
Radicular Intracanal Splitting Forces and Cutting Efficiency of NiTi Rotary Versus Reciprocating Systems: A Comparative In Vitro Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Registration
2.2. Power Calculation
2.3. Part 1: Sample Preparation for Lateral Splinting Force Testing
2.3.1. Sample Sectioning and Mounting for the Testing Platform
2.3.2. Creation of the Artificial Canal
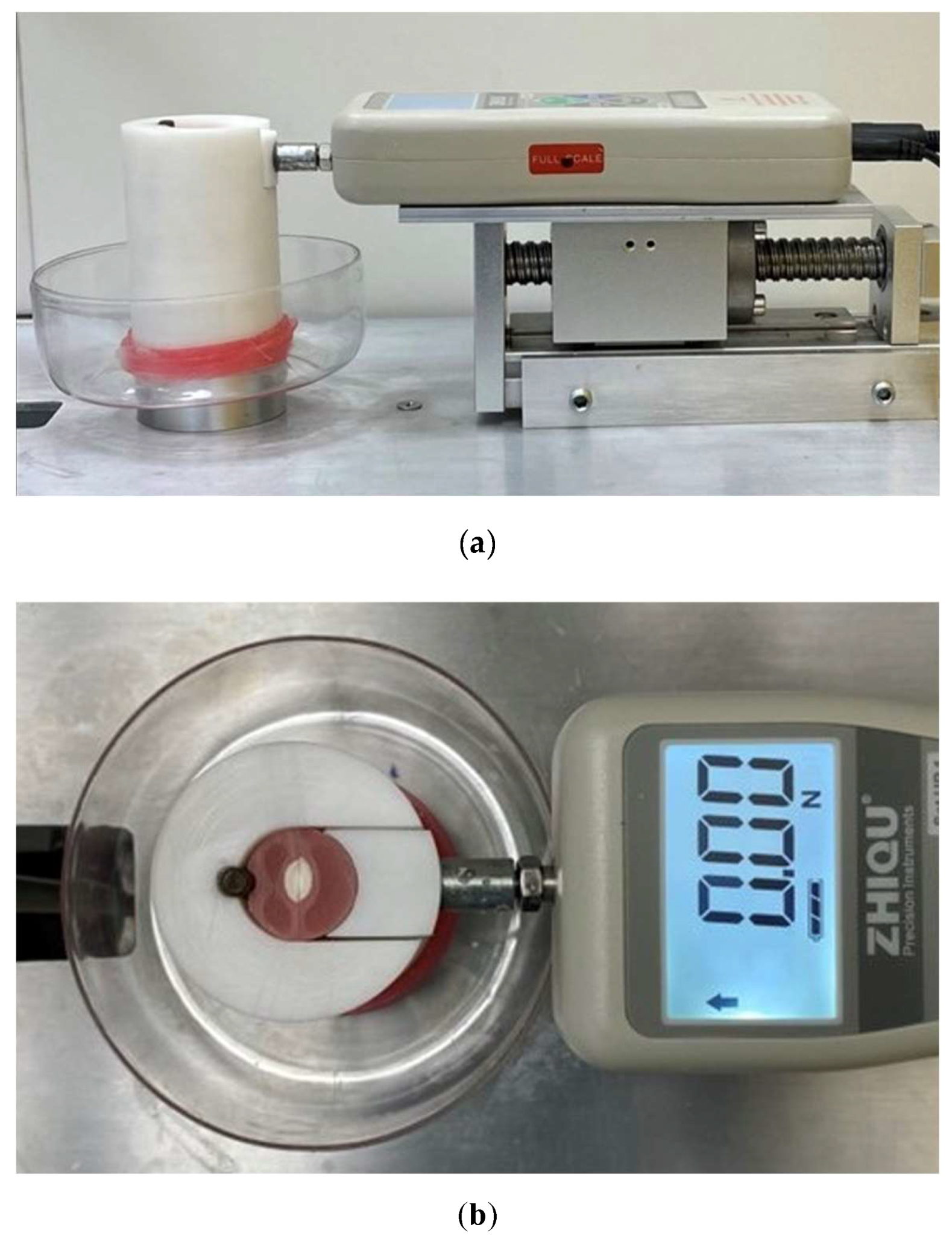
2.3.3. The Splitting Force Platform
2.4. Instrumentation
2.4.1. Instrumentation Protocol
2.4.2. Data Extraction
2.5. Part 2: Cutting Efficiency Testing Sample Preparation and Instrumentation
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- The maximum lateral splinting forces of the rotary system were significantly higher than those of the reciprocating system.
