Abstract
The aim of this study was to develop a topically applied formulation with the potential to alleviate arthritis ailments. A combination of two active ingredients, icariin from Epimedium L. (Species: Epimedium Koreanum) extract as a potential promoter of chondrogenesis and glucosamine sulfate as a precursor of cartilage tissues, was tested. In permeation studies, the potential for skin permeation of both substances was confirmed; however, the in vitro release test did not accurately reflect the degree of skin permeation. The in vitro release of icariin was at a level of 15.0–19.0% for the plant-extract-derived icariin and 29.0–35.0% for the pure substance. The level of glucosamine sulfate release was 38.4% (on average). For icariin of both origins, the release results were higher than those obtained via oral administration (about 12.0%), which shows the potential superiority of topical application. In addition, the physicochemical parameters that affect the in vitro release and performance of topical formulations were addressed. This preliminary research and permeation analysis of the formulation produced a promising picture of its prospects regarding arthritis treatment, although further investigation is needed.
1. Introduction
Musculoskeletal disorders are the second most common cause of disability in the elderly worldwide [1]. Among them, the most common is osteoarthritis (OA), which affects approximately 527.81 million people worldwide [2]. One of the effects of this disease is the progressive, permanent loss of cartilage within the joint, whose function is the protection of joint surfaces against frictional, compressive, shear, and tensile loads during movement. The cartilage tissue is composed of chondrocytes suspended in the intercellular matrix consisting of water, hyaluronic acid, minerals, proteoglycan, and collagen fibers, mainly of type II [3]. Due to the lack of blood vessels and nerves, damaged cartilage has only limited self-healing ability [4,5]. The excessive mechanical overloading of cartilage tissue stimulates chondrocytes to produce cytokines and tumor necrosis factor α (TNF-α), which activate the synthesis of metalloproteinases, tissue plasminogen activator, plasmins, and other proteases involved in tissue destruction [6]. As a consequence, a shift in the balance between the production of enzymes and their inhibitors, which regulate the process of cartilage formation, in favor of the destructive effect is observed, which precludes effective regeneration. Attempts to regenerate articular cartilage without removing mechanical loads lead to the formation of tissue with a changed biochemical composition. The decrease in the content of proteoglycans and change in their composition, leading to a shortening of the glycosaminoglycan chains and a weaker ability to bind hyaluronic acid, together with a lack of the ability to aggregate, have the greatest impact on the deterioration of the biomechanical properties of the tissue. The collagen content usually remains the same, but the fibers are much thinner and, therefore, form looser nets. With time, the volume of the cartilage decreases, and significant defects appear within it; additionally, the bones under the cartilage can also be damaged, which may lead to their remodeling, sclerotization, and the formation of osteophytes [7]. The whole process is accompanied by inflammation of the synovial membrane, which is associated with lympho- and monocytic infiltrates and the phagocytosis of mechanically damaged fragments of articular cartilage. Then, there is general inflammation of all surrounding structures, i.e., the joint capsule, ligaments, tendons, and muscles belonging to the affected joint. The clinical symptoms include, first and foremost, pain associated especially with the commencement of movement, but also limited mobility of the joint, stiffness after immobility, swelling and thickening, and visible changes in the joint’s outline [8]. Pain may be caused by damage to various tissues and may be related to the irritation of the nerve endings of the periosteum, damage to the subchondral layer of the bone, prolonged muscle tension, or improper tensioning of other structures to stabilize the joint and may also result from the presence of inflammation [9]. Many years of epidemiological studies conducted on various populations from around the world have allowed for the determination of differences in the incidence and factors increasing the risk of the disease, such as age, gender, or the environment. It has been repeatedly shown that the incidence of osteoarthritis increases with age, and more often affects women than men, while other factors increasing the risk of developing this disease include obesity, smoking, and injuries [2].
This disease leads to the progressive, permanent loss of cartilage within the joint. Due to the lack of blood vessels and nerves, damaged cartilage has only limited self-healing ability [5]. The excessive mechanical overloading of cartilage tissue stimulates chondrocytes to produce cytokines and tumor necrosis factor α (TNF-α), which activate the synthesis of substances involved in tissue destruction [6]. The result is a shift in the balance between the production of enzymes and their inhibitors, which regulate the process of cartilage formation, in favor of a destructive effect; thus, effective regeneration is precluded. The clinical symptoms include, first and foremost, pain associated especially with the commencement of movement, but also limited mobility of the joint, stiffness after immobility, swelling and thickening, and visible changes in the joint’s outline. Pain may be caused by damage to various tissues and may be related to the irritation of the nerve endings of the periosteum, damage to the subchondral layer of the bone, prolonged muscle tension, or improper tensioning of other structures to stabilize the joint and may also result from the presence of inflammation. To this day, no effective treatment for causal OA has been developed. The most commonly used therapy includes pain reduction, the inhibition of the disease’s progression, and joint function improvement, which are achieved through a combination of pharmacological and non-pharmacological methods and surgical treatment. For this purpose, generally available painkillers are used, and in the case of more severe pain and inflammation, drugs from the group of non-steroidal anti-inflammatory drugs (NSAIDs) are recommended [10]. However, their long-term use is not recommended due to the possibility of a number of side effects [11]. In pharmacological treatment, especially because of low toxicity, an alternative group of substances is used, namely, that of the symptomatic, slow-acting drugs for osteoarthritis (SYSADOA) [12,13,14]. This group includes both natural and synthetic substances that can be administered orally, intraarticularly, or topically. It has been shown that Epimedium L. (Species: Epimedium Koreanum) extract has an excellent beneficial impact on bone regeneration and can be involved in the regulation of multiple signaling pathways and biochemical processes [15]. Epimedium L. is one of the most commonly used herbs to treat bone fractures and osteoporosis in traditional Chinese medicine, wherein its assumed that Epimedium L. has the ability to “strengthen and regenerate bones” [16]. The Epimedium L. herb contains over 60 types of flavonoids, mainly glycosidic flavonoids, phenylpropanoids, alkaloids, polysaccharides, lignins, and sesquiterpenes [17,18,19,20], of which epimedin A, B, and C; icarizide_II; and icariin are considered the most important biologically active ingredients and constitute about 52% of the total content of flavonoids in the plant [21,22]. Pharmacological studies have shown that Epimedium L. has a number of anti-inflammatory, antioxidant, and tumor-inhibitory properties [23,24], and clinical studies have suggested a beneficial effect on the treatment of diabetes, depression, cardiovascular diseases, rheumatoid arthritis, osteoporosis, and osteoathritis [25,26,27,28]. Regarding the treatment of diseases of the musculoskeletal system, icariin has been shown to have the greatest impact on bone regeneration from among other constituents of Epimedium L. and can be involved in the regulation of multiple signaling pathways and biochemical processes [29]. In a mouse model of osteoarthritis, icariin reduced the destruction of cartilage, promoted chondrocyte differentiation, upregulated the expression of parathyroid hormone-related protein, and down-regulated the expression of Indian hedgehog [30]. Icariin belongs to the glycosyl flavonoids with phytoestrogen activity, and it is the 8-prenyl derivative of kaempferol 3,7-O-diglucoside with the molecular formula of C33H40O15. It is also safe, nontoxic, and its price is moderate, which makes it more attractive [31].
