

The Emerging Role of Induced Pluripotent Stem Cells as Adoptive Cellular Immunotherapeutics

Abstract
:Simple Summary
Abstract
1. Introduction
2. Discovery, Generation and Characterisation of iPSCs
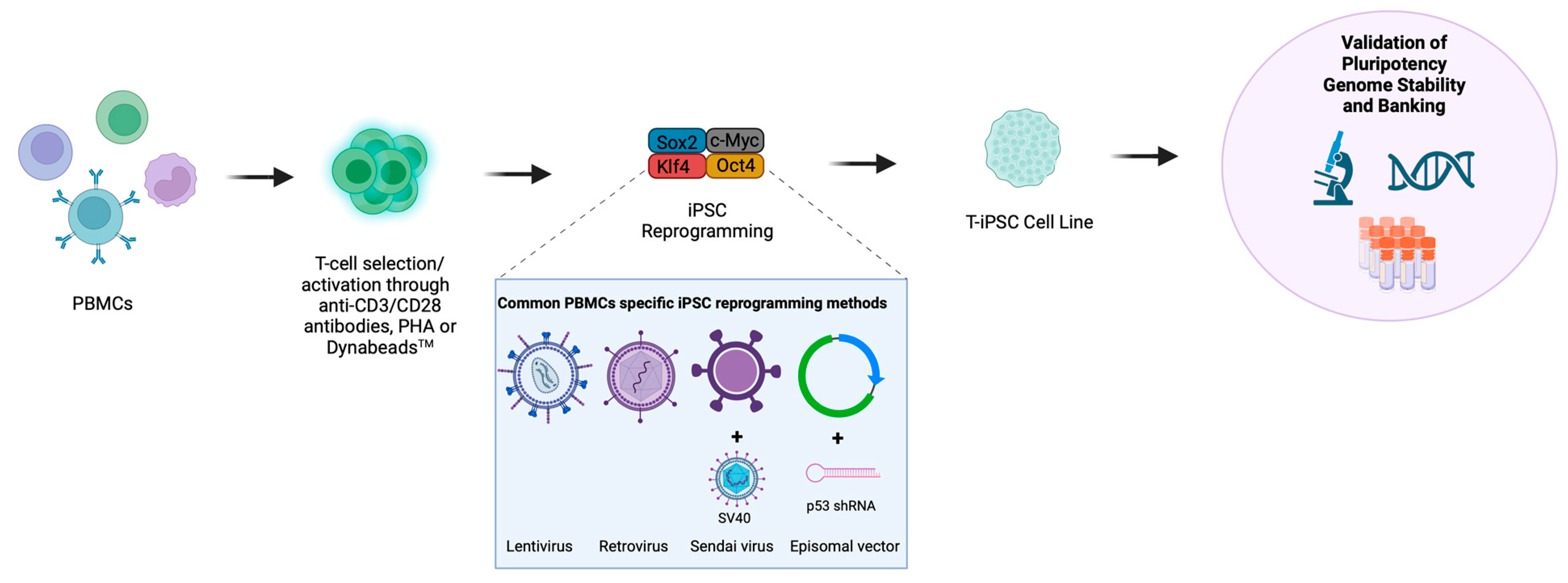
3. PBMC Reprogramming
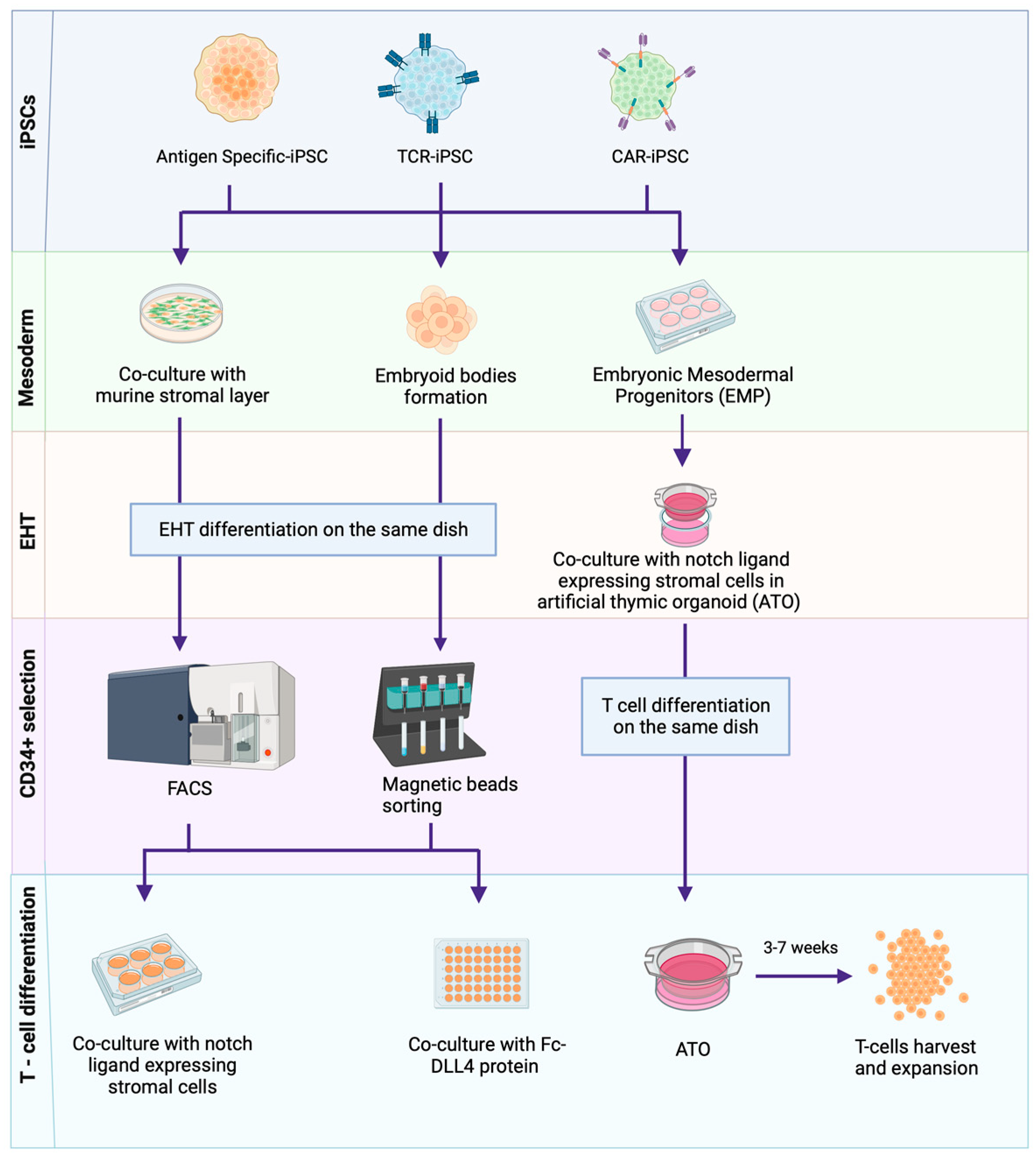
4. Methods of iPSC-to-T-Cell Differentiation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mesoderm/HSC Induction | |||
| Methods | Embryoid Bodies | Co-Culture with OP9/C3H10T1/2 | Artificial Thymic Organoids (ATOs) |
| Primary Culture Components | CHIR99021 10 µM | VEGF (15–50 ng/mL) | rhActivin A (10 ng/mL) |
| SB431542 6 µM | SCF (50 ng/mL) | rhBMP4 (10 ng/mL) | |
| BMP-4 (10–50 ng/mL) | FLT3L (10 ng/mL) | rhVEGF (10 ng/mL) | |
| bFGF (5–50 ng/mL) | rhFGF (10 ng/mL) | ||
| VEGF (15–50 ng/mL) | |||
| FLT3L (10 ng/mL) | |||
| SCF (50 ng/mL) | |||
| TPO(30 ng/mL) | |||
| References | [67,68,74] | [32,65,81] | [76] |
| T-cell differentiation | |||
| Methods | Fc-DLL4/Retronectin (stroma free) | Co-culture with OP9−DLL1/4 | Artificial thymic organoids (ATOs) |
| Primary Culture Components | rhFLT-3L (50 ng/mL) | rhFLT-3L (5–10 ng/mL) | rhFLT-3L (5 ng/mL) |
| rhIL-7 (50 ng/mL) | rhIL-7 (1–10 ng/mL) | rhIL-7, first 7 days (5 ng/mL) | |
| rhSCF (50 ng/mL) | rhSCF (5–10 ng/mL) | rhSCF, first 7 days, (10 ng/mL) | |
| rhTPO (100 ng/mL) | rhSCF, after 7 days (50 ng/mL) | ||
| rhSDF-1α (30 nM) | rhTPO, after 7 days, (5 ng/mL) | ||
| SB203580 (15 µM) | |||
| References | [68] | [32,65,66,67,79,81,82] | [76] |
| T-cell Maturation/Expansion | |||
| Methods | anti-CD3/CD28 mAbs | anti-CD3 | Phytohemagglutinin (PHA) |
| Primary Culture Components | hIL-7 (2–5 ng/mL) | hIL-7 (10 ng/mL) | hIL-7 (10 ng/mL) |
| hFlt-3L (0–5 ng/mL) | rhIL-2 (10 ng/mL) | IL-15 (5 ng/mL) | |
| hSCF (0–10 ng/mL) | dexamethasone 10 nM | PHA 2 μg/mL | |
| anti-human CD3 (50–5000 ng/mL) | Anti-human CD3 (OKT3) 500 ng/mL | ||
| anti-human CD28 (1000–2000 ng/mL) | |||
| hIL-2 (2 ng/mL/200 U/mL) | |||
| References | [74] | [68] | [64,82,83] |
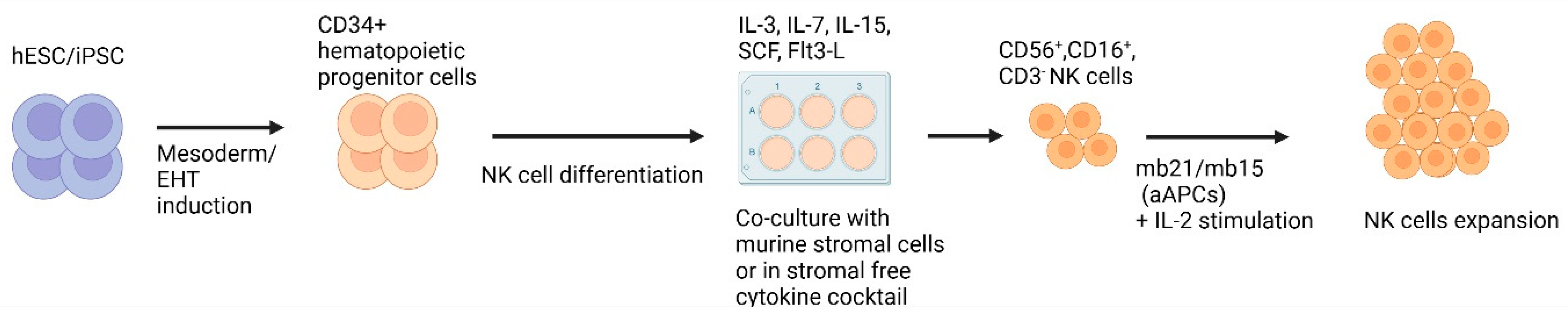
5. Methods of iPSC-to-NK Cell Differentiation
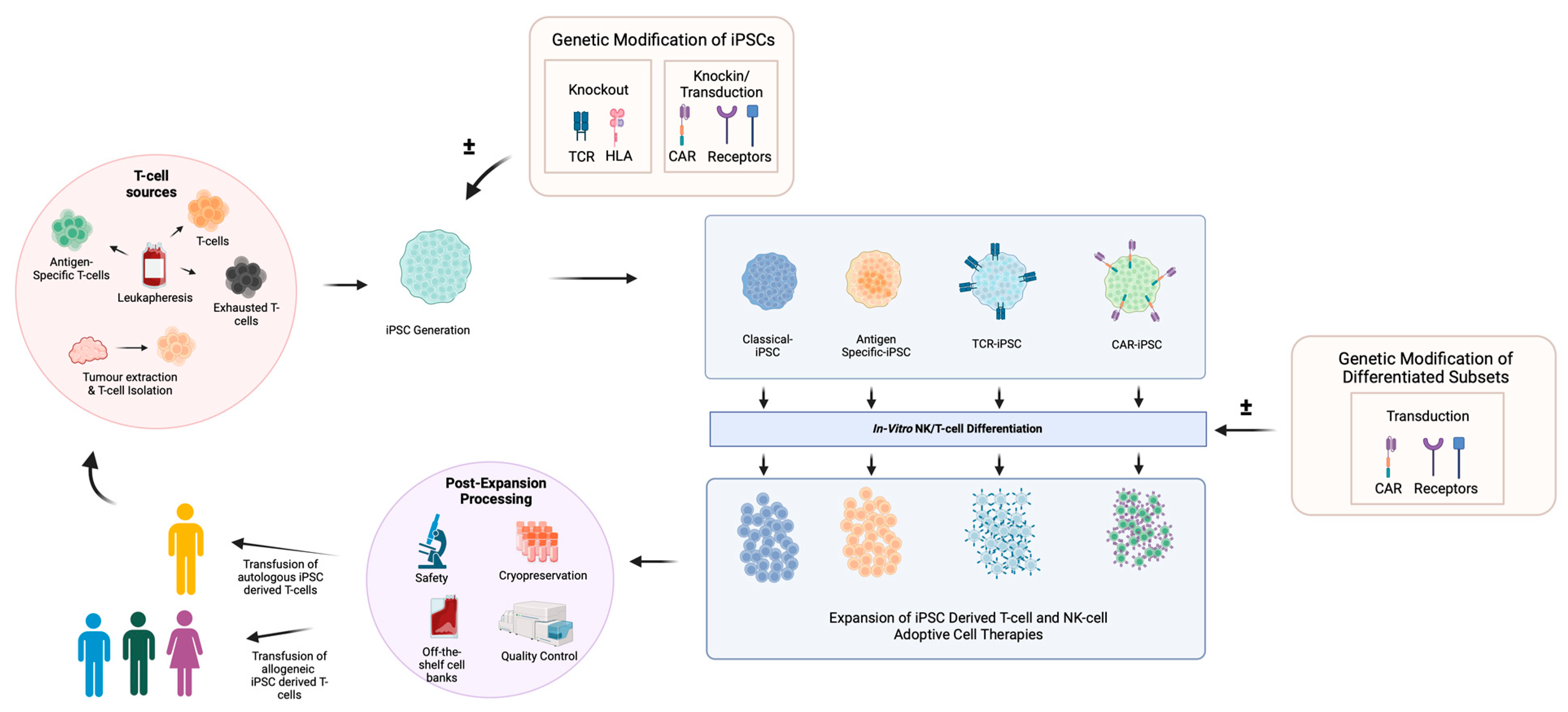
6. Use of iPSCs in Adoptive Cell Therapy
6.1. CAR T-Cell Therapy
6.2. CAR NK Cell Therapy
6.3. TIL Therapy
6.4. VST Therapy
7. Potential and Challenges of iPSC-Derived Adoptive Cell Therapies
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| aAPC | Artificial antigen-presenting cell |
| ACT | Adoptive cell therapy |
| ADCC | Antibody-dependent cellular cytotoxicity |
| Adv | Adenovirus |
| AICD | Activation-induced cell death |
| AP | Alkaline phosphatase |
| APC | Antigen-presenting cell |
| ATO | Artificial thymic organoids |
| BCMA | B-cell maturation antigen |
| bFGF | Basic fibroblast growth factor |
| BMP-4 | Bone morphogenetic protein 4 |
| CAR-T | Chimeric antigen receptor T-Cell |
| CMV | Cytomegalovirus |
| CRS | Cytokine release syndrome |
| CXCR | Chemokine receptor |
| DAG | Diacylglycerol |
| DLL | Delta-like ligand |
| DN | Double negative |
| DP | Double positive |
| EB | Embryoid body |
| EBV | Epstein–Barr virus |
| EHT | Endothelial-to-hematopoietic transition |
| EMO | Embryonic mesodermal progenitor |
| ESC | Embryonic stem cell |
| FDA | Food and Drug Administration |
| FLT3L | Fms-related tyrosine kinase 3 ligand |
| GPC-3 | Glypican-3 |
| GvHD | Graft-versus-host disease |
| HDR | Homology-directed repair |
| hEMP | Human embryonic mesoderm progenitor |
| HIV | Human immunodeficiency virus |
| HLA | Human leukocyte antigen |
| HPV16 | Human papilloma virus type 16 |
| HSC | Hematopoietic stem cell |
| IFN | Interferon |
| IL | Interleukin |
| iPSC | Induced pluripotent stem cell |
| ISP | Intermediate single positive |
| mb | Membrane-bound |
| MHC | Major histocompatibility complex |
| MM | Multiple myeloma |
| MOI | Multiplicity of infection |
| NK | Natural killer |
| Oct | Octamer-binding transcription factor |
| PBMC | Peripheral blood mononuclear cells |
| PD-1 | Programmed cell death protein 1 |
| PHA | Phytohemagglutinin |
| RAG | Recombination-activating gene |
| Rb | Retinoblastoma |
| REP | Rapid expansion protocol |
| SCF | Stem cell factor |
| scFv | Single-chain variable fragment |
| SDF-1α | Stromal cell-derived factor 1 alpha |
| shRNA | Short hairpin RNA |
| SNP | Single-nucleotide polymorphism |
| Tcm | Central memory T-cell |
| TCR | T-cell receptor |
| Te | Effector T-cell |
| Th | T helper |
| TIL | Tumour-infiltrating lymphocyte |
| TMG | Tandem minigene |
| Tn | Naïve T-cell |
| TPO | Thrombopoietin |
| TRAC | T-cell receptor α constant |
| Tte | Terminal T-cell |
| VEGF | Vascular endothelial growth factor |
| VST | Viral-specific T-cell |
| WGS | Whole-genome sequencing |
References
- Ghorashian, S.; Pule, M.; Amrolia, P. CD19 Chimeric Antigen Receptor T Cell Therapy for Haematological Malignancies. Br. J. Haematol. 2015, 169, 463–478. [Google Scholar] [CrossRef] [PubMed]
