
Plant and Herbal Extracts as Ingredients of Topical Agents in the Prevention and Treatment Radiodermatitis: A Systematic Literature Review



Abstract
1. Introduction
1.1. Skin Reactions following Radiotherapy
1.2. Skin Care during Radiotherapy–Preventive Measures for Radiodermatitis
1.3. Active Substances in Skin Care Preparations after Radiotherapy
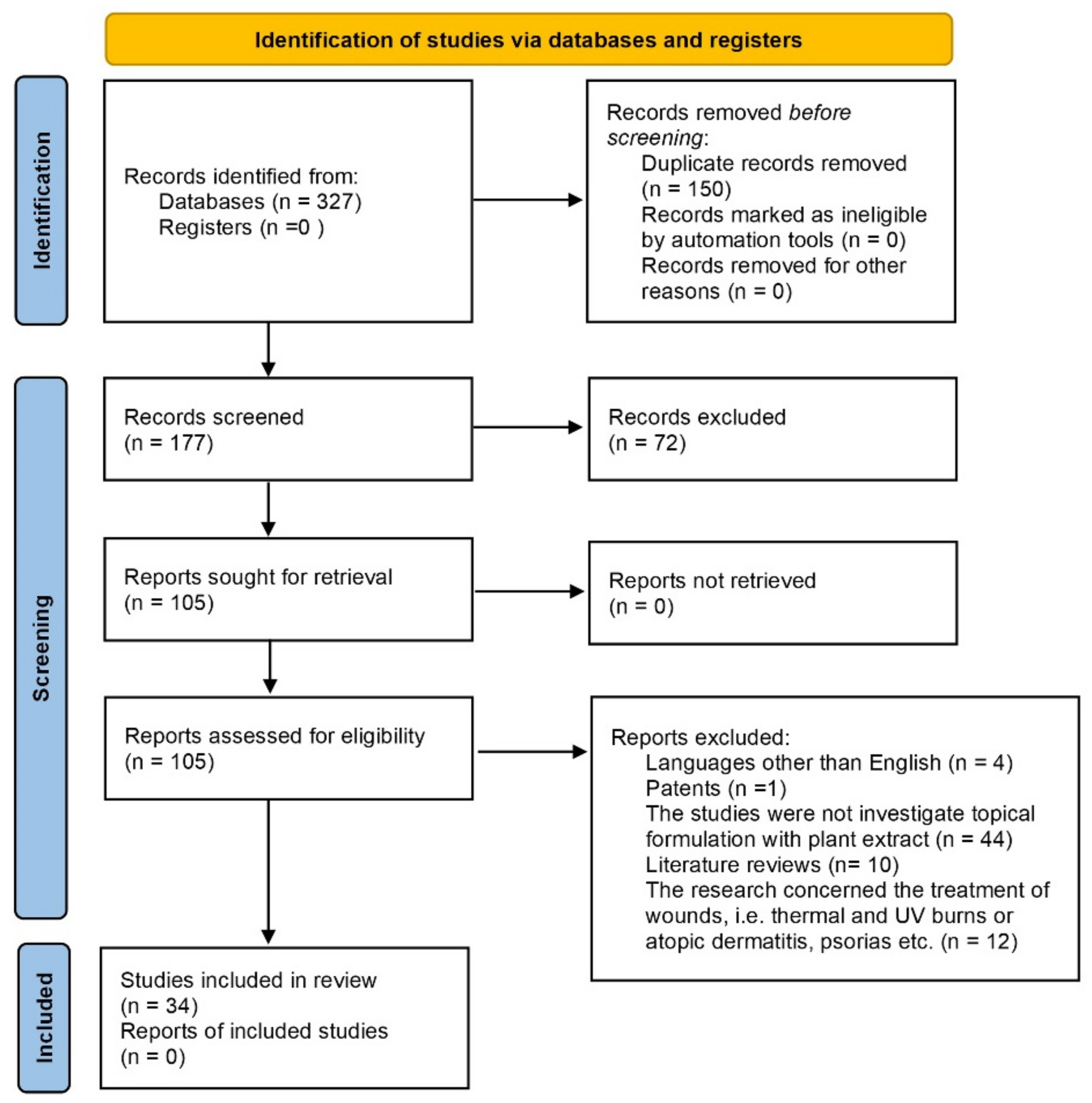
2. Materials and Methods
2.1. Scope
2.2. Methods
3. Results
4. Discussion
5. Conclusions
- The application of herbal extracts in preparations preventing radiodermatitis is important and still up-to-date (most recent publications about ongoing clinical studies are from 2021). Moreover, many herbal extracts such as Dilenia idica, and the Lamicale Family show potential in treating dermatitis but have not been introduced in the recipes of ointments, creams or gels.
- Herbal extracts obtained from plants can be added to recipes because they are part of a category of cosmeceutical supplements which are not subject to regulations and can be introduced into preparations without prescription. Herbal extracts can be a raw material from which active substances are isolated. For example, tea is a source of epigallocate-hin-3-gallatechin. Polysaccharides can be obtained from Annona muricata L. Both have potential in the treatment of dermatitis.
- The dominant actions among the plants are: anti-inflammatory, antioxidant and antimicrobial. This is linked to the mechanism of formation and healing of radiodermatitis but also to the physician’s actions aiming at preventing and treating inflammation, pain or skin damage and bleeding which are prone to bacterial superinfection. Some of the plants used in the study prove efficient in skin smoothing and moisturizing because dry skin with a pathological basis caused by dermatosis requires the same care as dry non-pathological skin.
- In the available study results there is conflicting information concerning the effectiveness in treatment and prevention of radiodermatitis by the products containing herbal extracts in their recipe (e.g., Aloe vera). There are also works mentioning that preparations such as ointments are poorly tolerated and appreciated by patients, and that some preparations cause allergies. Hence there are premises indicating that there is a need to widen the preparations offer for radiotherapy patients, the recipe of which is projected already at the evaluation stage of herbal extracts.
- The effectiveness evaluation for herbal extracts in radiotherapy is not an easy task since there are no strict guidelines. Studies should include both apparatus analyses of the skin condition and clinical studies including patients. They should also be preceded by the analysis of herbal extracts and recipe in terms of physicochemical, dermatological, and performance characteristics.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaffray, D.A.; Gospodarowicz, M.K. Chapter 14—Radiation Therapy for Cancer. In Cancer: Disease Control Priorities, 3rd ed.; Gelband, H., Jha, P., Sankaranarayanan, R., Horton, S., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2015; Volume 3, pp. 1–16. [Google Scholar]
- Byun, E.B.; Song, H.Y.; Sik Kim, W. Polysaccharides from Annona muricata leaves protect normal human epidermal keratinocytes and mice skin from radiation-induced injuries. Radiat. Phys. Chem. 2020, 170, 198672. [Google Scholar] [CrossRef]
- Wei, J.; Meng, L.; Hou, X.; Qu, C.; Wang, B.; Xin, Y.; Jiang, X. Radiation-induced skin reactions mechanism and treatment. Cancer Manag. Res. 2019, 11, 1670177. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tu, W.; Tang, Y.; Zhang, S. Prevention and treatment for radiation-induced skin injury during radiotherapy. Radiat. Med. Prot. 2020, 1, 60–68. [Google Scholar] [CrossRef]
- What Is Cancer Radiotherapy? Available online: https://www.zwrotnikraka.pl/na-czym-polega-radioterapia/ (accessed on 18 May 2022).
- Robson, V. Using honey to treat skin damaged by radiotherapy. Wounds 2009, 5, 51–57. [Google Scholar]
- Porock, D.; Kristjanosn, L. Skin reactions during radiotherapy for breast cancer: The use and impact of topical agents and dressings. Eur. J. Cancer Care 1999, 8, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Alavi, A.; Wong, R.; Akita, S. Radiodermatitis: A Review of Our Current Understanding. Am. J. Clin. Dermatol. 2016, 17, 277–292. [Google Scholar] [CrossRef]
- Hogl, W.P. Chapter 1—Overview of Skin Issues Related to the Oncology Patient. In Principles of Skin Care and the Oncology Patient; Haas, M.L., Moore-Higgs, G.J., Eds.; Oncology Nursing Society: Pittsburgh, PA, USA, 2011; pp. 1–32. [Google Scholar]
- Stone, H.B.; Coleman, C.N.; Anscher, M.; McBride, W.H. Effects of radiation on normal tissue: Consequences and mechanisms. Lancet Oncol. 2003, 4, 529–536. [Google Scholar] [CrossRef]
- Richardson, J.; Smith, J.; McIntyre, M.; Thomas, R.; Pilkington, K. Aloe Vera for Preventing Radiation-induced Skin Reactions: A Systematic Literature Review. Clin. Oncol. 2005, 17, 478–484. [Google Scholar] [CrossRef]
- Bensadoun, R.J.; Humbert, P.; Krutmann, J.; Luger, T.; Triller, R.; Rougier, A.; Seité, S.; Dreno, B. Daily baseline skin care in the prevention, treatment, and supportive care of skin toxicity in oncology patients: Recommendations from a multinational expert panel. Cancer Manag. Res. 2013, 5, 401–408. [Google Scholar] [CrossRef]
- Mendelsohn, F.A.; Divino, C.M.; Reis, E.D.; Kerstein, M.D. Wound Care After Radiation Therapy. Adv. Ski. Wound Care 2002, 15, 216–224. [Google Scholar] [CrossRef]
- McQuestion, M. Evidence-based skin care management in radiation therapy. Semin. Oncol. Nurs. 2006, 23, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Seité, S.; Bensadoun, R.-J.; Mazer, J.-M. Prevention and treatment of acute and chronic radiodermatitis. Breast Cancer Targets Ther. 2017, 9, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Wiśniewski, M.; Graczyk, M.; Szpinda, M.; Brzozowska-Mańkowska, S. Popromienne zapalenie skóry—Zasady postępowania. Med. Paliatywna W Prakt. 2013, 7, 41–45. [Google Scholar]
- Dormand, E.-L.; Banwell, P.E.; Goodacre, T.E. Radiotherapy and wound healing. Int. Wound J. 2005, 2, 112–127. [Google Scholar] [CrossRef] [PubMed]
- Kodiyan, J.; Amber, K.T. Topical antioxidants in radiodermatitis: A clinical review. Int. J. Palliat. Nurs. 2015, 21, 446–452. [Google Scholar] [CrossRef]
- De Conno, F.; Ventafridda, V.; Saita, L. Skin problems in advanced and terminal cancer patients. J. Pain Symptom Manag. 1991, 6, 247–256. [Google Scholar] [CrossRef]
- Haley, A.C.; Calahan, C.; Gandhi, M.; West, D.P.; Rademaker, A.; Lacouture, M.E. Skin care management in cancer patients: An evaluation of quality of life and tolerability. Support. Care Cancer 2010, 19, 545–554. [Google Scholar] [CrossRef]
- Michalewska, J. Odczyny popromienne w radioterapii oraz popromienne zapalenie skóry. Lett. Oncol. Sci. 2017, 14, 104–109. [Google Scholar] [CrossRef][Green Version]
- Skin Care Guidelines for Patients Receiving Radiotherapy. Available online: https://www.uhb.nhs.uk/Downloads/pdf/PiSkinCareGuideRadiotherapy.pdf (accessed on 17 October 2021).
- Stryczyńska, G. Assessment of the effectiveness and results of application research of soft cream Aquastop® Radioterapia (Ziołolek sp. z o.o.) in patients with dry and irritated skin, receiving radiotherapy. Contemp. Oncol. 2011, 15, 59–65. [Google Scholar]
- Topczewska-Bruns, J.; Filipowski, T.; Demska, M. Pielęgnacja i ochrona skóry w trakcie i po radioterapii. Opieka Onkol. 2014, 2, 56–58. [Google Scholar]
- Sauder, M.B.; Addona, M.; Andreiessen, A.; Butler, M.; Claveau, J.; Feugas, N.; Hijal, T.; Iannattone, L.; Kalia, S.; Teauge, L.; et al. The Role of Skin Care in Oncology Patients. Ski. Ther. Lett. 2020, 2–12. [Google Scholar]
- Draelos, Z.D. The science behind skin care: Moisturizers. J. Cosmet. Dermatol. 2018, 17, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Purnamawati, S.; Indrastuti, N.; Danarti, R.; Saefudin, T. The Role of Moisturizers in Addressing Various Kinds of Dermatitis: A Review. Clin. Med. Res. 2017, 15, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Werschler, W.P.; Trookman, N.S.; Rizer, R.L.; Ho, E.T.; Mehta, R. Enhanced efficacy of a facial hydrating serum in subjects with normal or self-perceived dry skin. J. Clin. Aesthetic Dermatol. 2011, 4, 51–55. [Google Scholar]
- Narasimhan, M.; Allotey, P.; Hardon, A. Self care interventions to advance health and wellbeing: A conceptual framework to inform normative guidance. BMJ 2019, 365, l688. [Google Scholar] [CrossRef]
- Yuen, F.; Arron, S. Chapter 4—Skin Care Products Used During Radiation Therapy. In Skin Care in Radiation Oncology: A Practical Guide, 1st ed.; Fowble, B., Yom, S.S., Yuen, F., Arron, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 31–45. [Google Scholar] [CrossRef]
- Lodén, M. Role of Topical Emollients and Moisturizers in the Treatment of Dry Skin Barrier Disorders. Am. J. Clin. Dermatol. 2003, 4, 771–788. [Google Scholar] [CrossRef]
- Kraft, J.N.; Lynde, C.W. Moisturizers: What they are and a practical approach to product selection. Ski. Ther. Lett. 2005, 10, 1–8. [Google Scholar]
- DebMandal, M.; Mandal, S. Coconut (Cocos nucifera L.: Arecaceae): In health promotion and disease prevention. Asian Pac. J. Trop. Med. 2011, 4, 241–247. [Google Scholar] [CrossRef]
- Danby, S.G.; AlEnzi, T.; Sultan, A.; Lavender, T.; Chittock, J.; Brown, K.; Cork, M.J. Effect of olive and sunflover seed oil on the adult skin barrier: Implications for neonatal skin care. Pediatr. Dermatol. 2013, 30, 42. [Google Scholar] [CrossRef]
- Nayak, B.; Raju, S.; Rao, A.C. Wound healing activity of Persea americana (avocado) fruit: A preclinical study on rats. J. Wound Care 2008, 17, 123–125. [Google Scholar] [CrossRef]
- Muangman, P.; Pundee, C.; Opasanon, S.; Muangman, S. A prospective, randomized trial of silver containing hydrofiber dressing versus 1% silver sulfadiazine for the treatment of partial thickness burns. Int. Wound J. 2010, 7, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Black, J.S.; Drake, D.B. A prospective randomized trial comparing silver sulfadiazine cream with watersoluble polyantimicrobial gel in partial-thickeness burn wounds. Plast. Surg. Nurs. 2015, 35, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Kerri, J.E. Principles of Topical Dermatologic Therapy. Available online: https://www.msdmanuals.com/professional/dermatologic-disorders/principles-of-topical-dermatologic-therapy/principles-of-topical-dermatologic-therapy (accessed on 18 May 2022).
