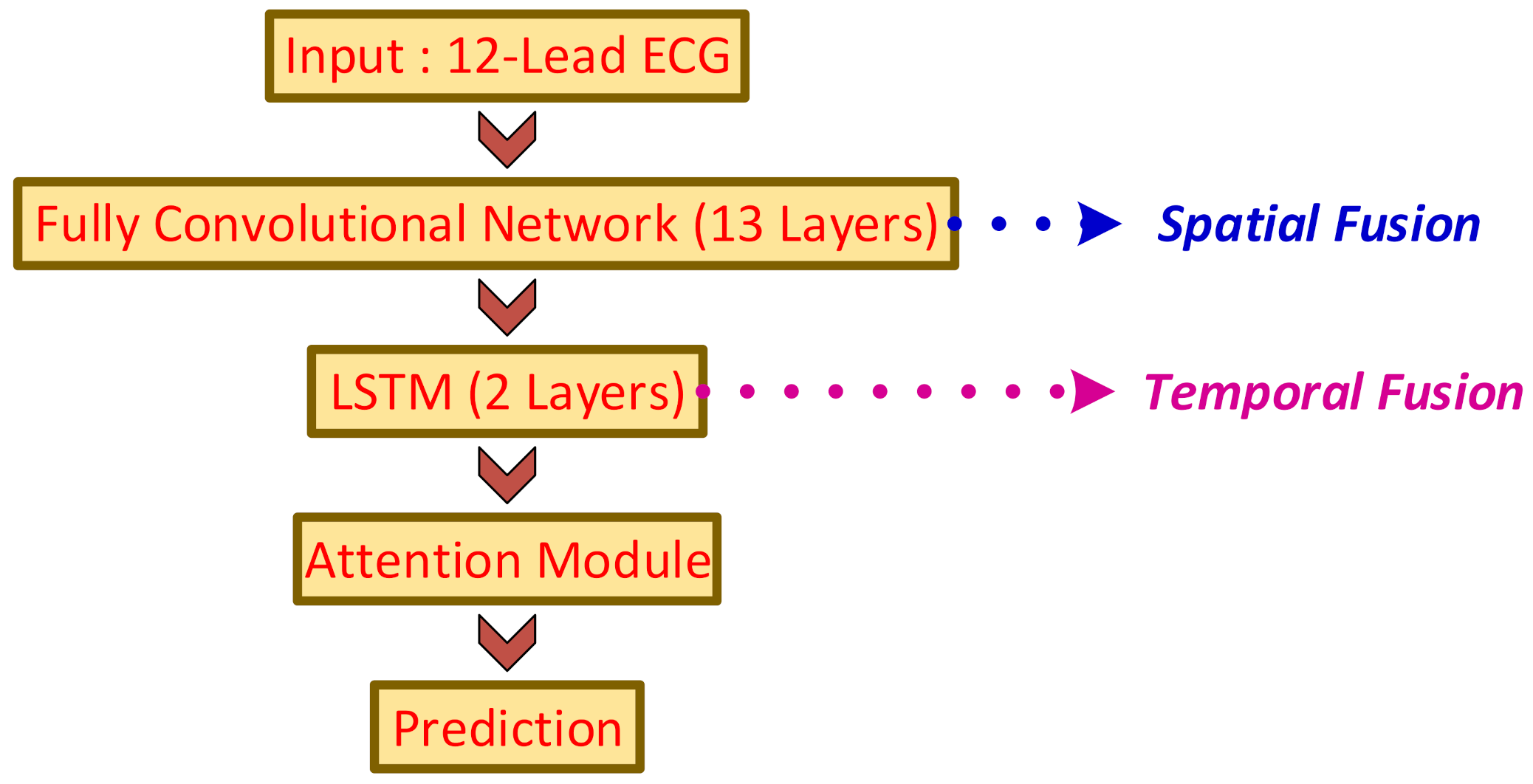
4.2.3. Use Case: Arrhythmia Detection for Varied-Length ECG using ATI-CNN
4.3. Other Computer Paradigms
4.3.1. Cloud Computing
4.3.2. Smartphone-Based Devices and Applications
4.3.3. Use Case: An Autonomic Cloud Environment for Hosting ECG Data Analysis Services
4.4. Existing Software Architectures for CVD Prediction and Classification
4.5. Privacy Preservation Techniques
5. Format Interoperability Perspective
5.1. Overview of Digital ECG Formats
- 1
- Supported by Standard Development Organizations (SDOs)
- –
- Widely known efforts The four commonly used ECG formats supported by SDOs are HL7 annotated ECG (HL7 aECG), computer-assisted electrocardiography (SCP-ECG) Standard Communications Protocol, Medical waveform Format Encoding Rules (MFER) and Digital Imaging and Communication in Medicine (DICOM) Waveform Supplement 30. HL7 aECG [176] is an ECG format based on XML and is an American standard from the American National Institute of Standards (ANSI). The SCP-ECG [177] is a binary encoding ECG format specification approved by the European Committee for Standardization (CEN) and is specifically intended for short-term diagnostic ECGs. Descriptions of the content and structure of the information to be transmitted between digital ECG devices and host ECG systems are presented in this format. The MFER [178] format, a Japanese standard, specializes in medical waveforms (EEG, respiratory waveforms, ECG etc.). This format is sponsored by the Japanese Healthcare Information systems Industry Association (JAHIS). Finally, DICOM Complement 30 [179] is a DICOM expansion for the regulation of biomedical signals such as ECG waveforms.
- –
- The X73 FamilyVital Signs Information Representation (VSIR) format, ENV 13734, also known as VITAL [180] was one of the first ECG formats in the X73 family and comprises of information and service model of object-oriented domains. The VSIR model is further improved by FEF, ENV 14271 [181] by considering the comprehensive nomenclature of biomedical measurements, comprising of data items observed in intensive care units, anesthesia departments, and clinical labs, including neurology. Finally, an update of both the VSIR and FEF versions is the IEEE P11073-10306 X73PoC (X73-Point of Care) specialization for ECG devices [182] format. The object-oriented design and study of the virtual ECG interface and the virtual medical system knowledge data model exchanged with the ECG are discussed in this format.
- 2
- Binary FormatsHolter applications utilize a specific ECG format, for recording a large amount of data, which is based on the requirements given by the International Society for Holter and Noninvasive Electrocardiology (ISHNE) [183,184]. The Hierarchical Data Format (HDF) is another binary ECG format that is utilized for high-resolution ECG signals [185]. In particular, HDF offers a collection of file formats and libraries that have been built to store and organize broad numerical data volumes [186]. Work in [187] suggested an improvement to the protocol of SCP-ECG and named it e-SCP-ECG+. More vital signs as well as demographic data can be handled by the revised format while also resolving some of the disadvantages of the previous protocol by creating new tags and parts.
- 3
- XML proposals
- –
- General PurposeThe Philips XML format [188] utilizes XML Schema Language and is available online along with the electrocardiograph documentation. This format uses a lossless algorithm to compress the ECG waveform data and utilizes a base 64 encoding scheme to encode the data into ASCII characters. Moreover, Scalable Vector Graphics (SVG) is the design format used by Philips XML and is capable of communicating with other display standards such as HL7 aECG or IHE Fetch ECG [189,190]. I-Med [191] consists of a domain-independent framework for transferring many forms of medical records, including ECG information, which can be explained by primary features such as QRS length and text-based interpretations. Work in [192] proposed a template solution called ecgML, for ECG data representation and exchange, to easily incorporate ECG data into electronic health records (EHRs) and medical guidance. The XML-ECG format was proposed in [193] compared to other XML-based ECG variants, like HL7 aECG which ecgML, and consists of a simple structure of just six modules and is more readable.
- –
- Environment SpecificTo overcome the technical limitations of mobile devices, the Mobile ElectroCardioGraphy Markup Language (mECGML) [194], which is a minimal XML format intended primarily for ECG sharing data and storing on smartphones, was proposed. Work in [195] proposed awareness of ECG, which is an XML-based markup language that offers information resources and expands reference criteria for ECG, to log a patient’s heart telemonitoring during daily operations. For the storage and archiving of sensor data from multiple recording systems, the Unified Data Format for Multi SENSor Data (UNISENS) format [196] was proposed. Several data types can be recorded in the format, such as events e.g. artifact areas, cause annotations, etc.), constant signals (e.g., thoracic impedance, ECG, acceleration, etc., and other biological values (e.g., breathing rhythm, blood pressure, pulse rate, etc.). The XML-BSPM format was suggested in [197] to promote the Body Surface Potential Map (BSPM) methods and was also checked alongside the Web-based XML-BSPM viewer [198].
- 4
- Intended for NeurophysiologyFor the neurophysiology environment, there is a need to record and transmit several biological signals such as the electrooculogram (EOG), the electroencephalogram (EEG) the electromyogram (EMG), etc. The standards developed to manage these signals can also be used to store ECG signals.
- –
- Data Format FamilyOne of the leading initiatives is the data format family that comprises multipurpose protocols. The European Data Format (EDF) [199] is one of the first Data Format Family initiatives and has a 16-bit format designed for time series conversion, like polygraphic storage. In addition, EDF is simpler and supports multiple scaling factors and sampling rates. Furthermore, the EDF protocol was enhanced to EDF+ [200], which included several changes, such as the ability to obtain intermittent records or the support of moment annotations, such as parameters of the ECG. To overcome certain limitations of EDF, the General Data Format (GDF) was proposed in [201] and supports many helpful applications that are not widely implemented in other formats only while providing a common event coding scheme. A 24-bit variant of the EDF 16-bit template, known as BioSemi Data Format (BDF) [201], was proposed that supports EEG, BSPM, and EMG applications. Finally, an XML-based EDF extension is proposed in [202]. This format is defined by Neurotronic and is called the OpenXDF protocol.
- –
- Others E1467 standard [203] is utilized to enable the free exchange of digital neurophysiological data among different computer systems. For some neurophysiological studies, this framework offers a method for waveform data exchange while also offering the ability to distort and label waveform data. Furthermore, ECG waveforms are also provided by the standard. Another digital biomedical signal format was proposed in [204], known as the signal interchange format (SIGIF), Supporting both raw and interpreted data, multiple mechanisms and representations of the signal, different epochs, and external analysis. The EBS file format [205,206] is binary and is utilized for saving Time-series multichannel recordings and related metadata. Specifically, this format can handle various biomedical data types such as EEG, ECG, MEG, ECoG, and other polygraphic recordings. An XML-based format is proposed in [207] to address the inherent incompatibility of different formats that are utilized for storing digital biomedical time-series signals. Finally, an interleaved file format (IFF) based format for physiological data called IFFPHYS is proposed in [208].
- 5
- DatabasesSeveral ECG databases offer their open data format. For instance, the Physionet database [13] offers the format of the Waveform Database. The Massachusetts Institute of Technology-Beth Israel Hospital (MIT-BIH) [14], the American Heart Association (AHA) [209], CSE [210,211,212], and the PTB-XL [175] are among the other databases.