Another potentially very helpful substance in OA treatment is glucosamine, which is a naturally occurring aminomonosacharide and acts as a precursor in the biochemical synthesis of glycosylated proteins or lipids. Of particular importance to this study, it is a constituent of glycosaminoglycans in cartilage and synovial fluids [32]. Glucosamine is an endogenous substance, i.e., a typical constituent of the polysaccharide chains of the cartilage matrix and of glycosaminoglycans in the synovial fluid. In vitro and in vivo studies have shown that glucosamine stimulates the synthesis of physiological glycosaminoglycans and proteoglycans via chondrocytes and hyaluronic acid via synoviocytes [33]. Glucosamine’s mechanism of action in humans is still not fully known, which makes it impossible to estimate the time required for the body to respond to the administered preparation. Glucosamine is a relatively small molecule (with a molecular weight of 179.00, while that of glucosamine sulfate potassium chloride is 605.50); it is easily soluble in water and in hydrophilic organic solvents. Only limited information is available on the pharmacokinetics of glucosamine. The commonly sold form of glucosamine that offers significant therapeutic effects is glucosamine sulfate [34,35,36,37]; in particular, crystalline glucosamine sulfate is considered highly bioavailable with a proven pharmacological effect [38,39,40]. The purpose of this study was to design and develop a topical formulation for the treatment of osteoarthritis. This formulation contains a combination of two active ingredients: icariin from Epimedium L. (Species: Epimedium Koreanum) extract, which may be a potential promoter of chondrogenesis, and glucosamine sulfate as a precursor of cartilage tissue; together, these two ingredients may exhibit multidirectional effects and offer excellent potential with respect to the treatment of osteoarthritis. To test the validity of further studies, including application and clinical trials, permeation tests were conducted as the first step. An in vitro release test was conducted to mirror the permeation study of the active ingredients to confirm their potential for topical application while avoiding the side effects accompanying long-term oral intake [41].
2. Materials and Methods
2.1. Reagents
D-glucosamine sulfate*2KCl (100%) was provided by Biomus Company (Białystok, Poland), Icariin (98.0%) was purchased from Chengdu Biopurity Phytochemicals Ltd. (Sichuan, China), and Epimedium L. extract (based on the dried aerial parts of Epimedium Koreanum plant) was obtained from The Garden of Naturalsolution Co., Ltd. (Osan-si, Republic of Korea). Basal substances used were as follows: sodium polyacrylate (BASF Care Creations, Germany), vitis vinifera L. seed oil, shea butter, xanthan gum, and PEG-40 hydrogenated castor oil (Brenntag Poland Sp. z.o.o., Poland); glyceryl stearate, stearyl alcohol, and Ceteareth-25 were purchased from Evonik—Personal Care (Poland). The following permeation promoters were used: propylene glycol (Chemitec, Sosnowiec, Poland); essential oils of rosemary, marjoram, clove, and cinnamon from Avicenna Oil (Wrocław, Poland); and d-menthol and d-camphor, which were provided by PPH Standard sp. z.o.o. (Lublin, Poland). Phosphate-buffered saline was purchased from Thermo Fisher Scientific (Waltham, MA, USA), methanol clean for analysis was obtained from StanLab (Lublin, Poland), and glacial acetic acid (99.5% clean) for analysis was provided by Chempur (Piekary Śląskie, Poland).
2.2. Preparation of a Formulation Containing Icariin and Glucosamine
The compositions of the formulations are shown in Table 1.

Table 1.
The compositions of the formulations proposed.
2.2.1. Preparation of Cream
Solid ingredients of the oil phase were melted at a temperature of 75 °C, and the liquid portion of the oil phase was added after melting of the solid portion. Glucosamine sulfate was dissolved in water phase with stirring (IKA RW 20 digital). The aqueous phase containing bioactive components was gradually added to the oil phase, with homogenization (IKA ULTRA TURRAX T25) at 9500–10,000 rpm for 2 min and continuous stirring at 320 rpm for 40 min until the temperature decreased to 40 °C.
2.2.2. Preparation of Gel
Sodium polyacrylate gel was prepared by a cold process. D-glucosamine sulfate potassium chloride salt was dissolved in water phase with stirring (IKA RW 20 digital) at 320 rpm for 10 min. Sodium polyacrylate was added to the water phase and mixed with continuous stirring at 450 rpm for 30 min. Sodium was added until homogenous. The oil phase was gradually added to the water phase upon continuous agitation.
2.2.3. Preparation of Ointment
The constituents of the ointment base were placed together and allowed to melt at 70 °C in water bath. After melting, the ingredients were stirred while gently maintaining temperature of 70 °C for 10 min, and then cooled with continuous stirring at 350 rpm. The active ingredients were added after lowering the temperature of the base to 40 °C and continuing to mix at 500 rpm for 20 min until a homogeneous mass was obtained.
2.2.4. Acceptance Criteria and Specifications
According to specific cosmetic guidelines, each topical preparation must satisfy certain important criteria, such as obtaining/maintaining a specific color, certain pH range, density, viscosity, and homogeneity, and producing no skin irritation effects.
2.3. Physicochemical Tests
2.3.1. Appearance and Homogeneity
The cream and gel bases prepared were inspected visually for clarity, homogeneity, color, and presence of any particles/aggregates.
2.3.2. Determination of pH of Formulations
Metrohm 827pH Lab pH meter (Metrohm Polska, Opacz-Kolonia, Poland) was used for determination of the pH of each formulation in triplicate. The pH meter was calibrated with standard buffer solutions before each use.
2.3.3. Density
Steel pycnometer (Quantachrome, Boynton Beach, FL, USA) with a capacity of 100 mL was used to determine density of the formulations. The pycnometer was filled with the product and measurements were repeated three times. Densities of the formulations were calculated using the following equation (Equation (1)):
where Ρs—formulation density (kg/m3); ms—substance mass (kg); vp—pycnometer volume (m3) 0.99985—atmospheric pressure factor; and 0.0012—coefficient accounting for air density.
Ρs = 0.99985 × ms/vp + 0.0012
Equation (1) Equation for calculating formulation density.
2.3.4. Dynamic Viscosity
Brookfield LVT rotational viscometer was used to determine dynamic viscosity of the prepared formulations. Viscosity was measured at room temperature (approximately 23 °C) with a spindle no. 3 for creams and no. 4 for gels, and spindle rotation speed of 12 rpm for gels and 1.5 rpm for emulsions.
2.3.5. Assay of Icariin Content in Epimedium L. (Species: Epimedium Koreanum) Extract—LC-MS
The icariin concentration in the commercially available extract of Epimedium L. (Species: Epimedium Koreanum) was determined using a Kinetex column 2.6 µm C18 (2.1-id x100 mm). Analysis conditions were as follows: column temperature of 35 °C, injection volume of 3 µL, and mobile phase flow of 0.3 mL/min. The mobile phases were A: water + 0.1 wt.% formic acid, and B: acetonitrile + 0.1 wt.% formic acid. Elution was performed using a stepwise gradient elution shown in Table 2.
Table 2.
Gradient mobile phase elution for icariin determination in Epimedium L. (Species: Epimedium Koreanum) extract via LC-MS.
2.3.6. Release of Icariin
In vitro release test for icariin from Epimedium L. extract (Species: Epimedium Koreanum) was conducted with 708-DS Dissolution Apparatus Agilent Technologies Inc. (Santa Clara, CA, USA), synthetic membrane, Acceptor Solution phosphate buffer pH 5.8, and UV–VIS spectrophotometer λ = 270 nm.
2.3.7. Release of Glucosamine
In vitro release test for glucosamine was conducted with Franz Vertical Diffusion Cell Test System (Copley Scientific TM, Notinghma, United Kingdom). Synthetic membrane was soaked for 30 min prior to the in vitro assay in phosphate-buffered saline (PBS) of pH 7.4. The amount of formulation in each Franz cell and the time it was assembled were recorded. Conditions used were as follows: 32 °C, agitation of 50 rpm, acceptor solution—phosphate buffer of pH 7.4, and the amount of formulation—0.1 g. Samples were taken from the sampling port every hour for five hours. After each sample was collected, the phosphate buffer volume was restored to maintain conditions.