- McQuestion, M. Evidence-Based Skin Care Management in Radiation Therapy: Clinical Update. Semin. Oncol. Nurs. 2011, 27, e1–e17. [Google Scholar] [CrossRef] [PubMed]
- Reszke, R.; Szepietowski, J. Special dermatological vehicles in concomitant therapy of chronic dermatoses. Forum Dermatol. 2016, 2, 48943. Available online: https://journals.viamedica.pl/forum_dermatologicum/article/view/48943/37310 (accessed on 18 May 2022).
- Elgharably, H.; Ganesh, K.; Dickerson, J.; Khanna, S.; Abas, M.; Das Ghatak, P.; Dixit, S.; Bergdall, V.; Roy, S.; Sen, C.K. A modified collagen gel dressing promotes angiogenesis in a preclinical swine model of chronic ischemic wounds. Wound Repair Regen. 2014, 22, 720–729. [Google Scholar] [CrossRef]
- Brett, D. A Review of Collagen and Collagen-based Wound Dressings. Wounds 2008, 20, 347–356. [Google Scholar]
- Macmillan, M.S.; Wells, M.; MacBride, S.; Raab, G.M.; Munro, A.; MacDougall, H. Randomized Comparison of Dry Dressings Versus Hydrogel in Management of Radiation-Induced Moist Desquamation. Int. J. Radiat. Oncol. 2007, 68, 864–872. [Google Scholar] [CrossRef]
- Gollins, S.; Gaffney, C.; Slade, S.; Swindell, R. RCT on gentian violet versus a hydrogel dressing for radiotherapy-induced moist skin desquamation. J. Wound Care 2008, 17, 268–275. [Google Scholar] [CrossRef]
- Sopata, M.; Szewczyk, M.T.; Zaporowska-Stachowiak, I.; Mościcka, P.; Jawień, A. Zastosowanie opatrunku w żelu w leczeniu ran przewlekłych. Leczenie Ran 2021, 18, 123–130. [Google Scholar] [CrossRef]
- Aderibigbe, B.A.; Buyana, B. Alginate in Wound Dressings. Pharmaceutics 2018, 10, 42. [Google Scholar] [CrossRef]
- Herst, P.M.; Bennett, N.C.; Sutherland, A.E.; Peszynski, R.I.; Paterson, D.B.; Jasperse, M.L. Prophylactic use of Mepitel Film prevents radiation-induced moist desquamation in an intra-patient randomised controlled clinical trial of 78 breast cancer patients. Radiother. Oncol. 2014, 110, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Fong, J.; Wood, F. Nanocrystaline silver dressings in wound management: A review. Int. J. Nanomed. 2006, 1, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Skalska-Kamińska, A.; Woźniak, A.; Paduch, R.; Kocjan, R.; Rejdak, R. Herbal preparation extract for skin after radiotherapy treatment. Part One—Preclinical tests. Acta Pol. Pharm. Drug Res. 2014, 71, 781–788. [Google Scholar]
- Griñan-Lison, C.; Blaya-Cánovas, J.L.; López-Tejada, A.; Ávalos-Moreno, M.; Navarro-Ocón, A.; Cara, F.E.; González-González, A.; Lorente, J.A.; Marchal, J.A.; Granados-Principal, S. Antioxidants for the Treatment of Breast Cancer: Are We There Yet? Antioxidants 2021, 10, 205. [Google Scholar] [CrossRef]
- Baliga, M.S.; Rao, S.; Rai, M.P.; D’souza, P. Radio protective effects of the Ayurvedic medicinal plant Ocimum santum Linn. (Holy Basil): A memoir. J. Cancer Res. Ther. 2016, 12, 20. [Google Scholar] [CrossRef]
- Szejk, M.; Kołodziejczyk-Czepas, J.; Żbikowska, H.M. Radioprotectors in radiotherapy—advances in the potential application of phytochemicals. Postepy Hig. Med. Dosw. 2016, 70, 722–734. [Google Scholar] [CrossRef]
- Unlu, A.; Nayir, E.; Kalenderoglu, M.D.; Kirca, O.; Ozdogan, M. Curcumin (Turmeric) and cancer. JBUON 2016, 21, 1050–1060. [Google Scholar]
- Ryan, J.L.; Heckler, C.E.; Ling, M.; Katz, A.; Williams, J.P.; Pentland, A.P.; Morrow, G.R. Curcumin for Radiation Dermatitis: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of Thirty Breast Cancer Patients. Radiat. Res. 2013, 180, 34–43. [Google Scholar] [CrossRef]
- Aqil, F.; Munagala, R.; Agrawal, A.K.; Gupta, R. Chapter 10—Anticancer Phytocompounds: Experimental and Clinical Updates. In New Look to Phytomedicine Advancements in Herbal Products as Novel Drug Leads; Ahmad Khan, M.S., Ahmad, I., Chattophadhyay, D., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 237–272. [Google Scholar] [CrossRef]
- Yahyapour, R.; Shabeeb, D.; Cheki, M.; Musa, A.E.; Farhood, B.; Rezaeyan, A.; Amini, P.; Fallah, H.; Najafi, M. Radiation Protection and Mitigation by Natural Antioxidants and Flavonoids: Implications to Radiotherapy and Radiation Disasters. Curr. Mol. Pharmacol. 2018, 11, 285–304. [Google Scholar] [CrossRef]
- Kalekhan, F.; Kudva, A.K.; Raghu, S.V.; Rao, S.; Hegde, S.K.; Simon, P.; Baliga, M.S. Traditionally Used Natural Products in Preventing Ionizing Radiation-Induced Dermatitis: First Review on the Clinial Study. Anti-Cancer Agents Med. Chem. 2022, 22, 64–82. [Google Scholar] [CrossRef]
- Heydarirad, G.; Ahadi, B.; Vardanjani, H.M.; Cramer, H.; Mirzaei, H.R.; Pasalar, M. Herbal Medicines for Treatment of Radiodermatitis: A Systematic Review and Meta-Analysis. J. Altern. Complement. Med. 2021, 27, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, M.; Sandoughdaran, S.; Shandiz, F.H.; Honary, S. The Efficacy of Licorice Root (Glycyrrhiza glabra) and Yarrow (Achillea millefolium) in Preventing Radiation Dermatitis in Patients with Breast Cancer: A Randomized, Double-Blinded, Placebo-Controlled Clinical Trial. Asian Pac. J. Cancer Care 2016, 1, 9–13. [Google Scholar] [CrossRef][Green Version]
- Roberts, D.B.; Travis, E.L. Acemannan-containing wound dressing gel reduces radiation-induced skin reactions in C3H mice. Int. J. Radiat. Oncol. 1995, 32, 1047–1052. [Google Scholar] [CrossRef]
- Williams, M.S.; Burk, M.; Loprinzi, C.L.; Hill, M.; Schomberg, P.J.; Nearhood, K.; O’Fallon, J.R.; Laurie, J.A.; Shanahan, T.G.; Moore, R.L.; et al. Phase III double-blind evaluation of an aloe vera gel as a prophylactic agent for radiation-induced skin toxicity. Int. J. Radiat. Oncol. Biol. Phys. 1996, 36, 345–349. [Google Scholar] [CrossRef]
- Heggie, S.; Bryant, G.P.; Tripcony, L.; Keller, J.; Rose, P.; Glendenning, M.; Heath, J. A Phase III Study on the Efficacy of Topical Aloe Vera Gel on Irradiated Breast Tissue. Cancer Nurs. 2002, 25, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Bosley, C.; Smith, J.; Baratti, P.; Pritchard, D.; Xiong, X.; Li, C.; Merchant, T. A phase III trial comparing an anionic phospholipid-based (APP) cream and aloe vera-based gel in the prevention and treatment of radiation dermatitis. Int. J. Radiat. Oncol. 2003, 57, S438. [Google Scholar] [CrossRef]
- Merchant, T.E.; Bosley, C.; Smith, J.; Baratti, P.; Pritchard, D.; Davis, T.; Li, C.; Xiong, X. A phase III trial comparing an anionic phospholipid-based cream and aloe vera-based gel in the prevention of radiation dermatitis in pediatric patients. Radiat. Oncol. 2007, 2, 45–48. [Google Scholar] [CrossRef]
- Hoopfer, D.; Holloway, C.; Gabos, Z.; Alidrisi, M.; Chafe, S.; Krause, B.; Lees, A.; Mehta, N.; Tankel, K.; Strickland, F.; et al. Three-Arm Randomized Phase III Trial: Quality Aloe and Placebo Cream Versus Powder as Skin Treatment During Breast Cancer Radiation Therapy. Clin. Breast Cancer 2015, 15, 181–190.e4. [Google Scholar] [CrossRef]
- Haddad, P.; Amouzgar-Hashemi, F.; Samsami, S.; Chinichian, S.; Oghabian, M.A. Aloe vera for prevention of radiation-induced dermatitis: A self-controlled clinical trial. Curr. Oncol. 2013, 20, e345–e348. [Google Scholar] [CrossRef]
- Olsen, D.L.; Raub, W., Jr.; Bradley, C.; Johnson, M.; Macias, J.L.; Love, V.; Markoe, A. The effect of aloe vera gel/mild soap versus mild soap alone in preventing skin reactions inpatients undergoing radiation therapy. Oncol. Nurs. Forum 2001, 28, 543–547. [Google Scholar]
- Goyal, P.K.; Gehlot, P. Radioprotective Effects of Aloe Vera Leaf Extract on Swiss Albino Mice against Whole-Body Gamma Irradiation. J. Environ. Pathol. Toxicol. Oncol. 2009, 28, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Shimpo, K.; Ida, C.; Chihara, T.; Beppu, H.; Kaneko, T.; Kuzuya, H. Aloe arborescens extract inhibits TPA-induced ear oedema, putrescine increase and tumour promotion in mouse skin. Phytother. Res. 2002, 16, 491–493. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.A.; Trevisan, G.; Hoffmeister, C.; Rossato, M.F.; Boligon, A.; Walker, C.; Klafke, J.Z.; Oliveira, S.M.; Silva, C.R.; Athayde, M.L.; et al. Anti-inflammatory and antioxidant effects of Aloe saponaria Haw in a model of UVB-induced paw sunburn in rats. J. Photochem. Photobiol. B Biol. 2014, 133, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Hegde, S.K.; Baliga-Rao, M.P.; Palatty, P.L.; George, T.; Baliga, M.S. An Aloe Vera-Based Cosmeceutical Cream Delays and Mitigates Ionizing Radiation-Induced Dermatitis in Head and Neck Cancer Patients Undergoing Curative Radiotherapy: A Clinical Study. Medicines 2017, 4, 44. [Google Scholar] [CrossRef] [PubMed]
- Nyström, J.; Svensk, A.-C.; Lindholm-Sethson, B.; Geladi, P.; Larson, J.; Franzén, L. Comparison of three instrumental methods for the objective evaluation of radiotherapy induced erythema in breast cancer patients and a study of the effect of skin lotions. Acta Oncol. 2007, 46, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Ahmadloo, N.; Kadkhodaei, B.; Omidvari, S.; Mosalaei, A.; Ansari, M.; Nasrolahi, H.; Hamedi, S.H.; Mohammadianpanah, M. Lack of Prophylactic Effects of Aloe Vera Gel on Radiation Induced Dermatitis in Breast Cancer Patients. Asian Pac. J. Cancer Prev. 2017, 18, 1139–1143. [Google Scholar] [CrossRef]
- Sharma, S.; Sharma, V.; Gupta, M.C.; Verma, Y. Comparative Evaluation of Efficacy and Safety of Herbal Preparation vis-à-vis Beclomethasone Cream on Radiation Induced Skin Injury in Head and Neck Carcinoma Patients Receiving Radiotherapy or Chemoradiation in Oncology Department at a Tertiary Care Hospital. Int. J. Med. Res. Prof. 2019, 5, 14–18. [Google Scholar]
- Sharma, S.; Sharma, V.; Gupta, M.C.; Verma, Y. Comparative Evaluation of Quality of Life in Patients of Head and Neck Carcinoma with Radiation Induced Skin-injury in Oncology Department at Tertiary Care Hospital. Int. J. Interdiscip. Multidiscip. Stud. 2019, 6, 65–79. [Google Scholar]
- Shin, S.; Jang, B.-H.; Suh, H.S.; Park, S.-H.; Lee, J.-W.; Yoon, S.W.; Kong, M.; Lim, Y.J.; Hwang, D.-S. Effectiveness, safety, and economic evaluation of topical application of a herbal ointment, Jaungo, for radiation dermatitis after breast conserving surgery in patients with breast cancer (GREEN study): Study protocol for a randomized controlled trial. Medicine 2019, 98, e15174. [Google Scholar] [CrossRef]
- Kim, E.H.; Yoon, J.-H.; Bin Park, S.; Lee, J.Y.; Chung, W.K.; Yoon, S.W. Comparative Efficacy of Jaungo, A Traditional Herbal Ointment, and the Water-in-Oil Type Non-Steroidal Moisturizer for Radiation-Induced Dermatitis in Patients With Breast Cancer: A Study Protocol for a Prospective, Randomized, Single-Blinded, Pilot Study. Front. Pharmacol. 2021, 12, 751812. [Google Scholar] [CrossRef]
- Kong, M.; Hwang, D.-S.; Lee, J.Y.; Yoon, S.W. The Efficacy and Safety of Jaungo, a Traditional Medicinal Ointment, in Preventing Radiation Dermatitis in Patients with Breast Cancer: A Prospective, Single-Blinded, Randomized Pilot Study. Evid. Based Complement. Altern. Med. 2016, 2016, 9481413. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, A. Clinical application of shinuko. J. Trad. Med. 2013, 30, 27–30. [Google Scholar]
- Maramaldi, G.; Togni, S.; Di Pierro, F.; Biondi, M. A cosmeceutical formulation based on boswellic acids for the treatment of erythematous eczema and psoriasis. Clin. Cosmet. Investig. Dermatol. 2014, 7, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Togni, S.; Maramaldi, G.; Bonetta, A.; Giacomelli, L.; Di Pierro, F. Clinical evaluation of safety and efficacy of Boswellia-based cream for prevention of adjuvant radiotherapy skin damage in mammary carcinoma: A randomized placebo controlled trial. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1338–1344. [Google Scholar]
- Pommier, P.; Gomez, F.; Sunyach, M.; D’Hombres, A.; Carrie, C.; Montbarbon, X. Phase III Randomized Trial of Calendula Officinalis Compared With Trolamine for the Prevention of Acute Dermatitis During Irradiation for Breast Cancer. J. Clin. Oncol. 2004, 22, 1447–1453. [Google Scholar] [CrossRef]
- Kodiyan, J.; Amber, K.T. A Review of the Use of Topical Calendula in the Prevention and Treatment of Radiotherapy-Induced Skin Reactions. Antioxidants 2015, 4, 293–303. [Google Scholar] [CrossRef]
- Sharp, L.; Finnilä, K.; Johansson, H.; Abrahamsson, M.; Hatschek, T.; Bergenmar, M. No differences between Calendula cream and aqueous cream in the prevention of acute radiation skin reactions—Results from a randomised blinded trial. Eur. J. Oncol. Nurs. 2013, 17, 429–435. [Google Scholar] [CrossRef]
- Siddiquee, S.; A McGee, M.; Vincent, A.D.; Giles, E.; Clothier, R.; Carruthers, S.; Penniment, M. Efficacy of topical Calendula officinalis on prevalence of radiation-induced dermatitis: A randomised controlled trial. Australas. J. Dermatol. 2021, 62, e35–e40. [Google Scholar] [CrossRef]
- Schneider, F.; Danski, M.T.R.; Vayego, S.A. Usage of Calendula officinalis in the prevention and treatment of radiodermatitis: A randomized double-blind controlled clinical trial. Rev. Esc. Enferm. USP 2015, 49, 221–228. [Google Scholar] [CrossRef]
- Hu, J.J.; Cui, T.; Rodriguez-Gil, J.L.; Allen, G.O.; Li, J.; Takita, C.; Lally, B.E. Complementary and alternative medicine in reducing radiation-induced skin toxicity. Radiat. Environ. Biophys. 2014, 53, 621–626. [Google Scholar] [CrossRef]