- 6
- IHE (Cardiology Framework) The goal of the IHE Cardiology System is to incorporate current standards and promote cardiology workflow, sharing information, and patient care. Retrieve ECG for Display (ECG) [213] stable final text is one of the IHE Cardiology System integration profiles and provides enterprise-wide access to ECG documents for analysis using the Portable Document Format (PDF) with vector sketch or the type format of SVG + XML Multipurpose Internet Mail Extensions. The integration profile of the Resting ECG Workflow (REWF) [214] describes the workflow linked to automated electrocardiography. The REWF profile that complies with the requirements outlined in the retrieval ECG document for the display transaction is submitted to the displayable ECGs Waveform Communication Management (WCM) [215] is an upcoming IHE-PCD profile that provides a way to pass near-real-time waveform data between a gateway and a health care information system using ISO/IEEE nomenclature and HL7 v2 observation messages. Instead of bit maps or PDF files, data packets in WCM will comprise raw data. Finally, standard export data format (SEAMAT) [174] was developed by the Japanese Circulation Society to export data belonging to ECG, catheterization, and ultrasound cardiography to external storage.
- 7
- Ontologies ECG ontology based on the SCP-ECG file structure was proposed in [216] to integrate and provide seamless access to heterogeneous sources in the form of an electronic health record [217]. The National Center for Biomedical Ontology (NCBO) Bio-Portal has developed an ontology-based annotation [218] to describe ECGs, their methods of capture, and their waveforms. An ontology and conceptual modeling study group named NEMO (Portuguese Nucleo de Estudos em Modelagem Conceitual e Ontologias) [219] have created another ontology-based annotation.
5.2. Relationships among Digital ECG Formats
6. Conclusions and Future Directions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADC | Analog-to-digital converter |
| AODV | Ad hoc On-Demand Distance Vector |
| AI | Artificial intelligence |
| ANN | Artificial neural network |
| AWS | Amazon Web Service |
| ANSI | American National Institute of Standards |
| AHA | American Heart Association |
| ATI-CNN | Attention-based time-incremental convolutional neural network |
| BWD | Body-worn devices |
| BSPM | Body Surface Potential Map |
| BDF | BioSemi Data Format |
| CNN | Convolutional neural network |
| CVD | Cardiovascular Disease |
| CBA | Commercial building automation |
| CVIS | Cardiovascular information system |
| DSSS | Direct sequence spread spectrum |
| DWT | Discrete wavelet transform |
| DL | Deep learning |
| DICOM | Digital Imaging and Communication in Medicine |
| ECG | Electrocardiogram |
| HER | Electronic Health Record |
| EOG | Electrooculogram |
| EEG | Electroencephalogram |
| EMG | Electromyogram |
| EMU | Energy Management Unit |
| EHRs | Electronic health records |
| FFT | Fast Fourier transform |
| FHSS | Frequency hopping spread spectrum |
| GDF | General Data Format |
| HPF | High pass filter |
| HA | Home automation |
| HIPAA | Health Insurance Portability and Accountability Act |
| HDF | Hierarchical Data Format |
| IrDA | Infrared Data Association |
| IR | Infrared |
| ISHNE | International Society for Holter and Noninvasive Electrocardiology |
| IFF | Interleaved file format |
| JAHIS | Japanese Healthcare Information Systems Industry Association |
| Li-Ion | Lithium-Ion |
| LPF | Low pass filter |
| LMS | Least Mean Squares |
| LSTM | Long short-term memory |
| MICS | Medical Implant Communication System |
| MSE | Mean-squared error |
| ML | Machine learning |
| MLaaS | Machine learning as a service |
| mHealthcare | Mobile healthcare |
| MFER | Medical waveform Format Encoding Rules |
| mECGQML | Mobile ElectroCardioGraphy Markup Language |
| MIT-BIH | Massachusetts Institute of Technology-Beth Israel Hospital |
| NIST | National Institute of Standard and Technology |
| NCBO | National Center for Biomedical Ontology |
| P/C | Programmer/controller |
| Portable Document Format | |
| PACS | Picture archiving and communication system |
| RPI | Raspberry PI |
| RLS | Recursive Least-Squares |
| REWF | Resting ECG Workflow |
| STFT | Short-time Fourier transform |
| SVM | Support vector machine |
| SE | Smart energy |
| SBDAs | Smartphone-based devices and applications |
| SDOs | Standard Development Organizations |
| SVG | Scalable Vector Graphics |
| SIGIF | Signal interchange format |
| TA | Telecom applications |
| VSIR | Vital Signs Information Representation |
| WHO | World Health Organization |
| WSA | Wireless sensor applications |
| WLAN | Wireless networks |
| WT | Wavelet transform |
| WTA | Winner-take-all |
| WCM | Waveform Communication Management |
References
- Arji, G.; Ahmadi, H.; Nilashi, M.; Rashid, T.A.; Hassan Ahmed, O.; Aljojo, N.; Zainol, A. Fuzzy logic approach for infectious disease diagnosis: A methodical evaluation, literature and classification. Biocybern. Biomed. Eng. 2019, 39, 937–955. [Google Scholar] [CrossRef] [PubMed]
- Tayefi, M.; Tajfard, M.; Saffar, S.; Hanachi, P.; Amirabadizadeh, A.R.; Esmaeily, H.; Taghipour, A.; Ferns, G.A.; Moohebati, M.; Ghayour-Mobarhan, M. hs-CRP is strongly associated with coronary heart disease (CHD): A data mining approach using decision tree algorithm. Comput. Methods Programs Biomed. 2017, 141, 105–109. [Google Scholar] [CrossRef]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. Neuroeng. Rehabil. 2012, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.M.; Gholamhosseini, H.; Connolly, M.J. A comprehensive survey of wearable and wireless ECG monitoring systems for older adults. Med. Biol. Eng. Comput. 2013, 51, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.K.; Tiwari, A.K. Heart monitoring systems-A review. Comput. Biol. Med. 2014, 54, 1–13. [Google Scholar] [CrossRef]
- Haritha, C.; Ganesan, M.; Sumesh, E.P. A survey on modern trends in ECG noise removal techniques. In Proceedings of the International Conference on Circuit, Power and Computing Technologies (ICCPCT), Nagercoil, India, 18–19 March 2016; pp. 1–7. [Google Scholar] [CrossRef]
- Ramasamy, S.; Balan, A. Wearable sensors for ECG measurement: A review. Sens. Rev. 2018. [Google Scholar] [CrossRef]
- Serhani, M.A.; El Kassabi, H.T.; Ismail, H.; Nujum Navaz, A. ECG Monitoring Systems: Review, Architecture, Processes, and Key Challenges. Sensors 2020, 20, 1796. [Google Scholar] [CrossRef]
- WHO. The Atlas of Heart Disease and Stroke/Judith Mackay and George Mensah with Shanthi Mendis and Kurt Greenland; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Felman, A. Cardiovascular Disease: Types, Symptoms, Prevention, and Causes. 2019. Available online: https://www.medicalnewstoday.com/articles/257484 (accessed on 3 September 2020).
- Laguna, P.; Jané, R.; Olmos, S.; Thakor, N.V.; Rix, H.; Caminal, P. Adaptive estimation of QRS complex wave features of ECG signal by the Hermite model. Med. Biol. Eng. Comput. 1996, 34, 58–68. [Google Scholar] [CrossRef]
- Devi, R.L.; Kalaivani, V. Machine learning and IoT-based cardiac arrhythmia diagnosis using statistical and dynamic features of ECG. J. Supercomput. 2019, 76. [Google Scholar] [CrossRef]
- Moody, G.B.; Mark, R.G.; Goldberger, A.L. PhysioNet: A Web-based resource for the study of physiologic signals. IEEE Eng. Med. Biol. Mag. 2001, 20, 70–75. [Google Scholar] [CrossRef]
- MIT-BIH Database and Software Catalog. Available online: http://ecg.mit.edu/dbinfo.html (accessed on 13 October 2020).
- Kusuma, S.; Udayan, D. Machine Learning and Deep Learning Methods in Heart Disease (HD) Research. Int. J. Pure Appl. Math. 2018, 119, 1483–1496. [Google Scholar]
- Janosi, A.; Steinbrunn, W.; Pfisterer, M.; Detrano, R. Heart Disease Data Set. Available online: https://archive.ics.uci.edu/ml/datasets/heart+Disease (accessed on 16 December 2020).
- Mythili, T.; Mukherji, D.; Padalia, N.; Naidu, A. A heart disease prediction model using SVM-Decision Trees-Logistic Regression (SDL). Int. J. Comput. Appl. 2013, 68, 11–15. [Google Scholar]
- ECG Lead Positioning. Available online: https://litfl.com/ecg-lead-positioning/ (accessed on 23 November 2020).
- 5-Lead ECG Placement and Cardiac Monitoring. Available online: https://www.ausmed.com/cpd/articles/5-lead-ecg (accessed on 23 November 2020).
- 12-Lead ECG Placement Guide with Illustrations. Available online: https://www.cablesandsensors.com/pages/12-lead-ecg-placement-guide-with-illustrations (accessed on 23 November 2020).
- Wang, G.; Wang, W.; Yu, L. Design and implementation of the wireless ECG monitor based on AD8232 and CC2530. Chin. J. Med. Instrum. 2018, 42, 18–21. [Google Scholar]
- Kanani, P.; Padole, M. Recognizing Real Time ECG Anomalies Using Arduino, AD8232 and Java. In Proceedings of the International Conference on Advances in Computing and Data Sciences, Dehradun, India, 20–21 April 2018; pp. 54–64. [Google Scholar]
- Agung, M.A.; Basari. 3-lead acquisition using single channel ECG device developed on AD8232 analog front end for wireless ECG application. In AIP Conference Proceedings; AIP Publishing LLC.: Melville, NY, USA, 2017. [Google Scholar]
- Lu, T.C.; Liu, P.; Gao, X.; Lu, Q.Y. A portable ECG monitor with low power consumption and small size based on AD8232 chip. In Applied Mechanics and Materials; Trans Tech Publisher: Zurich Switzerland, 2014; Volume 513, pp. 2884–2887. [Google Scholar]
- Gifari, M.W.; Zakaria, H.; Mengko, R. Design of ECG Homecare:12-lead ECG acquisition using single channel ECG device developed on AD8232 analog front end. In Proceedings of the International Conference on Electrical Engineering and Informatics (ICEEI), Bali, Indonesia, 10–11 August 2015; pp. 371–376. [Google Scholar]
- Bhosale, V.K.; Bhosale, K.E. Healthcare Based on IoT using Arduino and AD8232 Hearth Rate Monitoring Chip. Asian J. Converg. Technol. 2016, 2. [Google Scholar]
- Walinjkar, A.; Woods, J. Personalized wearable systems for real-time ECG classification and healthcare interoperability: Real-time ECG classification and FHIR interoperability. In Proceedings of the Internet Technologies and Applications, Wrexham, UK, 12–15 September 2017; pp. 9–14. [Google Scholar]
- Plourde, D. Flexible ECG Front-End IC Serves Ultralow Power IoT Edge Node Signal Processing Designs.