Concentrations of d-glucosamine sulfate in the samples were determined using HPLC-UV (Agilent Technologies) and C18 Column (3.5 μm, 4.6 mm id × 150 mm Waters) at temp. of 30 °C and wavelength of λ = 254 nm. The mobile phase consisted of methanol: water: glacial acetic acid (10:89, 96:0.04, pH 3.5); flow—1 mL/min; and injection volume of 20 µL. Accumulated amount of glucosamine sulfate was measured after derivatization of glucosamine to phenylthiocarbamyl glucosamine with phenyl isothiocyanate.
3. Results and Discussion
As a chronic degenerative and progressive disease, osteoarthritis affects the lives of people around the world, and to this day, no effective treatment has been developed. The main purpose of this study was to create dermocosmetic products with the potential to alleviate arthritis ailments. Glucosamine is an important precursor in the biochemical synthesis of glycosaminoglycans, which are major components of cartilage [32]. Moreover, icariin, due to its chondrogenic and osteoinductive potential, may be an effective promoter of bone regeneration [42,43,44]. In vitro studies have shown that icariin has the potential to promote bone engineering by initiating direct and stable chondrocyte differentiation, reducing its apoptosis, and creating an extracellular matrix by chondrocytes—without invoking a hypertrophy effect—due to the fact that it might be an effective accelerant of growth factors for cartilage [42,43]. A potent chondrogenic effect might be caused by the upregulation of the expression levels of aggrecan, collagen II, and SOX9 genes and the downregulation of the collagen I gene. Sun et al. have noted that the protection against cartilage and bone degradation is connected to the ability of icariin to inhibit the protease activity of cathepsin K [44]. Wiu et al. have established that icariin regulates articular bone loss, in part by regulating the receptor activator of the nuclear factor-B ligand RANKL (reduction) and osteoprotegrin OPG (enhancement) expression [45,46]. The data from clinical trials concerning the use of icariin in humans are limited. Only one blinded placebo control study has been reported. A randomized, double-blind study of Epimedium L. flavonoids that involved the administration of icariin (60 mg/day) to 100 postmenopausal women showed a significantly higher bone mineral density in the treatment group compared to the placebo group in 24 months [47]. It is important to remember that icariin has phytoestrogen activity, so it may disturb the endocrine system and connected pathways through oral administration, but this fact also indicates the superiority of topical application [48,49]. Unfortunately, there are just a few clinical studies that suggest that icariin might be helpful in OA treatment, and especially via topical administration, so this area needs to be further investigated. Both substances (icariin and glucosamine sulfate) are known to exhibit excellent therapeutic effects when used separately; due to their completely different mechanisms of action [33,50], they may also show a synergistic effect, which would be worth examining, especially due to the fact that glucosamine sulfate presents synergistic effects with a few NSAIDs and SYSADOA [40,51]. The determination of the icariin content in Epimedium L. (Species: Epimedium Koreanum) extract was essential in order to set the extract concentration in the target product formulation for further tests such that it is within the detection limits of the analytical devices used. The predicted concentration of icariin in the extract was very low based on the information from the manufacturer’s specification; the mixture that was provided contained only 5 wt.% of Epimedium L. (Species: Epimedium Koreanum) extract and a much smaller amount of icariin. The LC-MS method was selected to conduct content analysis due to its high specificity, as only selected ions produced from the analytes of interest are monitored. This analysis allowed for the determination of the quantitative composition of the formulation such that it fell within the limits of detection of the devices used. The calibration function for a standard was made by injecting five different concentrations of reference solution in triplicate. The regression coefficient was 0.999 for the calibration curve, which demonstrates good linearity over the linear range (Figure 1). The LC-MS analysis showed an average of 168.76 ng of icariin per 1 mL of Epimedium L. (Species: Epimedium Koreanum) extract, which would be under the detection limit while using the standard of 1–5 wt.% of the extract. This result enabled the content of the extract in the product mass, which was set at the level of 70%, to be within the detection limits of icariin for further analysis, and faclilitated the determination of the amount of icariin corresponding to the extract in the in vitro permeation study.
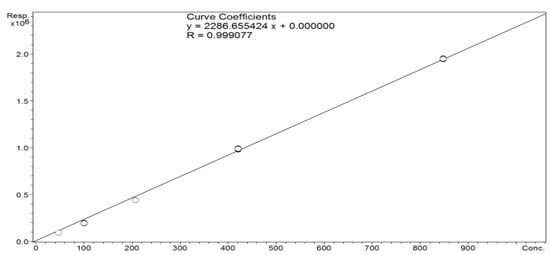
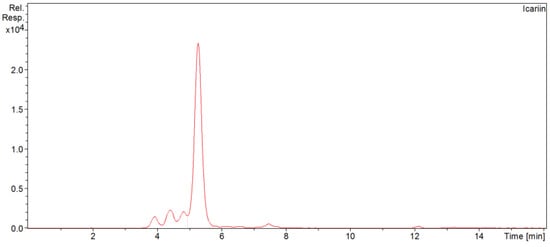
Figure 1.
Calibration curve and chromatogram of icariin in Epimedium L. (Species: Epimedium Koreanum) extract indicating its content of 168.90 ng/mL.
The formulations proposed (cream and gel) for arthritis management were successfully developed so that they met all the acceptance criteria and specifications. All formulations were visually assessed for phase homogeneity, agglomeration, and discoloration. They appeared smooth, homogeneous, free from agglomerates, and initially stable, with no mechanical impurities found in the product masses. This study confirmed that gels and emulsions are effective matrices with which to hold high concentrations of water-soluble molecules such as glucosamine sulfate and hydrophilic extracts and are able to deliver such molecules across the skin via topical application. The physicochemical parameters of the formulations are shown in Table 3. The rheological and sensorial properties, appearance, consistency, dynamic viscosity, density, and pH were reproducible and met the acceptance criteria.
Table 3.
Physicochemical properties of all formulations.
It has been established that some physicochemical parameters can have a significant impact on the degree of skin penetration by particular substances. Malzfeldt et al. [52] have proved that the viscosity of a medium has an influence on the release rate of the active ingredient and that the rate of release is higher in a solution than in a suspension, cream, or ointment. Therefore, the base components were selected such that the lowest possible viscosity of the medium was ensured while maintaining mass stability. The prepared formulations exhibited sufficient viscosity (33,600–38,200 mPa × s) and there was no appreciable change in viscosity over time. Another parameter that may influence the release rate is the pH of the formulations. As the proposed products are cosmetics, it was necessary to follow general guidelines for cosmetics and adjust the pH so that it would not affect the skin’s integrity and would not cause any adverse effects such as redness, rush, swelling, or changes in transepithelial water loss. The pH of the carrier may have a significant effect on the permeation of the substance, as it determines the solubility of active ingredients and the formulations’ stability during storage. After application, the pH may impact the partitioning of the active substances between the formulation and the skin. In this study, we did not ascertain the effect of pH changes on the ability to release active substances, so further studies are required in order to improve the release profile.
There is little information about the skin permeability of icariin in the literature. Iin et al. have shown that due to its low water solubility, membrane permeability, and low dissolution rate in biological fluids, icariin has low oral bioavailability of about 12% and poor absorption; thus, its clinical applications are limited [53]. The predicted skin bioavailability was poor, as icariin is a relatively large molecule with a molecular weight of 676.7 Da, poor water solubility, and membrane permeability.
