

Efficacy and Safety of Monopolar Radiofrequency for Tightening the Skin of Aged Faces

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. RF Therapy
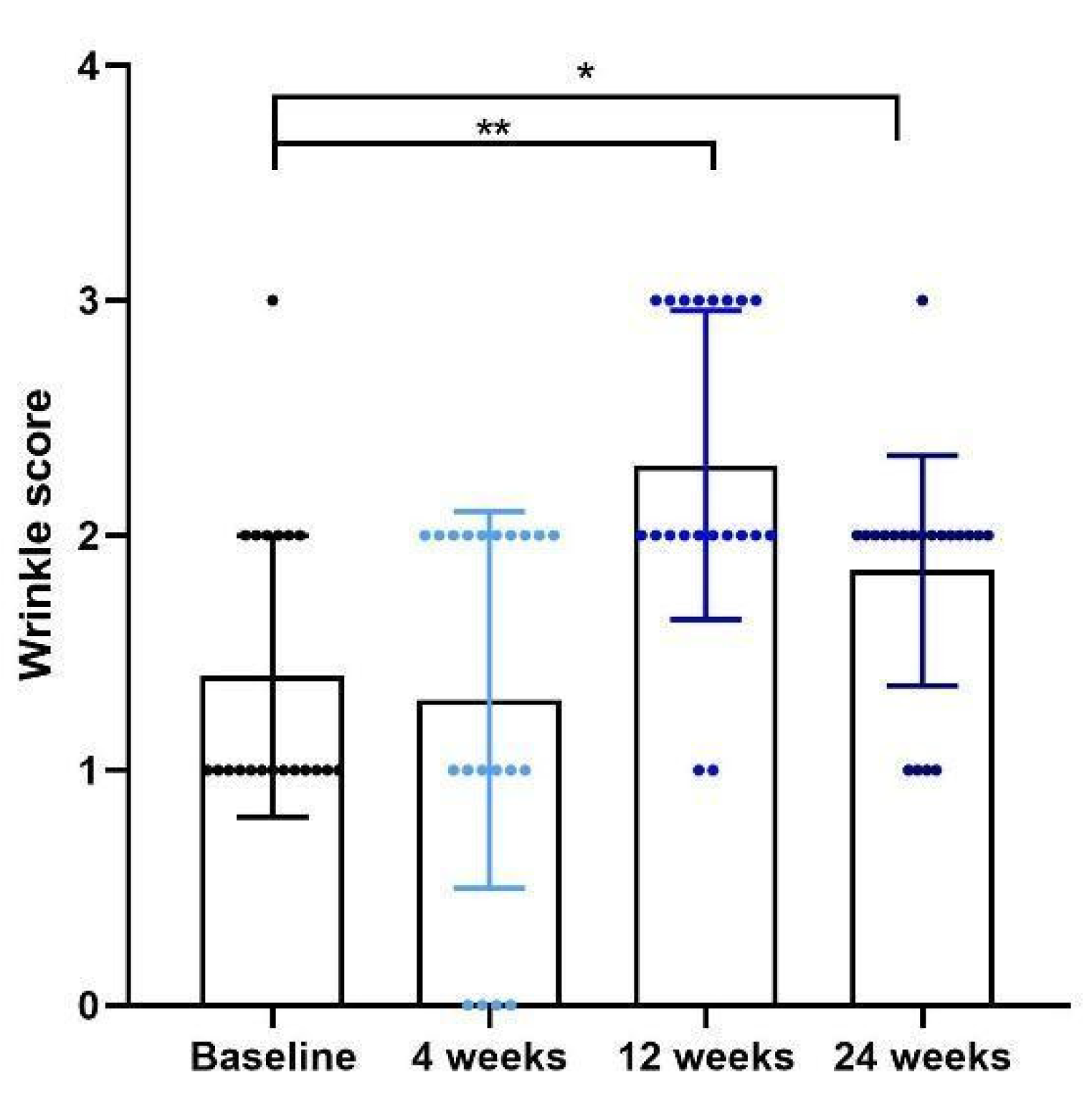
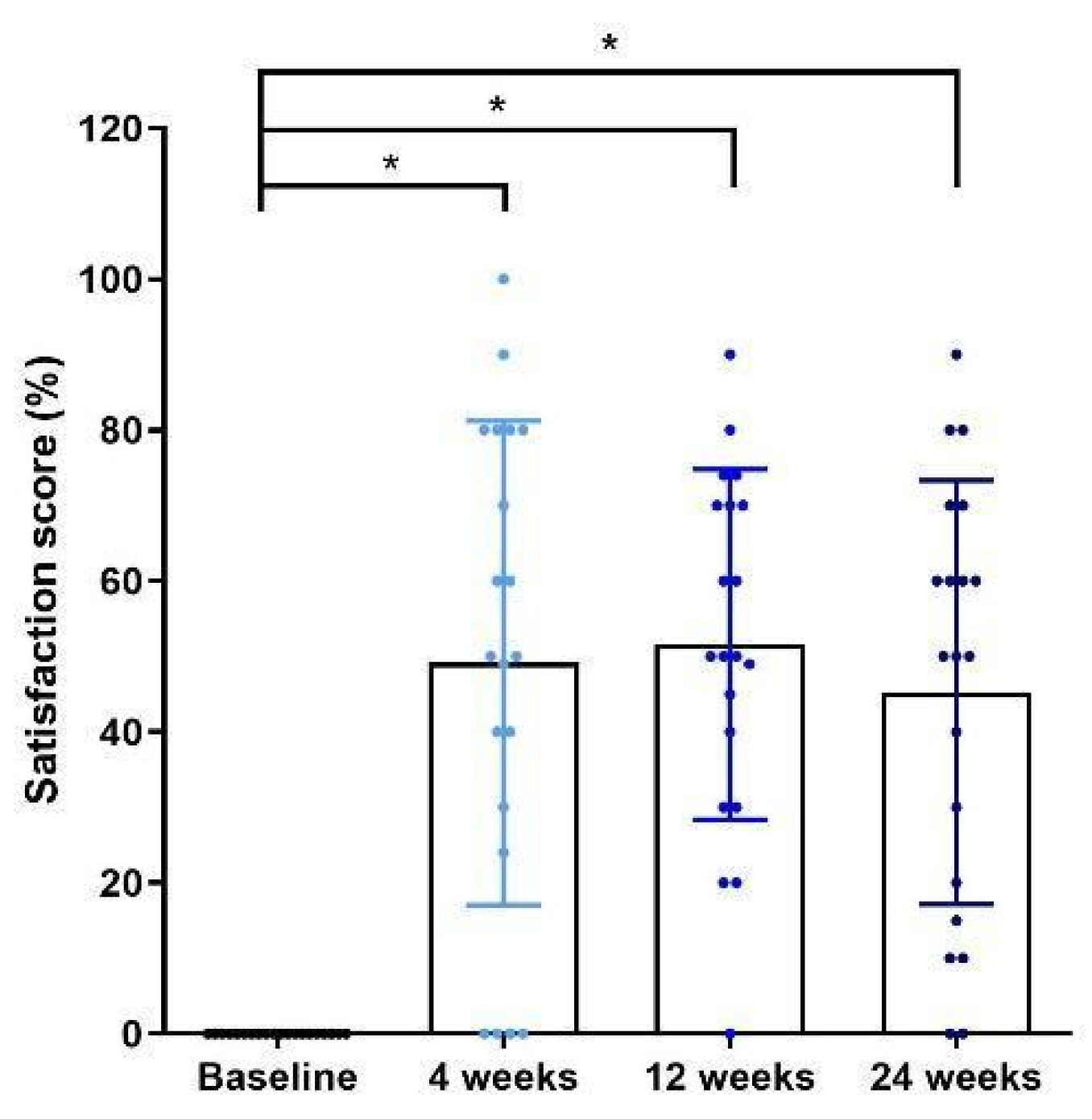
2.3. Clinical Outcome Evaluation
2.4. Facial Firmness Measurement
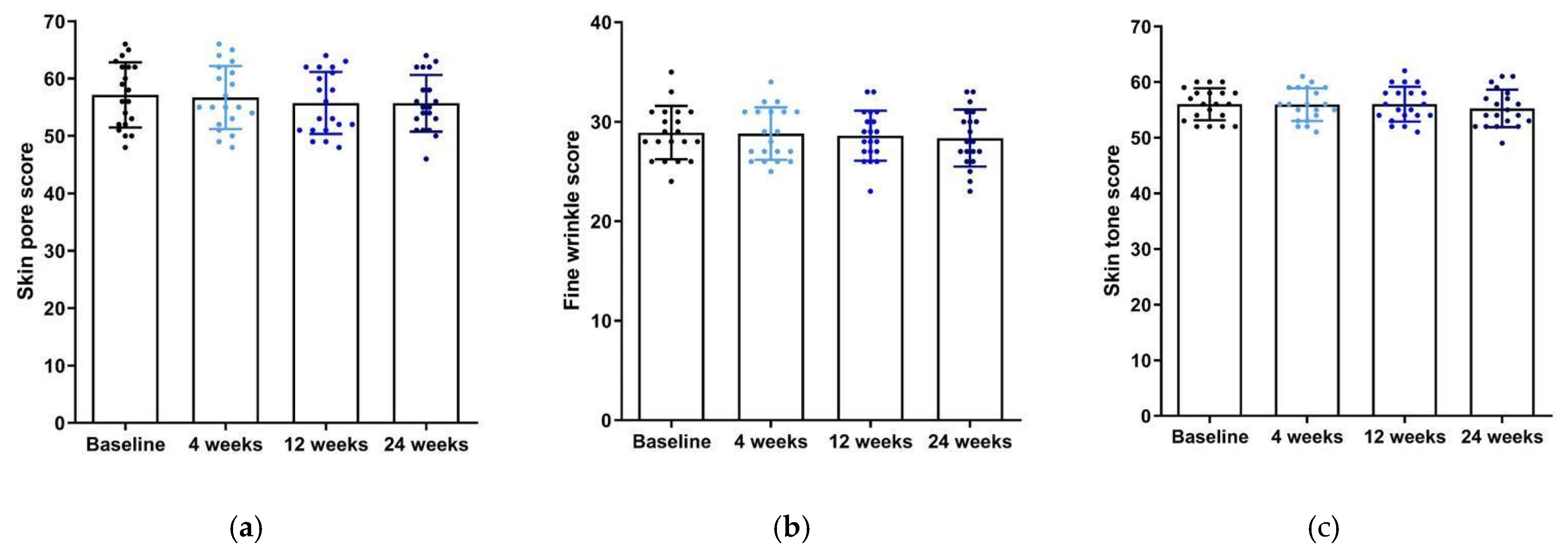
2.5. Skin Tone, Pores, and Fine Wrinkle Measurement
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beasley, K.L.; Weiss, R.A. Radiofrequency in cosmetic dermatology. Dermatol. Clin. 2014, 32, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Alster, T.S.; Lupton, J.R. Nonablative cutaneous remodeling using radiofrequency devices. Clin. Dermatol. 2007, 25, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Elsaie, M.L. Cutaneous remodeling and photorejuvenation using radiofrequency devices. Indian J. Dermatol. 2009, 54, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.G.; Jo, C.E.; Chapas, A.; Khetarpal, S.; Dover, J.S. Radiofrequency Microneedling: A Comprehensive and Critical Review. Dermatol. Surg. 2021, 47, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Arnoczky, S.P.; Aksan, A. Thermal modification of connective tissues: Basic science considerations and clinical implications. Instr. Course Lect. 2001, 50, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Dierickx, C.C. The role of deep heating for noninvasive skin rejuvenation. Lasers Surg. Med. 2006, 38, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Angra, K.; Alhaddad, M.; Boen, M.; Lipp, M.B.; Kollipara, R.; Hoss, E.; Goldman, M.P. Prospective Clinical Trial of the Latest Generation of Noninvasive Monopolar Radiofrequency for the Treatment of Facial and Upper Neck Skin Laxity. Dermatol. Surg. 2021, 47, 762–766. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jeong, E.T.; Lim, J.; Park, S.G. Development of the facial glycation imaging system for in situ human face skin glycation index measurement. J. Cosmet. Dermatol. 2021, 20, 2963–2968. [Google Scholar] [CrossRef] [PubMed]
