
Programmed Cell Death Ligand 1 Expression in Circulating Tumor Cells as a Predictor of Treatment Response in Patients with Urothelial Carcinoma

 ,
, 

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Blood Sample Collection
2.2. Immunomagnetic Bead Preparation for CTC Isolation
2.3. Sample Preparation
2.4. Sample Isolation and Collection
2.5. CTC Analysis and Immunofluorescence
2.6. Cell Culture and Spike-In Experiment
2.7. Immunocytochemistry for PD-L1
2.8. Statistical Analysis
3. Results
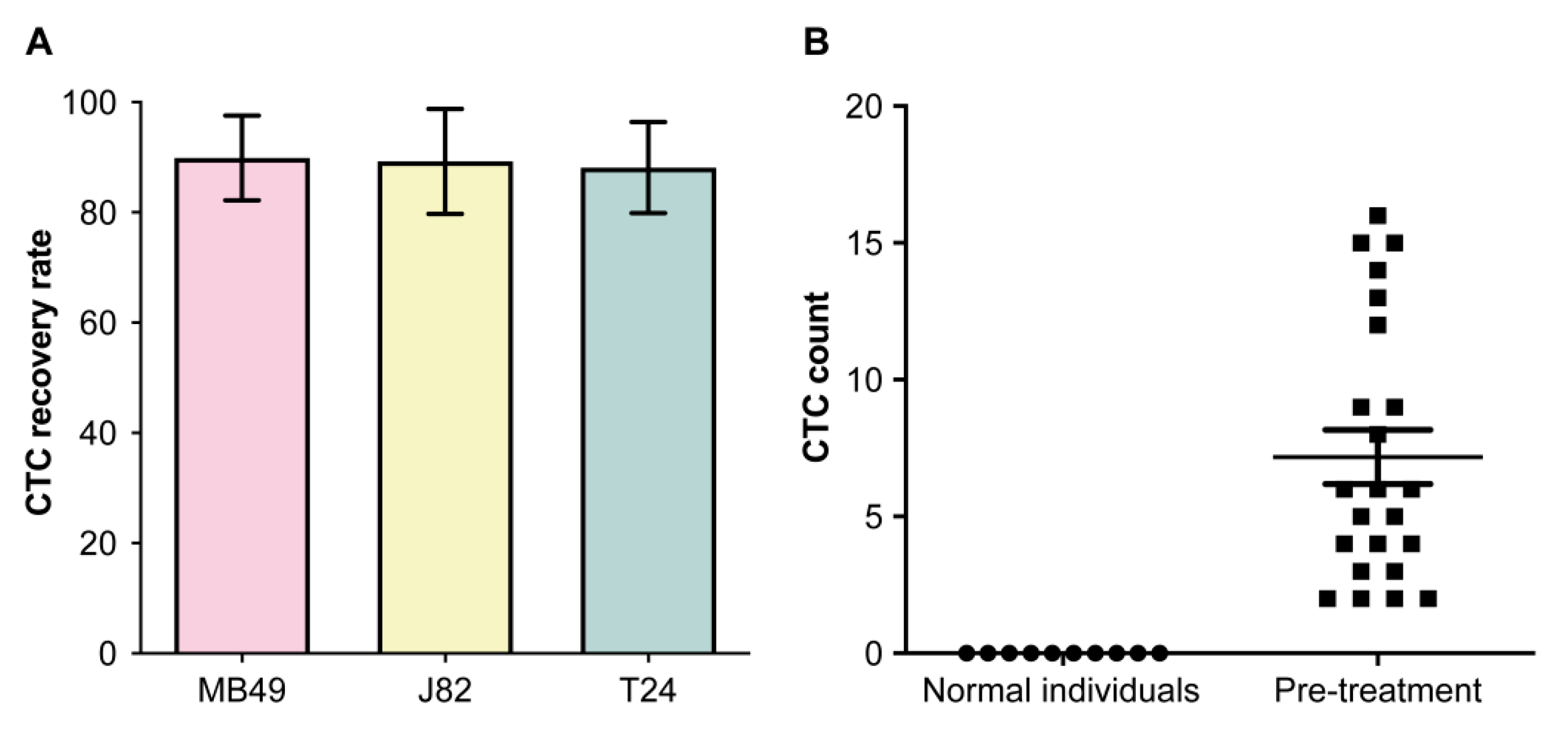
3.1. Detection of Circulating UC Cells
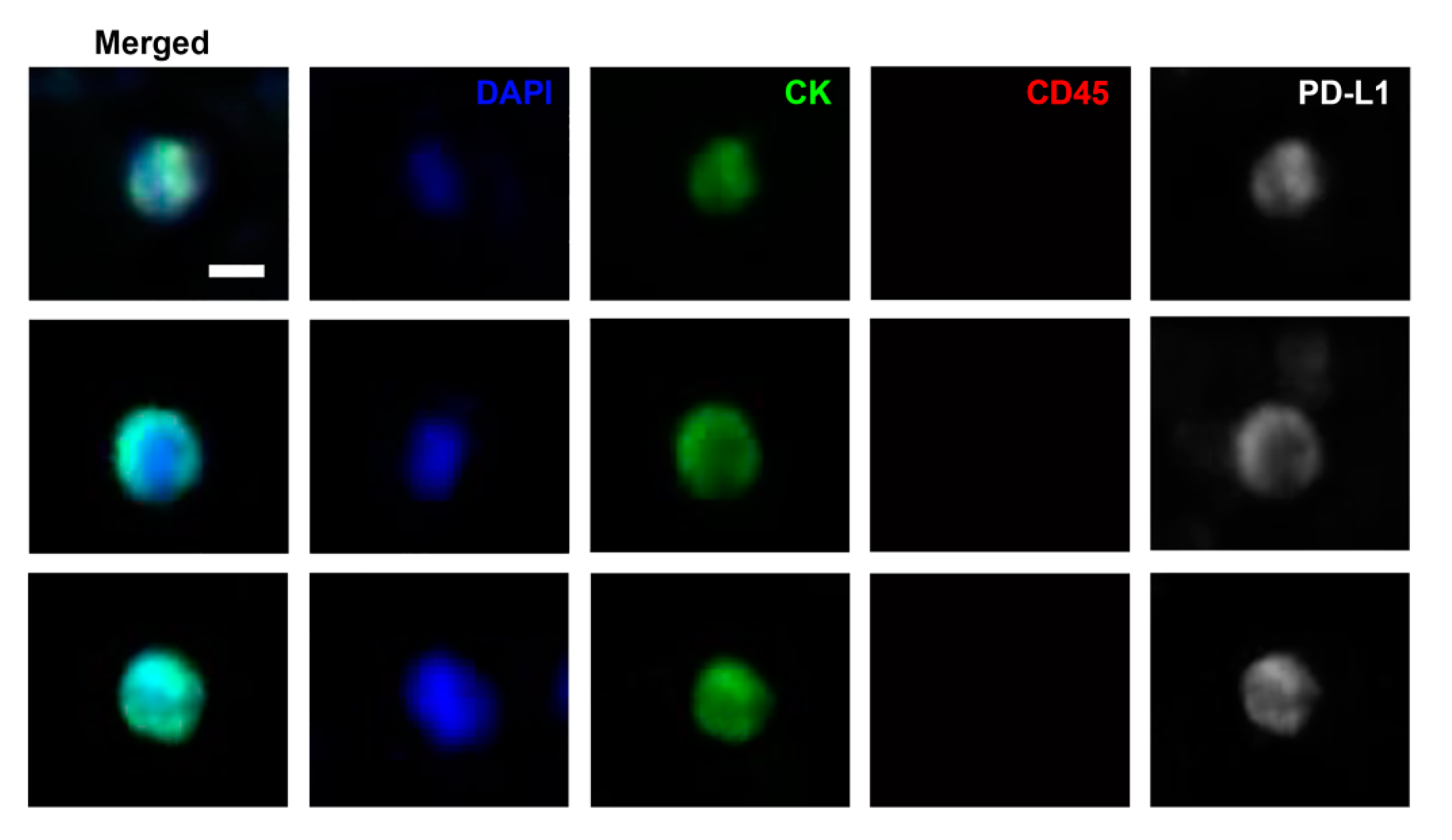
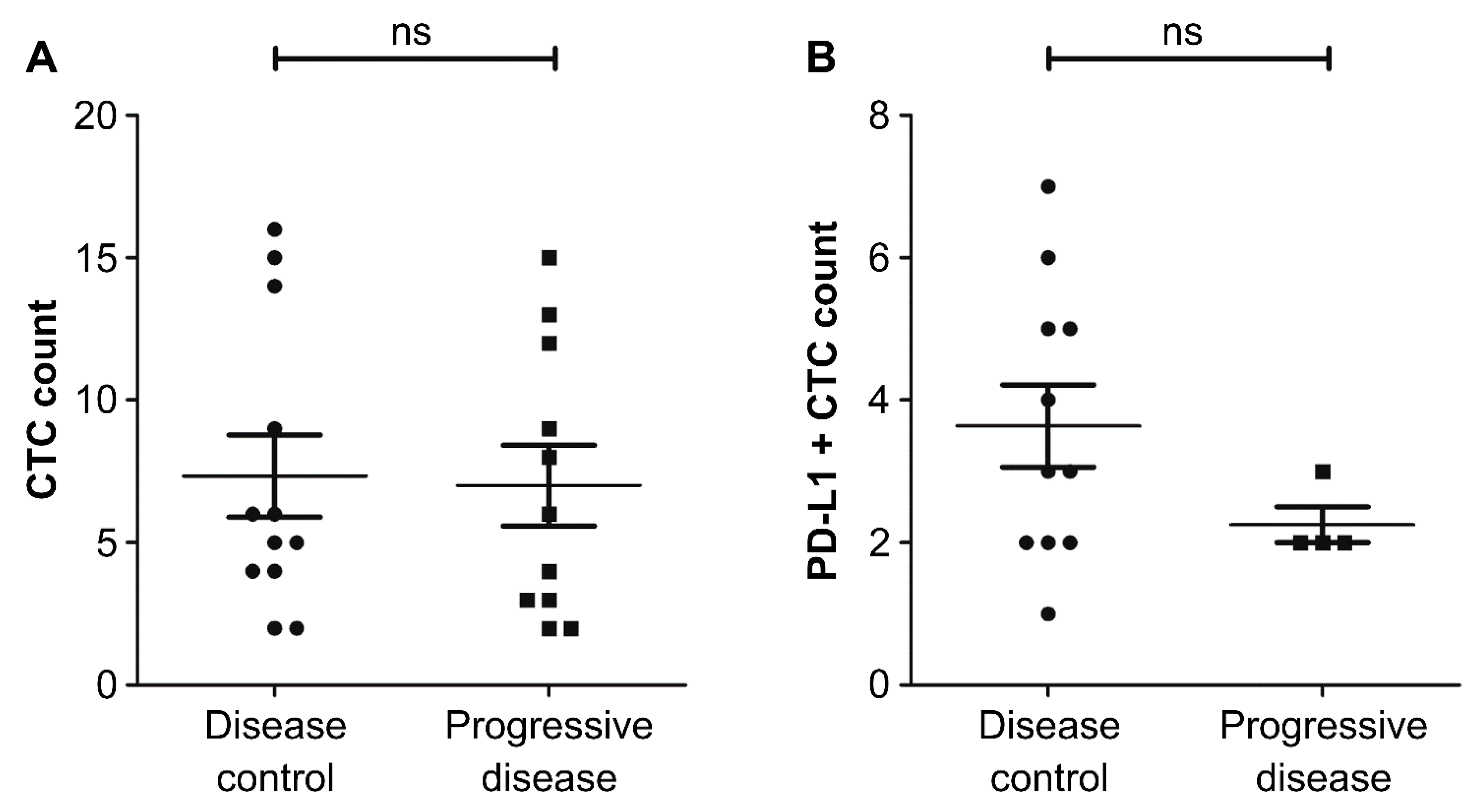
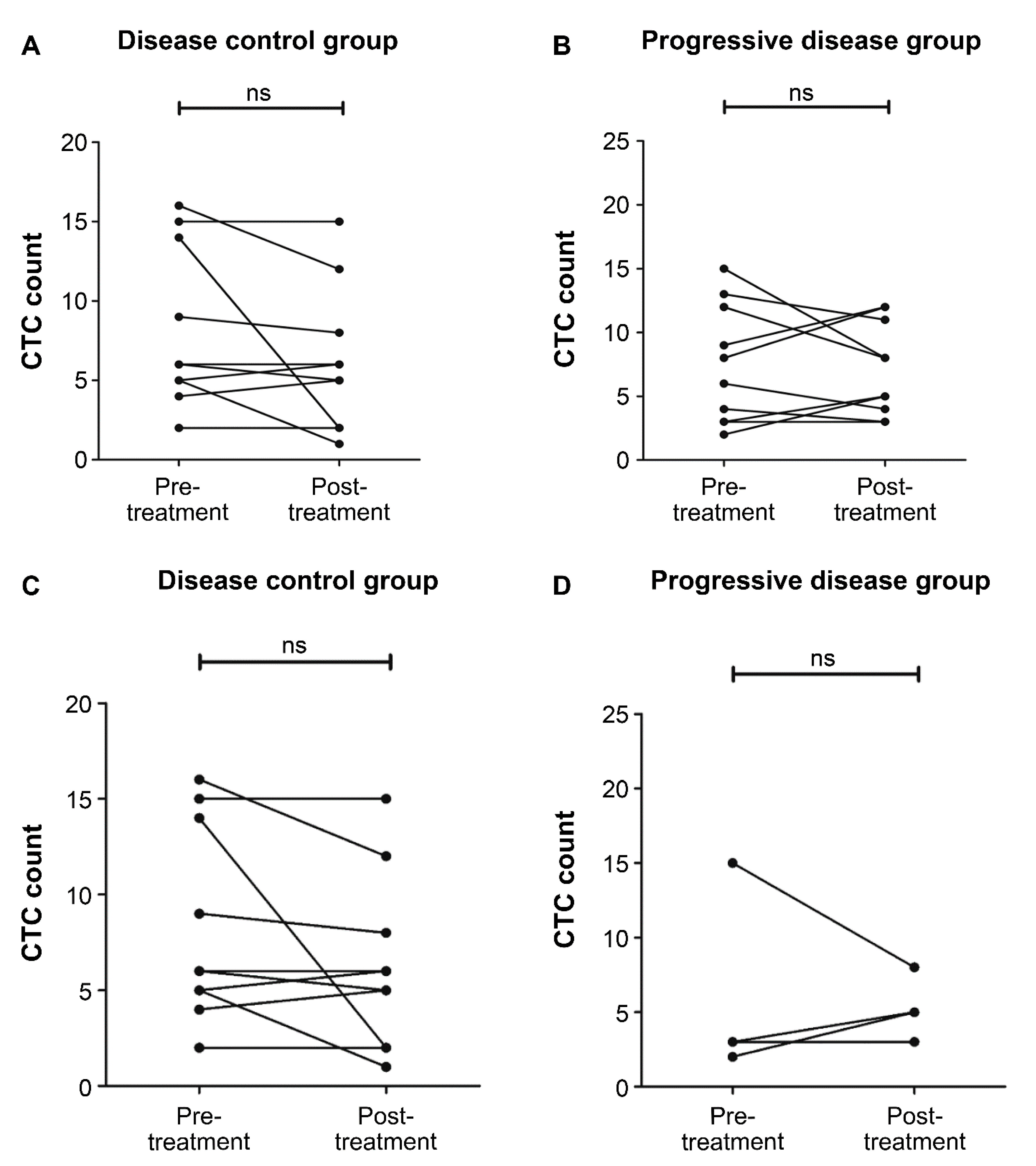
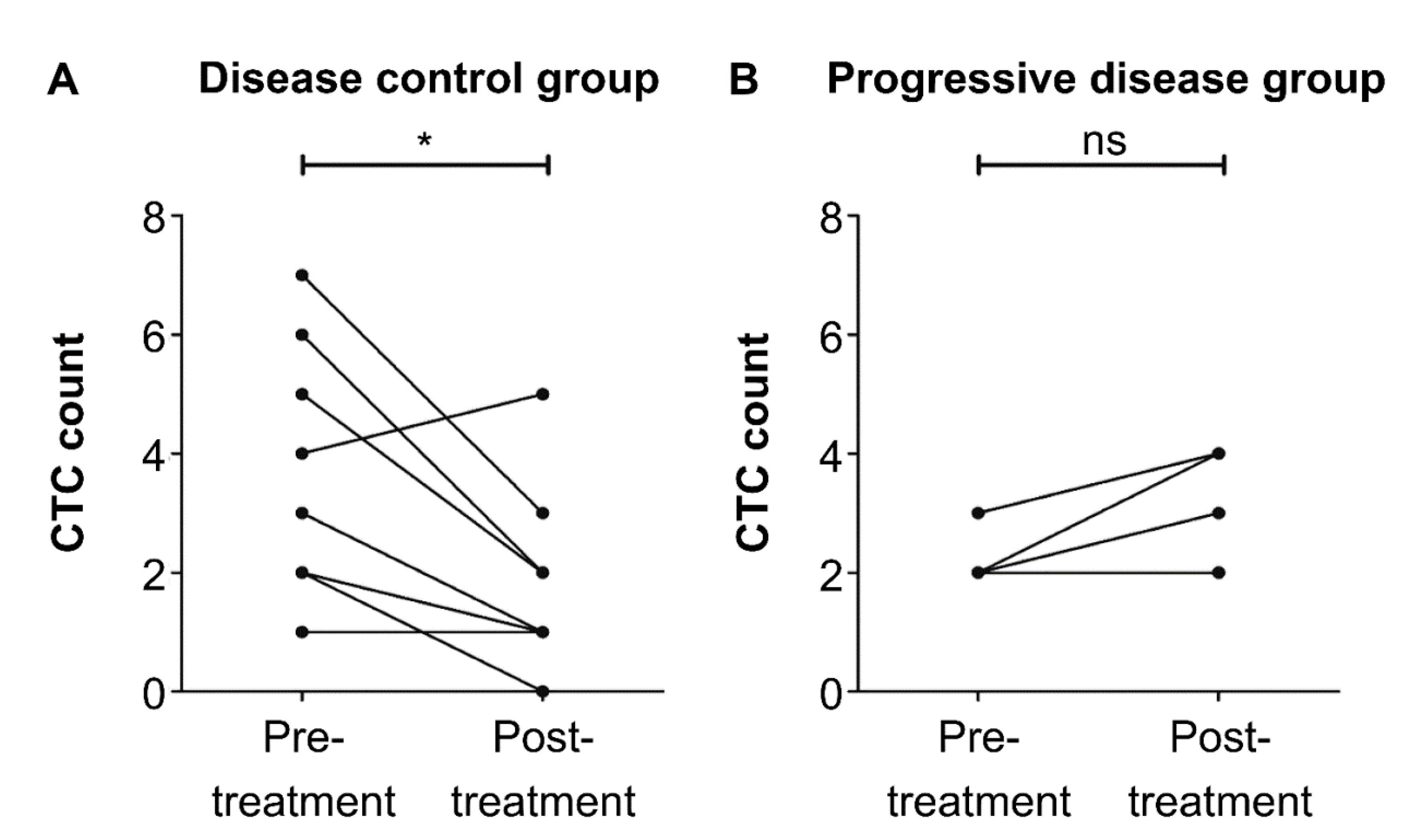
3.2. Detection of PD-L1-Positive CTCs and Its Related Clinical Outcomes
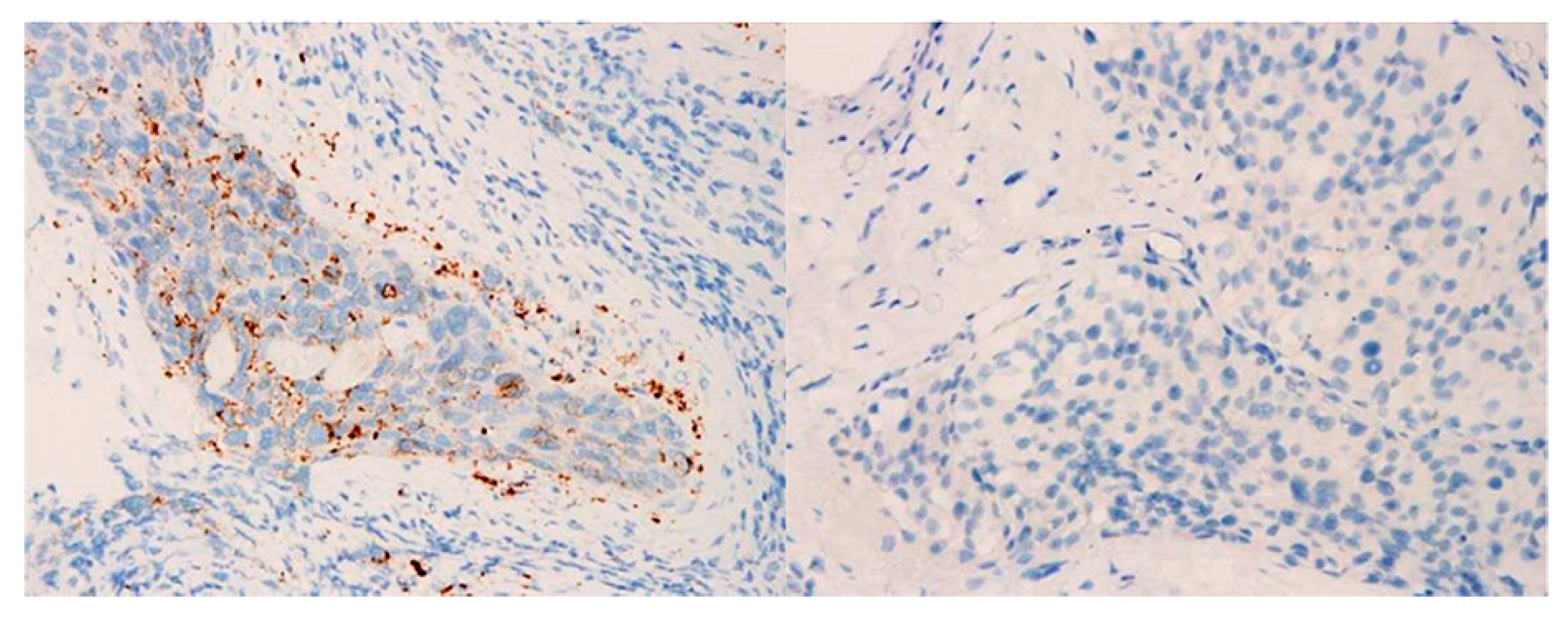
3.3. Comparison of PD-L1 Expression in CTCs and Tumor Biopsies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Darvin, P.; Toor, S.M.; Nair, V.S.; Elkord, E. Immune checkpoint inhibitors: Recent progress and potential biomarkers. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gevaert, T.; Cimadamore, A.; Eckstein, M.; Scarpelli, M.; Lopez-Beltran, A.; Cheng, L.; Montironi, R. Predictive biomarkers for immunotherapy in the treatment of advanced urothelial carcinoma: Where we stand and where we go. Future Oncol. 2019, 15, 2199–2202. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Armstrong, A.J.; Friedlander, T.W.; Kim, W.; Pal, S.K.; George, D.J.; Zhang, T. Biomarkers of immunotherapy in urothelial and renal cell carcinoma: PD-L1, tumor mutational burden, and beyond. J. Immunother. Cancer 2018, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendiratta, P.; Grivas, P. Emerging biomarkers and targeted therapies in urothelial carcinoma. Ann. Transl. Med. 2018, 6, 250. [Google Scholar] [CrossRef] [PubMed]