In this study, we used absorption enhancers that, in the initial formulation containing the Epimedium L. (Species: Epimedium Koreanum) extract, enabled the acquirement of an icariin release value of 15–19%. The use of another formulation containing the same amount of icariin as in the extract, but in the form of a pure substance, enabled the acquirement of an icariin release value of 29–35% (Figure 2). The gel matrix was very effective at holding 70% of the hydrophilic extracts and was able to deliver them across the skin via topical application. The results of the study of the in vitro skin permeation of icariin suggest that the use of pure icariin is more effective than the extract, which indicates that, in the case of a formulation with a herbal extract that contains over 260 other substances, there may be a competitive release of other active ingredients or extract-derived icariin may bond with other ingredients, which would impede permeation [20]. This study also showed potentially higher bioavailability via skin application than oral administration, although this supposition requires proof from further studies as it is based on the accumulated amount of icariin but not the actual level of skin permeation. In view of the fact that Xu et al. have reported a value of released icariin as high as 70%, much higher results may be obtained by the proper modification of the carrier and the use of more appropriate permeation promoters for pure icariin, which is known to display poor solubility both in water and lipid solutions. One group of authors obtained an icariin-loaded nanogel via the reverse microemulsion method, yielding very promising release results [54]. In our study, the challenge was to devise a carrier that is suitable for both substances while accounting for their different natures and that ensures an optimum release profile. This analysis and preliminary characterization of the formulation performed so far have painted a very promising picture of osteoarthritis treatment; however, the skin-penetrating ability, application, and bioavailability enhancement, particularly with respect to icariin, may require further investigation to increase their therapeutic effects. Further studies are underway to improve permeation of the actives, examine the applicational prospects, and confirm the properties of the product.
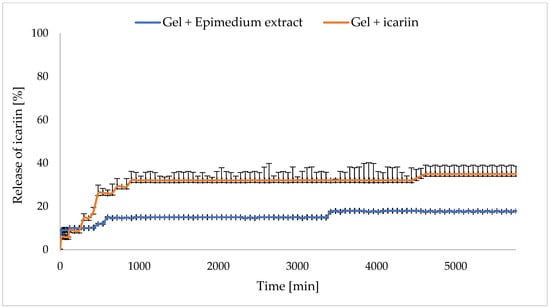
Figure 2.
Release of icariin from gel formulation.
Glucosamine is much better known and characterized in the literature than icariin, which facilitated the more precise selection of the analytical conditions. This substance stimulates proteoglycan synthesis via chondrocytes [55] and shows anti-inflammatory activities in different in vivo animal models [56,57]. Clinical studies have demonstrated its superior effect compared to a placebo in the short-term treatment of OA pain and movement limitation [36,58,59,60]; moreover, it has been shown that long-term (3-years) oral treatment with glucosamine sulfate retards the progression of Knee OA [36]. Not all researchers have been enthusiastic about glucosamine with respect to the treatment of OA, and there are some speculations about its low level of bioavailability [61]. Clinical studies conducted by Persiani et al. have shown increased concentrations of glucosamine after oral administration in both healthy subjects and OA sufferers [62,63]. The concentration was measured in plasma and synovial fluid, which indicates a positive influence on cartilage and relatively high bioavailability, but the levels were still lower than that required to positively affect the cartilage. A great deal of hope was elicited by subsequent studies in which it was shown that much higher concentrations of glucosamine can be absorbed upon topical application compared to the oral route [64], and that it can specifically enter synovial fluid [65]. Lower bioavailability of oral administration of glucosamine is connected to the hepatic first-pass effect [62], which is responsible for drug degradation. The drug’s absolute bioavailability is unknown. About 38% of an intravenous dose is excreted in an unchanged form in urine. The absolute bioavailability in humans after a single, oral dose was 25%. In the liver, more than 70% of the administered dose is metabolized. Absorption from the alimentary duct can be of about 90%; approximately 11% of the labeled dose was excreted in the feces [66]. Bypassing the gastrointestinal system is not the only benefit offered by topical administration. It has been widely established that transdermal application offers numerous advantages over oral delivery, especially in terms of targeted drug administration, where its use circumvents most of the undesirable side effects such as nausea, diarrhea, ulcers, and gastric inflammations, and is much safer in long-term treatment [67,68,69]. Due to its hydrophilic character, glucosamine sulfate is very water soluble, so it can be easily introduced into a medium, which allows for the prediction of its stability under selected conditions and the acquirement of results related to its accumulated amount that are close to the predictions for different carriers. In this study, the best results were obtained for the formulation containing 10 wt.% d-glucosamine sulfate (Table 4). It was also shown that the higher concentration of d-glucosamine sulfate in the formulation led to its higher accumulated amount. The formulations with d-glucosamine salt concentrations above 10 wt.% were not tested because of the difficulty of maintaining their stability. In this study, we used glucosamine sulfate, as it has been reported to exhibit much better effects compared to glucosamine hydrochloride [39]. The findings found in clinical trials with different glucosamine salts indicate the superiority of sulfates over hydrochlorides due to the increase in the sulfur concentration, which is essential for the synthesis of proteoglycans that are important for chondrocyte metabolism [70,71]. In addition, glucosamine sulphate has already shown a synergistic effect when combined with other osteoarthritis treatments [14,40].
Table 4.
In vitro cumulative glucosamine release results.
The in vitro active ingredient cumulative release from the formulations was on average 38.4% for the creams and 21.7% for the gels after 5 h. The formulations with all the concentrations had similar release profiles; initially, glucosamine was released from the gel formulations much faster, but ultimately, the glucosamine was released from the cream formulation in higher concentrations (Figure 3, Figure 4 and Figure 5).
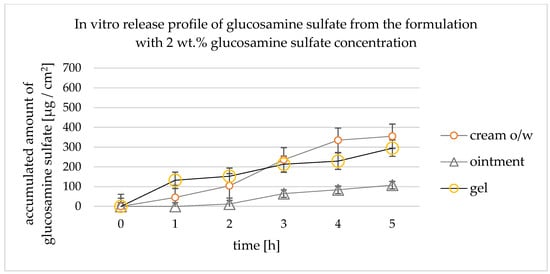
Figure 3.
Accumulated amount of glucosamine sulfate—in vitro release study for the formulation with 2 wt.% of glucosamine.
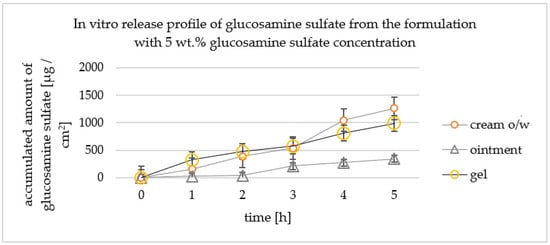
Figure 4.
Accumulated amount of glucosamine sulfate—in vitro release study for 5 wt.% formulation.
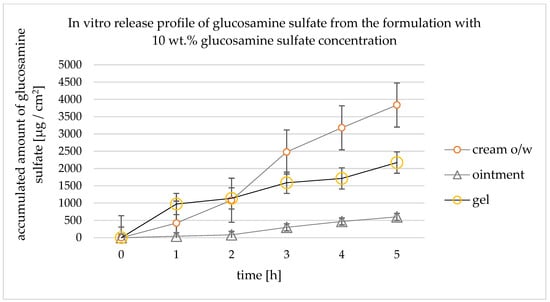
Figure 5.