- The dentine cutting efficiency was significantly greater using the reciprocating system than using the rotating system.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| System of Instrumentation | Maximum Force Exerted by System (N) | Time Required for Instrumentation (sec) |
|---|---|---|
| Operator 1, ProTaper Gold | 21.89 ± 4.72 A | 242.91 ± 39.56 A |
| Operator 1, WaveOne Gold | 13.50 ± 3.04 A | 157.14 ± 17.30 A |
| Operator 2, ProTaper Gold | 24.11 ± 4.17 B | 143.86 ± 89.27 B |
| Operator 2, WaveOne Gold | 16.92 ± 3.15 B | 150.50 ± 20.33 B |

References
- Hulsmann, M.; Peters, O.A.; Dummer, P.M. Mechanical preparation of root canals: Shaping goals, techniques and means. Endod. Top. 2005, 10, 30–76. [Google Scholar] [CrossRef]
- Fidan, M.E.; Erdemir, A. Effect of different irrigation activation techniques on irrigation penetration into the simulated lateral canals. Odontology 2022, 111, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Tabassum, S.; Zafar, K.; Umer, F. Nickel-Titanium Rotary File Systems: What’s New? Eur. Endod. J. 2019, 4, 111–117. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Afrashtehfar, K.I.; Corbella, S.; El-Kabbaney, A.; Perondi, I.; Taschieri, S. In Vivo and In Vitro Effectiveness of Rotary Nickel-Titanium vs Manual Stainless Steel Instruments for Root Canal Therapy: Systematic Review and Meta-analysis. J. Évid. Based Dent. Pr. 2018, 18, 59–69. [Google Scholar] [CrossRef]
- Amorim, A.C.; Caldeira, A.V.; Sampaio, S.C.; Neto, N.L.; Oliveira, T.M.; Nogueira, D.A.; Moretti, A.B.D.S.; Sakai, V.T. Comparison between the rotary (Hyflex EDM®) and manual (k-file) technique for instrumentation of primary molars: A 12-month randomized clinical follow-up study. J. Appl. Oral Sci. 2022, 30, e20210527. [Google Scholar] [CrossRef]
- Palma, P.J.; Messias, A.; Cerqueira, A.R.; Tavares, L.D.; Caramelo, F.; Roseiro, L.; Santos, J.M. Cyclic fatigue resistance of three rotary file systems in a dynamic model after immersion in sodium hypochlorite. Odontology 2018, 107, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Hu, B.; Peng, H.; Tang, M.; Song, J. The incidence of dentinal cracks during root canal preparations with reciprocating single-file and rotary-file systems: A meta-analysis. Dent. Mater. J. 2017, 36, 243–252. [Google Scholar] [CrossRef]
- Boonchoo, K.; Leelataweewud, P.; Yanpiset, K.; Jirarattanasopha, V. Simplify pulpectomy in primary molars with a single-file reciprocating system: A randomized controlled clinical trial. Clin. Oral Investig. 2019, 24, 2683–2689. [Google Scholar] [CrossRef]
- Moule, A.J.; Kahler, B. Diagnosis and management of teeth with vertical root fractures. Aust. Dent. J. 1999, 44, 75–87. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Macdonald, D. Vertical Tooth Root Fracture Detection through Cone-beam Computed Tomography: An Umbrella Review Protocol Testing Four Hypotheses. Open Dent. J. 2019, 13, 449–453. [Google Scholar] [CrossRef]
- Holcomb, J.Q.; Pitts, D.L.; Nicholls, J.I. Further investigation of spreader loads required to cause vertical root fracture during lateral condensation. J. Endod. 1987, 13, 277–284. [Google Scholar] [CrossRef]
- Silva, L.R.; de Lima, K.L.; Santos, A.A.; Leles, C.R.; Estrela, C.; Silva, B.S.D.F.; Yamamoto-Silva, F.P. Dentin thickness as a risk factor for vertical root fracture in endodontically treated teeth: A case-control study. Clin. Oral Investig. 2020, 25, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.K.; Cheung, G.S.P. A comparison of stainless steel and nickel-titanium K-files in curved root canals. Int. Endod. J. 1996, 29, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Rivera, E.M.; Williamson, A. Diagnosis and treatment planning: Cracked tooth. J. Tenn. Dent. Assoc. 2003, 83, 38–41. [Google Scholar] [PubMed]