- Mueller, K.T.; Grupp, S.A.; Maude, S.L.; Levine, J.E.; Pulsipher, M.A.; Boyer, M.W.; August, K.J.; Myers, G.D.; Tam, C.S.; Jaeger, U.; et al. Tisagenlecleucel Immunogenicity in Relapsed/Refractory Acute Lymphoblastic Leukemia and Diffuse Large B-Cell Lymphoma. Blood Adv. 2021, 5, 4980–4991. [Google Scholar] [CrossRef] [PubMed]
- Westin, J.R.; Oluwole, O.O.; Kersten, M.J.; Miklos, D.B.; Perales, M.-A.; Ghobadi, A.; Rapoport, A.P.; Sureda, A.; Jacobson, C.A.; Farooq, U.; et al. Survival with Axicabtagene Ciloleucel in Large B-Cell Lymphoma. N. Engl. J. Med. 2023, 389, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jain, P.; Locke, F.L.; Maurer, M.J.; Frank, M.J.; Munoz, J.L.; Dahiya, S.; Beitinjaneh, A.M.; Jacobs, M.T.; Mcguirk, J.P.; et al. Brexucabtagene Autoleucel for Relapsed or Refractory Mantle Cell Lymphoma in Standard-of-Care Practice: Results from the US Lymphoma CAR T Consortium. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2023, 41, 2594–2606. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, A.; Hoda, D.; Riedell, P.A.; Ghosh, N.; Hamadani, M.; Hildebrandt, G.C.; Godwin, J.E.; Reagan, P.M.; Wagner-Johnston, N.; Essell, J.; et al. Lisocabtagene Maraleucel as Second-Line Therapy in Adults with Relapsed or Refractory Large B-Cell Lymphoma Who Were Not Intended for Haematopoietic Stem Cell Transplantation (PILOT): An Open-Label, Phase 2 Study. Lancet Oncol. 2022, 23, 1066–1077. [Google Scholar] [CrossRef] [PubMed]
- Munshi, N.C.; Anderson, L.D.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef]
- Martin, T.; Usmani, S.Z.; Berdeja, J.G.; Agha, M.; Cohen, A.D.; Hari, P.; Avigan, D.; Deol, A.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene Autoleucel, an Anti-B-Cell Maturation Antigen Chimeric Antigen Receptor T-Cell Therapy, for Relapsed/Refractory Multiple Myeloma: CARTITUDE-1 2-Year Follow-Up. J. Clin. Oncol. 2023, 41, 1265–1274. [Google Scholar] [CrossRef]
- Liu, E.; Marin, D.; Banerjee, P.; Macapinlac, H.A.; Thompson, P.; Basar, R.; Nassif Kerbauy, L.; Overman, B.; Thall, P.; Kaplan, M.; et al. Use of CAR-Transduced Natural Killer Cells in CD19-Positive Lymphoid Tumors. N. Engl. J. Med. 2020, 382, 545–553. [Google Scholar] [CrossRef]
- Zhang, L.; Meng, Y.; Feng, X.; Han, Z. CAR-NK Cells for Cancer Immunotherapy: From Bench to Bedside. Biomark. Res. 2022, 10, 12. [Google Scholar] [CrossRef]
- Rohaan, M.W.; Borch, T.H.; van den Berg, J.H.; Met, Ö.; Kessels, R.; Geukes Foppen, M.H.; Stoltenborg Granhøj, J.; Nuijen, B.; Nijenhuis, C.; Jedema, I.; et al. Tumor-Infiltrating Lymphocyte Therapy or Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2022, 387, 2113–2125. [Google Scholar] [CrossRef]
- Zhao, Y.; Deng, J.; Rao, S.; Guo, S.; Shen, J.; Du, F.; Wu, X.; Chen, Y.; Li, M.; Chen, M.; et al. Tumor Infiltrating Lymphocyte (TIL) Therapy for Solid Tumor Treatment: Progressions and Challenges. Cancers 2022, 14, 4160. [Google Scholar] [CrossRef]
- Pfeiffer, T.; Tzannou, I.; Wu, M.; Ramos, C.; Sasa, G.; Martinez, C.; Lulla, P.; Krance, R.A.; Scherer, L.; Ruderfer, D.; et al. Posoleucel, an Allogeneic, Off-the-Shelf Multivirus-Specific T-Cell Therapy, for the Treatment of Refractory Viral Infections in the Post-HCT Setting. Clin. Cancer Res. 2023, 29, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Keller, M.D.; Bollard, C.M. Virus-Specific T-Cell Therapies for Patients with Primary Immune Deficiency. Blood 2020, 135, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Tumaini, B.; Lee, D.W.; Lin, T.; Castiello, L.; Stroncek, D.F.; Mackall, C.; Wayne, A.; Sabatino, M. Simplified Process for the Production of Anti-CD19-CAR Engineered T Cells. Cytotherapy 2013, 15, 1406–1415. [Google Scholar] [CrossRef]
- Roddie, C.; O’Reilly, M.; Dias Alves Pinto, J.; Vispute, K.; Lowdell, M. Manufacturing Chimeric Antigen Receptor T Cells: Issues and Challenges. Cytotherapy 2019, 21, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Vormittag, P.; Gunn, R.; Ghorashian, S.; Veraitch, F.S. A Guide to Manufacturing CAR T Cell Therapies. Curr. Opin. Biotechnol. 2018, 53, 164–181. [Google Scholar] [CrossRef]
- Hopewell, E.L.; Cox, C.; Pilon-Thomas, S.; Kelley, L.L. Tumor Infiltrating Lymphocytes Streamlining a Complex Manufacturing Process. Cytotherapy 2019, 21, 307–314. [Google Scholar] [CrossRef]
- Shafat, M.S.; Mehra, V.; Peggs, K.S.; Roddie, C. Cellular Therapeutic Approaches to Cytomegalovirus Infection Following Allogeneic Stem Cell Transplantation. Front. Immunol. 2020, 11, 1694. [Google Scholar] [CrossRef]
- Rohaan, M.W.; van den Berg, J.H.; Kvistborg, P.; Haanen, J.B.A.G. Adoptive Transfer of Tumor-Infiltrating Lymphocytes in Melanoma: A Viable Treatment Option. J. ImmunoTherapy Cancer 2018, 6, 102. [Google Scholar] [CrossRef]
- Inozume, T.; Hanada, K.; Wang, Q.J.; Ahmadzadeh, M.; Wunderlich, J.R.; Rosenberg, S.A.; Yang, J.C. Selection of CD8+PD-1+ Lymphocytes in Fresh Human Melanomas Enriches for Tumor-Reactive T-Cells. J. Immunother. 2010, 33, 956–964. [Google Scholar] [CrossRef]