- Park, H.U.; Cho, H.; Lee, S.J.; Cho, H.K. Use of 1,064-nm Q-switched Neodymium:Yttrium-aluminumgarnet Laser Therapy Assisted with Diamond Particle Suspension and Gold Microparticle Application for Acne Vulgaris and Enlarged Facial Pores. Med. Lasers 2021, 10, 242–245. [Google Scholar] [CrossRef]
- Carruthers, A.; Carruthers, J. A validated facial grading scale: The future of facial ageing measurement tools? J. Cosmet. Laser Ther. 2010, 12, 235–241. [Google Scholar] [CrossRef]
- Carruthers, J.; Flynn, T.C.; Geister, T.L.; Gortelmeyer, R.; Hardas, B.; Himmrich, S.; Jones, D.; Kerscher, M.; Maio, M.; Mohrmann, C.; et al. Validated assessment scales for the mid face. Dermatol. Surg. 2012, 38, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Narins, R.S.; Carruthers, J.; Flynn, T.C.; Geister, T.L.; Gortelmeyer, R.; Hardas, B.; Himmrich, S.; Jones, D.; Kerscher, M.; Maio, M.; et al. Validated assessment scales for the lower face. Dermatol. Surg. 2012, 38, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Chauny, J.M.; Paquet, J.; Lavigne, G.; Marquis, M.; Daoust, R. Evaluating acute pain intensity relief: Challenges when using an 11-point numerical rating scale. Pain 2016, 157, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Uehata, Y.; Yoshida, M.; Yabunaka, K.; Minematsu, T.; Tamai, N.; Sugama, J.; Sanada, H. Relationship of skin hardness of the temporal region to nutritional status. J. Nurs. Sci. Eng. 2017, 4, 49–57. [Google Scholar]
- Ivanova, Z.; Aleksiev, T.; Dobrev, H.; Atanasov, N. Use of a novel indentometer to evaluate skin stiffness in healthy and diseased human skin. Skin Res. Technol. 2023, 29, e13384. [Google Scholar] [CrossRef] [PubMed]