- Thanthong, S.; Nanthong, R.; Kongwattanakul, S.; Laebua, K.; Trirussapanich, P.; Pitiporn, S.; Nantajit, D. Prophylaxis of Radiation-Induced Dermatitis in Patients With Breast Cancer Using Herbal Creams: A Prospective Randomized Controlled Trial. Integr. Cancer Ther. 2020, 19, 1534735420920714. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, E.B.; Ciol, M.A.; De Meneses, A.G.; Bontempo, P.D.S.M.; Hoffman, J.M.; Dos Reis, P.E.D. Chamomile Gel versus Urea Cream to Prevent Acute Radiation Dermatitis in Head and Neck Cancer Patients: Results from a Preliminary Clinical Trial. Integr. Cancer Ther. 2020, 19, 1534735420962174. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, E.B.; Ciol, M.; Vasques, C.I.; Bontempo, P.D.S.M.; Vieira, N.N.P.; Silva, L.F.O.E.; Avelino, S.R.; Dos Santos, M.A.; Dos Reis, P.E.D. Gel of chamomile vs. urea cream to prevent acute radiation dermatitis in patients with head and neck cancer: A randomized controlled trial. J. Adv. Nurs. 2016, 72, 1926–1934. [Google Scholar] [CrossRef] [PubMed]
- Pajonk, F.; Riedisser, A.; Henke, M.; McBride, W.H.; Fiebich, B. The effects of tea extracts on proinflammatory signaling. BMC Med. 2006, 4, 28. [Google Scholar] [CrossRef] [PubMed]
- Näf, G.; Gasser, U.E.; Holzgang, H.E.; Schafroth, S.; Oehler, C.; Zwahlen, D.R. Prevention of Acute Radiation-Induced Skin Reaction with NPE® Camellia Sinensis Nonfermentatum Extract in Female Breast Cancer Patients Undergoing Postoperative Radiotherapy: A Single Centre, Prospective, Open-Label Pilot Study. Int. J. Breast Cancer 2018, 2018, 2479274. [Google Scholar] [CrossRef] [PubMed]
- Composition of Holoil® Series. Available online: https://www.holoil.it/site (accessed on 19 May 2022).
- Franco, P.; Potenza, I.; Moretto, F.; Segantin, M.; Grosso, M.; Lombardo, A.; Taricco, D.; Vallario, P.; Filippi, A.R.; Rampino, M.; et al. Hypericum perforatum and neem oil for the management of acute skin toxicity in head and neck cancer patients undergoing radiation or chemo-radiation: A single-arm prospective observational study. Radiat. Oncol. 2014, 9, 297. [Google Scholar] [CrossRef]
- Rafati, M.; Ghasemi, A.; Saeedi, M.; Habibi, E.; Salehifar, E.; Mosazadeh, M.; Maham, M. Nigella sativa L. for prevention of acute radiation dermatitis in breast cancer: A randomized, double-blind, placebo-controlled, clinical trial. Complement. Ther. Med. 2019, 47, 102205. [Google Scholar] [CrossRef]
- Karbasforooshan, H.; Hosseini, S.; Elyasi, S.; Pakdel, A.F.; Karimi, G. Topical silymarin administration for prevention of acute radiodermatitis in breast cancer patients: A randomized, double-blind, placebo-controlled clinical trial. Phytother. Res. 2018, 33, 379–386. [Google Scholar] [CrossRef]
- Becker-Schiebe, M.; Mengs, U.; Schaefer, M.; Bulitta, M.; Hoffmann, W. Topical use of a silymarin-based preparation to prevent radiodermatitis: Results of a prospective study in breast cancer patients. Strahlenther. Onkol. 2011, 187, 485. [Google Scholar] [CrossRef]
- Palatty, P.L.; Azmidah, A.; Rao, S.; Jayachander, D.; Thilakchand, K.R.; Rai, M.P.; Haniadka, R.; Simon, P.; Ravi, R.; Jimmy, R.; et al. Topical application of a sandal wood oil and turmeric based cream prevents radiodermatitis in head and neck cancer patients undergoing external beam radiotherapy: A pilot study. Br. J. Radiol. 2014, 87, 20130490. [Google Scholar] [CrossRef]
- Rao, S.; Hegde, S.K.; Baliga-Rao, M.P.; Lobo, J.; Palatty, P.L.; George, T.; Baliga, M.S. Sandalwood Oil and Turmeric-Based Cream Prevents Ionizing Radiation-Induced Dermatitis in Breast Cancer Patients: Clinical Study. Medicines 2017, 4, 43. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.R.; Gewandter, J.S.; Bautista, J.; Heckler, C.E.; Strasser, J.; Dyk, P.; Anderson, T.; Gross, H.; Speer, T.; Dolohanty, L.; et al. Utility of topical agents for radiation dermatitis and pain: A randomized clinical trial. Support. Care Cancer 2019, 28, 3303–3311. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.A.; Patel, N.J.; Patel, R.P. Formulation and Evaluation of Curcumin Gel for Topical Application. Pharm. Dev. Technol. 2008, 14, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, S.; Jeon, B.-S.; Jang, W.-S.; Lee, S.-J.; Son, Y.; Rhim, K.-J.; Lee, S.I.; Lee, S.-S. Therapeutic effect of topical application of curcumin during treatment of radiation burns in a mini-pig model. J. Vet. Sci. 2016, 17, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Palefsky, I. Rozdział Uwagi dotyczące wytwarzania kosmeceutyków. In Kosmeceutyki, 2nd ed.; Draelos, Z.D., Ed.; Elsevier Edra Urban & Partner: Wrocław, Poland, 2009; pp. 19–26. [Google Scholar]
- Thornfeldt, C.R. Rozdział 12: Rośliny jako kosmeceutyki. In Kosmeceutyki, 2nd ed.; Draelos, Z.D., Ed.; część 2; Elsevier Edra Urban & Partner: Wrocław, Poland, 2009; pp. 87–98. [Google Scholar]


{kind=link}
| 0 | I Degree | II Degree | III Degree | IV Degree | V Degree |
|---|---|---|---|---|---|
| no changes | mild erythema, dry desquamation, reduced sweating | moderate to severe erythema, intertriginous moist desquamation usually limited to skin folds and articulations, moderate edema | moist desquamation outside the skin folds and articulations, bleeding caused by minor trauma or abrasion, edematous skin | skin necrosis or ulceration across all the skin layers, spontaneous bleeding in the impacted | death |
| Product Type | Physicochemical Form | Purpose | Advantages | Disadvantages |
|---|---|---|---|---|
| For washing | Gel, aqueous solution, foam, soap | Skin cleansing | Cleansed skin, better absorption of other care products, limited exposure to bacteriological infection | Can cause irritation, reddening or desquamation |
| Lotion | Aqueous solution, emulsion | Skin pH equalization, smoothing, softening | Maintaining the skin in healthy condition by providing proper moisturizing substances, supplement to self-care * | Can cause irritation, requires additional steps in skin care, i.e., application of creams, due to the water content in the composition, it requires preservatives |
| Serum | Emulsion, gel | Providing of active ingredients | Reinforces and intensifies daily care, increases the action of cremes, additional moisturizing, light gel texture, evaporates quickly, supplement to self-care * | High concentration of active substances can lead to skin irritation, Need to apply a second product like nourishing cream or protection cream against UV radiation |
| Cream | Emulsion | Moisturization, lubrication, regeneration, nourishing | Moisturizing, soothing of side effects such as itching, burning or reddening | Need to apply several times during the day |
| Ointment | Emulsion, suspension | Treatment | Eliminates side effects | Greasy, heavy texture, hard to spread on skin |
| Type of Action | Mechanism of Operation | Types of Preparations | Advantages Disadvantages, Specific Traits | Active Substances in the Receipe | Ref. |
|---|---|---|---|---|---|
| Moisturizing | Maintain moisture, protect the skin in three ways: replacement of deficient agents (present in the product), occlusion, humectant action | Ointments, creams, pastes, foams, lotions, gels | Ointments are more penetrating that other forms such as creams or lotions, but they can be too occlusive and greasy, gels can dry on skin and cause irritation | Natural oils, ceramides, humectants, urea, sorbitol, panthenol hyaluronic acid, plant extracts | [30,31,32] |
| Emollient | Improve skin barrier function, supplement epidermal lipids, reduce itching and dermatitis | Creams, lotions, oils | Preparations based on petrolatum clog up pores, some emollients can cause hypersensitivity | Lanolin, bee wax, herbal and animal oils like: emu oil, coconut oil, olive oil, avocado oil, evening primrose, vegetable butters (i.e., shea butter), fatty alcohols | [30,33,34,35] |
| Curative: Anti-inflammatory | Reduce inflammatory skin reactions | Creams, ointments, lotions, solutions | According to MASCC directives, preventive use of steroids to be applied topically prevents and heals radiation dermatitis - there is no standard for the type of topical steroid to be used in the radiation oncology population. The concentration, frequency, and duration of steroid applications vary by institution. Long use of steroids is not indicated because of side effects. Steroid preparations are used together with emollients | Mometasone furoate, hydrocortisone | [30] |
| Washing (cleansing) | Help remove contaminants such as dirt, perspiration, oil, dead skin cells form the skin within the treatment area, supports cleansing, reduces potential bacterial and biological burden at the treatment site | Soaps, synthetic detergents | Because of its high pH, soap disturbs the hydro-lipid balance of the skin which might lead to irritations and bacterial overgrowth Synthetic detergents do not contain soap, they are based on surfactants, they are neutral or slightly acidic. More strongly recommended for the therapy of oncology patients | Some soaps contain additive antibacterial substances, they also contain humectants additional oils and/or lipids to prevent skin dryness Synthetic detergents also contain free fatty acids, lipids, proteins, preserving the natural epidermal barrier | [30] |
| Sisnfectant and antiinfective | Cleansing aids in decreasing potential bacterial and bio burden on the treatment site (especially dry and exfoliating) | Solutions, ointments, creams, powder forms | Antibacterial and antifungal preparations for local application are active in the application zone with a minimal systemic absorption | Chlorhexidine gluconate, clotrimazole, miconazole, nystatin, bacitracin, mupirocin, silver sulfadiazine cream | [30,36,37] |
| Dessicants and astringent agents | They have astringent, antibacterial properties, High humidity can cause skin irritation and maceration | Solutions for compresses, powders | Powders dry out macerated skin and reduce friction by absorbing humidity. Some has tend to clump which may cause irritation. Depending on the applied substance applied, granuloma may appear but also conditions conductive to fungus development | Burrow’s solution (5% aluminium sulfate tetradecahydrate) aluminum chloride solution, corn starch, talk | [30,38] |
| Barrier measures | Protect the skin against mechanical damage, abrasion by clothes or other parts of the skin. Reduces skin reaction severity | Cremes, ointments, liquids, protective films | Reduce injuries, keep moisture in intact skin and hence the limit potential friction and irradiated skin reactions, thereby reducing radiation injury. Reduction in frequency and duration of moist desquamation. | Create physical film barrier: polymers PVA, copolymer ethylene/acrylic acid, acrylate terpolymer, emollients: coconut oil, dimethicone, mineral oil, Because of high volume of water, liquid and creme preparations must contain preservatives. | [14,18,39] |
| Plant | Form of Product | Purpose of Study. Subjects. Methodology. Product Applications | Recipe. Add. Information. | Key Findings of Effectiveness of Action | Comments | Ref. |
|---|---|---|---|---|---|---|
| Achillea millefolium L. (Yarrow) | cream | Assess the effect of Glycyrrhiza glabra L. (Licorice root) and Achillea millefolium (Yarrow) on preventing RD RCT. Patients with BC, who undergone mastectomy, receive RT (50 Gray in 25 fractions, over five weeks) Patients were divided into 3 groups: 1 group received Glycyrrhiza glabra cream, 2 group placebo (vanishing cream base), 3 group Achillea millefolium cream. The rate and grade of radiation dermatitis were recorded at baseline, at the end of third week and at the end of treatment using (RTOG) grading tool. Time of application was of five weeks during RT. Preparations were applied daily. Patients were instructed do not to apply other topical skin care products. | The extract of Achillea millefolium L. and Glycyrrhiza glabra Root were incorporated into a vanishing cream base. Dry Extract constituted 0.6%. Vanishing cream ingredients: Stearic Acid 15%, Cetostearyl Alcohol 2%, Mineral Oil 2%, Borax 1%, Ammonium Hydroxide 28% 1%, Preservative 0.2%, Water 71.2%, Propylene Glycol 4%, Glycerin 3%. | At the end of the third week, the group receiving Achillea millefolium cream showed milder skin complications than other groups. At the end of treatment, rate of skin complications in groups receiving herbal drugs was lower than placebo group but it was not statistically significant. The results of this study did not present a significant difference between Glycyrrhiza glabra, Achillea millefolium L. and placebo on preventing RD. | According to Author, this is the first study that has evaluated the possible protective effect of these herbal drugs against radiotherapy induced skin dermatitis. Achillea millefolium L., especially at lower doses of radiation, might decrease radiation induced dermatitis. There were observed only two cases with grade 1 dermatitis at the end of third week in this group, so more research is required to verify this finding. | [59] |