- Ye, Q.; Song, D.-G.; Poussin, M.; Yamamoto, T.; Best, A.; Li, C.; Coukos, G.; Powell, D.J. CD137 Accurately Identifies and Enriches for Naturally Occurring Tumor-Reactive T Cells in Tumor. Clin. Cancer Res. 2014, 20, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R.; Cadieux, E.L.; Salgado, R.; Bakir, M.A.; Moore, D.A.; Hiley, C.T.; Lund, T.; Tanić, M.; Reading, J.L.; Joshi, K.; et al. Neoantigen-Directed Immune Escape in Lung Cancer Evolution. Nature 2019, 567, 479–485. [Google Scholar] [CrossRef]
- Donia, M.; Junker, N.; Ellebaek, E.; Andersen, M.H.; Straten, P.T.; Svane, I.M. Characterization and Comparison of “standard” and “Young” Tumour-Infiltrating Lymphocytes for Adoptive Cell Therapy at a Danish Translational Research Institution. Scand. J. Immunol. 2012, 75, 157–167. [Google Scholar] [CrossRef]
- Tran, K.Q.; Zhou, J.; Durflinger, K.H.; Langhan, M.M.; Shelton, T.E.; Wunderlich, J.R.; Robbins, P.F.; Rosenberg, S.A.; Dudley, M.E. Minimally Cultured Tumor-Infiltrating Lymphocytes Display Optimal Characteristics for Adoptive Cell Therapy. J. Immunother. 2008, 31, 742–751. [Google Scholar] [CrossRef]
- Fraietta, J.A.; Lacey, S.F.; Orlando, E.J.; Pruteanu-Malinici, I.; Gohil, M.; Lundh, S.; Boesteanu, A.C.; Wang, Y.; O’Connor, R.S.; Hwang, W.-T.; et al. Author Correction: Determinants of Response and Resistance to CD19 Chimeric Antigen Receptor (CAR) T Cell Therapy of Chronic Lymphocytic Leukemia. Nat. Med. 2021, 27, 561. [Google Scholar] [CrossRef] [PubMed]
- Tu, W.; Rao, S. Mechanisms Underlying T Cell Immunosenescence: Aging and Cytomegalovirus Infection. Front. Microbiol. 2016, 7, 2111. [Google Scholar] [CrossRef] [PubMed]
- Das, R.K.; Vernau, L.; Grupp, S.A.; Barrett, D.M. Naïve T-Cell Deficits at Diagnosis and after Chemotherapy Impair Cell Therapy Potential in Pediatric Cancers. Cancer Discov. 2019, 9, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Heipertz, E.L.; Zynda, E.R.; Stav-Noraas, T.E.; Hungler, A.D.; Boucher, S.E.; Kaur, N.; Vemuri, M.C. Current Perspectives on “Off-The-Shelf” Allogeneic NK and CAR-NK Cell Therapies. Front. Immunol. 2021, 12, 732135. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Lin, Q.; Song, Y.; Liu, D. Universal CARs, Universal T Cells, and Universal CAR T Cells. J. Hematol. Oncol. 2018, 11, 132. [Google Scholar] [CrossRef] [PubMed]
- Depil, S.; Duchateau, P.; Grupp, S.A.; Mufti, G.; Poirot, L. ‘Off-the-Shelf’ Allogeneic CAR T Cells: Development and Challenges. Nat. Rev. Drug Discov. 2020, 19, 185–199. [Google Scholar] [CrossRef]
- Martínez Bedoya, D.; Dutoit, V.; Migliorini, D. Allogeneic CAR T Cells: An Alternative to Overcome Challenges of CAR T Cell Therapy in Glioblastoma. Front. Immunol. 2021, 12, 640082. [Google Scholar] [CrossRef]
- Nishimura, T.; Kaneko, S.; Kawana-Tachikawa, A.; Tajima, Y.; Goto, H.; Zhu, D.; Nakayama-Hosoya, K.; Iriguchi, S.; Uemura, Y.; Shimizu, T.; et al. Generation of Rejuvenated Antigen-Specific T Cells by Reprogramming to Pluripotency and Redifferentiation. Cell Stem Cell 2013, 12, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Euchner, J.; Sprissler, J.; Cathomen, T.; Fürst, D.; Schrezenmeier, H.; Debatin, K.-M.; Schwarz, K.; Felgentreff, K. Natural Killer Cells Generated from Human Induced Pluripotent Stem Cells Mature to CD56brightCD16+NKp80+/-In-Vitro and Express KIR2DL2/DL3 and KIR3DL1. Front. Immunol. 2021, 12, 640672. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Iriguchi, S.; Waseda, M.; Ueda, N.; Ueda, T.; Xu, H.; Minagawa, A.; Ishikawa, A.; Yano, H.; Ishi, T.; et al. Generation of Hypoimmunogenic T Cells from Genetically Engineered Allogeneic Human Induced Pluripotent Stem Cells. Nat. Biomed. Eng. 2021, 5, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Bachanova, V.; Ghobadi, A.; Patel, K.; Park, J.H.; Flinn, I.W.; Shah, P.; Wong, C.; Bickers, C.; Szabo, P.; Wong, L.; et al. Safety and Efficacy of FT596, a First-in-Class, Multi-Antigen Targeted, Off-the-Shelf, IPSC-Derived CD19 CAR NK Cell Therapy in Relapsed/Refractory B-Cell Lymphoma. Blood 2021, 138, 823. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Mouse Embryonic and Adult Fibroblast Cultures by Defined Factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Adult Human Fibroblasts by Defined Factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef]
- Kunitomi, A.; Hirohata, R.; Arreola, V.; Osawa, M.; Kato, T.M.; Nomura, M.; Kawaguchi, J.; Hara, H.; Kusano, K.; Takashima, Y.; et al. Improved Sendai Viral System for Reprogramming to Naive Pluripotency. Cell Rep. Methods 2022, 2, 100317. [Google Scholar] [CrossRef]
- Yu, J.; Vodyanik, M.A.; Smuga-Otto, K.; Antosiewicz-Bourget, J.; Frane, J.L.; Tian, S.; Nie, J.; Jonsdottir, G.A.; Ruotti, V.; Stewart, R.; et al. Induced Pluripotent Stem Cell Lines Derived from Human Somatic Cells. Science 2007, 318, 1917–1920. [Google Scholar] [CrossRef]
- Kamath, A.; Ternes, S.; McGowan, S.; English, A.; Mallampalli, R.; Moy, A.B. Efficient Method to Create Integration-Free, Virus-Free, Myc and Lin28-Free Human Induced Pluripotent Stem Cells from Adherent Cells. Future Sci. OA 2017, 3, FSO211. [Google Scholar] [CrossRef]
- Haase, A.; Olmer, R.; Schwanke, K.; Wunderlich, S.; Merkert, S.; Hess, C.; Zweigerdt, R.; Gruh, I.; Meyer, J.; Wagner, S.; et al. Generation of Induced Pluripotent Stem Cells from Human Cord Blood. Cell Stem Cell 2009, 5, 434–441. [Google Scholar] [CrossRef]