- Niegisch, G. Predicting immune checkpoint inhibitor response in urothelial carcinoma: Another step in personalised medicine? Br. J. Cancer 2020, 122, 453–454. [Google Scholar] [CrossRef] [Green Version]
- Eckstein, M.; Cimadamore, A.; Hartmann, A.; Lopez-Beltran, A.; Cheng, L.; Scarpelli, M.; Montironi, R.; Gevaert, T. PD-L1 assessment in urothelial carcinoma: A practical approach. Ann. Transl. Med. 2019, 7, 690. [Google Scholar] [CrossRef]
- Alix-Panabieres, C.; Pantel, K. Characterization of single circulating tumor cells. FEBS Lett. 2017, 591, 2241–2250. [Google Scholar] [CrossRef] [Green Version]
- Msaouel, P.; Koutsilieris, M. Diagnostic value of circulating tumor cell detection in bladder and urothelial cancer: Systematic review and meta-analysis. BMC Cancer 2011, 11, 336. [Google Scholar] [CrossRef] [Green Version]
- Naoe, M.; Ohta, M.; Hasebe, Y.; Matsui, Y.; Unoki, T.; Shimoyama, H.; Nakasato, T.; Ogawa, Y.; Tsukada, M.; Sunagawa, M.; et al. Detection of circulating tumor cells and the importance of their measurement in urological cancers. Urol. Sci. 2018, 29, 4. [Google Scholar] [CrossRef]
- Nicolazzo, C.; Raimondi, C.; Mancini, M.L.; Caponnetto, S.; Gradilone, A.; Gandini, O.; Mastromartino, M.; Del Bene, G.; Prete, A.; Longo, F.; et al. Monitoring PD-L1 positive circulating tumor cells in non-small cell lung cancer patients treated with the PD-1 inhibitor Nivolumab. Sci. Rep. 2016, 6, 31726. [Google Scholar] [CrossRef] [PubMed]