- Walinjkar, A.; Woods, J. FHIR tools for healthcare interoperability. Biomed. J. Sci. Tech. Res. 2018, 9. [Google Scholar] [CrossRef]
- Yang, H.; Chai, J. A Portable Wireless ECG Monitor Based on MSP430FG439. In Proceedings of the International Conference on Intelligent Computation and Bio-Medical Instrumentation, Wuhan, China, 14–17 December 2011; pp. 148–151. [Google Scholar]
- Dwivedi, N.D.; Kumar, P. Design A Wirless ECG System.
- Yumang, A.N.; Talisic, G.C.; Oripaypay, L.F.; Balbin, J.R.; Lopez, C.E.V.; Fausto, J.C.; Mabbagu, C.J.P. Vital Signs Determination from ECG and PPG Signals Obtained from Arduino Based Sensors. In Proceedings of the 9th International Conference on Biomedical Engineering and Technology, Tokyo, Japan, 28–30 March 2019; pp. 235–239. [Google Scholar]
- Das, S.; Pal, S.; Mitra, M. Arduino-based noise robust online heart-rate detection. J. Med. Eng. Technol. 2017, 41, 170–178. [Google Scholar] [CrossRef]
- Asadina, H.; Hamzah, T.; Titisari, D.; Utomo, B. A Centrifuge Calibrator Based on Personal Computer Equipped with Data Processor. Indones. J. Electron. Electromed. Eng. Med. Inf. 2019, 1, 14–19. [Google Scholar] [CrossRef]
- Harjono, D.T.; Tamsir, A.S. Biomedical Sensor ECG, PPG, and spO2 Based on Arduino Which Result from Comparison with Portable; Technical Report; EasyChair: Manchester, UK, 2020. [Google Scholar]
- Hasan, D.; Ismaeel, A. Designing ECG Monitoring Healthcare System Based on Internet of Things Blynk Application. J. Appl. Sci. Technol. Trends 2020, 1, 106–111. [Google Scholar] [CrossRef]
- Ahamed, M.A.; Asraf-Ul-Ahad, M.; Sohag, M.H.A.; Ahmad, M. Development of low cost wireless ECG data acquisition system. In Proceedings of the International Conference on Advances in Electrical Engineering (ICAEE), Dhaka, Bangladesh, 17–19 December 2015; pp. 72–75. [Google Scholar]
- Puente, S.; Úbeda, A.; Torres, F. e-Health: Biomedical instrumentation with Arduino. IFAC-PapersOnLine 2017, 50, 9156–9161. [Google Scholar] [CrossRef]
- Pathoumvanh, S.; Bounnady, K.; Indahak, P.; Viravong, V. Implementation of the ECG biometric identification by using Arduino Microprocessor. In Proceedings of the 13th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology (ECTI-CON), Chiang Mai, Thailand, 28 June–1 July 2016; pp. 1–4. [Google Scholar]
- Tuna, G.; Das, R.; Tuna, A. Wireless sensor network-based health monitoring system for the elderly and disabled. Int. J. Comput. Networks Appl. (IJCNA) 2015, 2, 247–253. [Google Scholar]
- Alves, A.P.; Silva, H.; Lourenco, A.; Fred, A.L. BITtalino: A Biosignal Acquisition System based on the Arduino. In Proceedings of the BIODEVICES, Barcelona, Spain, 11–14 February 2013; pp. 261–264. [Google Scholar]
- Tanaka, Y.; Izumi, S.; Kawamoto, Y.; Kawaguchi, H.; Yoshimoto, M. Adaptive noise cancellation method for capacitively coupled ECG sensor using single insulated electrode. In Proceedings of the IEEE Biomedical Circuits and Systems Conference (BioCAS), Shanghai, China, 17–19 October 2016; pp. 296–299. [Google Scholar]
- Sharma, O.; Lewis, S.N.; Telang, U.; D’Almeida, L.; Lewis, L.E.S. Design of a bluetooth enabled health monitoring system for infants using wearable technology. J. Adv. Res. Dyn. Contrl. Syst 2017, 15, 887–894. [Google Scholar]
- Chen, W.; Nguyen, S.T.; Coops, R.; Oetomo, S.B.; Feijs, L. Wireless transmission design for health monitoring at neonatal intensive care units. In Proceedings of the 2nd International Symposium on Applied Sciences in Biomedical and Communication Technologies, Bratislava, Slovakia, 24–27 November 2009; pp. 1–6. [Google Scholar]
- Gia, T.N.; Jiang, M.; Rahmani, A.M.; Westerlund, T.; Mankodiya, K.; Liljeberg, P.; Tenhunen, H. Fog computing in body sensor networks: An energy efficient approach. In Proceedings of the IEEE International Body Sensor Networks Conference (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–7. [Google Scholar]
- Lai, S.; Hung, Y.; Chang, Y. Low-Cost Prototype Design of Biomedical Sensing Device for ECG and EMG Signal Acquisition System. In Proceedings of the International Conference BIOMDLORE, Białystok, Poland, 28–30 June 2018; pp. 1–2. [Google Scholar]
- Arun, C.S.; Alexander, A. Mobile ECG monitoring device using wearable non contact armband. In Proceedings of the International Conference on Circuit, Power and Computing Technologies (ICCPCT), Kollam, India, 20–21 April 2017; pp. 1–4. [Google Scholar]
- Abtahi, F.; Aslamy, B.; Boujabir, I.; Seoane, F.; Lindecrantz, K. An affordable ECG and respiration monitoring system based on Raspberry PI and ADAS1000: First step towards homecare applications. In Proceedings of the 16th Nordic-Baltic Conference on Biomedical Engineering, Gothenburg, Sweden, 14–16 October 2014; pp. 5–8. [Google Scholar]
- Gupta, M.S.D.; Patchava, V.; Menezes, V. Healthcare based on IoT using Raspberry Pi. In Proceedings of the International Conference on Green Computing and Internet of Things (ICGCIoT), Greater Noida, India, 8–10 October 2015; pp. 796–799. [Google Scholar]
- Singh, P.; Jasuja, A. IoT based low-cost distant patient ECG monitoring system. In Proceedings of the International Conference on Computing, Communication and Automation (ICCCA), Greater Noida, India, 5–6 May 2017; pp. 1330–1334. [Google Scholar]
- Clark, N.; Sandor, E.; Walden, C.; Ahn, I.S.; Lu, Y. A wearable ECG monitoring system for real-time arrhythmia detection. In Proceedings of the IEEE 61st International Midwest Symposium on Circuits and Systems (MWSCAS), Windsor, ON, Canada, 5–8 August 2018; pp. 787–790. [Google Scholar]
- Hafid, A.; Benouar, S.; Kedir-Talha, M.; Abtahi, F.; Attari, M.; Seoane, F. Full Impedance Cardiography Measurement Device Using Raspberry PI3 and System-on-Chip Biomedical Instrumentation Solutions. IEEE J. Biomed. Health Inf. 2018, 22, 1883–1894. [Google Scholar] [CrossRef]
- Automation.com. ZigBee Alliance Announces Gateway Standard. Available online: https://www.automation.com/en-us/articles/2011-2/zigbee-alliance-announces-gateway-standard (accessed on 8 September 2020).
- Ran, P.; Sun, M.; Zou, Y. ZigBee Routing Selection Strategy Based on Data Services and Energy-Balanced ZigBee Routing. In Proceedings of the 2006 IEEE Asia-Pacific Conference on Services Computing (APSCC’06), Guangzhou, China, 12–15 December 2006; pp. 400–404. [Google Scholar]
- Ergen, S.C. ZigBee/IEEE 802.15. 4 Summary. UC Berkeley Sept. 2004, 10, 11. [Google Scholar]
- Altun, A.A.; Bascifci, N. A wireless sensor network based on zigbee for ECG monitoring system. In Proceedings of the 2011 5th International Conference on Application of Information and Communication Technologies (AICT), Azerbaijan, Baku, 12–14 October 2011; pp. 1–5. [Google Scholar]
- Bluetooth. Available online: https://www.bluetooth.com/ (accessed on 8 September 2020).
- Ming, H.; Yajun, Z.; Xiaoping, H. Portable ECG Measurement Device based on MSP430 MCU. In Proceedings of the International Conference on BioMedical Engineering and Informatics, Sanya, Chain, 28–30 May 2008; Volume 2, pp. 667–671. [Google Scholar]
- Zhu, J.; Rao, N.; Liang, D.; Chen, W. Design of Pre-processing Circuit for Wireless ECG Monitoring System. In Proceedings of the International Conference on BioMedical Engineering and Informatics, Sanya, Chain, 28–30 May 2008; Volume 2, pp. 598–602. [Google Scholar]
- Tahat, A.A. Mobile personal electrocardiogram monitoring system and transmission using MMS. In Proceedings of the 7th International Caribbean Conference on Devices, Circuits and Systems, Cancun, Mexico, 28–30 April 2008; pp. 1–5. [Google Scholar]
- Kho, T.K.; Besar, R.; Tan, Y.S.; Tee, K.H.; Ong, K.C. Bluetooth-enabled ECG Monitoring System. In Proceedings of the TENCON 2005–2005 IEEE Region 10 Conference, Melbourn, Australia, 21–24 November 2005; pp. 1–5. [Google Scholar]
- Debbabi, M.; Saleh, M.; Talhi, C.; Zhioua, S. Java ME CLDC Security Analysis. In Embedded Java Security: Security for Mobile Devices; Springer: Berlin/Heidelberg, Germany, 2007; pp. 115–152. [Google Scholar]
- Hirt, W.; Hassner, M.; Heise, N. IrDA-VFIr (16 Mb/s): Modulation code and system design. IEEE Pers. Commun. 2001, 8, 58–71. [Google Scholar] [CrossRef]
- GajduŜek, M.; Overboom, T.; Damen, A.; van den Bosch, P. Infrared wireless data transfer for real-time motion control. IFAC Proc. Vol. 2009, 42, 198–203. [Google Scholar] [CrossRef]
- Knutson, C.D.; Diviney, G. Infrared Data Communications with IrDA; IrDA Test and Interoperability Committee: Corvallis, OR, USA, 1998. [Google Scholar]
- Savci, H.S.; Sula, A.; Wang, Z.; Dogan, N.S.; Arvas, E. MICS transceivers: Regulatory standards and applications. In Proceedings of the IEEE SoutheastCon 2005, Ft. Lauderdale, FL, USA, 8–10 April 2005; pp. 179–182. [Google Scholar]
- Islam, M.N.; Yuce, M.R. Review of Medical Implant Communication System (MICS) band and network. ICT Express 2016, 2, 188–194. [Google Scholar] [CrossRef]
- Poon, C.C.Y.; Zhang, Y.-T.; Bao, S.-D. A novel biometrics method to secure wireless body area sensor networks for telemedicine and m-health. IEEE Commun. Mag. 2006, 44, 73–81. [Google Scholar] [CrossRef]
- Yuce, M.R.; Ng, S.W.; Myo, N.L.; Khan, J.Y.; Liu, W. Wireless body sensor network using medical implant band. J. Med. Syst. 2007, 31, 467–474. [Google Scholar] [CrossRef]
- Yuce, M.R.; Chee Keong, H. Implementation of body area networks based on MICS/WMTS medical bands for healthcare systems. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 3417–3421. [Google Scholar]
- Ho, M.; Wang, J.; Shelby, K.; Haisch, H. IEEE 802.11g OFDM WLAN throughput performance. In Proceedings of the 2003 IEEE 58th Vehicular Technology Conference, VTC 2003-Fall (IEEE Cat. No.03CH37484), Orlando, FL, USA, 6–9 October 2003; Volume 4, pp. 2252–2256. [Google Scholar]
- IEEE Standard for Information technology-Telecommunications and Information Exchange between Systems Local and Metropolitan Area Networks-Specific Requirements—Part 11: Wireless LAN Medium Access Control (MAC) and Physical Layer (PHY) Specifications; IEEE Std 802.11-2016 (Revision of IEEE Std 802.11-2012); IEEE: Piscataway, PA, USA, 2016; pp. 1–3534.