- Lowry, W.E.; Richter, L.; Yachechko, R.; Pyle, A.D.; Tchieu, J.; Sridharan, R.; Clark, A.T.; Plath, K. Generation of Human Induced Pluripotent Stem Cells from Dermal Fibroblasts. Proc. Natl. Acad. Sci. USA 2008, 105, 2883–2888. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Rim, Y.A.; Yi, H.; Park, N.; Park, S.-H.; Ju, J.H. The Generation of Human Induced Pluripotent Stem Cells from Blood Cells: An Efficient Protocol Using Serial Plating of Reprogrammed Cells by Centrifugation. Stem Cells Int. 2016, 2016, 1329459. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, U.; Benvenisty, N. The Tumorigenicity of Human Embryonic and Induced Pluripotent Stem Cells. Nat. Rev. Cancer 2011, 11, 268–277. [Google Scholar] [CrossRef]
- Fusaki, N.; Ban, H.; Nishiyama, A.; Saeki, K.; Hasegawa, M. Efficient Induction of Transgene-Free Human Pluripotent Stem Cells Using a Vector Based on Sendai Virus, an RNA Virus That Does Not Integrate into the Host Genome. Proc. Jpn. Acad. Ser. B 2009, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Freed, C.R. Adenoviral Gene Delivery Can Reprogram Human Fibroblasts to Induced Pluripotent Stem Cells. Stem Cells 2009, 27, 2667–2674. [Google Scholar] [CrossRef]
- Okita, K.; Yamakawa, T.; Matsumura, Y.; Sato, Y.; Amano, N.; Watanabe, A.; Goshima, N.; Yamanaka, S. An Efficient Nonviral Method to Generate Integration-Free Human-Induced Pluripotent Stem Cells from Cord Blood and Peripheral Blood Cells. Stem Cells 2013, 31, 458–466. [Google Scholar] [CrossRef]
- Yu, J.; Hu, K.; Smuga-Otto, K.; Tian, S.; Stewart, R.; Slukvin, I.I.; Thomson, J.A. Human Induced Pluripotent Stem Cells Free of Vector and Transgene Sequences. Science 2009, 324, 797–801. [Google Scholar] [CrossRef]
- Warren, L.; Manos, P.D.; Ahfeldt, T.; Loh, Y.-H.; Li, H.; Lau, F.; Ebina, W.; Mandal, P.K.; Smith, Z.D.; Meissner, A.; et al. Highly Efficient Reprogramming to Pluripotency and Directed Differentiation of Human Cells with Synthetic Modified MRNA. Cell Stem Cell 2010, 7, 618–630. [Google Scholar] [CrossRef]
- Woltjen, K.; Michael, I.P.; Mohseni, P.; Desai, R.; Mileikovsky, M.; Hämäläinen, R.; Cowling, R.; Wang, W.; Liu, P.; Gertsenstein, M.; et al. PiggyBac Transposition Reprograms Fibroblasts to Induced Pluripotent Stem Cells. Nature 2009, 458, 766–770. [Google Scholar] [CrossRef]
- Jia, F.; Wilson, K.D.; Sun, N.; Gupta, D.M.; Huang, M.; Li, Z.; Robbins, R.C.; Kay, M.A.; Longaker, M.T.; Wu, J.C. A Nonviral Minicircle Vector for Deriving Human IPS Cells. Nat. Methods 2010, 7, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Baghbaderani, B.A.; Syama, A.; Sivapatham, R.; Pei, Y.; Mukherjee, O.; Fellner, T.; Zeng, X.; Rao, M.S. Detailed Characterization of Human Induced Pluripotent Stem Cells Manufactured for Therapeutic Applications. Stem Cell Rev. 2016, 12, 394–420. [Google Scholar] [CrossRef]
- Kuang, Y.-L.; Munoz, A.; Nalula, G.; Santostefano, K.E.; Sanghez, V.; Sanchez, G.; Terada, N.; Mattis, A.N.; Iacovino, M.; Iribarren, C.; et al. Evaluation of Commonly Used Ectoderm Markers in IPSC Trilineage Differentiation. Stem Cell Res. 2019, 37, 101434. [Google Scholar] [CrossRef]
- Martins-Taylor, K.; Xu, R.-H. Concise Review: Genomic Stability of Human Induced Pluripotent Stem Cells. Stem Cells 2012, 30, 22–27. [Google Scholar] [CrossRef]
- Kogut, I.; McCarthy, S.M.; Pavlova, M.; Astling, D.P.; Chen, X.; Jakimenko, A.; Jones, K.L.; Getahun, A.; Cambier, J.C.; Pasmooij, A.M.G.; et al. High-Efficiency RNA-Based Reprogramming of Human Primary Fibroblasts. Nat. Commun. 2018, 9, 745. [Google Scholar] [CrossRef] [PubMed]
- Malik, N.; Rao, M.S. A Review of the Methods for Human IPSC Derivation. Methods Mol. Biol. 2013, 997, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Okita, K.; Fusaki, N.; Sabel, M.S.; Chang, A.E.; Ito, F. Reprogramming of Melanoma Tumor-Infiltrating Lymphocytes to Induced Pluripotent Stem Cells. Stem Cells Int. 2016, 2016, 8394960. [Google Scholar] [CrossRef]
- Seki, T.; Yuasa, S.; Oda, M.; Egashira, T.; Yae, K.; Kusumoto, D.; Nakata, H.; Tohyama, S.; Hashimoto, H.; Kodaira, M.; et al. Generation of Induced Pluripotent Stem Cells from Human Terminally Differentiated Circulating T Cells. Cell Stem Cell 2010, 7, 11–14. [Google Scholar] [CrossRef]
- Gattinoni, L.; Speiser, D.E.; Lichterfeld, M.; Bonini, C. T Memory Stem Cells in Health and Disease. Nat. Med. 2017, 23, 18–27. [Google Scholar] [CrossRef]
- Banito, A.; Rashid, S.T.; Acosta, J.C.; Li, S.; Pereira, C.F.; Geti, I.; Pinho, S.; Silva, J.C.; Azuara, V.; Walsh, M.; et al. Senescence Impairs Successful Reprogramming to Pluripotent Stem Cells. Genes Dev. 2009, 23, 2134–2139. [Google Scholar] [CrossRef]
- Mali, P.; Ye, Z.; Hommond, H.H.; Yu, X.; Lin, J.; Chen, G.; Zou, J.; Cheng, L. Improved Efficiency and Pace of Generating Induced Pluripotent Stem Cells from Human Adult and Fetal Fibroblasts. Stem Cells 2008, 26, 1998–2005. [Google Scholar] [CrossRef]