- Kulasinghe, A.; Perry, C.; Kenny, L.; Warkiani, M.E.; Nelson, C.; Punyadeera, C. PD-L1 expressing circulating tumour cells in head and neck cancers. BMC Cancer 2017, 17, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anantharaman, A.; Friedlander, T.; Lu, D.; Krupa, R.; Premasekharan, G.; Hough, J.; Edwards, M.; Paz, R.; Lindquist, K.; Graf, R.; et al. Programmed death-ligand 1 (PD-L1) characterization of circulating tumor cells (CTCs) in muscle invasive and metastatic bladder cancer patients. BMC Cancer 2016, 16, 744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbe, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the evaluation of immune therapy activity in solid tumors: Immune-related response criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Zhang, Q.; Shuman, L.; Kaag, M.; Raman, J.D.; Merrill, S.; DeGraff, D.J.; Warrick, J.I.; Chen, G. Evaluation of PD-L1 and other immune markers in bladder urothelial carcinoma stratified by histologic variants and molecular subtypes. Sci. Rep. 2020, 10, 1439. [Google Scholar] [CrossRef]
- Warrick, J.I.; Sjodahl, G.; Kaag, M.; Raman, J.D.; Merrill, S.; Shuman, L.; Chen, G.; Walter, V.; DeGraff, D.J. Intratumoral heterogeneity of bladder cancer by molecular subtypes and histologic variants. Eur. Urol. 2019, 75, 18–22. [Google Scholar] [CrossRef]
- Pantel, K.; Hille, C.; Scher, H.I. Circulating tumor cells in prostate cancer: From discovery to clinical utility. Clin. Chem. 2019, 65, 87–99. [Google Scholar] [CrossRef] [Green Version]
- Pantel, K.; Alix-Panabieres, C. Circulating tumour cells in cancer patients: Challenges and perspectives. Trends Mol. Med. 2010, 16, 398–406. [Google Scholar] [CrossRef]
- Pantel, K.; Alix-Panabieres, C. The clinical significance of circulating tumor cells. Nat. Clin. Pract. Oncol. 2007, 4, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Aoki, M.; Shoji, H.; Kashiro, A.; Takeuchi, K.; Shimizu, Y.; Honda, K. Prospects for comprehensive analyses of circulating tumor cells in tumor biology. Cancers 2020, 12, 1135. [Google Scholar] [CrossRef]