- Au, L.K.; Wu, W.H.; Batalin, M.A.; McIntire, D.H.; Kaiser, W.J. MicroLEAP: Energy-aware Wireless Sensor Platform for Biomedical Sensing Applications. In Proceedings of the IEEE Biomedical Circuits and Systems Conference, Montreal, QC, Canada, 27–30 November 2007; pp. 158–162. [Google Scholar]
- Isaacson, M.J.; Hollandsworth, R.P.; Giampaoli, P.J.; Linkowsky, F.A.; Salim, A.; Teofilo, V.L. Advanced lithium ion battery charger. In Proceedings of the Fifteenth Annual Battery Conference on Applications and Advances (Cat. No.00TH8490), Long Beach, CA, USA, 11–14 January 2000; pp. 193–198. [Google Scholar]
- Chatterjee, S.; Thakur, R.S.; Yadav, R.N.; Gupta, L.; Raghuvanshi, D.K. Review of noise removal techniques in ECG signals. IET Signal Process. 2020, 14, 569–590. [Google Scholar] [CrossRef]
- Joshi, S.L.; Vatti, R.A.; Tornekar, R.V. A Survey on ECG Signal Denoising Techniques. In Proceedings of the International Conference on Communication Systems and Network Technologies, Gwalior, India, 6–8 April 2013; pp. 60–64. [Google Scholar] [CrossRef]
- Nussbaumer, H.J. The Fast Fourier Transform. In Fast Fourier Transform and Convolution Algorithms; Springer: Berlin/Heidelberg, Germany, 1981; pp. 80–111. [Google Scholar]
- Lin, H.Y.; Liang, S.Y.; Ho, Y.L.; Lin, Y.H.; Ma, H.P. Discrete-wavelet-transform-based noise removal and feature extraction for ECG signals. IRBM 2014, 35, 351–361. [Google Scholar] [CrossRef]
- Thakor, N.V.; Zhu, Y. Applications of adaptive filtering to ECG analysis: Noise cancellation and arrhythmia detection. IEEE Trans. Biomed. Eng. 1991, 38, 785–794. [Google Scholar] [CrossRef] [PubMed]
- AlMahamdy, M.; Riley, H.B. Performance Study of Different Denoising Methods for ECG Signals. Procedia Comput. Sci. 2014, 37, 325–332. [Google Scholar] [CrossRef]
- Widrow, B.; Glover, J.R.; McCool, J.M.; Kaunitz, J.; Williams, C.S.; Hearn, R.H.; Zeidler, J.R.; Eugene Dong, J.; Goodlin, R.C. Adaptive noise cancelling: Principles and applications. Proc. IEEE 1975, 63, 1692–1716. [Google Scholar] [CrossRef]
- Haykin, S.S. Adaptive Filter Theory; Pearson Education India: Delhi, India, 2008. [Google Scholar]
- Douglas, S.C. Introduction to adaptive filters. In Digital Signal Processing Handbook; Madisetti, V.K., Williams, D.B., Eds.; CRC Press LLC.: Boca Raton, FL, USA, 1999. [Google Scholar]
- Ahlstrom, M.L.; Tompkins, W.J. Digital Filters for Real-Time ECG Signal Processing Using Microprocessors. IEEE Trans. Biomed. Eng. 1985, BME-32, 708–713. [Google Scholar] [CrossRef]
- Proakis, J.G.; Salehi, M. Digital Communications, 5th ed.; McGraw-Hill Education: New York, NY, USA, 2007. [Google Scholar]
- Savitzky, A.; Golay, M.J.E. Smoothing and Differentiation of Data by Simplified Least Squares Procedures. Anal. Chem. 1964, 36, 1627–1639. [Google Scholar] [CrossRef]
- Schafer, R.W. What Is a Savitzky-Golay Filter? [Lecture Notes]. IEEE Signal Process. Mag. 2011, 28, 111–117. [Google Scholar] [CrossRef]
- Lord, N. Matrix Computations, 3rd ed.; Golub, G.H., Loan, C.F.V., Eds.; Johns Hopkins University Press: Baltimore, MD, USA, 1999; Volume 83. [Google Scholar]
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef]
- Dhawan, A.; Wenzel, B.; George, S.; Gussak, I.; Bojovic, B.; Panescu, D. Detection of Acute Myocardial Infarction from serial ECG using multilayer support vector machine. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 2704–2707. [Google Scholar]
- Lillo-Castellano, J.M.; Mora-Jimenez, I.; Santiago-Mozos, R.; Chavarria-Asso, F.; Cano-Gonzalez, A.; Garcia-Alberola, A.; Rojo-Alvarez, J.L. Symmetrical Compression Distance for Arrhythmia Discrimination in Cloud-Based Big-Data Services. IEEE J. Biomed. Health Inf. 2015, 19, 1253–1263. [Google Scholar] [CrossRef]
- Abdar, M.; Książek, W.; Acharya, U.R.; Tan, R.S.; Makarenkov, V.; Pławiak, P. A new machine learning technique for an accurate diagnosis of coronary arterytery disease. Comput. Methods Programs Biomed. 2019, 179, 104992. [Google Scholar] [CrossRef]
- Devadharshini, M.S.; Heena Firdaus, A.S.; Sree Ranjani, R.; Devarajan, N. Real Time Arrhythmia Monitoring with Machine Learning Classification and IoT. In Proceedings of the 2019 International Conference on Data Science and Engineering (ICDSE), Patna, India, 26–28 September 2019; pp. 1–4. [Google Scholar]
- Shao, M.; Zhou, Z.; Bin, G.; Bai, Y.; Wu, S. A Wearable Electrocardiogram Telemonitoring System for Atrial Fibrillation Detection. Sensors 2020, 20, 606. [Google Scholar] [CrossRef]
- Hall, L.O.; Chawla, N.; Bowyer, K.W. Decision tree learning on very large data sets. In Proceedings of the SMC’98 Conference Proceedings. 1998 IEEE International Conference on Systems, Man, and Cybernetics (Cat. No. 98CH36218), San Diego, CA, USA, 14 October 1998; Volume 3, pp. 2579–2584. [Google Scholar] [CrossRef]
- Shao, M.; Bin, G.; Wu, S.; Bin, G.; Huang, J.; Zhou, Z. Detection of atrial fibrillation from ECG recordings using decision tree ensemble with multi-level features. Physiol. Meas. 2018, 39, 094008. [Google Scholar] [CrossRef] [PubMed]
- Mandala, S.; Cai Di, T.; Sunar, M.S.; Adiwijaya. ECG-based prediction algorithm for imminent malignant ventricular arrhythmias using decision tree. PLoS ONE 2020, 15, e0231635. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Chuang, C.; Yen, C.; Huang, S.; Chen, J.; Lee, S. An AIoT Wearable ECG Patch with Decision Tree for Arrhythmia Analysis. In Proceedings of the IEEE Biomedical Circuits and Systems Conference (BioCAS), Nara, Japan, 17–19 October 2019; pp. 1–4. [Google Scholar] [CrossRef]
- Hyvärinen, A.; Oja, E. Independent component analysis: Algorithms and applications. Neural Netw. 2000, 13, 411–430. [Google Scholar] [CrossRef]
- Barhatte, A.S.; Ghongade, R.; Tekale, S.V. Noise analysis of ECG signal using fast ICA. In Proceedings of the Conference on Advances in Signal Processing (CASP), Shanghai, China, 20–25 March 2016; pp. 118–122. [Google Scholar] [CrossRef]
- Gupta, V.; Mittal, M.; Mittal, V. R-peak detection based chaos analysis of ECG signal. Analog. Integr. Circuits Signal Process. 2020, 102, 479–490. [Google Scholar] [CrossRef]
- Mirza, S.; Bhole, K.; Singh, P. Fetal ECG Extraction and QRS Detection using Independent Component Analysis. In Proceedings of the 16th IEEE International Colloquium on Signal Processing Its Applications (CSPA), Langkawi, Malaysia, 28–29 February 2020; pp. 157–161. [Google Scholar] [CrossRef]
- Jain, A.K. Data clustering: 50 years beyond K-means. Pattern Recognit. Lett. 2010, 31, 651–666. [Google Scholar] [CrossRef]
- Balouchestani, M.; Krishnan, S. Advanced K-means clustering algorithm for large ECG data sets based on a collaboration of compressed sensing theory and K-SVD approach. Signal Image Video Process. 2016, 10, 113–120. [Google Scholar] [CrossRef]
- Peterson, L.E. K-nearest neighbor. Scholarpedia 2009, 4, 1883. [Google Scholar] [CrossRef]
- Venkatesan, C.; Karthigaikumar, P.; Varatharajan, R. A novel LMS algorithm for ECG signal preprocessing and KNN classifier based abnormality detection. Multimed. Tools Appl. 2018, 77, 10365–10374. [Google Scholar] [CrossRef]
- Bouaziz, F.; Boutana, D.; Oulhadj, H. Diagnostic of ECG Arrhythmia using Wavelet Analysis and K-Nearest Neighbor Algorithm. In Proceedings of the International Conference on Applied Smart Systems (ICASS), Medea, Algeria, 24–25 November 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Altman, N.; Krzywinski, M. Simple linear regression. Nat. Methods 2015, 12, 999–1000. [Google Scholar] [CrossRef]
- Aspuru, J.; Ochoa-Brust, A.; Felix, R.A.; Mata-Lopez, W.; Mena, L.J.; Ostos, R.; Martinez-Pelaez, R. Segmentation of the ECG Signal by Means of a Linear Regression Algorithm. Sensors 2019, 19, 775. [Google Scholar] [CrossRef]
- Zhou, S.; Abdel Wahab, A.; Sapp, J.L.; Warren, J.W.; Horáček, B.M. Localization of ventricular activation origin from the 12-lead ECG: A comparison of linear regression with non-linear methods of machine learning. Ann. Biomed. Eng. 2019, 47, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Loog, M. A benchmark and comparison of active learning for logistic regression. Pattern Recognit. 2018, 83, 401–415. [Google Scholar] [CrossRef]