- Wanitphakdeedecha, R.; Yogya, Y.; Yan, C.; Phumariyapong, P.; Nanchaipruek, Y.; Thongjaroensirikul, P.; Maneeprasopchoke, P.; Techapichetvanich, T.; Eimpunth, S.; Manuskiatti, W. Efficacy and Safety of Monopolar Radiofrequency for Treatment of Lower Facial Laxity in Asians. Dermatol. Ther. 2022, 12, 2563–2573. [Google Scholar] [CrossRef] [PubMed]
- Rabe, J.H.; Mamelak, A.J.; McElgunn, P.J.S.; Morison, W.L.; Sauder, D.N. Photoaging: Mechanisms and repair. J. Am. Acad. Dermatol. 2006, 55, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Gold, M.H. Updates on radiofrequency devices for skin tightening and body contouring. Dermatol. Rev. 2020, 1, 75–83. [Google Scholar] [CrossRef]
- Schoellhammer, C.M.; Blankschtein, D.; Langer, R. Skin permeabilization for transdermal drug delivery: Recent advances and future prospects. Exp. Opin. Drug Deliv. 2014, 11, 393–407. [Google Scholar] [CrossRef]
- Alster, T.S.; Tanzi, E. Improvement of neck and cheek laxity with a nonablative radiofrequency device: A lifting experience. Dermatol. Surg. 2004, 30, 503–507. [Google Scholar] [CrossRef]
- Bogle, M.A.; Ubelhoer, N.; Weiss, R.A.; Mayoral, F.; Kaminer, M.S. Evaluation of the multiple pass, low fluence algorithm for radiofrequency tightening of the lower face. Lasers Surg. Med. 2007, 39, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Abraham, M.T.; Mashkevich, G. Monopolar radiofrequency skin tightening. Fac. Plast. Surg. Clin. N. Am. 2007, 15, 169–177. [Google Scholar] [CrossRef]
- Zelickson, B.D.; Kist, D.; Bernstein, E.; Brown, D.B.; Ksenzenko, S.; Burns, J.; Kilmer, S.; Mehregan, D.; Pope, K. Histological and ultrastructural evaluation of the effects of a radiofrequency-based nonablative dermal remodeling device: A pilot study. Arch. Dermatol. 2004, 140, 204–209. [Google Scholar] [CrossRef]
- Fritz, M.; Counters, J.T.; Zelickson, B.D. Radiofrequency treatment for middle and lower face laxity. Arch. Fac. Plast. Surg. 2004, 6, 370–373. [Google Scholar] [CrossRef]