- Chen, S.; El-Heliebi, A.; Kroneis, T. Biological and molecular characterization of circulating tumor cells: A creative strategy for precision medicine? Adv. Clin. Chem. 2017, 82, 71–103. [Google Scholar] [PubMed]
- Lim, S.B.; Yeo, T.; Di Lee, W.; Bhagat, A.A.S.; Tan, S.J.; Tan, D.S.W.; Lim, W.-T.; Lim, C.T. Addressing cellular heterogeneity in tumor and circulation for refined prognostication. Proc. Natl. Acad. Sci. USA 2019, 116, 17957–17962. [Google Scholar] [CrossRef] [Green Version]
- Onstenk, W.; Gratama, J.W.; Foekens, J.A.; Sleijfer, S. Towards a personalized breast cancer treatment approach guided by circulating tumor cell (CTC) characteristics. Cancer Treat. Rev. 2013, 39, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.L.; Zhang, P.; Li, H.-C.; Yang, X.-J.; Zhang, Y.-P.; Li, Z.-L.; Xue, L.; Xue, Y.-Q.; Li, H.-L.; Chen, Q.; et al. Dynamic changes of different phenotypic and genetic circulating tumor cells as a biomarker for evaluating the prognosis of RCC. Cancer Biol. Ther. 2019, 20, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Cappelletti, V.; Verzoni, E.; Ratta, R.; Vismara, M.; Silvestri, M.; Montone, R.; Miodini, P.; Reduzzi, C.; Claps, M.; Sepe, P.; et al. Analysis of single circulating tumor cells in renal cell carcinoma reveals phenotypic heterogeneity and genomic alterations related to progression. Int. J. Mol. Sci. 2020, 21, 1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.J.; Kakehi, Y.; Takahashi, T.; Wu, X.X.; Yuasa, T.; Yoshiki, T.; Okada, Y.; Terachi, T.; Ogawa, O. Detection of circulating cancer cells by reverse transcription-polymerase chain reaction for uroplakin II in peripheral blood of patients with urothelial cancer. Clin. Cancer. Res. 2000, 6, 3166–3171. [Google Scholar]