- Cai, L.; Chen, C.; Wang, X.; Yang, X.; Lin, S.; Huang, J.; Jiang, J.; Datta, R.; Du, M.; Jiang, H.; et al. Sleep Disorder Classification Method based on Logistic Regression with Apnea-ECG Dataset. In Proceedings of the International Conference on Artificial Intelligence and Advanced Manufacturing, Dublin, Ireland, 16–18 October 2019; pp. 1–4. [Google Scholar]
- Lazaric, A.; Restelli, M.; Bonarini, A. Reinforcement learning in continuous action spaces through sequential monte carlo methods. Adv. Neural Inf. Process. Syst. 2007, 20, 833–840. [Google Scholar]
- Bartocci, E.; Bortolussi, L.; Sanguinetti, G. Learning temporal logical properties discriminating ECG models of cardiac arrhytmias. arXiv 2013, arXiv:1312.7523. [Google Scholar]
- Abdi, H.; Williams, L.J. Principal component analysis. WIREs Comput. Stat. 2010, 2, 433–459. [Google Scholar] [CrossRef]
- Langley, P.; Bowers, E.J.; Murray, A. Principal Component Analysis as a Tool for Analyzing Beat-to-Beat Changes in ECG Features: Application to ECG-Derived Respiration. IEEE Trans. Biomed. Eng. 2010, 57, 821–829. [Google Scholar] [CrossRef]
- Sadr, N.; de Chazal, P. A Fast Principal Component Analysis Method For Calculating The ECG Derived Respiration. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; pp. 5294–5297. [Google Scholar] [CrossRef]
- Gupta, V.; Mittal, M. R-Peak Detection in ECG Signal Using Yule-Walker and Principal Component Analysis. IETE J. Res. 2019, 1–14. [Google Scholar] [CrossRef]
- Watkins, C.J.; Dayan, P. Q-learning. Mach. Learn. 1992, 8, 279–292. [Google Scholar] [CrossRef]
- Insani, A.; Jatmiko, W.; Sugiarto, A.T.; Jati, G.; Wibowo, S.A. Investigation Reinforcement Learning Method for R-Wave Detection on Electrocardiogram Signal. In Proceedings of the International Seminar on Research of Information Technology and Intelligent Systems (ISRITI), Yogyakarta, Indonesia, 5–6 December 2019; pp. 420–423. [Google Scholar] [CrossRef]
- Khoshgoftaar, T.M.; Golawala, M.; Hulse, J.V. An Empirical Study of Learning from Imbalanced Data Using Random Forest. In Proceedings of the 19th IEEE International Conference on Tools with Artificial Intelligence (ICTAI 2007), Patras, Greece, 29–31 October 2007; Volume 2, pp. 310–317. [Google Scholar] [CrossRef]
- Zabihi, M.; Rad, A.B.; Katsaggelos, A.K.; Kiranyaz, S.; Narkilahti, S.; Gabbouj, M. Detection of atrial fibrillation in ECG hand-held devices using a random forest classifier. In Proceedings of the Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Mahajan, R.; Kamaleswaran, R.; Howe, J.A.; Akbilgic, O. Cardiac rhythm classification from a short single lead ECG recording via random forest. In Proceedings of the Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Manibardo, E.; Irusta, U.; Ser, J.D.; Aramendi, E.; Isasi, I.; Olabarria, M.; Corcuera, C.; Veintemillas, J.; Larrea, A. ECG-based Random Forest Classifier for Cardiac Arrest Rhythms. In Proceedings of the 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1504–1508. [Google Scholar] [CrossRef]
- Rummery, G.A.; Niranjan, M. On-Line Q-Learning Using Connectionist Systems; University of Cambridge, Department of Engineering: Cambridge, UK, 1994; Volume 37. [Google Scholar]
- Levy, A.E.; Biswas, M.; Weber, R.; Tarakji, K.; Chung, M.; Noseworthy, P.A.; Newton-Cheh, C.; Rosenberg, M.A. Applications of machine learning in decision analysis for dose management for dofetilide. PLoS ONE 2020, 14, e0227324. [Google Scholar] [CrossRef]
- Klema, V.; Laub, A. The singular value decomposition: Its computation and some applications. IEEE Trans. Autom. Control. 1980, 25, 164–176. [Google Scholar] [CrossRef]
- Liu, T.Y.; Lin, K.J.; Wu, H.C. ECG Data Encryption Then Compression Using Singular Value Decomposition. IEEE J. Biomed. Health Inf. 2018, 22, 707–713. [Google Scholar] [CrossRef]
- Kabir, S.S.; Rizve, M.N.; Hasan, M.K. ECG signal compression using data extraction and truncated singular value decomposition. In Proceedings of the IEEE Region 10 Humanitarian Technology Conference (R10-HTC), Bangladesh, Dhaka, 21–23 December 2017; pp. 5–7. [Google Scholar] [CrossRef]
- Kumar, R.; Kumar, A.; Singh, G.K. Hybrid method based on singular value decomposition and embedded zero tree wavelet technique for ECG signal compression. Comput. Methods Programs Biomed. 2016, 129, 135–148. [Google Scholar] [CrossRef]
- Noble, W.S. What is a support vector machine? Nat. Biotechnol. 2006, 24, 1565–1567. [Google Scholar] [CrossRef]
- Oresko, J.J.; Jin, Z.; Cheng, J.; Huang, S.; Sun, Y.; Duschl, H.; Cheng, A.C. A Wearable Smartphone-Based Platform for Real-Time Cardiovascular Disease Detection Via Electrocardiogram Processing. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gui, Q.; Liu, B.; Jin, Z.; Chen, Y. Enabling Smart Personalized Healthcare: A Hybrid Mobile-Cloud Approach for ECG Telemonitoring. IEEE J. Biomed. Health Inf. 2014, 18, 739–745. [Google Scholar] [CrossRef]
- Venkatesan, C.; Karthigaikumar, P.; Satheeskumaran, S. Mobile cloud computing for ECG telemonitoring and real-time coronary heart disease risk detection. Biomed. Signal Process. Control. 2018, 44, 138–145. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, J. Application of Heartbeat-Attention Mechanism for Detection of Myocardial Infarction Using 12-Lead ECG Records. Appl. Sci. 2019, 9, 3328. [Google Scholar] [CrossRef]
- Sakib, S.; Fouda, M.M.; Fadlullah, Z.M.; Nasser, N. Migrating Intelligence from Cloud to Ultra-Edge Smart IoT Sensor Based on Deep Learning: An Arrhythmia Monitoring Use-Case. In Proceedings of the 2020 International Wireless Communications and Mobile Computing (IWCMC), Limassol, Cyprus, 15–19 June 2020; pp. 595–600. [Google Scholar]
- Huda, N.; Khan, S.; Abid, R.; Shuvo, S.B.; Labib, M.M.; Hasan, T. A Low-cost, Low-energy Wearable ECG System with Cloud-Based Arrhythmia Detection. medRxiv 2020. [Google Scholar] [CrossRef]
- Jain, A.K.; Jianchang, M.; Mohiuddin, K.M. Artificial neural networks: A tutorial. Computer 1996, 29, 31–44. [Google Scholar] [CrossRef]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef]
- Medsker, L.R.; Jain, L. Recurrent Neural Networks. Design and Applications; CRC Press: Boca Raton, FL, USA; London, UK; New York, NY, USA; Washington, DC, USA, 2001. [Google Scholar]
- Prabhakararao, E.; Dandapat, S. Myocardial Infarction Severity Stages Classification From ECG Signals Using Attentional Recurrent Neural Network. IEEE Sens. J. 2020, 20, 8711–8720. [Google Scholar] [CrossRef]
- Cheng, M.; Sori, W.J.; Jiang, F.; Khan, A.; Liu, S. Recurrent Neural Network Based Classification of ECG Signal Features for Obstruction of Sleep Apnea Detection. In Proceedings of the IEEE International Conference on Computational Science and Engineering (CSE) and IEEE International Conference on Embedded and Ubiquitous Computing (EUC), Guangzhou, China, 21–24 July 2017; Volume 2, pp. 199–202. [Google Scholar] [CrossRef]
- Xie, P.; Wang, G.; Zhang, C.; Chen, M.; Yang, H.; Lv, T.; Sang, Z.; Zhang, P. Bidirectional Recurrent Neural Network And Convolutional Neural Network (BiRCNN) For ECG Beat Classification. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; pp. 2555–2558. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef] [PubMed]
- Saadatnejad, S.; Oveisi, M.; Hashemi, M. LSTM-Based ECG Classification for Continuous Monitoring on Personal Wearable Devices. IEEE J. Biomed. Health Inf. 2020, 24, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Hou, B.; Yang, J.; Wang, P.; Yan, R. LSTM-Based Auto-Encoder Model for ECG Arrhythmias Classification. IEEE Trans. Instrum. Meas. 2020, 69, 1232–1240. [Google Scholar] [CrossRef]
- Yao, Q.; Wang, R.; Fan, X.; Liu, J.; Li, Y. Multi-class Arrhythmia detection from 12-lead varied-length ECG using Attention-based Time-Incremental Convolutional Neural Network. Inf. Fusion 2020, 53, 174–182. [Google Scholar] [CrossRef]
- Liu, F.; Liu, C.; Zhao, L.; Zhang, X.; Wu, X.; Xu, X.; Liu, Y.; Ma, C.; Wei, S.; He, Z.; et al. An Open Access Database for Evaluating the Algorithms of Electrocardiogram Rhythm and Morphology Abnormality Detection. J. Med. Imaging Health Inf. 2018, 8, 1368–1373. [Google Scholar] [CrossRef]
- Lu, Y.; Xu, X.; Xu, J. Development of a Hybrid Manufacturing Cloud. J. Manuf. Syst. 2014, 33, 551–566. [Google Scholar] [CrossRef]
- Amazon, E. Amazon Web Services. 2015. Available online: http://aws.amazon.com/es/ec2/ (accessed on 21 December 2020).