- Suh, D.H.; Lee, S.J.; Ryou, J.H.; Son, H.C.; Kim, H.J.; Kim, H.S. Monopolar radiofrequency treatment in Asian skin: Do multiple RF treatments over time have beneficial effects? An observational report with long-term follow-up in eight patients. Dermatol. Surg. 2013, 39, 670–672. [Google Scholar] [CrossRef] [PubMed]
- Techapichetvanich, T.; Manuskiatti, W.; Wongdama, S.; Viriyaskultorn, N.; Li, J.B.; Jantanapornchai, N. Nonablative monopolar radiofrequency for the reduction of facial pores and sebum excretion in Thai patients: A novel approach. Lasers Surg. Med. 2023, 55, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Ross, E.V.; Tidwell, W.J.; Guss, L.; Sutton, A.V. Study of a 532/1064 fractional picosecond laser for facial rejuvenation. Dermatol. Surg. 2022, 48, 109–113. [Google Scholar] [CrossRef]
- Almukhtar, R.M.; Wood, E.S.; Fabi, S.G. Efficacy and safety of intense pulsed light and nonablative fractional 1440-nm diode laser to a combination of the 2 modalities for facial rejuvenation. Dermatol. Surg. 2023, 49, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Ziai, K.; Wright, H.V. Carbon dioxide laser rejuvenation of the facial skin. Clin. Plast. Surg. 2023, 50, 421–436. [Google Scholar] [CrossRef]
- Tolone, M.; Bennardo, L.; Zappia, E.; Scali, E.; Nisticò, S.P. New insight into nonablative 675-nm laser technology: Current applications and future perspectives. Dermatol. Clin. 2024, 42, 45–50. [Google Scholar] [CrossRef]
- Kushikata, N.; Negishi, K.; Tezuka, Y.; Takeuchi, K.; Wakamatsu, S. Is topical anesthesia useful in noninvasive skin tightening using radiofrequency? Dermatol. Surg. 2005, 31, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, M.; Hameed, S.; Mysore, V. Nonablative lasers and nonlaser systems in dermatology: Current status. Indian J. Dermatol. Venereol. Leprol. 2011, 77, 380–388. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age, mean ± SD | 47.95 ± 6.02 |