Accumulated amount of glucosamine sulfate—in vitro release profiles of the formulation containing 10 wt.% of glucosamine.
The differences in the in vitro permeation of glucosamine through membranes are correlated with the type of carrier. As the emulsion consists of oil and water phases, it has a greater affinity to the skin than the formulation that consists of only a water phase and a gelling agent. The initial faster release afforded by the gel was probably due to the fact that the active ingredient does not need to partition the two phases and may immediately cross the membrane. The in vitro release study confirmed the potential in an in vitro skin permeation study of both active substances (glucosamine and icariin). Due to the relatively hydrophilic character of glucosamine, the expected in vitro skin permeation was very low especially in the gel formulation. As glucosamine does not contain a chromophore, to make its detection possible via the UV detector used, a derivatization was necessary, which confirmed the results of Kanwischer et al. [72]. A combination of permeation promoters from different groups of chemicals, such as camphor, menthol, propylene glycol, alcohol denat., and essential oils, in the formulations proposed permitted relatively high in vitro release of glucosamine sulfate from the prepared formulation, which was on average 38.4% for the creams after 5 h. A higher permeation result was predicted for the emulsion formulation as it was known that a combination of oil and water phases has greater affinity to the skin and is more compatible with the lipophilic nature of skin, which, eventually, yields a more desirable permeation profile, slower release at the beginning, and much a higher concentration of the active ingredient at the end. A better release profile constitutes a longer duration of action with higher concentrations of the active ingredient.
In permeation studies, the use of different polymeric membranes designed to mimic the human skin, such as polysulfone, polyethersulfone, cellulose, and polydimethylsiloxane, has been suggested by the FDA [73] because they are inert, do not occlude the penetration of the active substances, and provide good permeability [74,75]. Membrane selection is a significant factor in permeation studies as its type should match a given carrier. In this study, synthetic membranes were used to assuage ethical concerns and because of their easier accessibility. Considering the use of semi-liquid carriers in the form of emulsions and gels, it was most advantageous to choose hydrophilic membranes, such as polysulfone and cellulose, which demonstrated significantly better in vitro release results for emulsions and gels than for ointments. These observations confirm that the type and features of the membrane have an impact on the release rate and general accumulation of topical dosage forms. In the case of ointments, the use of a hydrophobic membrane and a carrier that is compatible with it would probably yield much better results. It has been suggested that polydimethylsiloxane membranes could be used to predict the skin permeability of lipophilic substances such as ointments with adequate results [64,76]. Despite their many advantages, such as the ease with which their size and composition can be adjusted; the ease of their use, acquisition, and storage; and the lack of variability, thus matching the intrinsic properties of the skin, unfortunately, the selected membranes (both polysulfone and cellulose) cannot provide an insight into the interaction of the formulation’s ingredients with the skin [77]. This is related to the impossibility of accounting for the lipid perturbation effect, cell metabolism, and the heterogeneous nature of the skin, which are difficult to recreate due to the synthetic nature of the membranes. A validated in vitro release test can provide screening information about the potential of a substance to cross the skin barrier, and the way the structural differences between the tested products may affect the rate and amount of the released substance, so long as the analyses are run under the same conditions. The use of artificial membranes instead of human or animal skin provides information on the release characteristics of a given substance instead of the permeation of the active substances, so further research is required to obtain information on the real degree of permeation. Other factors that can have an impact on the active ingredient’s release results are the type and characteristics of the prepared carriers. In the case of the formulation composition, the manufacturing process is crucial. The gel formulation was prepared using a cold process to avoid affecting the stabilities of the active ingredients, but the preparation of the emulsion required 75 °C to melt the solid components of the oil phase, which increased the risk of the decomposition of the active substances. Fortunately, the active substances used were stable at such a temperature and the production process did not affect their concentrations in the formulation. The higher total accumulated amount of the active substance released from the emulsion than from the gel formulation can be explained by the fact that the surfactants in the emulsion reduce surface tension and may also improve the wetting of the membrane surface and increase the contact area with the membrane, as confirmed by Ferreira et al. [78]. An initial faster release from the gel was expected, since, in the gel, the active ingredient does not need to partition the two phases and is immediately able to cross the membrane. It has been well known for many years that the skin is a significant barrier to the ingress of many compounds, and protection against any external factors is its most significant function. The penetration of active substances is hindered mostly by the large species diversity and the lipophilic nature of the lipid layer; therefore, to increase the therapeutic effectiveness of topical application, the use of permeation enhancers is needed. In this study, a combination of permeation enhancers that facilitate the absorption of active substances through the skin by temporarily diminishing the skin’s impermeability was used. Dimethyl sulfoxide (DMSO) is one of the most important compounds that enhances the transdermal permeation of a variety of drugs; unfortunately, it is forbidden in cosmetic applications, so the search for other enhancers was necessary. Terpenes, such as menthol and camphor and the terpene constituents of essential oils, increase the solubility of the active substances by forming a eutectic mixture with the penetrating compound and altering the barrier properties of the stratum corneum. The lowering of the melting point affects the solubility of many compounds and thus the degree of skin permeation. The use of ethanol offered several potential advantages. Alcohols act as penetration enhancers by leaching lipids from the stratum corneum, and they also release the sulfhydryl groups in keratin proteins of the stratum corneum, thus significantly increasing the possibility of the penetration of hydrophilic substances. They also acts as carriers for the terpenes used to increase the skin penetration and enhance the solubility of icariin [79]. It is important to note that in this study, two main active substances were used: glucosamine sulfate, which is highly hydrophilic, and the aqueous extract of Epimedium L. (Species: Epimedium Koreanum), which contains hydrophobic icariin. The physiochemical characteristics of the active ingredients’ molecules constitute another aspect that is crucial to defining the tendency of their release, and they might have impacted the data obtained in this study. In this research, we considered the use of icariin and glucosamine sulfate in a potential chondrogenic combination. It has been known for many years that the influence of ethanol on the ability to increase the permeation of hydrophilic compounds is usually connected to a simultaneous reduction in the penetration of hydrophobic ones, but icariin displays poor solubility both in water and lipid solutions. Thus, propylene glycol was added as an additional permeation promoter and co-solvent.
4. Conclusions
Demonstrating the possibility of a topical product’s therapeutic effects can be challenging. In this study, the potential of active ingredients to permeate the skin was shown. However, the obtained results of the release study do not reflect the actual degree of skin permeation but refer only to the accumulated amount of the active ingredient, as it was impossible to account for the interaction between the skin components and the lipid barrier that naturally occurs on the skin. We obtained the release of icariin at a level of 15.0–19.0% for the substance derived from the plant extract, and at a level of 29.0–35.0% for the pure substance. In both cases, the release was higher than for oral administration (by about 12.0%).
The average release level of glucosamine sulfate was 38.4%, which is sufficient. Both the cream and gel matrices effectively held 70.0% of the hydrophilic extracts, were stable at a 10.0% glucosamine sulfate concentration, and were able to deliver the substance across the synthetic membrane, thus mimicking topical application.
The lowest results were obtained for the ointment carrier, which is most likely due to the strongly hydrophilic nature of the active substances used. Other parameters that also have an impact on the in vitro release of active ingredients and the performance of a topical product were identified, namely, the initial concentration, process parameters, physicochemical properties such as viscosity and pH, the type of selected carrier, and permeation enhancers. This analysis and preliminary research on the formulations created has painted a very promising picture of osteoarthritis treatment, but further investigations are needed to increase their therapeutic effects and verify the actual degree of skin permeation. Due to global demographic changes and gradual lifestyle changes, the number of people suffering from OA is increasing, which, combined with the lack of effective treatments, is mobilizing a constant search for alternative therapies. The idea of using icariin, with its potentially strong ability to activate chondrogenesis and intercellular matrix regeneration by chondrocytes in a hitherto unexplored topical application, provides new insights into the potential use of this active substance and its properties with respect to the treatment of OA. In addition, the novel combination of the two substances (icariin and glucosamine sulfate), which show excellent effects separately due to their completely different mechanisms of action, may exhibit a synergistic effect, which would be worth confirming. Further studies are underway to confirm the properties of the product.