- Ifrah, S. Get Started with Microsoft Azure. In Getting Started with Containers in Azure; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–26. [Google Scholar]
- Bisong, E. Google AutoML: Cloud Natural Language Processing. In Building Machine Learning and Deep Learning Models on Google Cloud Platform; Springer: Berlin/Heidelberg, Germany, 2019; pp. 599–612. [Google Scholar]
- Vashist, S.K.; Schneider, E.M.; Luong, J.H. Commercial Smartphone-Based Devices and Smart Applications for Personalized Healthcare Monitoring and Management. Diagnostics 2014, 4, 104–128. [Google Scholar] [CrossRef]
- Pandey, S.; Voorsluys, W.; Niu, S.; Khandoker, A.; Buyya, R. An autonomic cloud environment for hosting ECG data analysis services. Future Gener. Comput. Syst. 2012, 28, 147–154. [Google Scholar] [CrossRef]
- Pandey, S.; Voorsluys, W.; Rahman, M.; Buyya, R.; Dobson, J.E.; Chiu, K. A grid workflow environment for brain imaging analysis on distributed systems. Concurr. Comput. Pract. Exp. 2009, 21, 2118–2139. [Google Scholar] [CrossRef]
- Vecchiola, C.; Chu, X.; Buyya, R. Aneka: A software platform for .NET-based cloud computing. High Speed Large Scale Sci. Comput. 2009, 18, 267–295. [Google Scholar]
- Lin, Y.; Hu, Y.H. Power-Line Interference Detection and Suppression in ECG Signal Processing. IEEE Trans. Biomed. Eng. 2008, 55, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Sannino, G.; De Pietro, G. A deep learning approach for ECG-based heartbeat classification for arrhythmia detection. Future Gener. Comput. Syst. 2018, 86, 446–455. [Google Scholar] [CrossRef]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65. [Google Scholar] [CrossRef]
- Son, J.; Park, J.; Oh, H.; Bhuiyan, M.Z.A.; Hur, J.; Kang, K. Privacy Preserving Electrocardiogram Monitoring for Intelligent Arrhythmia Detection. Sensors 2017, 17, 1360. [Google Scholar] [CrossRef]
- Ibaida, A.; Khalil, I. Wavelet-Based ECG Steganography for Protecting Patient Confidential Information in Point-of-Care Systems. IEEE Trans. Biomed. Eng. 2013, 60, 3322–3330. [Google Scholar] [CrossRef]
- Lee, W.; Lee, C. A Cryptographic Key Management Solution for HIPAA Privacy/Security Regulations. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 34–41. [Google Scholar] [CrossRef]
- Wang, H.; Peng, D.; Wang, W.; Sharif, H.; Chen, H.; Khoynezhad, A. Resource-aware secure ECG healthcare monitoring through body sensor networks. IEEE Wirel. Commun. 2010, 17, 12–19. [Google Scholar] [CrossRef]
- Lazzeretti, R.; Guajardo, J.; Barni, M. Privacy Preserving ECG Quality Evaluation. In Proceedings of the on Multimedia and Security; Association for Computing Machinery: New York, NY, USA, 2012; Volume 12, pp. 165–174. [Google Scholar] [CrossRef]
- Page, A.; Kocabas, O.; Soyata, T.; Aktas, M.; Couderc, J.P. Cloud-Based Privacy Preserving Remote ECG Monitoring and Surveillance. Ann. Noninvasive Electrocardiol. 2015, 20, 328–337. [Google Scholar] [CrossRef]
- Chou, C.; Chang, E.; Li, H.; Wu, A. Low-Complexity Privacy Preserving Compressive Analysis Using Subspace-Based Dictionary for ECG Telemonitoring System. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 801–811. [Google Scholar] [CrossRef]
- Rahimi Moosavi, S.; Nigussie, E.; Levorato, M.; Virtanen, S.; Isoaho, J. Low-Latency Approach for Secure ECG Feature Based Cryptographic Key Generation. IEEE Access 2018, 6, 428–442. [Google Scholar] [CrossRef]
- Huang, P.; Guo, L.; Li, M.; Fang, Y. Practical Privacy Preserving ECG-Based Authentication for IoT-Based Healthcare. IEEE Internet Things J. 2019, 6, 9200–9210. [Google Scholar] [CrossRef]
- Ibaida, A.; Abuadbba, A.; Chilamkurti, N. Privacy preserving compression model for efficient IoMT ECG sharing. Comput. Commun. 2020, 166, 1–8. [Google Scholar] [CrossRef]
- Xu, G. IoT-Assisted ECG Monitoring Framework With Secure Data Transmission for Health Care Applications. IEEE Access 2020, 8, 74586–74594. [Google Scholar] [CrossRef]
- Tariq, N.; Qamar, A.; Asim, M.; Khan, F.A. Blockchain and Smart Healthcare Security: A Survey. Procedia Comput. Sci. 2020, 175, 615–620. [Google Scholar] [CrossRef]
- Chenthara, S.; Ahmed, K.; Wang, H.; Whittaker, F. Security and privacy preserving challenges of e-health solutions in cloud computing. IEEE Access 2019, 7, 74361–74382. [Google Scholar] [CrossRef]
- Trigo, J.D.; Alesanco, A.; Martinez, I.; Garcia, J. A Review on Digital ECG Formats and the Relationships Between Them. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 432–444. [Google Scholar] [CrossRef]
- Nakayama, M.; Takehana, K.; Kohro, T.; Matoba, T.; Tsutsui, H.; Nagai, R.; on behalf of the IHE Cardiology Team and SEAMAT Committee. Standard Export Data Format for Extension Storage of Standardized Structured Medical Information Exchange. Circ. Rep. 2020, 2, 587–616. [Google Scholar] [CrossRef]
- Wagner, P.; Strodthoff, N.; Bousseljot, R.D.; Kreiseler, D.; Lunze, F.I.; Samek, W.; Schaeffter, T. PTB-XL, a large publicly available electrocardiography dataset. Sci. Data 2020, 7, 1–15. [Google Scholar] [CrossRef]
- Brown, B.; Kohls, M.; Stockbridge, N. FDA XML Data Format Design Specification; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2002.
- Rubel, P.; Pani, D.; Schloegl, A.; Fayn, J.; Badilini, F.; Macfarlane, P.W.; Varri, A. SCP-ECG V3.0: An enhanced standard communication protocol for computer-assisted electrocardiography. In Proceedings of the Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016; pp. 309–312. [Google Scholar]
- Committee Nihon Kohden Corp. Medical Waveform Description Format Encoding Rules; MFER Part I, Version; Committee Nihon Kohden Corp: Tokyo, Japan, 2011. [Google Scholar]
- Committee, D.S. Working Group 1-Cardiac and Vascular Information: Digital Imaging and Communications in Medicine (DICOM) Supplement 30: Waveform Interchange. 2000. Available online: http://dicom.nema.org/Dicom/supps/sup30_lb.pdf (accessed on 2 December 2020).
- Zywietz, C. Standardized representation of vital signs for continuous care in cardiology. In Proceedings of the Computers in Cardiology 1998. Vol. 25 (Cat. No.98CH36292), Cleveland, OH, USA, 13–16 September 1998; pp. 205–208. [Google Scholar]
- Värri, A. ENV 14271, File Exchange Format for Vital Signs and its use in digital ECG archiving. In Proceedings of the OpenECG Workshop Integration of the ECG into EHR and Interoperability of ECG Device Systems, Berlin, Germany, 1–3 April 2004. [Google Scholar]
- ISO. Health Informatics: Point-of-Care Medical Device Communication. Nomenclature; IEEE: Piscataway, PA, USA, 2004. [Google Scholar]
- Zareba, W.; Locati, E.; Maison Blanche, P. The ISHNE holter standard output file format : A step toward compatibility of holter systems. Ann. Noninvasive Electrocardiol. 1998. [Google Scholar] [CrossRef]
- Badilini, F. The ISHNE holter standard output file format. Ann. Noninvasive Electrocardiol. 1998, 3, 263–266. [Google Scholar] [CrossRef]
- Herrera, R.E.; Cain, J.T.; Cape, E.G.; Boyle, G.J. A high resolution ECG tool for detection of atrial and ventricular late potentials. In Proceedings of the Computers in Cardiology, Indianapolis, IN, USA, 8–11 September 1996; pp. 629–632. [Google Scholar]
- Fortner, B. HDF: The hierarchical data format. Dr. Dobb’s J Softw. Tools Prof Program 1998, 23, 42. [Google Scholar]
- Mandellos, G.J.; Koukias, M.N.; Lymberopoulos, D.K. Structuring the e-SCP-ECG+ protocol for multi vital-sign handling. In Proceedings of the 8th IEEE International Conference on BioInformatics and BioEngineering, Athens, Greece, 8–10 October 2008; pp. 1–6. [Google Scholar]
- Long, N. Open ECG data standard: Philips medical systems perspective. J. Electrocardiol. 2003, 36, 167. [Google Scholar] [CrossRef]
- Helfenbein, E.; Gregg, R.; Zhou, S. Philips Medical Systems support for open access and use of electrocardiographic data. J. Electrocardiol. 2005, 38, 35. [Google Scholar] [CrossRef]
- Zhou, S.; Helfenbein, E. OpenECG Format, Philips Experience. In Proceedings of the OpenECG Workshop Proceeding, Berlin, Germany, 1–3 April 2004. [Google Scholar]
- Connelly, P. I-Med Exchange Evaluation. IAPAC MONTHLY 2002, 8, 142–150. [Google Scholar]
- Wang, H.; Azuaje, F.; Jung, B.; Black, N. A markup language for electrocardiogram data acquisition and analysis (ecgML). BMC Med. Inf. Decis. Mak. 2003, 3, 4. [Google Scholar] [CrossRef]
- Lu, X.; Duan, H.; Zheng, H. XML-ECG: An XML-Based ECG Presentation for Data Exchanging. In Proceedings of the 1st International Conference on Bioinformatics and Biomedical Engineering, Wuhan, China, 6–8 July 2007; pp. 1141–1144. [Google Scholar]
- Fang, Q.; Sufi, F.; Cosic, I. A mobile device based ECG analysis system. Data Min. Med. Biol. Res. 2008, 42, 217–222. [Google Scholar]
- Gonçalves, B.; Pereira Filho, J.G.; Andreão, R.V. ECGWARE: An ECG Markup Language for Ambulatory Telemonitoring and Decision Making Support. HEALTHINF 2008, 2, 37–43. [Google Scholar]
- Kirst, M.; Ottenbacher, J.; Nedkov, R. UNISENS—Ein Universelles Datenformat for Multisensordaten (UNISENS—A Universal Data Format for Multi-Sensor Data); Workshop Biosignalverarbeitung, Universität Potsdam: Potsdam, Germany, 2008. [Google Scholar]
- Bond, R.R.; Finlay, D.D.; Nugent, C.D.; Moore, G. XML-BSPM: An XML format for storing Body Surface Potential Map recordings. BMC Med. Inf. Decis. Mak. 2010, 10, 28. [Google Scholar] [CrossRef]
- Bond, R.R.; Finlay, D.D.; Nugent, C.D.; Moore, G. A Web-based tool for processing and visualizing body surface potential maps. J. Electrocardiol. 2010, 43, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Kemp, B.; Värri, A.; Rosa, A.C.; Nielsen, K.D.; Gade, J. A simple format for exchange of digitized polygraphic recordings. Electroencephalogr. Clin. Neurophysiol. 1992, 82, 391–393. [Google Scholar] [CrossRef]
- Kemp, B.; Olivan, J. European data format ’plus’ (EDF+), an EDF alike standard format for the exchange of physiological data. Clin. Neurophysiol. 2003, 114, 1755–1761. [Google Scholar] [CrossRef]
- Schlögl, A. An overview on data formats for biomedical signals. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Munich, Germany, 7–12 September 2009; pp. 1557–1560. [Google Scholar]
- OpenXDF Consortium, Open eXchange Data Format Specification. 2008. Available online: http://www.openxdf.org/specs/OpenXDF_Specification_1.0.pdf (accessed on 2 December 2020).