| Sex, no. (%) | |
| Female | 20 (100) |
| Race/ethnicity | |
| Asian, no. (%) | 20 (100) |
| Merz skin laxity scale, no. (%) | |
| Mild (1) | 13 (65) |
| Moderate (2) | 7 (35) |
| Severe (3) | 0 (0) |
| Very severe (4) | 0 (0) |
| Energy delivered by monopolar RF, no. (%) | |
| Total energy 37.80 kJ | 16 (80) |
| Total energy 31.80 kJ | 4 (20) |
| Baseline Mean ± SD | 4 Weeks Mean ± SD | 12 Weeks Mean ± SD | 24 Weeks Mean ± SD | p-Value | |
|---|---|---|---|---|---|
| Skin pore score | 57.15 ± 5.67 | 56.70 ± 5.52 | 55.75 ± 5.41 | 55.70 ± 4.95 | p = 0.80 |
| Fine wrinkle score | 28.90 ± 2.67 | 28.80 ± 2.63 | 28.60 ± 2.52 | 28.35 ± 2.87 | p = 0.96 |
| Skin tone score | 56.00 ± 2.87 | 55.95 ± 2.93 | 56.00 ± 3.11 | 55.25 ± 3.35 | p = 0.86 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, J.; Sung, Y.; Jin, S.; Hwang, C.-L.; Kim, H.; Hong, D.; Jung, K.E.; Seo, Y.-J.; Lee, Y. Efficacy and Safety of Monopolar Radiofrequency for Tightening the Skin of Aged Faces. Cosmetics 2024, 11, 71. https://doi.org/10.3390/cosmetics11030071
Shin J, Sung Y, Jin S, Hwang C-L, Kim H, Hong D, Jung KE, Seo Y-J, Lee Y. Efficacy and Safety of Monopolar Radiofrequency for Tightening the Skin of Aged Faces. Cosmetics. 2024; 11(3):71. https://doi.org/10.3390/cosmetics11030071
Chicago/Turabian StyleShin, JungMin, Yeounkuk Sung, Soyoung Jin, Cho-Long Hwang, Hyunjung Kim, Dongkyun Hong, Kyung Eun Jung, Young-Joon Seo, and Young Lee. 2024. "Efficacy and Safety of Monopolar Radiofrequency for Tightening the Skin of Aged Faces" Cosmetics 11, no. 3: 71. https://doi.org/10.3390/cosmetics11030071
APA StyleShin, J., Sung, Y., Jin, S., Hwang, C.-L., Kim, H., Hong, D., Jung, K. E., Seo, Y.-J., & Lee, Y. (2024). Efficacy and Safety of Monopolar Radiofrequency for Tightening the Skin of Aged Faces. Cosmetics, 11(3), 71. https://doi.org/10.3390/cosmetics11030071