- Flaig, T.W.; Wilson, S.; van Bokhoven, A.; Varella-Garcia, M.; Wolfe, P.; Maroni, P.; Genova, E.E.; Morales, D.; Lucia, M.S. Detection of circulating tumor cells in metastatic and clinically localized urothelial carcinoma. Urology 2011, 78, 863–867. [Google Scholar] [CrossRef] [Green Version]
- Naoe, M.; Ogawa, Y.; Morita, J.; Omori, K.; Takeshita, K.; Shichijyo, T.; Okumura, T.; Igarashi, A.; Yanaihara, A.; Iwamoto, S.; et al. Detection of circulating urothelial cancer cells in the blood using the CellSearch System. Cancer 2007, 109, 1439–1445. [Google Scholar] [CrossRef]
- de Wit, S.; van Dalum, G.; Lenferink, A.T.M.; Tibbe, A.G.J.; Hiltermann, T.J.N.; Groen, H.J.M.; van Rijn, C.J.M.; Terstappen, L.W.M.M. The detection of EpCAM(+) and EpCAM(-) circulating tumor cells. Sci. Rep. 2015, 5, 12270. [Google Scholar] [CrossRef] [Green Version]
- Alva, A.; Friedlander, T.; Clark, M.; Huebner, T.; Daignault, S.; Hussain, M.; Lee, C.; Hafez, K.; Hollenbeck, B.; Weizer, A.; et al. Circulating tumor cells as potential biomarkers in bladder cancer. J. Urol. 2015, 194, 790–798. [Google Scholar] [CrossRef]
- Goldkorn, A.; Tangen, C.; Plets, M.; Morrison, G.M.; Cunha, A.; Xu, T.; Pinski, J.K.; Ingles, S.A.; Triche, T.; Harzstark, A.L.; et al. Baseline circulating tumor cell (CTC) count as a prognostic marker of PSA response and progression in metastatic castrate sensitive prostate cancer (mCSPC): Results from SWOG S1216, a phase III randomized trial of androgen deprivation plus orteronel (cyp17 inhibitor) or bicalutamide. J. Clin. Oncol. 2020, 38, 5506. [Google Scholar]
- Coumans, F.A.; Ligthart, S.T.; Terstappen, L.W. Interpretation of changes in circulating tumor cell counts. Transl. Oncol. 2012, 5, 486–491. [Google Scholar] [CrossRef] [Green Version]