- Chou, B.-K.; Mali, P.; Huang, X.; Ye, Z.; Dowey, S.N.; Resar, L.M.; Zou, C.; Zhang, Y.A.; Tong, J.; Cheng, L. Efficient Human IPS Cell Derivation by a Non-Integrating Plasmid from Blood Cells with Unique Epigenetic and Gene Expression Signatures. Cell Res. 2011, 21, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Galić, Z.; Kitchen, S.G.; Kacena, A.; Subramanian, A.; Burke, B.; Cortado, R.; Zack, J.A. T Lineage Differentiation from Human Embryonic Stem Cells. Proc. Natl. Acad. Sci. USA 2006, 103, 11742–11747. [Google Scholar] [CrossRef] [PubMed]
- Vodyanik, M.A.; Bork, J.A.; Thomson, J.A.; Slukvin, I.I. Human Embryonic Stem Cell–Derived CD34+ Cells: Efficient Production in the Coculture with OP9 Stromal Cells and Analysis of Lymphohematopoietic Potential. Blood 2005, 105, 617–626. [Google Scholar] [CrossRef]
- Nagano, S.; Maeda, T.; Ichise, H.; Kashima, S.; Ohtaka, M.; Nakanishi, M.; Kitawaki, T.; Kadowaki, N.; Takaori-Kondo, A.; Masuda, K.; et al. High Frequency Production of T Cell-Derived IPSC Clones Capable of Generating Potent Cytotoxic T Cells. Mol. Ther. Methods Clin. Dev. 2019, 16, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Ueda, T.; Shiina, S.; Iriguchi, S.; Terakura, S.; Kawai, Y.; Kabai, R.; Sakamoto, S.; Watanabe, A.; Ohara, K.; Wang, B.; et al. Optimization of the Proliferation and Persistency of CAR T Cells Derived from Human Induced Pluripotent Stem Cells. Nat. Biomed. Eng. 2022, 7, 24–37. [Google Scholar] [CrossRef]
- Themeli, M.; Kloss, C.C.; Ciriello, G.; Fedorov, V.D.; Perna, F.; Gonen, M.; Sadelain, M. Generation of Tumor-Targeted Human T Lymphocytes from Induced Pluripotent Stem Cells for Cancer Therapy. Nat. Biotechnol. 2013, 31, 928–933. [Google Scholar] [CrossRef]
- Iriguchi, S.; Yasui, Y.; Kawai, Y.; Arima, S.; Kunitomo, M.; Sato, T.; Ueda, T.; Minagawa, A.; Mishima, Y.; Yanagawa, N.; et al. A Clinically Applicable and Scalable Method to Regenerate T-Cells from IPSCs for off-the-Shelf T-Cell Immunotherapy. Nat. Commun. 2021, 12, 430. [Google Scholar] [CrossRef]
- van der Stegen, S.J.C.; Lindenbergh, P.L.; Petrovic, R.M.; Xie, H.; Diop, M.P.; Alexeeva, V.; Shi, Y.; Mansilla-Soto, J.; Hamieh, M.; Eyquem, J.; et al. Generation of T-Cell-Receptor-Negative CD8αβ-Positive CAR T Cells from T-Cell-Derived Induced Pluripotent Stem Cells. Nat. Biomed. Eng. 2022, 6, 1284–1297. [Google Scholar] [CrossRef]
- Schwanbeck, R.; Just, U. The Notch Signaling Pathway in Hematopoiesis and Hematologic Malignancies. Haematologica 2011, 96, 1735–1737. [Google Scholar] [CrossRef]
- Montel-Hagen, A.; Crooks, G.M. From Pluripotent Stem Cells to T Cells. Exp. Hematol. 2019, 71, 24–31. [Google Scholar] [CrossRef]
- Leung, A.; Zulick, E.; Skvir, N.; Vanuytsel, K.; Morrison, T.A.; Naing, Z.H.; Wang, Z.; Dai, Y.; Chui, D.H.K.; Steinberg, M.H.; et al. Notch and Aryl Hydrocarbon Receptor Signaling Impact Definitive Hematopoiesis from Human Pluripotent Stem Cells. Stem Cells 2018, 36, 1004–1019. [Google Scholar] [CrossRef] [PubMed]
- Mohtashami, M.; Shah, D.K.; Nakase, H.; Kianizad, K.; Petrie, H.T.; Zúñiga-Pflücker, J.C. Direct Comparison of Dll1- and Dll4-Mediated Notch Activation Levels Shows Differential Lymphomyeloid Lineage Commitment Outcomes. J. Immunol. 2010, 185, 867–876. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.; Awong, G.; Sturgeon, C.M.; Ditadi, A.; LaMotte-Mohs, R.; Zúñiga-Pflücker, J.C.; Keller, G. T Lymphocyte Potential Marks the Emergence of Definitive Hematopoietic Progenitors in Human Pluripotent Stem Cell Differentiation Cultures. Cell Rep. 2012, 2, 1722–1735. [Google Scholar] [CrossRef] [PubMed]
- Vizcardo, R.; Masuda, K.; Yamada, D.; Ikawa, T.; Shimizu, K.; Fujii, S.; Koseki, H.; Kawamoto, H. Regeneration of Human Tumor Antigen-Specific T Cells from IPSCs Derived from Mature CD8+ T Cells. Cell Stem Cell 2013, 12, 31–36. [Google Scholar] [CrossRef]
- Montel-Hagen, A.; Seet, C.S.; Li, S.; Chick, B.; Zhu, Y.; Chang, P.; Tsai, S.; Sun, V.; Lopez, S.; Chen, H.-C.; et al. Organoid-Induced Differentiation of Conventional T Cells from Human Pluripotent Stem Cells. Cell Stem Cell 2019, 24, 376–389.e8. [Google Scholar] [CrossRef]
- Trotman-Grant, A.C.; Mohtashami, M.; De Sousa Casal, J.; Martinez, E.C.; Lee, D.; Teichman, S.; Brauer, P.M.; Han, J.; Anderson, M.K.; Zúñiga-Pflücker, J.C. DL4-Μbeads Induce T Cell Lineage Differentiation from Stem Cells in a Stromal Cell-Free System. Nat. Commun. 2021, 12, 5023. [Google Scholar] [CrossRef]
- Vizcardo, R.; Klemen, N.D.; Islam, S.M.R.; Gurusamy, D.; Tamaoki, N.; Yamada, D.; Koseki, H.; Kidder, B.L.; Yu, Z.; Jia, L.; et al. Generation of Tumor Antigen-Specific IPSC-Derived Thymic Emigrants Using a 3D Thymic Culture System. Cell Rep. 2018, 22, 3175–3190. [Google Scholar] [CrossRef]
- Maeda, T.; Nagano, S.; Ichise, H.; Kataoka, K.; Yamada, D.; Ogawa, S.; Koseki, H.; Kitawaki, T.; Kadowaki, N.; Takaori-Kondo, A.; et al. Regeneration of CD8αβ T Cells from T-Cell–Derived IPSC Imparts Potent Tumor Antigen-Specific Cytotoxicity. Cancer Res. 2016, 76, 6839–6850. [Google Scholar] [CrossRef] [PubMed]