| Aloe vera L. Burman | gel ointment | To determine: whether a gel with acemannan extracted from aloe leaves affects the severity of ARSR if so, whether other commercially products (personal lubricating jelly and healing ointment) have similar effect and when the gel with extract should be applied for maximum effect. Male C3H mice received graded single doses of gamma radiation ranging from 30 to 47.5 Gy to the right leg. Groups of mice (gel treated, untreated, jelly-treated, ointment-treated) The right inner thigh of each mouse was scored on a scale of 0 to 3.5 for severity of radiation reaction from the seventh to the 35th day after irradiation. EDSo values, and 95% confidence limits were also obtained. The gel was applied daily to the irradiated area beginning immediately after irradiation. To determine timing of application for best effect, gel was applied beginning on day −7, 0, or +7 relative to the day of irradiation (day 0) and continuing for 1, 2, 3, 4, or 5 weeks. | Wound dressing gel: Purified water, Povidone, Panthenol, Carbomer 940, Triethanolamine, Allantoin, Glutamic acid, Sodium chloride, Methylparaben, Imidazolidinyl urea, Sodium Benzoate, Potassium Sorbate, Acemannan hydrogel, Citric acid, Sodium metabisulfite. Personal lubricating jelly (water soluble hydrogel, similar in solubility and consistency to the accemannan gel): Chlorhexidine gluconate, Gluconodelta lactone, Glycerin, Hydroxyethylcellulose, Methylparaben, Purified water, Sodium hydroxide. Healing ointment: Petrolatum, Mineral oil, Mineral wax, Wool wax Alcohol, Panthenol, Glycerin, Bisabolol (Chamomile essence) | The average peak skin reactions of gel-treated mice were lower than those of the untreated mice at all radiation doses tested. The EDSo values for skin reactions of 2.0–2.75 were approximately 7 Gy higher in the wound dressing gel-treated mice. The average peak skin reactions and the EDSo values for mice treated with personal lubricating jelly or healing ointment were similar to irradiated control values. Reduction in the percentage of mice with skin reactions of 2.5 or more was greatest in the groups that received gel for at least 2 weeks beginning immediately after irradiation. | In this case, Aloe vera leaves were the raw material for extraction of Acemannan. Healing ointment contained the essence of chamomile. The authors of the study tried to define the time for starting the application of the preparation. | [60] |
| Aloe vera L. Burman | gel | To determine effectiveness aloe vera gel for radiation-induced skin reactions. BC patients undergoing RT to breast and/or chest wall, minimum field 10 × 10 cm and minimum dose 50c Gy. RCT. Two groups: aloe vera gel or PL gel—first phase of trial, aloe vera gel or no treatment—second phase of trial. State of the skin was evaluated—patients self-graded skin reactions and clinical assessment by physician. Rated: severity, time of occurrence and duration of severe dermatitis. The evaluation was carried out once a week. Gel (aloe vera or placebo) was applied to the chest wall by the patient twice a day, starting 3 days within of radiation initiation. Usual skin-care (soap) advice were recommended. | No detailed information available concerning the products recipe and their quality control Aloe vera gel—98% aloe gel plus 2% inert gel for consistency. | Aloe vera gel was not effective. The dermatitis was less severe than expected. Allergic reactions were observed among patients both in groups using aloe vera gel and placebo gel. | [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61] | |
| Aloe vera L. Burman | gel cream | To determine if aloe vera gel is beneficial in reducing skin side-effects of RT when compared with aqueous cream. Women with BC undergoing RT post-lumpectomy or partial mastectomy. RCT. Two group: aloe vera gel and topical aqueous cream. Evaluation of the skin by nurse—limitation of side-effects such as erythema, pain, itching, dry desquamation, moist desquamation. Standard care was recommended on top of preparations application. Topical products were applied by patients three times a day after treatment and for 2 weeks after completing care. Weekly skin assessments were performed by nursing staff. | No information available concerning the products recipe and their quality control. | Aqueous cream was significantly better than aloe vera gel in reducing dry desquamation and treatment-related pain. Allergic reactions were observed in patients using both gel and cream. | No information available to objectively evaluate the efficiency of the study (including the dose of radiation administered to patients). | [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] |
| Aloe vera L. Burman | gel cream | Compare effectiveness of an anionic polar phospholipid (APP)-based cream and an aloe vera-based gel in preventing and treating RD. Pediatric patients with various diagnoses (RT with at least 23.4 Gy dose). Subject’s skin comfort, dermatologic assessment, and CTC were evaluated. The study was carried out before, during and after completion of treatment (4–6 weeks). APP cream and aloe vera gel were symmetrically applied within the irradiated field after each treatment. | Aloe vera (market product) contain: D-panthenol, Triethanoloamine, Carbomer 943P, Hyaluronic acid, Potassium Sorbate, Diazolidinyl Urea, Methylparaben, Propylparaben. APP skin cream (Ocular Research of Boston) is an oil-in-water emulsion, not commercially available. Include: triglycerides and phospholipids, Benzyl Alcohol, Methylparaben, Propyl paraben, Diaxolipinyl urea. | APP cream improves skin comfort variables such as: dry, soft, feels good, rough, smooth and dermatologic variables: dryness, erythema and peely as compared with aloe vera gel (statistically significant differences). APP cream is more effective in prevention and treatment of RD. Grouped CTC scores were supportive of APP cream. In comparing the first and last assessments, two dermatologic variables, dryness and peely, favored APP cream. | Results in concordance with Boosley’s study [63] | [64] |
| Aloe vera L. Burman | cream powder | Test the efficacy of quality-tested Aloe vera extract in reducing the severity of radiation-induced skin injury. Examine the effect of a moist cream versus a dry powder skin care regimen. RCT. Patients with BC, previous mastectomy or segmental resection. RT (45–50 Gy). Acute skin toxicity was scored weekly and after treatment at weeks 1, 2, and 4 using a modified 10-point Catterall scale. The patients scored their symptom severity using a 6-point Likert scale and kept an acute phase diary. Standard radiation skin care guidelines were complied. The patients apply nonmetallic baby powder or cornstarch to the irradiated intact skin during the treatment course followed by 1 month of Glaxal base cream twice daily. If they developed moist desquamation, they were advised to discontinue the powder. Patients apply approximately 2.5 cm3 of cream to the irradiated skin, 3 times daily (avoid application within 3 h of radiation) throughout the course of radiation and for 1 month after radiation. Treatment of moist desquamation and other skin reactions, such as infection, was according to each physician’s pattern of practice. Any prescribed treatment was to be applied 30 min before the use of the study creams. | Placebo cream contain: Aquatrix II, Lexamul 56, Methylparaben, Dimethicone, Isopropyl Myristate, Propylene Glycol, Cetyl Alcohol, Stearic acid, triethanolamine. The aloe cream formulation was 30 mg of the processed aloe (1000–5000 MW fraction) per 100 cm3 of placebo cream. This represents the highest concentration possible without causing cream demulsification and is relatively equivalent to 50 mg of the 1000 to 5000 MW fraction of unprocessed fresh leaf gel extract. | The aloe formulation did not reduce acute skin toxicity or symptom severity. Study speaks in favor of dry care instead of introducing herbal extracts into creams or applying creams only. | Were excluded from the study people with confirmed allergy to Aloe vera. Placebo cream was chosen for its ability to penetrate the outermost skin layers and therefore to theoretically enable absorption of the aloe elemental components. The study included also the analysis of the extract itself introduced into the recipe of the cream. Such as: murine bioassay testing under the supervision of 1 of us (F.S.). The assay testing was conducted to determine whether the aloe oligosaccharides that prevent ultraviolet B (UVB)-induced immune suppression of T-cell-mediated immune responses were active in this study. The mechanism of aloe skin protection is unknown, and this element might be necessary for aloe extract to be effective in reducing RSR severity. | [65] |
| Aloe vera L. Burman | lotion | Evaluation of aloe vera lotion for prevention of RD. CT. Patients with a prescription of RT to a minimum dose of 40 Gy, were treatment area could be divided into two symmetrical halves. The grade of dermatitis in each half was recorded (according to RTOG) weekly until 4 weeks after the end of radiotherapy. In the case of symptomatic dermatitis, topical corticosteroids were prescribed to the patients to use on the entire treatment area. Lotion were use twice daily from the beginning of treatment until 2 weeks after the end of RT, with no medication to be used on the other half. | Market product. The recipe contains: Lanolin oil, Glyceryl Stearate, Diluted Collagen, Tocopherol, Allantoin, and paraben. | Age and radiation field size had a significant effect on the grade of dermatitis. The prophylactic use of Aloe vera reduces the intensity of radiation induced dermatitis. The effect was more evident in patients undergoing radiotherapy with larger treatment field and higher doses of radiation. | The study verified the quantity (dose) of the lotion used. | [66] |
| Aloe vera L. Burman | gel soap | Determine whether the use of mild soap and aloe vera gel versus mild soap alone would decrease the incidence of skin reactions in patients undergoing RT. RCT. Oncological patients qualified for the RT. Group of patients applying mild soap and additional aloe vera gel and second group—control treatment used only soap. RTOG Acute Radiation Morbidity scale assessed weekly by physician or nurse. Unscented soap plus aloe vera gel or soap was applied liberally to the affected area daily after the RT in case of gel reapplied through day. Gel was washed off before RT. Standard care was recommended. | No information available concerning the composition, the quality assessment of the products. Gel without other active components | Aloe vera gel seemed to offer a protective effect over soap alone when the cumulative dose increased over time. At low cumulative dose levels no difference existed in the effect of adding aloe to soap regimen. | Soap is not a typical product to compare. Besides, the differences in treatment depended on the radiation doses applied and those were different for the control group and for the group using gel with aloe and soap which leads to conflicting results. | [67] |
| Aloe vera L. Burman | gel cream | Compare a anionic phospholipid-based (APP) cream and an aloe vera-based gel in the prevention and treatment of radiation dermatitis RCT. Pediatric patients treated by radiotherapy (dose of 23.4 Gy). Control group use APP cream. Subject skin comfort and dermatologic assessments were conducted before and weekly during treatment. Photography was performed at each evaluation time point and patients were seen 4–6 weeks after the completion of RT. CTC was used. Aloe vera-based gel or APP cream were applied symmetrically, once a day by nurse daily next to the radiation area after RT. | No information available concerning the composition and the quality assessment of the products. | APP-based cream showed a statistically significant advantage over aloe vera gel for skin comfort and dermatological assessment variables. Cream reduced dryness, redness, desquamation. No changes in CTC score before and after the treatment. | Complete data unavailable for objective evaluation of the study. | [11,63] |
| Aloe vera L. Burman | cream oil | To evaluate the efficacy of topical application of an aloe vera-based cream (AVC) for the prevention of ionizing RD. Clinical study. Head and neck cancer patients requiring therapeutic radiation treatment (dose >62 Gy). Patients were treated with AVC or Johnson Baby Oil (JBO). Acute skin reaction was monitored and classified according to RTOG four-point rating scale on a weekly basis. The preparation was applied 5 times per day at defined timespans after RT. During the study it was recommended not to use other preparations. When moist desquamation occurred, the topical application of JBO or ACV was discontinued topically and continued on the remaining skin area. | AVC and JBO are is market products Composition unavailable. Application: 5 cm3 JBO and 5 g AVC. | There was a statistically significant delay in the incidence of dermatitis at week three in the AVC application group. Application of AVC reduced the incidence of Grade 1, 2, and 3 dermatitis at subsequent time points, while Grade 4 dermatitis was not seen in either cohort. Continued application of AVC two weeks after the completion of RT was effective in reducing the average grade of dermatitis and was statistically significant. | This research and research with [67] indicate the usefulness of Aloe vera in delaying and mitigating dermatitis and promoting recovery. The action of this preparation is linked to the antioxidant properties of the Aloe vera. Plants from the aloe vera family decrease UVB-induced nociception, leukocyte infiltration, inflammation, and edema. Additionally, are effective in scavenging reactive oxygen and protecting DNA [68,69,70]. | [71] |