- Kloten, V.; Lampignano, R.; Krahn, T.; Schlange, T. Circulating tumor cell PD-L1 expression as biomarker for therapeutic efficacy of immune checkpoint inhibition in NSCLC. Cells 2019, 8, 809. [Google Scholar] [CrossRef] [Green Version]
- Janning, M.; Kobus, F.; Babayan, A.; Wikman, H.; Velthaus, J.-L.; Bergmann, S.; Schatz, S.; Falk, M.; Berger, L.-A.; Bottcher, L.-M.; et al. Determination of PD-L1 expression in circulating tumor cells of NSCLC patients and correlation with response to PD-1/PD-L1 inhibitors. Cancers 2019, 11, 835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strati, A.; Kousodontis, G.; Papaxoinis, I.; Angelidis, I.; Zavridou, M.; Economopoulou, P.; Kotsantis, I.; Avgeris, M.; Mazel, M.; Perisanidis, C.; et al. Prognostic significance of PD-L1 expression on circulating tumor cells in patients with head and neck squamous cell carcinoma. Ann. Oncol. 2017, 28, 1923–1933. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, M.A.; Koutsopoulos, A.V.; Tsoulfas, P.G.; Lagoudaki, E.; Aggouraki, D.; Monastirioti, A.; Koutoulaki, C.; Apostolopoulou, C.A.; Merodoulaki, A.C.; Papadaki, C.; et al. Clinical relevance of immune checkpoints on circulating tumor cells in breast cancer. Cancers 2020, 12, 376. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.H.; Imrali, A.; Heeschen, C. Circulating cancer stem cells: The importance to select. Chin. J. Cancer Res. 2015, 27, 437–449. [Google Scholar] [PubMed]
- Jacot, W.; Mazel, M.; Mollevi, C.; Pouderoux, S.; D’Hondt, V.; Cayrefourcq, L.; Bourgier, C.; Boissiere-Michot, F.; Berrabah, F.; Lopez-Crapez, E.; et al. Clinical correlations of programmed cell death ligand 1 status in liquid and standard biopsies in breast cancer. Clin. Chem. 2020, 66, 1093–1101. [Google Scholar] [CrossRef]