- Jacobs, E.C.; Lagerlund, T.D.; Collura, T.F.; Burgess, R.C. A standard for transfer of digital neurophysiological data. In Proceedings of the 14th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Paris, France, 29 October–1 November 1992; Volume 3, pp. 1236–1237. [Google Scholar]
- Cunha, M.B.; Cunha, J.P.; Oliveira e Silva, T. SIGIF: A digiw signal interchange format for biological signals. In Proceedings of the 15th Annual International Conference of the IEEE Engineering in Medicine and Biology Societ, San Diego, CA, USA, 31 October 1993; pp. 644–645. [Google Scholar]
- Hellmann, G.; Kuhn, M.; Prosch, M.; Spreng, M. Extensible biosignal (EBS) file format: Simple method for EEG data exchange. Electroencephalogr. Clin. Neurophysiol. 1996, 99, 426–431. [Google Scholar] [CrossRef]
- Kuhn, M. EBS-Extensible Bio-Signal File Format. 2007. Available online: https://www.cl.cam.ac.uk/~mgk25/ebs/ (accessed on 21 December 2020).
- Durka, P.J.; Ircha, D. SignalML: Metaformat for description of biomedical time series. Comput. Methods Programs Biomed. 2004, 76, 253–259. [Google Scholar] [CrossRef]
- Rector, D.; Burk, P.; Harper, R.M. A data acquisition system for long-term monitoring of physiological and video signals. Electroencephalogr. Clin. Neurophysiol. 1993, 87, 380–384. [Google Scholar] [CrossRef]
- American Heart Association ECG Database USB. Available online: https://www.ecri.org/american-heart-association-ecg-database-usb (accessed on 13 October 2020).
- Party, T.C.W. Recommendations for measurement standards in quantitative electrocardiography. Eur. Heart J. 1985, 6, 815–825. [Google Scholar]
- Willems, J.L.; Arnaud, P.; van Bemmel, J.H.; Bourdillon, P.J.; Degani, R.; Denis, B.; Harms, F.M.; Macfarlane, P.W.; Mazzocca, G.; Meyer, J.; et al. Establishment of a reference library for evaluating computer ECG measurement programs. Comput. Biomed. Res. 1985, 18, 439–457. [Google Scholar] [CrossRef]
- Willems, J.; Arnaud, P.; Van Bemmel, J.; Degani, R.; Macfarlane, P.; Zywietz, C. Common standards for quantitative electrocardiography: Goals and main results. Methods Inf. Med. 1990, 29, 263–271. [Google Scholar]
- ACC, H. RSNA: IHE Cardiology Technical Framework Year 2: 2005–2006 Volume Integration Profiles Revision 2.1 Final Text Version.
- IHE Cardiology Technical Framework Supplement. Resting ECG Workflow (REWF). Available online: www.ihe.net/Technical_Framework/upload/IHE_CARD_Suppl_REWF_Rev1-1_TI_2010-07-30.pdf (accessed on 14 October 2020).
- IHE Cardiology Technical Framework Supplement. Waveform Communication Management (WCM). Available online: www.ihe.net/Technical_Framework/upload/IHE_PCD_Suppl_WCM.pdf (accessed on 14 October 2020).
- Kokkinaki, A.; Chouvarda, I.; Maglaveras, N. Integrating SCP-ECG files and patient records: An ontology based approach. Inf. Technol. Appl. Biomed. 2006. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.127.2502&rep=rep1&type=pdf (accessed on 2 December 2020).
- Kokkinaki, A.; Chouvarda, I.; Maglaveras, N. An ontology-based approach facilitating unified querying of biosignals and patient records. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 21–24 August 2008; pp. 2861–2864. [Google Scholar]
- Whetzel, P.L.; Noy, N.F.; Shah, N.H.; Alexander, P.R.; Nyulas, C.; Tudorache, T.; Musen, M.A. BioPortal: Enhanced functionality via new Web services from the National Center for Biomedical Ontology to access and use ontologies in software applications. Nucleic Acids Res. 2011, 39, W541–W545. [Google Scholar] [CrossRef]
- Gonçalves, B. An Ontological Theory of the Electrocardiogram with Applications. Master’s Thesis, Universidade Federal Do Espírito Santo, Vitória, Brazil, 2009. [Google Scholar]
- Sakkalis, V.; Chiarugi, F.; Kostomanolakis, S.; Chronaki, C.E.; Tsiknakis, M.; Orphanoudakis, S.C. A gateway between the SCP-ECG and the DICOM supplement 30 waveform standard. In Proceedings of the Computers in Cardiology, Thessaloniki Chalkidiki, Greece, 21–24 September 2003; pp. 25–28. [Google Scholar]
- Wang, L.; Rao, N.; Pu, L.; Wang, G. Developing a DICOM Middleware to Implement ECG Conversion and Viewing. In Proceedings of the IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 31 August–3 September 2005; pp. 6953–6956. [Google Scholar]
- Helfenbein, E.D.; Gregg, R.; Zhou, S. Philips medical systems support for open ECG and standardization efforts. In Proceedings of the Computers in Cardiology, Chicago, IL, USA, 19–22 September 2004; pp. 393–396. [Google Scholar]
- Schloegl, A.; Chiarugi, F.; Cervesato, E.; Apostolopoulos, E.; Chronaki, C.E. Two-way converter between the HL7 aECG and SCP-ECG data formats using BioSig. In Proceedings of the Computers in Cardiology, Durham, NC, USA, 30 September–3 October 2007; pp. 253–256. [Google Scholar]
- Jumaa, H.; Fayn, J.; Rubel, P. XML based mediation for automating the storage of SCP-ECG data into relational databases. In Proceedings of the Computers in Cardiology, Bologna, Italy, 14–17 September 2008; pp. 445–448. [Google Scholar]
- Wang, H.; Azuaje, F.; Clifford, G.; Jung, B.; Black, N. Methods and tools for generating and managing ecgML-based information. In Proceedings of the Computers in Cardiology, Chicago, IL, USA, 19–22 September 2004; pp. 573–576. [Google Scholar]
- Trigo, J.D.; Chiarugi, F.; Alesanco, A.; Martinez-Espronceda, M.; Serrano, L.; Chronaki, C.E.; Escayola, J.; Martinez, I.; Garcia, J. Interoperability in Digital Electrocardiography: Harmonization of ISO/IEEE x73-PHD and SCP-ECG. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 1303–1317. [Google Scholar] [CrossRef] [PubMed]
- Zywietz, C.; Kraemer, M.; Fischer, R.; Widiger, B. Integrating the ECG enterprise-HES-EKG with the built-in vital signs information nomenclature. In Proceedings of the Computers in Cardiology, Chicago, IL, USA, 19–22 September 2004; pp. 41–44. [Google Scholar]
- Chiang, C.C.; Yang, Y.C.; Tzeng, W.C.; Tseng, W.D.; Hsieh, J.C. An SCP compatible 12-lead electrocardiogram database for signal transmission, storage, and analysis. In Proceedings of the Computers in Cardiology, Chicago, IL, USA, 19–22 September 2004; pp. 621–624. [Google Scholar]
- Chiang, C.C.; Tzeng, W.C.; Cheng, H.C.; Lin, C.T.; Yang, Y.C.; Liang, S.F.; Lim, S.B. Construction and Application of an Electronic ECG Management System. J. Inf. Technol. Appl. 2007, 2, 135–140. [Google Scholar]
- de Wijs, M.C.J.; van Ettinger, M.; Meij, S.H.; Nelwan, S.P. Integration of multiple ECG databases into a unified framework. In Proceedings of the Computers in Cardiology, Lyon, France, 25–28 September 2005; pp. 447–450. [Google Scholar]
- van Ettinger, M.J.B.; Lipton, J.A.; de Wijs, M.C.J.; van der Putten, N.; Nelwan, S.P. An open source ECG toolkit with DICOM. In Proceedings of the Computers in Cardiology, Bologna, Italy, 14–17 September 2008; pp. 441–444. [Google Scholar]
- Hsieh, J.C.; Lo, H.C. The clinical application of a PACS-dependent 12-lead ECG and image information system in E-medicine and telemedicine. J. Digit. Imaging 2010, 23, 501–513. [Google Scholar] [CrossRef]
- Trigo, J.; Kollmann, A.; González, A.; Hayn, D.; Alesanco, A.; Schreier, G.; García, J. A Framework for the Integration and Homogeneous Management of Electrocardiography Formats; Med-e-Tel: Luxembourg, 2010. [Google Scholar]
- Goncalves, B.; Guizzardi, G.; Pereira Filho, J.G. Using an ECG reference ontology for semantic interoperability of ECG data. J. Biomed. Inf. 2011, 44, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Lee, Y. Structure Conversion Between International Standards for ECG Storage. Adv. Sci. Lett. 2017, 23, 9667–9670. [Google Scholar] [CrossRef]
- Stamenov, D.; Gusev, M.; Armenski, G. Interoperability of ECG standards. In Proceedings of the 41st International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 21–25 May 2018; pp. 0319–0323. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CVD Type | Symptoms | Cause | Prevention Methods |
|---|---|---|---|
| Heart Attack | Discomfort, Indigestion, Sweating, Vomiting, Irregular heartbeats. | Artery plaques attributable to calcium, fatty matter, proteins, and cells which are inflammatory. | Narcotics (aspirin, brilinta, etc.)surgical procedure Processes-Angioplasty |
| Coronary Heart Disease | Chest pain, Aching, Heaviness | Pulmonary embolism, Cardiomyopathy, Pericarditis, | Angioplasty, Bypass surgery. |
| Ischemic stroke | Headache, paralysis, or facial numbness, leg and arm, trouble with talking | Blocked artery hemorrhagic stroke. | Carotid endarterectomy, Angioplasty |
| Arrhythmia | Palpitations, fainting, dizziness, weakness, fatigue. | Electrolyte’s incorrect balance in the blood, muscle changes in the heart | Medication, Change lifestyle, and surgery. |
| Heart valve Disease | Swelling of the feet, ankles, or abdomen, trouble with breathing and rapid gain in weight | Acquired valve disease, Congenital valve disease, Rheumatic fever | Medication, brush carefully to prevent teeth and gums infection |
| Enlarged Heart (Cardiomegaly) | Shortness of breath, weight gain, fatigue and leg swelling | Genetic and inherited conditions, infection of HIV, abnormal heart valve, high blood pressure. | Cardiac catheterization, high-blood regulation pressure, Avoiding the usage of harmful alcohol substances and caffeine |
| Heart Murmurs | High Blood Pressure and Anemia | Fever and hyperactive thyroid,. | Prevention of blood clots, surgery and diuretics through medicines |
| Cardiac Arrest | Racing Heartbeat, Dizziness | Abnormal Heart rhythms (Arrhythmia) | Consistently following-up with the doctors, surgery and medication |
| Attributes | Values |
|---|---|
| Age | — |
| Sex | 1 = Male, 0 = Female |
| cp: Chest pain type | 1 = Typical angina, 2 = Atypical angina, 3 = Non-anginal, 4 = Asymptomatic |
| Trestbps: Resting Blood; Pressure (in mm Hg) | |
| Chol: Serum cholesterol in mg/dL | |
| Fbs: fasting blood sugar >120 mg/dL | 1 = True, 0 = False |
| Restecg: resting electrocardiographic results | 0 = Normal, 1 = Having ST-T wave abnormality, 2 = Showing probable or definite left ventricular hypertrophy |
| Thalach: maximum heart rate achieved | |
| Exang: exercise-induced angina | 1 = Yes, 0 = No |
| Old speak: = ST depression induced by exercise relative to rest | |
| slope: the slope of the peak exercise ST segment | 1 = Up sloping, 2 = Flat, 3 = Down sloping |
| ca: number of major vessels (0–3) colored by fluoroscopy | |
| Thal: Heart condition summary | 3 = Normal, 6 = Fixed defect, 7 = Reversible defect |
| Num: Diagnosis of heart disease (angiographic disease status) | 0: <50% diameter narrowing 1: 50% diameter narrowing |
| ML Algorithm | ECG Applications | Learning Category | Summary |
|---|---|---|---|