| Aloe vera L. Burman | gel lotion | A non-blinded three armed study of the effect of aloe vera gel, Essex lotion and no lotion on erythema was performed. BC patients who had undergone total mastectomy. Treatment with high-energy electrons (total dose 50 Gy). For measuring the erythema Near Infrared Spectroscopy, Laser Doppler Imaging and Digital Colour Photography were applied. Measurements were performed before the start of RT and there after once a week during the course of treatment. Aloe vera gel and Essex lotion were applied twice every radiation day in selected sites. | Aloe vera gel: Aloe barbadensis 97%, Aqua, Carbomer, Sodium Hydroxide, Phenoxyethanol, Methylparben, Butylparben, Ethylparben, Propylparben. Essex lotion consists of: Aqua, Petrolatum, Glycerin, Methyl Glucose Sesquistearate, Dimethicone, PEG-20, Palmitic acid, Steric acid, Cetyl Alcohol, Xanthan Gum, Magnesium Aluminum Silicate, Carbomer, Sodium Hydroxide. | The extent of erythema developed differed between patients. Some of them developed more severe erythema; however, no one had to stop their radiation treatment because of severe skin reactions. No significant median differences were observed between the pairs no lotion-Essex, no lotion-Aloe vera and Essex-Aloe vera for any of the techniques tested. | As indicated in manuscript Essex lotion is a commonly used lotion that is not registered as a medical product and therefore there are no specific recommendations for its use. | [72] |
| Aloe vera L. Burman | gel | Whether the adjunctive use of aloe vera gel might reduce the prevalence and/or severity of radiotherapy induced dermatitis. Randomized study patients with newly diagnosed BC (total dose 50 Gy). One group received aloe vera gel. Second group no treatment during RT. The patients were examined weekly by 2 physicians and dermatitis grade was registered (according ARMSC). In case of patients with second or higher degree dermatitis, additional local or systemic treatment such as antibiotics, corticosteroid or analgesics were applied. Aloe vera gel was applied twice a day in at least six hour intervals with a thickness of 1–2 mm on the radiation therapy field. | Aloe vera gel contain 1% additive such as: pectin, vitamin C and Natamycin | After 2 weeks first dermatitis was found among patients of both groups. Comparing the time of occurrence of dermatitis and their degree, no significant statistic difference were observed in both groups. Aloe vera gel did not show positive effect on prevalence or severity of radiation dermatitis in this study. | [73] | |
| Aloe vera L. Burman Turmeric curcuma longa L. Valeton Azadirachta indica A. Juss. Ocimum sanctum Linn | paste | Evaluation of efficacy and safety herbal paste compared to Beblomethasone cream in prevention radiation induced skin injury. CT. Patients of head and neck carcinoma. First group—patients received Beclomethasone cream. Second group received herbal paste. To assess radiation-induced reaction RTOG score were applied and group I versus group II compered. EORTC QLC-C30 was used for QoL assessment. Preparations were topically applied from the day-1 of radiotherapy till 4-weeks after completion of RT. | Paste was properly mixed with 100 g of Aloe vera juice and fresh Ocimum sanctum leaves, Azadirachta indica leaves (50 g each) and Curcuma longa roots (5 g). Herbal plants have been grounded up before mixing. | During the timespans of the study, i.e., after the 4th, 5th, 7th week and also after 6 months, skin reactions were less severe within the group using herbal preparation. On evaluating EORTC QLC-C30, on functional scale, physical, emotional, cognitive and role functioning deteriorated in Group 1 patients (except social functioning), while in Group patients all these modalities showed improvement at 6 months post-treatment. Evaluation on symptom scale revealed that fatigue, pain, dyspnea, appetite loss and insomnia got worsened in Beclomethasone group, except for diarrhea, constipation and nausea or vomiting, while in herbal pasta group patients, all 9 symptoms showed improvement 6 months after of completion of treatment. | Aloe vera was the basis for the powdered plants. Patients known to be allergic to ingredients of herbal paste or with allergy to steroids were excluded from study. No information available on the Gy dose applied to patients. | [74,75] |
| Angelica gigas NakaiLithospermum erythrorhizonSiebold and Zucc. | ointment | Efficiency and security evaluation of adjuvant application of Jaungo (JUG) for RD in comparison with general supportive care (GSC). RTC. Women with unilateral BC, after breast conservation surgery, undergoing RT, (total dose >45 Gy). Both groups will be subjected to GSC, but only the JUG group participants will apply adjuvant JUG ointment on the irradiated skin, twice a day (not applied within 4 h of daily RT). Treatment started at onset of RT and continued until 4 weeks after RT was completed or until radiation dermatitis subsided. Assessment of incidence rate of RD using the RTOG for toxicity gradation of 2 or more. Onset and duration of RD, and maximum pain score were also evaluated. GSC—skin clean and dry by gentle washing with neutral pH soap and patting with soft towel. No prophylactic creams or lotions for radiation dermatitis were allowed to either group. | Jaungo is a herbal ointment consisting of Angelica gigas radix (60.6 mg/g) and Lithospermum radix (72.7 mg/g). Carriers: Sesame Seed Oil, Beeswax, Swine Oil. Bioactive constituents shikonin 0.07 mg/g, decursin 3.6 mg/g. | JUG reduced the incidence of grade >2 and grade >3 RD in comparison with GSC. Delayed the onset of grade 2 dermatitis in terms of time onset of grade 3 and duration dermatitis and maximum pain score showed results comparable to those achieved with GSC, no adverse effect was observed. | Because of a low number of patients (29), the authors recommended further studies with a bigger sample of people. Those studies are currently ongoing [76] and [77]. In this article market product (composition unavailable) was compared with emulsion w/o (X-derm)—composition unavailable. | [78] |
| Angelica gigas NakaiLithospermum erythrorhizonSiebold and Zucc. | ointment | Estimate clinical application of Shiunko for reducing complications related to cancer treatment such as RD and hand foot syndrome induced by molecular target drugs. Various groups of patients took part in the research: 1st group patients with simple scalp dermatitis induced by RT for brain tumors. 2nd group: severe dermatitis from concurrent treatment with chemotherapy and RT for cancers including nasopharyngeal cancer. 3th group patients with dermal complications caused by molecular target drugs including hand-foot syndrome. Shiunko was applied in the same manner as in the treatment with standard ointment. The efficiency was assessed by defining the improvement degree—excellent (more than 80%), good (more than 50%), fair (less than 50%), and no effect (less than 30%). In comparison people were treated by corticosteroid. | Recipe unavailable. | Ointment is effective in treatment of scalp dermatitis caused by radiation and dermal complications induced by molecular target drugs since favorable therapeutic effects were observed in all group of patients. Shiunko showed prominent analgesic effect in all cases which were not achieved in corticosteroid treatment but also promoted healing in areas eroded by radiations. | Ointment Shiunko is the JUG ointment JUG, the same as in the study [78]. In our document we only showed cases treated with this ointment and its positive effect. No information available on the group using placebo. | [79] |
| Annona muricata L. | cream | Investigate the protective effects of Annona muricata leaf polysaccharide (ALP) on radiation induced skin injuries by using in vitro and in vivo models. Normal human epidermal keratinocytes (NHEKs) irradiated cell using 137Cs source in a Gammacell 40 Exactor. The dose rate used was 1 Gy/min. Performed cell viability, terminal deoxynucleotidyl transferase-mediated dUTP nic-end labeling assay and annexin V/propidium iodide (PI) staining to detect apoptosis. Pro-inflammatory cytokines (level of TNF-IL-6, and IL-1ß in the cell culture supernatants) were measured using ELISA. The mice were divided into five groups: (1) Normal group; (2) Irradiation + vehicle cream group; (3) Irradiation + 0.04% ALP (w/v) cream; (4) Irradiation + 0.2% ALP cream. The skin on the back was topically treated with 100 µL of vehicle or ALP cream for 7 days before and after irradiation. After treatment, mouse’s skin was under histopathological observation. | Vehicle cream: Water, Butyl Hydroxyl Toluene (0.001%), Dibasic Potassium Phosphate (0.2%), Cetyl Alcohol (0.5%), polyglyceryl-3-methylglucose distearate (5%). ALP extract was added to the vehicle cream at concentrations of 0.04 or 0.2%. | In normal human epidermal keratinocytes (NHEKs), ALP treatments reduced irradiation-induced apoptosis by increasing antioxidant enzymes activities, including (SOD) and catalase. Furthermore, ALP treatments decreased levels of interleukin-1ß, nucleotide-binding domain and leucine-rich-repeat-containing family pyrin 3 (NLRP3), and cleavage of caspase-1 and caspase-3. The topical application of the ALP cream showed protective efficacy against irradiation exposure, including the reduction of epidermal thickening, as well as an increase in the number of apoptotic cells and antioxidant enzyme (SOD and catalase) activities in skin tissue. ALP can be potentially used to treat radiation-induced skin injuries. | To determine whether ALP protects gamma irradiation- induced cell death by regulating antioxidant enzymes and in flammasome complexes, Authors analyzed the intracellular antioxidant enzymes activity and levels of pro inflammator cytokines. Hence, they are ones of the first studies of antioxidant action. Defines the mechanism of action of polysaccharides isolated from the extract and, based on that, the action of the cream, not only clinical studies or skin observation. | [2] |
| Boswellia serrata Roxb. ex Colebr. | cream | The cream was evaluated in terms of its safety, efficiency for the prevention and relief of radiation induced adverse effects. Clinical study. Patients adjuvant RT after surgery for mammary carcinoma. All measures, including photographic evaluations, were performed after the patients received a dose/breast of 50 Gy, usually reached in 5 weeks of irradiation, 5 doses weekly. Skin reactions were evaluated clinically using visual intensity and computer assisted skin color analysis whereas the toxicity was assessed according to RTOG scale. Visual grading scale: slight (slight redness, spotty, and diffuse), moderate (moderate and uniform redness), intense (intense redness). Cream was applied twice daily: immediately after RT and before bed-time in radiation therapy days, in the morning and at night in days with no radiotherapy administration. | Boswellia cream (2%, Bosexil) and placebo cream composition is unavailable. However, based on a cosmeceutical formulation based on Boswellic acids for the treatment of erythematous eczema and psoriasis [80] Bosexil contains: Aqua, Glycerin; Lecithin, Boswellia Serrata Resin Extract; Disodium Ethylenediaminotetraacetic Acid, Imidazolidinyl Urea, Polyacrylamide, C13-C14 Isoparaffin, Laureth-7, Hydrogenated polydecane, Carpylic/Capric Trigliceryde, Lecithin, Tocopherol, Ascorbyl Palmitate, Citric Acid, Phenoxyethanol. | Those studies indicate that applying cream with Boswellia S. is efficient for limiting the use of topical corticosteroids and can reduce the erythema and external dermal symptoms. The degree of reduction depended on the intensity of changes. The results in terms of visual intensity revealed that erythema was recorded as intense in a higher number of patients treated with base cream, compared with patients treated with boswellia cream (49.0% vs. 22.0%). Slight and moderate intensity of erythema were scored more frequently in the boswellia cream group than in base cream group: 36.4% vs. 20.3% and 41.8% vs. 30.5%, respectively. The mode values of the intensity of erythema for these samples were: intense (70.7%) for the base cream group and slight (62.5%) for the boswellia cream group. | It is not clear if 2% is the concentration of the extract in the recipe or the concentration of boswellic acids extracted from Boswellia serrata—those acids have anti-inflammatory properties. B. serrata extract reduces skin reddening and irritation, they even out the color and sooth the skin. According to the authors, further studies are necessary to compare with other topical preparations. | [81] |