- Koh, Y.; Yagi, S.; Akamatsu, H.; Kanai, K.; Hayata, A.; Tokudome, N.; Akamatsu, K.; Higuchi, M.; Kanbara, H.; Nakanishi, M.; et al. Heterogeneous expression of programmed death receptor-ligand 1 on circulating tumor cells in patients with lung cancer. Clin. Lung Cancer 2019, 20, 270–277.e1. [Google Scholar] [CrossRef] [Green Version]
- Ghate, K.; Amir, E.; Kuksis, M.; Hernandez-Barajas, D.; Rodriguez-Romo, L.; Booth, C.M.; Vera-Badillo, F.E. PD-L1 expression and clinical outcomes in patients with advanced urothelial carcinoma treated with checkpoint inhibitors: A meta-analysis. Cancer Treat. Rev. 2019, 76, 51–56. [Google Scholar] [CrossRef]
- Wang, C.; Qiao, W.; Jiang, Y.; Zhu, M.; Shao, J.; Ren, P.; Liu, D.; Liet, W. Effect of sex on the efficacy of patients receiving immune checkpoint inhibitors in advanced non-small cell lung cancer. Cancer Med. 2019, 8, 4023–4031. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Cowley, L.A.; Liu, X.S. Sex differences in cancer immunotherapy efficacy, biomarkers, and therapeutic strategy. Molecules 2019, 24, 3214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Ju, Q.; Jia, K.; Yu, J.; Shi, H.; Wu, H.; Jiang, M. Correlation between sex and efficacy of immune checkpoint inhibitors (PD-1 and CTLA-4 inhibitors). Int. J. Cancer 2018, 143, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daste, A.; Domblides, C.; Gross-Goupil, M.; Chakiba, C.; Quivy, A.; Cochin, V.; de Mones, E.; Larmonier, N.; Soubeyran, P.; Ravaud, A. Immune checkpoint inhibitors and elderly people: A review. Eur. J. Cancer 2017, 82, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Wang, Q.; Tang, X.; Xu, R.; Zhang, L.; Chen, X.; Xue, Q.; Wang, Z.; Shi, R.; Wang, F.; et al. Correlation between patients’ age and cancer immunotherapy efficacy. Oncoimmunology 2019, 8, e1568810. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | No. of Patients | % | |
|---|---|---|---|