| Decision Tree [95] | [96,97,98] | Supervised | Based on multiple input variables, the model utilizes a decision tree to predict the target variable’s value. |
| Independent Component Analysis [99] | [100,101,102] | Unsupervised | A method to divide independent sources from a mixed signal. |
| K-means clustering [103] | [104] | Unsupervised | A vector quantization method that divides multiple observations into k clusters where every observation relates to the nearest mean cluster. |
| k-Nearest neighbor classifier [105] | [91,106,107] | Supervised | The input comprises the k closest training instances of the specific feature, and the output is a class membership. Here, the object is attributed to the class most prevalent between its nearest k neighbors. |
| Linear regression [108] | [109,110] | Supervised | Model is trained based on two variables, that are correlated linearly on the x-axis and y-axis, to predict the behavior of the data. |
| Logistic regression [111] | [112] | Supervised | Based on the binary target variable, the probability of it being in either of the two clauses is predicted. |
| Monte Carlo [113] | [114] | Reinforcement | A method that carries out several random sampling to collect numerical results. |
| Principal Component Analysis [115] | [116,117,118] | Unsupervised | A dimensionality-reduction method that transforms an extensive set of variables into a smaller one while retaining most of the information available in the original set. |
| Q-learning [119] | [120] | Reinforcement | A technique to find an optimal policy to maximize the expected value of the total reward beginning from the current state to over any successive steps. |
| Random forest [121] | [93,122,123,124] | Supervised | Comprises several decision trees and to setup a forest of trees which is uncorrelated, utilizes bagging and feature randomness during individual tree creation. |
| SARSA [125] | [126] | Reinforcement | A technique to enable the learning of a Markov decision process policy |
| Singular Value Decomposition [127] | [128,129,130] | Unsupervised | A matrix factorization technique that decomposes a matrix into singular values and singular vectors. |
| Support vector machine [131] | [90,92] | Supervised | A technique to obtain a hyperplane that splits the data into different classes. |
| DL Algorithm | ECG Applications | Summary |
|---|---|---|
| Artificial neural network [138] | [132,133] | A technique to enable the simulation of the network of neurons, similar to a human brain, to automate the learning and decision making of a computer. |
| Convolutional neural network [139] | [136,137] | A type of ANN designed for pixel data processing and is most widely used for analyzing visual imagery. |
| Recurrent neural network [140] | [141,142,143] | A class of ANN that utilizes the previous step’s output as input for the current step. |
| Long short-term memory [144] | [135,145,146] | Recurrent neural networks that, in sequence prediction problems, can learn the order of dependence. |
| Work | Year | CVD Type | Denoising | AI Technique | AI Algorithm Used | Cloud Computing | SBDA-Based |
|---|---|---|---|---|---|---|---|
| [132] | 2010 | Arrhythmia | Bandpass filter | DL | Artificial neural network | Not utilized | Yes |
| [90] | 2012 | Myocardial infarction | — | ML | Support vector machine | Not utilized | No |
| [133] | 2014 | Arrhythmia | PLI detection and suppression [157] | DL | Artificial neural network | Utilized | No |
| [91] | 2015 | Arrhythmia | — | ML | k-Nearest Neighbors Classification | Utilized | No |
| [134] | 2018 | Coronary artery disease | Adaptive filter (LMS) | DL | Adaptive neuro fuzzy inference system | Utilized | No |
| [158] | 2018 | Arrhythmia | 1D-Median Filtering | DL | Deep Neural Network | Not utilized | No |
| [159] | 2019 | Arrhythmia | — | DL | Deep Neural Network | Not utilized | No |
| [92] | 2019 | Coronary artery disease | — | ML | Support vector machine | Not utilized | No |
| [135] | 2019 | Myocardial infarction | DWT-based | DL | Bidirectional, long short-term memory | Not utilized | No |
| [93] | 2019 | Arrhythmia | — | ML | Random forest | Utilized | Yes |
| [94] | 2020 | Arrhythmia | Bandpass filter | ML | CatBoost | Utilized | Yes |
| [136] | 2020 | Arrhythmia | — | DL | Convolutional neural network | Utilized | No |
| [137] | 2020 | Arrhythmia | Anti-aliasing filter and low-pass filter | DL | Convolutional neural network | Utilized | Yes |
| Work | Year | Cloud Computing | Summary |
|---|---|---|---|
| [163] | 2010 | Not utilized | Secure cross-layer-based body sensor network platform comprising critical ECG data identification and low-delay adaptive encryption features. |
| [164] | 2012 | Not utilized | Homomorphic encryption and Yao’s garbled circuits-based hybrid multi-party computation protocol to preserve the privacy of ECG quality. |
| [161] | 2013 | Utilized | Hiding patient’s confidential information in an ECG signal by utilizing a wavelet-based steganography technique that is an integration of encryption and scrambling techniques. |
| [165] | 2015 | Utilized | Remote monitoring system utilizing fully homomorphic encryption to the ECG data privacy |
| [160] | 2017 | Utilized | Public-key cryptosystem-based privacy preserving ECG monitoring system for arrhythmia detection with secure communication feature. |
| [166] | 2018 | Not utilized | Low-complexity privacy preserving compressive analysis utilizing subspace-based representation for arrhythmia detection. |
| [167] | 2018 | Not utilized | Low-latency privacy preserving approach for ECG monitoring systems utilizing several ECG features-based cryptographic key generation. |
| [168] | 2019 | Not utilized | An Internet of things-based ECG monitoring framework that utilizes biometric authentication to enable privacy preserving during sharing of ECG data. |
| [169] | 2020 | Utilized | SessionID/SessionKey-based privacy preserving compression model to enable efficient ECG sharing over Internet of Medical Things. |
| [170] | 2020 | Utilized | Internet of things-assisted ECG monitoring framework that enables secure ECG data transmission by utilizing lightweight access control, while also comprising of a lightweight secure health storage system. |
| Work | Year | Input Format Type | Output Format Type | Conversion Process | Remarks |
|---|---|---|---|---|---|
| [220] | 2003 | SCP-ECG | DICOM | Not reversible | Using an online SCP-ECG to DICOM adapter to translate the SCP-ECG signals into the DICOM medical environment. |
| [221] | 2005 | SCP-ECG | DICOM | Not reversible | SCP-ECG to DICOM one-way mapping comprising a viewer for the two formats. |
| [222] | 2004 | PhilipsXML | HL7 aECG | Not reversible | Conversion of Philips XML ECGs into the HL7 aECG by utilizing a PC-based application. |
| [223] | 2007 | SCP-ECG | GDF, HL7 aECG | Reversible | Usage of GDF as an intermediate framework to allow the two-way conversion between the formats SCP-ECG and HL7 aECG. |
| [224] | 2008 | SCP-ECG | XML | Reversible | Integrating SCP-ECG files by utilizing a backward-compatible ECG adapter to convert into XML-based relational databases. |
| [225] | 2008 | MIT-BIH | ecgML | Not reversible | Offers an ECG converter to support users using applications based on ecgML. |
| [226] | 2010 | IEEE P11073 | SCP-ECG | Reversible | Mapping of necessary classes and attributes to minimize the SCP-ECG fields and sections for IEEE P11073. |
| [227] | 2004 | SCP-ECG + VSIR | HL7 aECG | Not reversible | The HL7 aECG file is created by an automated signal processing tool named HES-EKG by combining the patient and raw data from the SCP-ECG record. |
| [228] | 2004 | SCP-ECG | XML and ASCII | Not reversible | The XML and ASCII-based formats are accessed by transcoding the SCP-ECG input files received from the database. |
| [229] | 2007 | ecgML and HL7 aECG | ASCII and XML | Not reversible | Based on [228], access to the database through PHP web application is provided, and the extension includes new formats. In addition, rendering ECG signals are achieved through different viewers. |
| [230] | 2005 | SCP-ECG | UNIPRO and SIFOR | Reversible | SCP-ECG as the central format based multiple format converter tool. |
| [231] | 2008 | SCP-ECG, UNIPRO, and HL7 aECG | DICOM | Not reversible | An enhancement to [230] that is based on the combination of the open standards within a DICOM-based picture archiving and communication system (PACS). |
| [193] | 2007 | SCP-ECG, ECG-9x, MFER, and HL7 aECG | XML-ECG | Reversible | A converter to check the compatibility of XML-based ECG format with other ECG formats. |
| [232] | 2010 | PhilipsXML and SCP-ECG | DICOM | Not reversible | A 12-lead ECG system based on PACS consisting of two converters is presented. |
| [233] | 2010 | SCP-ECG, HL7 aECG, DICOM, and PhilipsXML | XML -based format | Not reversible | A Java-based application to convert an XML-based central format. |
| [234] | 2011 | MIT-BIH, SCP-ECG, and HL7 aECG | ECG ontology | Reversible | A hypothesis to check the possibility of semantic integration among ECG data formats utilizing ECG ontology as reference. |
| [235] | 2017 | SCP-ECG | MFER | Not reversible | Conversion of the digital SCP-ECG used in clinical practice to the MFER standard for use in health care. Specifically, the structure of each section of SCP-ECG is converted to the format comprising of tag, length, and value and expressed in MFER format using different tags according to the expression contents. |
| [236] | 2018 | raw ECG | SCP-ECG, HL7 aECG and ISHNE format | Reversible | An adapter system named ECGConvert offers interoperability on raw ECG to HL7 aECG and SCPECG, while also supporting ISHNE format to HL7 aECG conversion. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Husain, K.; Mohd Zahid, M.S.; Ul Hassan, S.; Hasbullah, S.; Mandala, S. Advances of ECG Sensors from Hardware, Software and Format Interoperability Perspectives. Electronics 2021, 10, 105. https://doi.org/10.3390/electronics10020105
Husain K, Mohd Zahid MS, Ul Hassan S, Hasbullah S, Mandala S. Advances of ECG Sensors from Hardware, Software and Format Interoperability Perspectives. Electronics. 2021; 10(2):105. https://doi.org/10.3390/electronics10020105
Chicago/Turabian StyleHusain, Khaleel, Mohd Soperi Mohd Zahid, Shahab Ul Hassan, Sumayyah Hasbullah, and Satria Mandala. 2021. "Advances of ECG Sensors from Hardware, Software and Format Interoperability Perspectives" Electronics 10, no. 2: 105. https://doi.org/10.3390/electronics10020105
APA StyleHusain, K., Mohd Zahid, M. S., Ul Hassan, S., Hasbullah, S., & Mandala, S. (2021). Advances of ECG Sensors from Hardware, Software and Format Interoperability Perspectives. Electronics, 10(2), 105. https://doi.org/10.3390/electronics10020105