| Calendula officinalis L. | ointment | Compare the effectiveness of calendula ointment with trolamine. Patients operated on for BC, received postoperative RT (2 Gy per session, five session per week). RTC. Two groups: 1st applied trolamine, 2nd calendula on the irradiated fields after each session. Occurrence of acute dermatitis of grade 2 or higher, occurrence of pain, the quantity of topical agent used, and patient satisfaction were investigated. Prognostic factors, including treatment modalities and patient characteristics, were also examined. Preparations were applied twice a day or more, depending on the occurrence of dermatitis and pain, until completion radiotherapy (not to use the agent 2 h or less before an irradiation session or before the treatment evaluation). Acute dermal toxicity was evaluated according to the RTOG scale at each irradiated volume. Pain was assessed each week on a 10-cm visual analog scale (VAS). No other prophylactic creams, lotions, or gels were allowed. Physicians can treat established dermatitis of grade 2 or higher and/or allergy as they considered appropriate. | Calendula ointment (market product) fabricated from a plant of the marigold family, Calendula officinalis. The digest is obtained by incubation at 75 °C in petroleum jelly to extract the liposoluble components of the plant. | The occurrence of acute dermatitis of grade 2 or higher was significantly lower (41% vs. 63%) with the use of calendula ointment than with trolamine. Patients receiving calendula has less frequent interruption of RT and significantly reduced radiation induced pain. | Trolamine is considered in many medical institutions as reference topical agent, Calendula ointment was more difficult to apply, but self-assessed satisfaction was greater. | [82,83] |
| Calendula officinalis L. | cream | Compare Calendula Weleda cream versus Essex cream in reducing the risk of serve ARSR. RCT. Patients with BC (2 Gy five day a week, total dose 50 Gy). ARSR was assessed by the nurse based on the RTOG score. Cream was applied twice a day, starting at the onset of RT and continuing until two weeks after final RT session or until ARSR was healed. Application topical agent include whole treatment area. Patients do not apply the cream within two hours of their RT. Daily washing with perfume-free soap and tap water were advised. | Calendula Weleda cream (market product) contains extract of Marigold Plants Officinalis 10%, Wool fat and Sesame Oil. Detailed composition not available. Essex cream probably contains: Water, Petrolatum, Liquid Paraffin. Both products contain no perfume nor coloring agent. | No differences in ARSR between calendula cream and aqueous cream and in patient reported symptoms (pain, burning, itching, pulling, tenderness) from the treatment area at any of the evaluation points. Thus, there is no reason to recommend one of the studied skin care product over the other. | Patients describe the calendula cream to be more difficult in application and absorption when compared to the Essex cream. Probably because it contains Wool fat. Essex patients were strongly advised to refrain from using other topical agents in the irradiated area. Calendula cream used in this study was not the same market product as the one used in Pommier [82] study (however, both contained 10% extract), besides, possible differences in efficiency can result from the reference sample, in this case Essex cream. | [83,84] |
| Calendula officinalis L. | lotion cream | Compare Calendula topical lotion efficacy versus standard of care sorbolene in reducing the prevalence of RD. RCT. Women undergoing BC RT, treatment phase up to 6 weeks Evaluate a prevalence of acute radiation-induced dermatitis (RTOG grade 2+) assessed at multiple skin sites. Participants were encouraged to begin applying their treatment 2–3 days prior to commencement of radiation therapy. | Calendula lotion (<5% v/v): Calendula tincture and extract, Lecithin, Glycerine, Ethanol, Xanthan Gum, Distilates (Rose, Chamomile, witch hazel, extracts (Citrus, Gum, Rosemary), Rice Bran Oil, Ascorbic acid, Wheatgerm Oil, Arrowroot, Guar Gum, Sodium Hyaluronate, Lactacid acid. Sorbolene: 10% glycerin in cetomacrogol cream other ingredients: Ceteareth-20, Cetearyl Alcohol, Glycerin, Mineral oil, p-chloro-m-cresol, Petrolatum, Aqua. | No detectable difference in prevalence of radiation-induced dermatitis grade 2+ between Calendula and Sorbolene groups. | Study carried out on a small group of people. People with allergy to Marigold, salicylate, or taking aspirin were excluded from study. | [85] |
| Calendula officinalis L. | oil | Efficiency evaluation of Calendula officinalis in relation to Essential Fatty Acids (EFA) for prevention and treatment of RD. RCT. Patients with head and neck cancer, received RT. Two groups: control applied EFA and experimental used Calendula oil. Radiodermatitis were assessed by the toxicity grade, according to the criteria RTOG. The participant’s skin in the irradiation field was evaluated in the first radiotherapy session, every five sessions and 30 days after the end of treatment. The evaluation of skin toxicity was performed by a team of trained researchers. Participants applied EFA or calendula topically. Research protocol: mode of application—application to the skin with a gauze soaked with the product of research in all treatment field every 12 h (twice/day), from the first to the last day of RT session; first application—hospital: conducted by the research collaborator—average of 10 cm3/application; during application, study participant and/or family member. | EFA: Sunflower Oil, 1% Vitamin A, 0.2% Vitamin E and 5% Caprylic acid Calendula oil: 4% Calendula Oil, 1% Vitamin A and Liquid vaseline. | Statistically significant evidence that the proportion of radiodermatitis grade 2 in EFA group is higher than Calendula group. Lower risk of developing radiodermatitis grade 1, form experimental group, it makes the usage of Calendula oil more effective. | Excluded patients with allergic reaction in the use of one of the research products (EFA or Calendula officinalis). Due to the physicochemical form of the products, they were applied to gauze. | [86] |
| Calendula officinalis L. | ointment | Evaluation of anti-inflammatory action and of the impact on ionizing radiation induced skin toxicity of the extract from Calendula officinalis (CO) and Ching Wan Hung (CWH)—ointment. SKH-hr1 hairless mice (10 Gy/day for 4 days). Skin toxicity and inflammatory factors (Serum interleukin (IL)-1α monocyte, chemotactic protein-1 (MCP1), keratinocyte-derived chemokine (KC), and granulocyte colony-stimulating factor (G-CSF)) were evaluated at multiple time points up to15 days post-radiation. Mice were evaluated every 2 days following IR with and without topical treatment of CO and CWH. IR-induced skin reactions, erythema, blood vessel dilation, and crust/scaling, were noted. Gross assessment of early radiation dermatitis, erythema, edema, dyspigmentation, desquamation, exudation, and ulceration, was conducted using the dermatoscope. Skin toxicity was evaluated and scored as either 0 (no visible lesion), 1 (moderate lesion), or 2 (severe lesion), for both erythema and blood vessel dilation. | CWH is a Chinese herbal ointment which is sold as an over-counter soothing lotion for burns. Some of the active ingredients include: lobelia (27.5%), myrrh (17.5%), tangkuei (12%), borneol (12%), sanguisorba (8.5%), chaenomeles (8.5%), frankincense (8.5%), carthamus (8.5%), and pistacia (8.5%), CO extract to ointment available with the trade name Pommade au Calendula Par Digestion. Contains the extract in 4% concentration. | Both CO and CWH significantly inhibited IR-induced MCP1 KC and G-CSF. IR-induced erythema and blood vessel dilation were significantly reduced by CWH but not by CO at day 10 post-IR. Both agents inhibited IR-induced IL-1α, MCP1 and vascular endothelial growth factor. There were continuous inhibitory effects of CWH on IR-induced skin toxicities and inflammation. In contrast, CO treatment resulted in skin reactions compared to IR alone both CO and CWH reduce IR-induced inflammation and CWH reduced IR-induced erythema. | Looking at the composition, it is not surprising that the preparation with higher quantity of active substances showed better result. The same market product as in Pommier study [82]. | [87] |
| Centella asiaticaL. | cream | Attempted to determine whether prophylactic treatment with herbal creams as well as a commercial moisturizing cream could reduce acute skin reaction RCT. BC patients undergoing RT (total physical dose 40-5-Gy). 5 different groups: 1—no treatment (standard care, no creams or substances). Other groups using creams containing respectively extracts from Centella asiatica L., Cucumis sativus L., Thunbergia laurifolia or using moisturizing market product (Johnson and Johnson). Participants’ skin was evaluated by an oncologist-radiologist weekly up to one month after the irradiation in order to identify all kinds of dermatologic reaction (according to RTOG score). Satisfaction with the preparation was also evaluated (scale 1–5 with 5 being mostly satisfied and 1 being least). Creams were applied once a day after the first session of radiotherapy up to one month after the irradiation. | Centella asiatica 7% (w/w) Information on other components unavailable. They do not contain fragrance. Market creams available in Thailand. | Topical application of all herbal cream or the moisturizing cream could neither reduce the severity nor delay onset of dermatitis compared with no treatment group. Cucumis sativus cream was shown to help with skin recovery post-irradiation. Study authors advise to prophylactically use moisturizing preparations on the irradiated area of skin. | One clinical study which evaluated three plants Centella asiatica L., Cucumis sativus L., Thunbergia laurifolia. Before the study allergic tests were made for unwanted reaction to the extracts and the moisturizing cream. | [88] |
| Chamomilla recutita L. Rauschert (Matricaria chamomilla L.) | gel cream | Assessed safety and potential efficacy of a chamomile gel compared with urea cream to prevent and delay acute RD. Before starting the comparative clinical study chamomile gel in various concentrations was analyzed: 2.5%, 5.00% and 8.35%. Considering the effectiveness and the safety, the concentration of 8.35% was chosen for the clinical study. Safety assessment was based on the presence or absence of skin toxicity according to RTOG score and time to development of erythema, measured as number of sessions of radiation therapy before erythema development. RCT. Patients with head and neck cancer receiving RT with or without concomitant CT. Group chamomile gel comparing with urea cream group. Nurse was evaluated the person’s skin weekly (skin toxicity according RTOG score) until the end of treatment. Photographs of the regions of the participant’s head and neck on a weekly basis were taken. During the study, it was recommended to use skin care with a moisturizing soap (DoveTM) and not to apply any products to the irradiated area to avoid undesirable bolus effects. Product were applied topically 3 times a day (morning, afternoon and night) on the skin of the irradiated area for the entire period of the RT (5 day week for 6–8 week). | Data about composition not available. Both product’s validity was 3 months. | The gel containing 8.35% chamomile was still safe when compared to concentrations of 2.5% and 5.0% used by participants receiving RT for head and neck cancer. Increasing concentrations tended to delay the development of erythema in those participants. Formulation of 8.35% chamomile gel was not statistically different from urea cream in the delay the development of grades 1 (2.08 to 2.2 weeks) and 2 (5.1 weeks to 4.5 weeks) RD, though the effect size of delay of Grade 2 was of moderate size. No statistical differences over time were seen between the groups on adverse events. Itching, burning and hyperpigmentation were more frequently reported in the urea group. | According to the Brazilian Health Surveillance Agency (Agęncia de Vigilância Sanitária—ANVISA), products made of Chamomile recutita do not require proof of safety because chamomile is already registered at the Brazilian Simplified Registry of Traditional Phytotherapic Products. The study in which the concentration of the active substance was defined before starting the comparative study. | [89,90] |
| Cucumis sativus L. | cream | the same as in Centella asiatica L. research [88] | Cucumis sativus L. 20% (w/w) No information available on remaining components. They do not contain fragrance. Market creams available in Thailand | Topical application of all herbal cream or the moisturizing cream could neither reduce the severity nor delay onset of dermatitis compared with no treatment group. Cucumis sativus cream was shown to help with skin recovery post-irradiation. It is related to the high content of water and soothing properties reducing irritations and skin oedema in cucumber. Cucumber cream proved efficient in regeneration of irradiated skin which most probably is also linked to the presence of tannins and flavonoids. | One clinical study analyzing three plants: Centella asiatica L., Cucumis sativus L., Thunbergia laurifolia. Before the study there were allergic tests made to check on side effects of the extracts and moisturizing creams. Cucumber has protective effects against both reactive oxygen species and reactive carbonyl species by free radical scavenging activity. | [88] |
| Glycyrrhiza glabra Torr. (Licorice root) | cream | The same as in Achillea milefolium L. research [59] | The same as in Achillea milefolium L. research [59] | The same as in Achillea milefolium L. research [59] | The same as in Achillea milefolium L. research | [59] |