- Yoldas, O.; Yilmaz, S.; Atakan, G.; Kuden, C.; Kasan, Z. Dentinal Microcrack Formation during Root Canal Preparations by Different NiTi Rotary Instruments and the Self-Adjusting File. J. Endod. 2012, 38, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.S.S.; Ghani, N.R.N.A.; Noorani, T.Y. The existence of butterfly effect and its impact on the dentinal microhardness and crack formation after root canal instrumentation. Odontology 2021, 109, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Plotino, G.; Nagendrababu, V.; Bukiet, F.; Grande, N.M.; Veettil, S.K.; De-Deus, G.; Ahmed, H.M.A. Influence of Negotiation, Glide Path, and Preflaring Procedures on Root Canal Shaping—Terminology, Basic Concepts, and a Systematic Review. J. Endod. 2020, 46, 707–729. [Google Scholar] [CrossRef] [PubMed]
- Jamleh, A.; Komabayashi, T.; Ebihara, A.; Nassar, M.; Watanabe, S.; Yoshioka, T.; Miyara, K.; Suda, H. Root surface strain during canal shaping and its influence on apical microcrack development: A preliminary investigation. Int. Endod. J. 2014, 48, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Ustun, Y.; Aslan, T.; Sagsen, B.; Kesim, B. The effects of different nickel-titanium instruments on dentinal microcrack formations during root canal preparation. Eur. J. Dent. 2015, 09, 041–046. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.-Y.; Kim, H.-C.; Kim, E. Kinematic Effects of Nickel-Titanium Instruments with Reciprocating or Continuous Rotation Motion: A Systematic Review of In Vitro Studies. J. Endod. 2016, 42, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-H.; Lu, Y.; Song, D.; Zhou, X.; Zheng, Q.-H.; Gao, Y.; Huang, D.-M. Occurrence of Dentinal Microcracks in Severely Curved Root Canals with ProTaper Universal, WaveOne, and ProTaper Next File Systems. J. Endod. 2015, 41, 1875–1879. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-C.; Lee, M.-H.; Yum, J.; Versluis, A.; Lee, C.-J.; Kim, B.-M. Potential Relationship between Design of Nickel-Titanium Rotary Instruments and Vertical Root Fracture. J. Endod. 2010, 36, 1195–1199. [Google Scholar] [CrossRef]
- Wilcox, L.R.; Roskelley, C.; Sutton, T. The relationship of root canal enlargement to finger-spreader induced vertical root fracture. J. Endod. 1997, 23, 533–534. [Google Scholar] [CrossRef]
- Monga, P.; Bajaj, N.; Mahajan, P.; Garg, S. Comparison of incidence of dentinal defects after root canal preparation with continuous rotation and reciprocating instrumentation. Singap. Dent. J. 2015, 36, 29–33. [Google Scholar] [CrossRef] [PubMed]
- PradeepKumar, A.R.; Shemesh, H.; Archana, D.; Versiani, M.A.; Sousa-Neto, M.D.; Leoni, G.B.; Silva-Sousa, Y.T.; Kishen, A. Root Canal Preparation Does Not Induce Dentinal Microcracks In Vivo. J. Endod. 2019, 45, 1258–1264. [Google Scholar] [CrossRef] [PubMed]
- Hatton, J.F.; Ferrillo, P.J.; Wagner, G.; Stewart, G.P. The effect of condensation pressure on the apical seal. J. Endod. 1988, 14, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Deari, S.; Zehnder, M.; Al-Jadaa, A. Effect of dentine cutting efficiency on the lateral force created by torque-controlled rotary instruments. Int. Endod. J. 2020, 53, 1153–1161. [Google Scholar] [CrossRef]