Author Contributions
Conceptualization, K.P. and A.F.-G.; methodology, K.P. and A.F.-G.; investigation, K.P. and A.F.-G.; data curation, K.P. and A.F.-G.; writing—original draft preparation, K.P.; writing—review and editing, A.F.-G. and I.N.; visualization, K.P.; supervision, A.F.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Liu, Q.; Yin, H.; Wang, K.; Diao, N.; Zhang, Y.; Lin, J.; Guo, A. Prevalence Trends of Site-Specific Osteoarthritis From 1990 to 2019: Findings From the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022, 74, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.A.J.; Bedi, A.; Rodeo, S.A. The Basic Science of Articular Cartilage: Structure, Composition, and Function. Sport. Health A Multidiscip. Approach 2009, 1, 461–468. [Google Scholar]
- Frenkel, S.R.; Clancy, R.M.; Ricci, J.L.; Di Cesare, P.E.; Rediske, J.J.; Abramson, S.B. Effects of nitric oxide on chondrocyte migration, adhesion, and cytoskeletal assembly. Arthritis Rheum. 1996, 39, 1905–1912. [Google Scholar] [CrossRef]
- Klein, T.J.; Rizzi, S.C.; Reichert, J.C.; Georgi, N.; Malda, J.; Schuurman, W. Strategies for zonal cartilage repair using hydrogels. Macromol. Biosci. 2009, 9, 1049–1058. [Google Scholar] [CrossRef]
- Grunke, M. Successful treatment of inflammatory knee osteoarthritis with tumour necrosis factor blockade. Ann. Rheum. Dis. 2006, 65, 555–556. [Google Scholar] [CrossRef]
- Deshpande, P.; Patil, K.; Guledgud, M.V.; D’souza, R.S. Diagnostic Imaging in TMJ Osteoarthritis: A Case Report and Overview. Int. J. Dent. Sci. Res. 2015, 3, 56–59. [Google Scholar]
- Kean, W.F.; Kean, R.; Buchanan, W.W. Osteoarthritis: Symptoms, signs and source of pain. InflammoPharmacology 2004, 12, 3–31. [Google Scholar] [CrossRef]
- Hunter, D.J.; McDougall, J.J.; Keefe, F.J. The Symptoms of Osteoarthritis and the Genesis of Pain. Rheum. Dis. Clin. North Am. 2008, 34, 623–643. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- Pelletier, J.P.; Martel-Pelletier, J.; Rannou, F.; Cooper, C. Efficacy and safety of oral NSAIDs and analgesics in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Semin. Arthritis Rheum. 2016, 45, S22–S27. [Google Scholar] [CrossRef] [PubMed]
- Permuy, M.; Guede, D.; López-Peña, M.; Muñoz, F.; Caeiro, J.R.; González-Cantalapiedra, A. Comparison of various SYSADOA for the osteoarthritis treatment: An experimental study in rabbits. BMC Musculoskelet Disord. 2015, 16, 120. [Google Scholar] [CrossRef]
- Veronese, N.; Ecarnot, F.; Cheleschi, S.; Fioravanti, A.; Maggi, S. Possible synergic action of non-steroidal anti-inflammatory drugs and glucosamine sulfate for the treatment of knee osteoarthritis: A scoping review. BMC Musculoskelet Disord. 2022, 23, 1084. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Cooper, C.; Bruyère, O.; Al-Daghri, N.M.; Branco, J.; Cavalier, E.; Reginster, J.Y. Multimodal Multidisciplinary Management of Patients with Moderate to Severe Pain in Knee Osteoarthritis: A Need to Meet Patient Expectations. Drugs. 2022, 82, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Wu, C.F.; Lai, W.P.; Yang, X.J.; Cheung, P.Y.; Yao, X.S.; Leung, P.C.; Wong, M.S. The osteoprotective effect of Herba epimedii (HEP) extract in vivo and in vitro. Evid Based Complement Altern. Med. 2005, 2, 353–361. [Google Scholar] [CrossRef]
- Pei, L.K.; Guo, B.L. A review on research of raw material and cut crude drug of Herba epimedii in last ten years. China J. Chin. Mater. Medica. 2007, 32, 466–471. [Google Scholar]
- Liu, R.; Li, A.; Sun, A.; Cui, J.; Kong, L. Preparative isolation and purification of three flavonoids from the Chinese medicinal plant Epimedium koreanum Nakai by high-speed counter-current chromatography. J. Chromatogr. A 2005, 1064, 53–57. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Yang, X.; Wang, K.; Ni, J.; Qu, X. Inhibitory effect of Epimedium extract on S-adenosyl-L-homocysteine hydrolase and biomethylation. Life Sci. 2005, 78, 180–186. [Google Scholar] [CrossRef]
- Wu, H.; Lien, E.J.; Lien, L.L. Chemical and pharmacological investigations of Epimedium species: A survey. Prog. Drug Res. 2003, 60, 1–57. [Google Scholar]
- Ma, H.P.; He, X.R.; Yang, Y.; Li, M.X.; Hao, D.J.; Jia, Z.P. The genus Epimedium: An ethnopharmacological and phytochemical review. J. Ethnopharmacol. 2011, 134, 519–541. [Google Scholar] [CrossRef]
- Guo, B.; Xiao, P. Determination of flavonoids in different parts of five Epimedium plants. China J. Chin. Mater. Med. 1996, 21, 523–525. [Google Scholar]
- Wang, Y.A.; Guo, Z.M.; Jin, Y.; Zhang, X.L.; Wang, L.; Xue, X.Y.; Liang, X.M. Identification of prenyl flavonoid glycosides and phenolic acids in Epimedium koreanum Nakai by Q-TOF-MS combined with selective enrichment on click oligo (ethylene glycol) column. J. Pharm. Biomed. Anal. 2010, 51, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.F.; Zhang, X.; Yang, X.H.; Qiu, N.X.; Wang, Y.; Wang, Z.Z. Microwave assisted extraction of flavonoids from cultivated Epimedium sagittatum: Extraction yield and mechanism, antioxidant activity and chemical composition. Ind. Crop. Prod. 2013, 50, 857–865. [Google Scholar] [CrossRef]
- Sze, S.C.; Tong, Y.; Ng, T.B.; Cheng, C.L.; Cheung, H.P. Herba Epimedii: A antioxidative properties and its medical implications. Molecules 2010, 15, 7861–7870. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Song, J.; Jia, X.B. Phytochemistry and ethnopharmacology of Epimedium L. species. Chin. Herb. Med. 2015, 7, 204–222. [Google Scholar] [CrossRef]
- Liu, Y.Q.; Han, X.F.; Liu, T.G.; Cheng, M.C.; Xiao, H.B. A cell-based model of bone remodeling for identifying activity of icarrin in the treatment of osteoporosis. Biotechnol. Lett. 2015, 37, 219–226. [Google Scholar] [CrossRef]
- Pan, Y.; Kong, L.D.; Xia, X.; Zhang, W.Y.; Xia, Z.H.; Jiang, F.X. Antidepressant-like effect of icariin and its possible mechanism in rats. Pharmacol. Biochem. Behav. 2005, 82, 686–694. [Google Scholar] [CrossRef]