| Green tee Black tee | cream compress of aqueous tea extracts | To explore the effect of topically-applied tea extracts on the duration of radiation-induced skin toxicity. Patients with head, neck or pelvis area cancer undergoing RT (daily fractions of 1.8–2.0 Gy). During the study, patients used standard skin care program which consisted of once-daily treatment with moisturizing creme. In case of erythema, the cream was applied 2–3 times and stopped with occurrence of moist desquamation. Green or black tea extracts were applied to the irradiated skin area with lesions of 2nd degree and higher (RTOG score) 3 times per day for 10 min from the occurrence of moist desquamation. Dermal toxicity was evaluated daily by the qualified medical personnel before each extract application. The disappearance of moist desquamation was considered as the end of the study. Tea extracts were compared for their ability to modulate IL-1ß, IL-6, IL-8, TNFα and PGE2 release from human monocytes. Effects of tea extracts on 26S proteasome function were also assessed and NF-κβ activity was monitored by EMSAs. Viability and radiation response of macrophages after exposure to tea extracts was measured by MTT assays. | Moisturizing cream—market preparation containing 3% of urea. | Tea extracts are effective for treatment of patients suffering from acute dermal toxicity caused by irradiation. Tea extracts supported the restitution of skin integrity, inhibited proteasome function and suppressed cytokine release. NF-κβ activity was altered by tea extracts in a complex, caspase dependent manner, which differed from the effects of epigallocatechin gallate. Analyzed tea extracts, as well as epigallocatechin-gallate, slightly protected macrophages from ionizing radiation. The molecular mechanisms underlying the beneficial effects are complex, and most likely not exclusively dependent on effects of tea polyphenols such as epigallocatechin-gallate. No difference between green and black tea in duration of grade 2+ skin reactions in patients treated for cancer of the head and neck region. | There is no information, if without the application of moisturizing cream the extracts effect on skin would be the same. | [91] |
| Camellia sinensis L. Kuntze (Chinese tea) | gel lotion cream | Evaluation of the effectiveness for the preparations with Camellia Sinesis Nonfermentatum extract (CSNF) (NPE®) in prevention and recovery of ARSR and skin care during postoperative whole breast RT. Open label Pilot-study. 20 patients received adapted post-operatory radiotherapy (45 Gy/20 fraction boost: 10–15 Gy/4–6 fractions or ± whole breast: 40 Gy/15 fractions). Data from these study were compared with 100 retrospectively collected matched data sets derived from hospital records. These routine medical care patients were treated according to the hospital treatment guidelines and recommendations of the SASRO. The assessments of ARSR Grades 1, 2, 3, and 4 were performed according to CTCAE. Lotion (0.4% CSNF) was applied 2x per day 7 days before RT—during RT on irradiated zones (but not directly before the RT), 4–8 weeks after RT if necessary. CSNF prophylactic gel (2.5%) was applied 1–2 h before each RT session on the day of irradiation. Irradiated zones were: thoracic and supraclavicular zones, front and back. | Composition unavailable. The only information available concerns the % of extract in the given form of preparation and that the extract is proprietary. Comparative preparations were various market preparations such as Excipial® hydrolotion (oil-in-water emulsion containing urea), Bepanthol® body lotion or Bepanthen® cream (preparations contained dexpanthenol and sodium hyaluronate or sodium hyaluronate and silver sulfadiazine. | The study showed that combined use of gel and CSNF balsam retarded the occurrence of ARSR ≥ G2 and can reduce the risk of moist desquamation of irradiated skin by 50%. The proportion of patients requiring rescue treatment during RT and follow-up was markedly higher in the control compared to the CSNF group (1% to 51% vs. 0% to 15%). CSNF gel and lotion were well tolerated both during and after RT. Camellia Sinensis Nonfermentatum Extract is potentially effective in healing skin irritation in women with breast cancer. | Comparative studies with the data from hospital files. The first study in which two types of skin care preparations were used, they contained the extract from a given plant but there was no comparison with the placebo group. According to Authors, preparations containing oils cannot be used directly before the RT because they can increase the risk of skin irritation following radiation concentration in tissues. The CSNF extract reduces oxidative stress and DNA damage, downregulates numerous factors related to apoptosis, inflammation, and carcinogenesis in experimental studies, and showed a similar protective effect for skin of healthy volunteers exposed to UV-light. | [92] |
| Hypericum perforatum L. | ointment (gel) oil | Effectiveness of Holoil® series in treatment of acute skin toxicity (G2 acute). Sigle-arm, prospective observational study. Patients undergoing RTor chemo radiotherapy for head and neck cancer (70 Gy/35 fractions (2 Gy daily). Medical evaluation consisted of a weekly clinical evaluation with a visual examination of the neck region skin performed by the physician in charge of the patient and a consequent physician-rated score of acute skin toxicity up to 90 day after end of treatment (according to RTOG/EORTC toxicity scale). Holoil® product series treatment were started whenever bright erythema, moderate oedema or patchy moist desquamation were observed. For erythema and/or oedema gel preparation was employed. For patchy moist desquamation the oil preparation was administered. Holoil® was used during all RT course and during follow up time, until acute skin toxicity recovery. Before the lesions appeared, patients received moisturizing cream. Holoil® was applied on the bilateral neck 2–3 times a day, at least 3 h before treatment session. Other creams or cosmetic products in the irradiated area were prohibited. | No information available on the product composition (market products). Carrier for Hypercium perforatum L. was neem oil. According to [93]: Holoil® gel: Ingredients: Melia Azadirachta Seed Oil; Olea Europaea Oil; Hypericum Perforatum Flower Extract, Excipients: Aqua; Propylene Glycol; Ciclodextrin; Carbomer; Triethanolamine; Phenoxyethanol; Benzoic Acid; Dehydroacetic Acid; Sodium Dehydroacetate; Ethylhexylglycerin; Aroma. Holoil® oil: Ingredients: Melia Azadirachta Seed Oil; Olea Europaea Oil; Hypericum Perforatum Flower Extract. | The maximum detected acute skin toxicity was Grade 1 in 7% of patients, Grade 2 in 68%, Grade 3 in 25%, while at the end of RT was Grade 0 in 3.5%, Grade 1 in 32%, Grade 2 in 61%, Grade 3 in 3.5%. G2 acute skin toxicity mainly started at weeks 4–5; G3 begun during weeks 5–6. Median times spent with G2 or G3 toxicity were 17.5 and 11 days. Time between maximum acute skin toxicity and complete skin recovery after RT was 27 days. | Various physicochemical forms were used in the studies, depending on the radiodermatitis type: Holoil® as gel (erythema and oedema) or oil formulation (moist desquamation). Patient’s compliance was consistent, with no particular complaints or difficulties. Carrier neem oil itself has anti-inflammatory, antioxidant and regenerating properties. No information available on the concentration of Hypercium perforatum L. in products. According to Authors Holoil® proved to be a safe and active option in the management of acute skin toxicity. A prophylactic effect in the prevention of moist desquamation may be hypothesized for hypericum and neem oil and need to be tested within a prospective controlled study. | [94] |
| Nigela sativa L. | gel | Evaluate the effectiveness of Nigella sativa L. extract on preventing the incidence of ARD. RCT. BC patients undergoing RT after breast surgery (minimum total prescribed dose, 50 Gy). 2 group: placebo and N. sativa 5% gel. The severity of ARD, the incidence of moist desquamation, worst experienced pain, and skin-related quality of life (SRQOL) scores were assessed weekly during RT. Preparations application: twice daily during RT period at least two hours before and after RT. After applying the gel, patients were asked to wait for at least 10 min before dressing and not to wash the affected area for at least 2 h. | N. sativa dried extract (5% w/w), Glycerol (5%), Carbopol®940 (1%), Triethanolamine (0.09%), Methylparaben (0.18%), propylparaben (0.02%), water up to 100% Placebo gel contain all of these ingredients except the N. sativa extract. | Group of patients treated with the N. sativa gel developed ARD significantly less frequently compared to those who used the placebo. The incidence time of grade 2 and 3 dermatitis was prolonged significantly with N. sativa gel as compared to placebo (35 vs. 29 days and 42 vs. 40 days, respectively). Also occurrence of moist desquamation was delayed 37 vs. 33 days for N. sativa gel vs. placebo respectively. At week 3 the mean score of the worst pain that patients experienced in N. sativa gel was significantly lower than in placebo group. No significant effect on the SRQOL after application of N. sativa gel was observed. | Both extract and gels were obtained by the authors. Active substance in the isolated extract was Thymoquinone the concentration of which in gel was 0.01% Gels were also studied with respect to their microbiological purity and stability. Participants with known allergy or hypersensitivity to N. sativa or any ingredients of the gel were excluded from the study. | [95] |
| Silybum marianum (L.) Gaertner | gel | Investigate the efficacy of silymarin gel in prevention of RD. RCT. Patients with BC received placebo or silymarin gel on chest walk skin following modified radical mastectomy (total radiation dose of 50 Gy). RD severity was assessed weekly based on RTOG and NCI-CTCAE criteria radiodermatitis grading scale for 5 weeks. Preparations (half fingertip unit) applied daily starting at the first day of RT for 5 weeks. | 1% silymarin gel Used in the recipe dry extract contain 80% active ingredient based on silymarin flavonolignans (including silybin, silychristin, silydianin, 2,3-dehydrosilybin, and 2,3-dihydrosilychristin). No information available on the remaining components for both placebo gel and silymarin gel | The median NCI-CTCAE and RTOG scores were significantly lower in silymarin group at the end of the third to fifth weeks. The scores increased significantly in both placebo and silymarin groups during RT but there was a delay in RD development and progression in silymarin group. Prophylactic administration of silymarin gel could significantly reduce the severity of RD and delay its occurrence after 5 weeks of application (80% patients in this group remained asymptomatic). None of patients in silymarin group experienced grades higher than 1 during RT in contrast to placebo group were was patients with grade 2 and grade 3. | Were excluded from the study people with history of allergy to silymarin, history of autoimmune and connective tissue diseases, concomitant use of nonsteroidal anti-inflammatory drugs, corticosteroids, and other immunosuppressive or antioxidant medications. Because Silymarin could reduce the severity of radiodermatitis the silymarin gel should be prescribe before the beginning of the RT. The authors of the study suggest that the silymarin 1% gel, and increasing the silymarin content of the gel may increase its efficacy in RD prevention. | [96] |
| Silybum marianum (L.) Gaertner | cream | Silymarin-based cream (Leviaderm®) was tested in efficacy in prevention of RD comparison to standard of care (SOC). Patients with histologically documented diagnosis of BC were evaluated after breast-conserving surgery followed by RT with 50.4 Gy plus boost 9–16 Gy. Participants were documented consecutively before, during, and 4 weeks after the scheduled end of RT. The occurrence of side effects and adverse drug reactions were recorded unblinded by the medical staff of the department during the weekly clinical examinations. One group of patients were treated with the silymarin based cream, second group were documented receiving a panthenol-containing cream interventionally, if local skin lesions occurred. The acute skin reactions were classified according to the RTOG and VASscores. SOC treatment consisting out of 5% dexpanthenol containing cream, which was applied as an interventional treatment to the affected breast skin after occurrence of the first signs of skin alterations (e.g., erythema) every day during RT and, thereafter, until skin recovered to normal. Silymarin-based cream was applied to the skin three times a day, 2 weeks before beginning RT, during RT, and 2 weeks afterwards. During RT, silymarin-based cream was applied daily at least 2 h before radiation. Silymarin-based cream was not applied to open wounds. | Leviaderm® market product, patented. It is mainly based on silymarin (Silybum marianum, content 0.25%), Adelmidrol®, vitamin E, bisabolol, and extracts from Vitis vinifera, Epilobium angustifolium, and Hordeum vulgare. The reference cream was the cream used in standard care. No detailed recipe for the product (contains 5% dexpanthenol) | The median time to toxicity was prolonged significantly with silymarin-based cream (45 vs. 29 days (SOC)). Only 9.8% of patients using silymarin-based cream showed grade 2 toxicity in week 5 of RT in comparison to 52% with SOC. At the end of RT, 23.5% of patients in the silymarin-based study group developed no skin reactions vs. 2% with SOC, while grade 3 toxicity occurred only in 2% in the silymarin-based arm compared to 28% (SOC).These results reaching statistical significance for RTOG are in line with those determined for subjective toxicity (VAS). Silymarin-based cream was well tolerated and can, thus, be used over several weeks. | Patients with allergies to the product were excluded from study. According to Authors Leviaderm® represents a new concept of cream by combining prevention and therapy of RD. It may induce antioxidative actions when skin is exposed to irradiation because silymarin, protect against free radical-induced inflammation. Additonaly Adelmidrol®, or N,N-bis (hydroxyethyl)-nonandiamide, here used in a subclinical concentration of 0.5%, belongs to a family of lipidic molecules collectively defined as ALIAmides, which in preclinical and clinical testing using therapeutical concentrations (at least 2%) have been reported to restore skin reactivity by down regulating mast cell hyperactivity. To confirm the results of this nonrandomized, observational trial, this product should be tested in larger multicenter studies in this setting. | [97] |