- Yano, H.; Shinohara, T.; Koga, K.; Iriguchi, S.; Miyake, Y.; Song, X.; Tada, M.; Kassai, Y.; Kiyoi, H.; Kaneko, S. Guided Polarization of IPSC-Derived CD4SP Helper T Cells By CRISPR/Cas9-Based Genome-Editing. Blood 2019, 134, 1937. [Google Scholar] [CrossRef]
- Minagawa, A.; Yoshikawa, T.; Yasukawa, M.; Hotta, A.; Kunitomo, M.; Iriguchi, S.; Takiguchi, M.; Kassai, Y.; Imai, E.; Yasui, Y.; et al. Enhancing T Cell Receptor Stability in Rejuvenated IPSC-Derived T Cells Improves Their Use in Cancer Immunotherapy. Cell Stem Cell 2018, 23, 850–858.e4. [Google Scholar] [CrossRef]
- Kawai, Y.; Kawana-Tachikawa, A.; Kitayama, S.; Ueda, T.; Miki, S.; Watanabe, A.; Kaneko, S. Generation of Highly Proliferative, Rejuvenated Cytotoxic T Cell Clones through Pluripotency Reprogramming for Adoptive Immunotherapy. Mol. Ther. 2021, 29, 3027–3041. [Google Scholar] [CrossRef] [PubMed]
- Knorr, D.A.; Ni, Z.; Hermanson, D.; Hexum, M.K.; Bendzick, L.; Cooper, L.J.N.; Lee, D.A.; Kaufman, D.S. Clinical-Scale Derivation of Natural Killer Cells from Human Pluripotent Stem Cells for Cancer Therapy. Stem Cells Transl. Med. 2013, 2, 274–283. [Google Scholar] [CrossRef]
- Woll, P.S.; Grzywacz, B.; Tian, X.; Marcus, R.K.; Knorr, D.A.; Verneris, M.R.; Kaufman, D.S. Human Embryonic Stem Cells Differentiate into a Homogeneous Population of Natural Killer Cells with Potent In Vivo Antitumor Activity. Blood 2009, 113, 6094–6101. [Google Scholar] [CrossRef] [PubMed]
- Ni, Z.; Knorr, D.A.; Clouser, C.L.; Hexum, M.K.; Southern, P.; Mansky, L.M.; Park, I.-H.; Kaufman, D.S. Human Pluripotent Stem Cells Produce Natural Killer Cells That Mediate Anti-HIV-1 Activity by Utilizing Diverse Cellular Mechanisms. J. Virol. 2011, 85, 43–50. [Google Scholar] [CrossRef]
- Hermanson, D.L.; Ni, Z.; Kaufman, D.S. Human Pluripotent Stem Cells. In Hematopoietic Differentiation of Human Pluripotent Stem Cells; Cheng, T., Ed.; SpringerBriefs in Stem Cells; Springer: Dordrecht, The Netherlands, 2015; Volume 6, pp. 69–79. ISBN 978-94-017-7311-9. [Google Scholar]
- Denman, C.J.; Senyukov, V.V.; Somanchi, S.S.; Phatarpekar, P.V.; Kopp, L.M.; Johnson, J.L.; Singh, H.; Hurton, L.; Maiti, S.N.; Huls, M.H.; et al. Membrane-Bound IL-21 Promotes Sustained Ex Vivo Proliferation of Human Natural Killer Cells. PLoS ONE 2012, 7, e30264. [Google Scholar] [CrossRef]
- Hermanson, D.L.; Bendzick, L.; Pribyl, L.; McCullar, V.; Vogel, R.I.; Miller, J.S.; Geller, M.A.; Kaufman, D.S. Induced Pluripotent Stem Cell-Derived Natural Killer Cells for Treatment of Ovarian Cancer. Stem Cells 2016, 34, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Nianias, A.; Themeli, M. Induced Pluripotent Stem Cell (IPSC)–Derived Lymphocytes for Adoptive Cell Immunotherapy: Recent Advances and Challenges. Curr. Hematol. Malig. Rep. 2019, 14, 261–268. [Google Scholar] [CrossRef]
- Nakatsuji, N.; Nakajima, F.; Tokunaga, K. HLA-Haplotype Banking and IPS Cells. Nat. Biotechnol. 2008, 26, 739–740. [Google Scholar] [CrossRef]
- Taylor, C.J.; Peacock, S.; Chaudhry, A.N.; Bradley, J.A.; Bolton, E.M. Generating an IPSC Bank for HLA-Matched Tissue Transplantation Based on Known Donor and Recipient HLA Types. Cell Stem Cell 2012, 11, 147–152. [Google Scholar] [CrossRef]
- Yumlu, S.; Stumm, J.; Bashir, S.; Dreyer, A.-K.; Lisowski, P.; Danner, E.; Kühn, R. Gene Editing and Clonal Isolation of Human Induced Pluripotent Stem Cells Using CRISPR/Cas9. Methods 2017, 121–122, 29–44. [Google Scholar] [CrossRef]
- Feucht, J.; Sun, J.; Eyquem, J.; Ho, Y.-J.; Zhao, Z.; Leibold, J.; Dobrin, A.; Cabriolu, A.; Hamieh, M.; Sadelain, M. Calibration of CAR Activation Potential Directs Alternative T Cell Fates and Therapeutic Potency. Nat. Med. 2019, 25, 82–88. [Google Scholar] [CrossRef]
- Mehta, A.; Farooq, U.; Chen, A.; McGuirk, J.P.; Ly, T.; Wong, L.; Cooley, S.; Valamehr, B.; Elstrom, R.; Chu, Y.-W.; et al. Interim Phase I Clinical Data of FT819-101, a Study of the First-Ever, Off-the-Shelf, IPSC-Derived TCR-Less CD19 CAR T-Cell Therapy for Patients with Relapsed/Refractory B-Cell Malignancies. Blood 2022, 140, 4577–4578. [Google Scholar] [CrossRef]
- Hermanson, D.L.; Kaufman, D.S. Utilizing Chimeric Antigen Receptors to Direct Natural Killer Cell Activity. Front. Immunol. 2015, 6, 195. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hermanson, D.L.; Moriarity, B.S.; Kaufman, D.S. Human IPSC-Derived Natural Killer Cells Engineered with Chimeric Antigen Receptors Enhance Anti-Tumor Activity. Cell Stem Cell 2018, 23, 181–192.e5. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.; Patel, S.; Patel, M.; Musni, K.; Anderson, M.; Cooley, S.; Valamehr, B.; Chu, W. 380 Preliminary Results of an Ongoing Phase I Trial of FT500, a First-in-Class, off-the-Shelf, Induced Pluripotent Stem Cell (IPSC) Derived Natural Killer (NK) Cell Therapy in Advanced Solid Tumors. J. Immunother. Cancer 2020, 8, A405. [Google Scholar] [CrossRef]
- Gutierrez, M.; Patel, M.; Liu, F.; Szabo, P.; Valamehr, B.; Chu, Y.-W.; Beagle, B.; Chou, J.; Hong, D. 726 Phase I Results of FT516, an off-the-Shelf, IPSC-Derived NK Cell Therapy Expressing a High-Affinity, Non-Cleavable CD16 (HnCD16) Combined with Avelumab in Patients with Advanced Solid Tumors. J. Immunother. Cancer 2022, 10. [Google Scholar] [CrossRef]