- Wang, Z.Q.; Lou, Y.J. Proliferation-stimulating effects of icariin and desmethylicaritin in MCF-7 cells. Eur. J. Pharmacol. 2004, 504, 147–153. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, T.; Huang, Y.; Wismeijer, D.; Liu, Y. Icariin: Does It Have An Osteoinductive Potential for Bone Tissue Engineering? Phytother. Res. 2013, 28, 498–509. [Google Scholar] [CrossRef]
- Luo, Y.; Zhang, Y.; Huang, Y. Icariin Reduces Cartilage Degeneration in a Mouse Model of Osteoarthritis and is Associated with the Changes in Expression of Indian Hedgehog and Parathyroid Hormone-Related Protein. Med Sci Monit. 2018, 24, 6695–6706. [Google Scholar] [CrossRef]
- Zhao, J.; Ohba, S.; Komiyama, Y.; Shinkai, M.; Chung, U.; Nagamune, T. Icariin: A Potential Osteoinductive Compound for Bone Tissue Engineering. Tissue Eng. Part A 2010, 16, 233–243. [Google Scholar] [CrossRef]
- Hamerman, D. The biology of osteoarthritis. N. Engl. J. Med. 1989, 320, 1322–1330. [Google Scholar] [PubMed]
- Jerosch, J. Effects of Glucosamine and Chondroitin Sulfate on Cartilage Metabolism in OA: Outlook on Other Nutrient Partners Especially Omega-3 Fatty Acids. Int. J. Rheumatol. 2011, 2011, 969012. [Google Scholar] [CrossRef]
- Serni, U. Profile of glucosamine sulfate as an example of Slow Acting Drug in Osteoarthritis. Rev. Esp. Reumatol. 1993, 20 (Suppl. S1), 222. [Google Scholar]
- Avouac, B. Slow Acting Drugs in osteoarthritis: A step towards disease modification. Rev. Esp. Reumatol. 1993, 20 (Suppl. S1), 221–222. [Google Scholar]
- Pavelká, K.; Gatterová, J.; Olejarová, M.; Machacek, S.; Giacovelli, G.; Rovati, L.C. Glucosamine Sulfate Use and Delay of Progression of Knee Osteoarthritis. Arch. Inter. Med. 2002, 162, 2113–2123. [Google Scholar] [CrossRef] [PubMed]
- Mullerfasbender, H.; Bach, G.; Haase, W.; Rovati, L.; Sentikar, I. Glucosamine sulfate compared to ibuprofen in osteoarthritis of the knee. Osteoarthr. Cartil. 1994, 2, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.D. Glucosamine therapy for knee osteoarthritis: Pharmacokinetic considerations. Expert Rev. Clin. Pharmacol. 2009, 2, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Kucharz, E.J.; Kovalenko, V.; Szántó, S.; Bruyère, O.; Cooper, C.; Reginster, J.Y. A review of glucosamine for knee osteoarthritis: Why patented crystalline glucosamine sulfate should be differentiated from other glucosamines to maximize clinical outcomes. Curr. Med. Res. Opin. 2016, 32, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Cheleschi, S.; Tenti, S.; Giannotti, S.; Veronese, N.; Reginster, J.Y.; Fioravanti, A. A Combination of Celecoxib and Glucosamine Sulfate Has Anti-Inflammatory and Chondroprotective Effects: Results from an In Vitro Study on Human Osteoarthritic Chondrocytes. Int. J. Mol. Sci. 2021, 22, 8980. [Google Scholar] [CrossRef]
- Rapalli, V.K.; Mahmood, A.; Waghule, T.; Gorantla, S.; Kumar Dubey, S.; Alexander, A.; Singhvi, G. Revisiting techniques to evaluate drug permeation through skin. Expert Opin. Drug Deliv. 2021, 18, 1829–1842. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, X.; Li, K.F.; Li, D.X.; Xiao, Y.M.; Fan, Y.J.; Zhang, X.D. Icariin Promotes Extracellular Matrix Synthesis and Gene Expression of Chondrocytes In Vitro. Phytother. Res. 2012, 26, 1385–1392. [Google Scholar] [CrossRef]
- Wang, Z.C.; Sun, H.J.; Li, K.H.; Fu, C.; Liu, M.Z. Icariin promotes directed chondrogenic differentiation of bone marrow mesenchymal stem cells but not hypertrophy in vitro. Exp. Med. 2014, 8, 1528–1534. [Google Scholar] [CrossRef]
- Sun, P.; Liu, Y.; Deng, X.; Yu, C.; Dai, N.; Yuan, X. An inhibitor of cathepsin K, icariin suppresses cartilage and bone degradation in mice of collagen induced arthritis. Phytomedicine 2013, 20, 975–979. [Google Scholar] [CrossRef]
- Wei, C.C.; Ping, D.Q.; You, F.T.; Qiang, C.Y.; Tao, C. Icariin Prevents Cartilage and Bone Degradation in Experimental Models of Arthritis. Mediat. Inflamm. 2016, 2016, 1–10. [Google Scholar]
- Liu, Y.J.; Feng, W.; He, D.Y.; Wang, Q.Q. Effect of icariin on bone destruction and serum RANKL/OPG levels in type II collagen-induced arthritis rats. China J. Chin. Mater. Med. 2013, 33, 1221–1225. [Google Scholar]
- Zhang, G.; Qin, L.; Shi, Y. Epimedium-derived phytoestrogen flavonoids exert beneficial effect on preventing bone loss in late postmenopausal women: A 24-month randomized, double-blind and placebocontrolled trial. J. Bone Min. Res. 2007, 22, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.K.; Choi, Y.H.; Kwon, H.; Lee, S.B.; Kim, D.H.; Sung, C.K.; Park, Y.I.; Dong, M.S. Estrogenic/antiestrogenic activities of a Epimedium koreanum extract and its major components: In vitro and in vivo studies. Food Chem. Toxicol. 2012, 50, 2751–2759. [Google Scholar] [CrossRef]
- Zanoli, P.; Benelli, A.; Zavatti, M.; Rivasi, M.; Baraldi, C.; Baraldi, M. Improved sexual behavior in male rats treated with a Chinese herbal extract: Hormonal and neuronal implications. Asian J. Androl. 2008, 10, 937–945. [Google Scholar] [CrossRef]
- Yang, A.; Yu, C.; Lu, Q.; Li, H.; Li, Z.; He, C. Mechanism of Action of Icariin in Bone Marrow Mesenchymal Stem Cells. Stem Cells Int. 2019, 4, 5747298. [Google Scholar] [CrossRef]
- Calamia, V.; Mateos, J.; Fernández-Puente, P.; Lourido, L.; Rocha, B.; Fernández-Costa, C.; Montell, E.; Vergés, J.; Ruiz-Romero, C.; Blanco, F.J. A pharmacoproteomic study confirms the synergistic effect of chondroitin sulfate and glucosamine. Sci. Rep. 2014, 4, 5069. [Google Scholar] [CrossRef]
- Malzfeldt, E.; Lehmann, P.; Goerz, G.; Lippold, B.C. Influence of drug solubility in the vehicle on clinical efficacy of ointments. Arch. Dematol. Res. 1989, 281, 193–197. [Google Scholar] [CrossRef]
- Jin, J.; Wang, H.; Hua, X.; Chen, D.; Huang, C.; Chen, Z. An outline for the pharmacological effect of icariin in the nervous system. Eur. J. Pharmacol. 2019, 842, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Lu, Y.R.; Kou, N.; Hu, M.J.; Wang, Q.S.; Cui, Y.L. Intranasal delivery of icariin via a nanogel-thermoresponsive hydrogel compound system to improve its antidepressant-like activity. Int. J. Pharm. 2020, 586, 119550. [Google Scholar] [CrossRef]