| Thunbergia laurifoliaLindl. | cream | The same as Centella asiatica research [88] | Thunbergia laufrifolia 5% (w/w) No information available concerning the remaining components. They do not contain fragrance Market creams available in Thailand. | Topical application of all herbal cream or the moisturizing cream could neither reduce the severity nor delay onset of dermatitis compared with no treatment group. Cucumis sativus cream wash shown to help with skin recovery post-irradiation. Authors recommend prophylactic application of moisturizing preparations on irradiated area of skin. | One clinical study in which three plants were analyzed: Centella asiatica L., Cucumis sativus L., Thunbergia laurifolia. Before the study, allergy tests were carried out to prevent side effects of extracts and moisturizing cream. | [88] |
| Turmeric curcuma longaL. | cream oil | Assess effectiveness of Vicco turmeric cream (VTC) on radiodermatitis. RCT. Patients with head and neck cancer scheduled to receive chemoradiotherapy or RT (dose 60 Gy). Two groups of patients first received topical Johnson’s baby oil (JBO), second group received VTC. Acute skin reactions were assessed twice weekly (according to RTOG scores) by an investigator who was unaware of the details. Time of application: 2 weeks after the end of the RT, starting on day 1, preparations were applied 5 times per day on the irradiated area. | VTC contain: extracts of Turmeric curcuma longa (16% w/w), Sandalwood Oil in a non-greasy base Oil—petroleum oil Oil and VTC cream both are market preparations. | Cream based on Curcuma longa and Sandalwood oil was effective against post-radiation dermatitis. Significant reduction in grades of dermatitis was seen at all time points, including 2 weeks post RT. The occurrence of grade 3 dermatitis was lower in the cohorts using VTC and was statistically significant. No adverse effects (allergic reactions) were found in the groups, indicating that Curcuma cream is safe for patients with head and neck cancer. | VTC was shown to be effective in preventing radiodermatitis and needs to be validated in larger double-blind trials. | [98] |
| Turmeric Curcuma longaL. | cream oil | To ascertain the benefit of Vicco turmeric Ayurvedic cream (VTC) in preventing radiodermatitis. Investigator-blinded randomized trial (double blind). Women receiving breast radiation therapy (50 Gy in 2 Gy fractions daily for 5 weeks). Two groups of patients first received topical Johnson’s baby oil (JBO) second group received VTC. To assess the delay in the appearance and the degree of severity (RTG score) of dermatitis throughout the study period. Application of products 5 times a day. | Market preparations. No information on composition available. VTC contain: extracts of Turmeric Curcuma longa (16% w/w), Sandalwood Oil in a non-greasy base. | Topical application of VTC delayed and mitigated the radiodermatitis. Compared to the JBO significant decrease in the incidence of 1 grade was seen at two week, and also in grade 2 and 3 at week 3 and 4 respectively in the VCT cohort. VCT cream significantly reduced radiation dermatitis. | Studies extended with regards to Pallaty [98]. Studies carried out with Johnson&Johnson company. Cream dose 5 g at each application and 5 cm3 for the oil. The authors tend to attribute the effectiveness to the curcuma and oil properties such as: anti- inflammatory, antioxidant, modulating cytokines and enhancing wound healing process. All of it contributes to the mechanism giving protective effects. | [99] |
| Turmeric Curcuma longaL. Valeton | gel lotion | The assessment of the prophylactical application of topical means in preventing or reducing RD and associated pain. RCT. BC patients, scheduled to receive conventional fractionated RT (total dose 44 to 66 Gy). Market preparations: Psoria Gold Curcumin gel (containing Curcumin extract), HPR Plus and placebo gel were applied. For pain assessment Skin Pain Inventory form was used. The evaluation of RDS (radiation dermatitis severity) was done by the physician or by qualified personnel. Preparations were applied on irradiated areas three times daily starting the first day of RT until 1 week after treatment completion. Standard self-care was recommended. | Psoria Gold Curcumin gel: Water Aloe Vera Leaf Juice Powder, Curcumin Extract, Hydroxypropyl Methylcellulose, Isopropyl Alcohol, Glycerin, Niacinamide (Vitamin B3) Acrylates/C10-30 Alkyl Acrylate Crosspolymer, Aminomethyl Propanol, Caprylhydroxamic Acid, Glyceryl Caprylate, Citric Acid. HPR Plus (lotion): Sodium Magnesium Fluorosilicate, Cyclomethicone, Phosphoric Acid, Sodium Chloride, Sodium Bicarbonate, Hypochlorus Acid, Water. Placebo gel (Psoria Gold)—composition unavailable | Mean RDS scores did not significantly differ between study arms. Additionally, no differences were detected in self-reported skin problems or pain ratings between the treatment groups in the total study sample. Exploratory subgroup analysis suggests that prophylactic treatment with topical curcumin may be effective for minimizing skin reactions and pain for patients with high breast separation who may have the worst skin reactions. | In the recipe including curcumin there’s also aloe vera extract. | [100] |
| Turmeric Curcuma longaL. Valeton | gel | Determining the effect of topical curcumin treatment on radiation burns Mini-pig model. Histological and clinical changes (ulceration, erythema, moist desquamation, dry desquamation) were observed five weeks after radiation exposure (total dose 50 Gy). Curcumin gel with ethanolic extract applied twice a day for 35 days. First application just after radiation. The reference sample was vehicle cream. The preparation dose was 200 mg/cm2 of skin. | Curcumin gel: Carbopol 934P, Water, Methanol, Ethanol, Triethanoloamine Dose of curcumin 200 mg/2 cm3 ethanol on 200 mg carbomer. Vehicle cream (hydrogel): the same ingredients as curcumin gel but without active ingredients such as curcumin extract. | Decreased the epithelial desquamation after radiation group treated with curcumin—showed reduced expression of cyclooxygenase-2 and nuclear factor-kappaB. Curcumin treatment stimulated wound healing. | The authors obtained the gel with the extract themselves. They also refer to the results of study [101] which demonstrated that the gel showed the highest permeability of curcumin without skin irritation or anti-inflammatory effects. Physicochemical study of the preparation was not presented. Besides, in the study the authors use the terminology vehicle cream whereas it is a gel (hydrogel) with no active substance (curcumin) added. | [102] |
| Action | Plant Species | Chemical Compounds | Indications |
|---|---|---|---|
| Anti-inflammatory | Achiellea millefolium L. | flavonoids | skin irritation sensitive skin dry skin |
| Aloe vera L. Burman | polysaccharides, mucilage | ||
| Annona muricata L. | flavonols, sesquiterpene lactones, acetogenins | ||
| Azadriachta indica A. Juss | isoprenoids, catechins, tannins, | ||
| Boswellia serrata Roxb. ex Colebr. | boswelin acids | ||
| Calendula officinalis L. | saponins, flavonoids, polysaccharides | ||
| Centella asiatica L. | triterpene saponins | ||
| Chamomilla recutita Rauschert | flavonoids | ||
| Cucumis sativus L. | cucurbitacins, phytosterole, unsaturated fatty acids | ||
| Glycyrrhiza glabra Torr. | triterpene saponins, flavanones | ||
| Green tea | polyphenols | ||
| Hypercium perforatum L. | flavonoids, oligomeric proanthocyanindines, xanthones, acylfluoroglucinols, derivatives of caffeic acid | ||
| Lithospermum erythrorhizon Siebold and Zucc. | naftochinony | ||
| Nigela sativa L. | flavonoids, alkaloids, unsaturated fatty acids | ||
| Ocimum santum Linn | terpenes, unsaturated fatty acids, saponins | ||
| Silybum mariannum L. Gaerther | unsaturated fatty acids, flavonolignans | ||
| Thunbergia laurifolia Lindl. | iridoid glucosides, rosmarinic acid | ||
| Turmeric curcuma longa L. Valeton | curcuminoids | ||
| accelerating skin healing and regeneration | Aloe vera L. Burman | glycoprotein, mukopolysaccharides, amino acids, hydroxyquinone glycosides, minerals | wounds burns scars sensitive skin |
| Hypercium perforatum L. | hyperforin, flavonoids | ||
| Annona muricata L. | lactones, acetogenins | ||
| Lithospermum erythrorhizon Siebold and Zucc. | naphthoquinones | ||
| Cucumis sativus L. | phytosterols, tannins, | ||
| Calendula officinalis L. | saponins, flavonoids | ||
| Azadirachta indica A. Juss | tanins | ||
| Centella asiatica L. | triterpenes, flavonoids | ||
| antimicrobial (bacteria, fungi) | Achiellea millefolium L. | polyacetylenes, flavonoids, sesquiterpene lactones, tannins | skin infections protection of the skin against infection |
| Angelica gigas Nakai | tannins, tannins, aliphatic acids | ||
| Azadirachta indica A. Juss | isoprenoids, tannins, polyphenols | ||
| Calendula officinalis L. | aliphatic acids, polysaccharides, saponins, flavonoids | ||
| Camellia sinesis L. Kuntze | catechins | ||
| Centella asiatica L. | triterpene saponins | ||
| Chamomilla recutita L. Rauschert | cyclic ethers, sesquiterpene alcohols | ||
| Glycyrrhiza glabra Torr. | flavonoids, triterpene saponins | ||
| Lithospermum erythrorhizon Siebold and Zucc. | naphthoquinones | ||
| Nigela sativa L. | alkaloids, triterpene saponins | ||
| Ocimum santum Linn | phenols, triterpenoids, tannins | ||
| Turmeric curcuma longa Valeton | curcuminoids | ||
| moisturizing | Aloe vera L. Burman | polysaccharides, glycoprotein | dry skin sensitive skin |
| Azadirachta indica A. Juss | polysaccharides, proteins | ||
| Cucumis sativus L. | amino acids, minerals, pectins, | ||
| antioxidant | Annona muricata L. | phenolic compounds, vitamins, carotenoids, enzymes | neutralization of free radicals, protection of DNA strands and support of collagen and elastin production delay in lipid oxidation regeneration of primary antioxidants |
| Azadirachta indica A. Juss | polyphenols, limonoids | ||
| Camellia sinesis L. Kuntze | polyphenols, flavonoids, phenolic acids, vitamins | ||
| Centella asiatica L. | flavonoids, triterpenes | ||
| Chamomilla recutita L. Rauschert | flavonoids, phenolic compound | ||
| Cucumis sativus L. | phenolic compounds, vitamins, | ||
| Glycyrrhiza glabra Torr. | flavonoids | ||
| Green tea | Catechins | ||
| Lithospermum erythrorhizon Siebold and Zucc. | naphthoquinones | ||
| Nigela sativa L. | tannins, vitamins, flavonols | ||
| Silybum marianum L. Gaertner | flavonolignans, phenolic compound | ||
| Thunbergia laurifolia Lindl. | flavonoids, polyphenols, | ||
| Turmeric curcuma longa Valeton | feluric acids, polyphenols | ||
| antiseptic—disinfecting | Angelica gigas Nakai | tannins, alifactic acids, | cleansing of skin and wounds |
| Azadirachta indica A. Juss | isoprenoids, polyphenols | ||
| analgesic anesthetics | Achillea millefolium L. | flavonoids, alkaloids | local analgesic effect |
| Boswellia serrata Roxb. ex Colebr. | boswellic acids | ||
| Ocimum santum Linn. | triterpenoids | ||
| antipruritic | Ocimum santum Linn. | terpenes, tanins | itch |
| anti-edematous | Cucumis sativus L. | tanins | swelling |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulawik-Pióro, A.; Goździcka, W.J. Plant and Herbal Extracts as Ingredients of Topical Agents in the Prevention and Treatment Radiodermatitis: A Systematic Literature Review. Cosmetics 2022, 9, 63. https://doi.org/10.3390/cosmetics9030063
Kulawik-Pióro A, Goździcka WJ. Plant and Herbal Extracts as Ingredients of Topical Agents in the Prevention and Treatment Radiodermatitis: A Systematic Literature Review. Cosmetics. 2022; 9(3):63. https://doi.org/10.3390/cosmetics9030063
Chicago/Turabian StyleKulawik-Pióro, Agnieszka, and Weronika Joanna Goździcka. 2022. "Plant and Herbal Extracts as Ingredients of Topical Agents in the Prevention and Treatment Radiodermatitis: A Systematic Literature Review" Cosmetics 9, no. 3: 63. https://doi.org/10.3390/cosmetics9030063
APA StyleKulawik-Pióro, A., & Goździcka, W. J. (2022). Plant and Herbal Extracts as Ingredients of Topical Agents in the Prevention and Treatment Radiodermatitis: A Systematic Literature Review. Cosmetics, 9(3), 63. https://doi.org/10.3390/cosmetics9030063