- Goulding, J.; Hancock, B.; Blum, R.; Ge, M.; Gaidarova, S.; Rogers, P.; Mahmood, S.; Mbofung, R.; Yeh, W.-I.; Yang, B.-H.; et al. 117 FT536 Path to IND: Ubiquitous Targeting of Solid Tumors with an off-the-Shelf, First-of-Kind MICA/B-Specific CAR-INK Cellular Immunotherapy. J. Immunother. Cancer 2021, 9. [Google Scholar] [CrossRef]
- Dhakal, B.; Berdeja, J.G.; Gregory, T.; Ly, T.; Bickers, C.; Zong, X.; Wong, L.; Goodridge, J.P.; Cooley, S.; Valamehr, B.; et al. Interim Phase I Clinical Data of FT576 As Monotherapy and in Combination with Daratumumab in Subjects with Relapsed/Refractory Multiple Myeloma. Blood 2022, 140, 4586–4587. [Google Scholar] [CrossRef]
- Yannoutsos, N.; Wilson, P.; Yu, W.; Chen, H.T.; Nussenzweig, A.; Petrie, H.; Nussenzweig, M.C. The Role of Recombination Activating Gene (RAG) Reinduction in Thymocyte Development In Vivo. J. Exp. Med. 2001, 194, 471–480. [Google Scholar] [CrossRef]
- Ito, T.; Kawai, Y.; Yasui, Y.; Iriguchi, S.; Minagawa, A.; Ishii, T.; Miyoshi, H.; Taketo, M.M.; Kawada, K.; Obama, K.; et al. The Therapeutic Potential of Multiclonal Tumoricidal T Cells Derived from Tumor Infiltrating Lymphocyte-Derived IPS Cells. Commun. Biol. 2021, 4, 694. [Google Scholar] [CrossRef] [PubMed]
- Honda, T.; Ando, M.; Ando, J.; Ishii, M.; Sakiyama, Y.; Ohara, K.; Toyota, T.; Ohtaka, M.; Masuda, A.; Terao, Y.; et al. Sustainable Tumor-Suppressive Effect of IPSC-Derived Rejuvenated T Cells Targeting Cervical Cancers. Mol. Therapy 2020, 28, 2394–2405. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Ando, J.; Yamazaki, S.; Ishii, M.; Sakiyama, Y.; Harada, S.; Honda, T.; Yamaguchi, T.; Nojima, M.; Ohshima, K.; et al. Long-Term Eradication of Extranodal Natural Killer/T-Cell Lymphoma, Nasal Type, by Induced Pluripotent Stem Cell-Derived Epstein-Barr Virus-Specific Rejuvenated T Cells In Vivo. Haematologica 2020, 105, 796–807. [Google Scholar] [CrossRef]
- Terakura, S.; Yamamoto, T.N.; Gardner, R.A.; Turtle, C.J.; Jensen, M.C.; Riddell, S.R. Generation of CD19-Chimeric Antigen Receptor Modified CD8+ T Cells Derived from Virus-Specific Central Memory T Cells. Blood 2012, 119, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Bonifacius, A.; Lamottke, B.; Tischer-Zimmermann, S.; Schultze-Florey, R.; Goudeva, L.; Heuft, H.-G.; Arseniev, L.; Beier, R.; Beutel, G.; Cario, G.; et al. Patient-Tailored Adoptive Immunotherapy with EBV-Specific T Cells from Related and Unrelated Donors. J. Clin. Investig. 2023, 133, e163548. [Google Scholar] [CrossRef]
- Cobbold, M.; Khan, N.; Pourgheysari, B.; Tauro, S.; McDonald, D.; Osman, H.; Assenmacher, M.; Billingham, L.; Steward, C.; Crawley, C.; et al. Adoptive Transfer of Cytomegalovirus-Specific CTL to Stem Cell Transplant Patients after Selection by HLA-Peptide Tetramers. J. Exp. Med. 2005, 202, 379–386. [Google Scholar] [CrossRef]
- Fang, F.; Wang, W.; Chen, M.; Tian, Z.; Xiao, W. Technical Advances in NK Cell-Based Cellular Immunotherapy. Cancer Biol. Med. 2019, 16, 647–654. [Google Scholar] [CrossRef]
- Gras Navarro, A.; Björklund, A.T.; Chekenya, M. Therapeutic Potential and Challenges of Natural Killer Cells in Treatment of Solid Tumors. Front. Immunol. 2015, 6, 202. [Google Scholar] [CrossRef]
- Carlsten, M.; Childs, R.W. Genetic Manipulation of NK Cells for Cancer Immunotherapy: Techniques and Clinical Implications. Front. Immunol. 2015, 6, 266. [Google Scholar] [CrossRef]
- Afolabi, L.O.; Adeshakin, A.O.; Sani, M.M.; Bi, J.; Wan, X. Genetic Reprogramming for NK Cell Cancer Immunotherapy with CRISPR/Cas9. Immunology 2019, 158, 63–69. [Google Scholar] [CrossRef]
- Kang, S.; Gao, X.; Zhang, L.; Yang, E.; Li, Y.; Yu, L. The Advances and Challenges of NK Cell-Based Cancer Immunotherapy. Curr. Oncol. 2021, 28, 1077–1093. [Google Scholar] [CrossRef] [PubMed]
- Lindenberg, M.; Retèl, V.; Rohaan, M.; van den Berg, J.; Haanen, J.; van Harten, W. Evaluating Different Adoption Scenarios for TIL-Therapy and the Influence on Its (Early) Cost-Effectiveness. BMC Cancer 2020, 20, 712. [Google Scholar] [CrossRef] [PubMed]
- Webster, B.; Xiong, Y.; Hu, P.; Wu, D.; Alabanza, L.; Orentas, R.J.; Dropulic, B.; Schneider, D. Self-Driving Armored CAR-T Cells Overcome a Suppressive Milieu and Eradicate CD19+ Raji Lymphoma in Preclinical Models. Mol. Therapy 2021, 29, 2691–2706. [Google Scholar] [CrossRef]
- Heinze, D.; Park, S.; McCracken, A.; Haratianfar, M.; Lindstrom, J.; Villacorta-Martin, C.; Mithal, A.; Wang, F.; Yang, M.W.; Murphy, G.; et al. Notch Activation during Early Mesoderm Induction Modulates Emergence of the T/NK Cell Lineage from Human IPSCs. Stem Cell Rep. 2022, 17, 2610–2628. [Google Scholar] [CrossRef] [PubMed]
- Challenge Theme R&D Spotlight: Development of an End-to-End Closed IPSC Expansion Process—Cell and Gene Therapy. Available online: https://ct.catapult.org.uk/news/challenge-theme-r-d-spotlight-development-of-an-end-to-end-closed-ipsc-expansion-process (accessed on 28 October 2023).