- Bassleer, C.; Henrotin, Y.; Franchimont, P. In-vitro evaluation of drugs proposed as chondroprotective agents. Int. J. Tissue React. 1992, 14, 231–241. [Google Scholar]
- Setnikar, I.; Cereda, R.; Pacini, M.A.; Revel, L. Antireactive properties of glucosamine sulfate. Arzneimittelforschung 1991, 41, 157–161. [Google Scholar] [PubMed]
- Setnikar, I.; Pacini, M.A.; Revel, L. Antiarthritic effects of glucosamine sulfate studied on animal models. Arzneimittelforschung 1991, 41, 542–545. [Google Scholar]
- Noack, W.; Fischer, M.; FSrster, K.K.; Rovati, L.C.; Setnikar, I. Glucosamine sulfate in osteoarthritis of the knee. Osteoarthr. Cart 1994, 2, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Rovati, L.C.; Setnikar, I.; FSrster, K.K.; Reichelt, A.; Noack, W. Glucosamine sulfate in gonarthrosis: Efficacy in placebo controlled studies. Rev Esp Reum. 1993, 20 (Suppl. S1), 72. [Google Scholar]
- Giacovelli, G.; Rovati, L.C. Clinical efficacy of glucosamine sulfate in osteoarthritis of the spine. Rev. Esp. Reum. 1993, 20 (Suppl. S1), 96. [Google Scholar]
- Silva, J.A.; Apolinário, A.C.; Souza, M.S.R.; Damasceno, B.P.G.L.; Medeiros, A.C.D. Cutaneous Administration of Drugs: Challenges and Strategies for the Development of Trans-dermal Formulations. Rev. De Ciências Farm. Básica 2010, 31, 125–131. [Google Scholar]
- Persiani, S.; Rotini, R.; Trisolino, G.; Rovati, L.C.; Locatelli, M.; Paganini, D.; Antonioli, D.; Roda, A. Synovial and plasma glucosamine concentrations in osteoarthritic patients following oral crystalline glucosamine sulphate at therapeutic dose. Osteoarthr. Cartil. 2007, 15, 764–772. [Google Scholar] [CrossRef]
- Persiani, S.; Roda, E.; Rovati, L.C.; Locatelli, M.; Giacovelli, G.; Roda, A. Glucosamine oral bioavailability and plasma pharmacokinetics after increasing doses of crystalline glucosamine sulfate in man. Osteoarthr. Cartil. 2005, 13, 1041–1049. [Google Scholar] [CrossRef]
- Lee, C.W.; Li, Z.; Patel, K.; Olobo, J.O.; Lee, E.J.D.; Goh, L.B. The Transdermal Profiles of Mediflex™ Glucosamine Cream in Mouse and Man. Available online: https://docplayer.net/31056811-The-transdermal-profiles-of-mediflex-tm-glucosamine-cream-in-mouse-and-man.html (accessed on 10 February 2023).
- Kong, M.; Hashim, K.B.; Lin, P.; Coestesquis, G.; Xu, A.Y.; Lebes, F.; Ting, C.M. Penetration of Topical Glucosamine Sulfate into the Synovial Fluid of Patients with Knee Osteoarthritis: A Nonrandomized, OpenLabel, Single Dose, Bioavailability Study. J. Biosci. Med. 2019, 7, 76–90. [Google Scholar] [CrossRef]
- Huskisson, E.C. Glucosamine and Chondroitin for Osteoarthritis. J. Int. Med. Res. 2008, 36, 6. [Google Scholar] [CrossRef] [PubMed]
- Leite, C.B.S.; Coehlo, J.M.; Muehlmann, L.A.; de Azevedo, R.B.; Sousa, M.H. Skin Delivery of Glucosamine and Chondroitin Sulphates—A Perspective on the Conservative Treatment for Osteoarthritis of the Knee. J. Biosci. Med. 2017, 5, 11–20. [Google Scholar] [CrossRef]
- Miki, R.; Ichitsuka, Y.; Yamada, T.; Kimura, S.; Egawa, Y.; Seki, T.; Morimoto, Y. Development of a membrane impregnated with a poly(dimethylsiloxane)/poly(ethylene glycol) copolymer for a high-throughput screening of the permeability of drugs, cosmetics, and other chemicals across the human skin. Eur. J. Pharm. Sci. 2015, 66, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Flaten, G.E.; Palac, Z.; Engesland, A.; Filipović-Grčić, J.; Vanić, Ž.; Škalko-Basnet, N. In vitro skin models as a tool in optimization of drug formulation. Eur. J. Pharm. Sci. 2015, 75, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L.J.; Kaplan, L.N.; Hamadeh, M.J.; Grigoriu, A.C.; Baron, M. Sulfate could mediate the therapeutic effect of glucosamine sulfate. Metabolism. 2001, 50, 767–770. [Google Scholar] [CrossRef]
- Cordoba, F.; Nimni, M.E. Chondroitin sulfate and other sulfate containing chondroprotective agents may exhibit their effects by overcoming a deficiency of sulfur amino acids. Osteoarthr. Cartil. 2003, 11, 228–230. [Google Scholar] [CrossRef]
- Kanwischer, M.; Kim, S.Y.; Bian, S.; Kwon, K.A.; Kim, J.S.; Kim, D.D. Evaluation of the Physicochemical Stability and Skin Permeation of Glucosamine Sulfate. Drug Dev. Ind. Pharm. 2005, 31, 91–97. [Google Scholar] [CrossRef] [PubMed]
- FDA. Guidance for Industry. Nonsterile semisolid dosage forms, scale-up and postapproval changes: Chemistry, manufacturing, and controls; in vitro release testing and in vivo bioequivalence documentation. Cent. Drug Eval. Res. 1997, CMC 7, 19–25.
- EMA. Guideline on Quality of Transdermal Patches; European Medicines Agency: London, UK, 2014; Volume 24. [Google Scholar]
- Argoff, C.E.; Gloth, F.M. Topical Nonsteroidal Anti-Inflammatory Drugs for Management of Osteoarthritis in Long-Term Care Patients. Ther. Clin. Risk Manag. 2011, 7, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.F.; Rouse, J.J.; Sanderson, F.D.; Eccleston, G.M. The relevance of polymeric synthetic membranes in topical formulation assessment and drug diffusion study. Arch. Pharmacal Res. 2012, 35, 579–593. [Google Scholar] [CrossRef] [PubMed]
- Ameri, M.; Lewis, H.; Lehman, P. Effect of Skin Model on In Vitro Performance of an Adhesive Dermally Applied Microarray Coated with Zolmitriptan. J. Pharm. 2018, 3, 7459124–7459130. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.A.M.; Seiller, M.; Grossiord, J.L.; Marty, J.P.; Wepierre, J. Vehicle influence on in vitro release of metronidazole: Role of w/o/w multiple emulsion. Int. J. Pharm. 1994, 109, 251–259. [Google Scholar] [CrossRef]
- Lin, H.M.; Lin, L.F.; Sun, M.Y.; Liu, J.; Wu, Q. Topical Delivery of Four Neuroprotective Ingredients by Ethosome-Gel: Synergistic Combination for Treatment of Oxaliplatin-Induced Peripheral Neuropathy. Int. J. Nanomed. 2020, 15, 3251–3266. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).