- Karatas, E.; Gunduz, H.A.; Kirici, D.O.; Arslan, H. Incidence of dentinal cracks after root canal preparation with ProTaper Gold, Profile Vortex, F360, Reciproc and ProTaper Universal instruments. Int. Endod. J. 2015, 49, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Ashwinkumar, V.; Krithikadatta, J.; Surendran, S.; Velmurugan, N. Effect of reciprocating file motion on microcrack formation in root canals: An SEM study. Int. Endod. J. 2013, 47, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Al-Omari, M.; Aurich, T.; Wirtti, S. Shaping canals with ProFiles and K3 instruments: Does operator experience matter? Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. Endodontology 2010, 110, e50–e55. [Google Scholar] [CrossRef] [PubMed]
- Bailey, E.; Tickle, M.; Campbell, S. Patient safety in primary care dentistry: Where are we now? Br. Dent. J. 2014, 217, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Jamleh, A.; Alfouzan, K.; Awawdeh, L.; Alfadley, A.; Ibrahim, N.; Alhijji, S.; Masuadi, E. Successive spreader insertion forces induced by undergraduate students during canal obturation. Saudi Endod. J. 2017, 7, 110–114. [Google Scholar]
- Fonseca, R.; Haiter-Neto, F.; Carlo, H.; Soares, C.; Sinhoreti, M.; Puppin-Rontani, R.; Correr-Sobrinho, L. Radiodensity and hardness of enamel and dentin of human and bovine teeth, varying bovine teeth age. Arch. Oral Biol. 2008, 53, 1023–1029. [Google Scholar] [CrossRef] [PubMed]






| Tested Group Instruments | Mean (SD) | p-Value |
|---|---|---|
| PTG (F2) | 23.00 (4.43) | |
| <0.001 | ||
| WOG (Primary) | 15.21 (3.46) |
| Tested Group Instruments | Mean (SD) | p-Value |
|---|---|---|
| PTG (F2) | 0.89 (0.22) | |
| <0.001 | ||
| WOG (Primary) | 1.34 (0.26) |
| Maximum Force Exerted by File and Stroke, (N) | Total Instrumentation Time (s) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| System Instrumentation Sequence | |||||||||||
| Sequence | 1 | 2 | 3 | 4 | 5 | ||||||
| Instrument/Stroke | SX | Stroke 1 | S1 | Stroke 2 | S2 | Stroke 3 | F1 | Stroke 4 | F2 | Stroke 5 | |
| WOG | 3.38 ± 2.42 abcde | 7.17 ± 2.02 abe | 8.75 ±1.74 ace | 10.03 ± 3.88 ade | 15.16 ± 3.50 abcde | 150.50 ± 20.33 | |||||
| PTG | 3.94 ± 2.17 abcde | 23.00 ± 4.46 abcde | 13.14 ± 6.39 abc | 11.97 ± 4.84 abd | 11.16 ± 5.85 abe | 272.81 ± 73.24 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Jadaa, A.; Alsmadi, R.F.; Salem, W.M.; Abdulridha, A.A.; Afrashtehfar, K.I. Radicular Intracanal Splitting Forces and Cutting Efficiency of NiTi Rotary Versus Reciprocating Systems: A Comparative In Vitro Study. Cosmetics 2023, 10, 23. https://doi.org/10.3390/cosmetics10010023
Al-Jadaa A, Alsmadi RF, Salem WM, Abdulridha AA, Afrashtehfar KI. Radicular Intracanal Splitting Forces and Cutting Efficiency of NiTi Rotary Versus Reciprocating Systems: A Comparative In Vitro Study. Cosmetics. 2023; 10(1):23. https://doi.org/10.3390/cosmetics10010023
Chicago/Turabian StyleAl-Jadaa, Anas, Ranya F. Alsmadi, Wesal M. Salem, Aya A. Abdulridha, and Kelvin I. Afrashtehfar. 2023. "Radicular Intracanal Splitting Forces and Cutting Efficiency of NiTi Rotary Versus Reciprocating Systems: A Comparative In Vitro Study" Cosmetics 10, no. 1: 23. https://doi.org/10.3390/cosmetics10010023
APA StyleAl-Jadaa, A., Alsmadi, R. F., Salem, W. M., Abdulridha, A. A., & Afrashtehfar, K. I. (2023). Radicular Intracanal Splitting Forces and Cutting Efficiency of NiTi Rotary Versus Reciprocating Systems: A Comparative In Vitro Study. Cosmetics, 10(1), 23. https://doi.org/10.3390/cosmetics10010023