- Pandey, P.R.; Tomney, A.; Woon, M.T.; Uth, N.; Shafighi, F.; Ngabo, I.; Vallabhaneni, H.; Levinson, Y.; Abraham, E.; Friedrich Ben-Nun, I. End-to-End Platform for Human Pluripotent Stem Cell Manufacturing. Int. J. Mol. Sci. 2019, 21, 89. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Kempf, H.; Hetzel, M.; Hesse, C.; Hashtchin, A.R.; Brinkert, K.; Schott, J.W.; Haake, K.; Kühnel, M.P.; Glage, S.; et al. Bioreactor-Based Mass Production of Human IPSC-Derived Macrophages Enables Immunotherapies against Bacterial Airway Infections. Nat. Commun. 2018, 9, 5088. [Google Scholar] [CrossRef] [PubMed]
| iPSC-Derived NK Cell Therapy | ||||||
| Clinical Trial | Description | Condition | Company | Phase | Cell Product | Status |
| NCT03841110 | FT500 in combination with checkpoint inhibitors against solid tumours | Advanced solid tumour | Fate Therapeutics | I | iPSC-derived NK (allogenic) | Completed |
| NCT04106167 | Long-term, non-interventional, observational study following treatment with Fate Therapeutics FT500 | Cancer/Tumour | Fate Therapeutics | N/A | PSC-derived NK (allogenic) | Terminated |
| NCT05182073 | FT576 in subjects with multiple myeloma (MM) | Multiple myeloma | Fate Therapeutics | I | iPSC-derived NK (allogenic) | Recruiting |
| NCT04630769 | FT516 and IL2 with Enoblituzumab for ovarian cancer | Ovarian cancer; fallopian tube adenocarcinoma, primary peritoneal cavity cancer | Masonic Cancer Centre, University of Minnesota | I | iPSC-derived NK (non-cleavable CD16 Fc receptor) (allogenic) | Completed |
| NCT04023071 | FT516 in combination with CD20-directed monoclonal antibodies | Advanced haematological malignancies | Fate Therapeutics | I | iPSC-derived NK cells (allogenic) | Terminated |
| NCT04551885 | FT516 in combination with monoclonal antibodies | Advanced solid tumours | Fate Therapeutics | I | iPSC-derived NK | Terminated |
| NCT04245722 | FT596 as a monotherapy and in combination with anti-CD20 monoclonal antibodies | B-cell lymphoma, chronic lymphocytic leukaemia | Fate Therapeutics | I | FT596 (hnCD16/anti-CD19 CAR/IL-15RF) iPSC-derived NK cells | Terminated |
| NCT04555811 | FT596 with rituximab | Non-Hodgkin lymphoma, diffuse large B-cell lymphoma, high-grade B-cell lymphoma | Masonic Cancer Centre, University of Minnesota | I | (hnCD16/anti-CD19 CAR/IL-15RF) iPSC-derived NK cells | Active, not recruiting |
| NCT05395052 | FT536 monotherapy and in combination with monoclonal antibodies | Advanced solid tumours | Fate Therapeutics | I | (hCD16/CD38KO/anti-MICA/B CAR/IL-15RF) iPSC-derived NK cells (allogeneic) | Terminated |
| NCT05069935 | FT538 in combination with monoclonal antibodies | Advanced solid tumours | Fate Therapeutics | I | FT538 (hnCD16/CD38KO/IL-15RF) iPSC-derived NK cells | Terminated |
| NCT04714372 | FT538 in combination with daratumumab | Acute myeloid leukaemia | Masonic Cancer Centre, University of Minnesota | I | FT538 (hnCD16/CD38KO/IL-15RF) iPSC-derived NK cells | Recruiting |
| NCT04614636 | FT538 | Advanced hematologic malignancies | Fate Therapeutics | I | FT538 (hnCD16/CD38KO/IL-15RF) iPSC-derived NK cells | Terminated |
| IRCT20200429047241N1 | Personalized immunology of patients with advanced breast cancer using induced pluripotent stem cell-derived natural killer cells | Breast cancer | Tehran University of Medical Science | I | Autologous iPSC-derived NK cells | Recruiting |
| iPSC-Derived T-cell Therapy | ||||||
| NCT05336409 | CNTY-101 | CD19-positive B-cell malignancies (ELiPSE-1) | Century Therapeutics, Inc. | I | (sIL-15/EGFRt/anti-CD19 CAR) iPSC-derived T-cells with IL-2 | Recruiting |
| NCT04629729 | FT819 | B-cell malignancies | Fate Therapeutics | I | iPSC-T (CAR-19, TCR-KO) | Recruiting |
| NCT03407040 | Generation of cancer antigen-specific T-cells from human induced pluripotent stem cells (iPSC) for research and potential future therapy | Gastrointestinal cancers, breast cancer, pancreatic cancer, melanoma, lung cancer | National Cancer Institute (NCI) | N/A | Cancer antigen-specific T-cells from human induced pluripotent stem cells | Terminated |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehra, V.; Chhetri, J.B.; Ali, S.; Roddie, C. The Emerging Role of Induced Pluripotent Stem Cells as Adoptive Cellular Immunotherapeutics. Biology 2023, 12, 1419. https://doi.org/10.3390/biology12111419
Mehra V, Chhetri JB, Ali S, Roddie C. The Emerging Role of Induced Pluripotent Stem Cells as Adoptive Cellular Immunotherapeutics. Biology. 2023; 12(11):1419. https://doi.org/10.3390/biology12111419
Chicago/Turabian StyleMehra, Vedika, Jyoti Bikram Chhetri, Samira Ali, and Claire Roddie. 2023. "The Emerging Role of Induced Pluripotent Stem Cells as Adoptive Cellular Immunotherapeutics" Biology 12, no. 11: 1419. https://doi.org/10.3390/biology12111419
APA StyleMehra, V., Chhetri, J. B., Ali, S., & Roddie, C. (2023). The Emerging Role of Induced Pluripotent Stem Cells as Adoptive Cellular Immunotherapeutics. Biology, 12(11), 1419. https://doi.org/10.3390/biology12111419