| Age | 59.7 ± 5.6 | 23 | 100 |
| Sex | |||
| Male | 11 | 48 | |
| Female | 12 | 52 | |
| Tumor location | |||
| Bladder | 12 | 52 | |
| Kidney | 6 | 26 | |
| Ureter | 5 | 22 | |
| Metastatic sites | |||
| Visceral | 11 | 48 | |
| Liver | 6 | 26 | |
| Lymph nodes | 5 | 22 | |
| Brain | 1 | 4 | |
| Follow-up duration (months) | 6.6 ± 2.2 |
| CTC Populations | No. of Patients | Pre-Treatment Count/7.5 mL (Mean ± SD) | Post-Treatment Count/7.5 mL (Mean ± SD) | p-Value |
|---|---|---|---|---|
| Total CTC count | 23 | 7.2 ± 4.8 | 6.3 ± 3.8 | 0.63 |
| PD-L1-positive CTC count | 15 (65%) | 3.3 ± 1.8 | 2.1 ± 1.4 | 0.06 |
| Overall Responses | No. of Patients | Pre-Treatment CTC Count/ 7.5 mL (Mean ± SD) | Post-Treatment CTC Count/ 7.5 mL (Mean ± SD) | p Value | Pre-Treatment PD-L1-Positive CTC Count/ 7.5 mL (Mean ± SD) | Post-Treatment PD-L1-Positive CTC Count/ 7.5 mL (Mean ± SD) | p Value |
|---|---|---|---|---|---|---|---|
| All Patients | |||||||
| Disease control, n (%) | 12 (52) | 7.3 ± 5.0 | 5.8 ± 4.2 | 0.22 | - | - | - |
| Progressive disease, n (%) | 11 (48) | 7.0 ± 4.7 | 6.9 ± 3.5 | 0.88 | - | - | - |
| Patients with PD-L1-Positive CTCs | |||||||
| Disease control, n (%) | 11 (73) | 7.6 ± 5.1 | 5.8 ± 4.4 | 0.14 | 3.6 ± 1.9 | 1.7 ± 1.3 | 0.01 |
| Progressive disease, n (%) | 4 (27) | 5.8 ± 6.2 | 5.3 ± 2.1 | 1.00 | 2.3 ± 0.5 | 3.3 ± 1.0 | 0.17 |
| Patients without PD-L1-Positive CTCs | |||||||
| Disease control, n (%) | 1 (12.5) | 4 | 5 | - | - | - | - |
| Progressive disease, n (%) | 7 (87.5) | 7.7 ± 4.0 | 7.9 ± 3.9 | 1.00 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, P.-J.; Xu, T.; Cha, T.-L.; Tsai, Y.-T.; Liu, S.-Y.; Wu, S.-T.; Meng, E.; Tsao, C.-W.; Kao, C.-C.; Chen, C.-L.; et al. Programmed Cell Death Ligand 1 Expression in Circulating Tumor Cells as a Predictor of Treatment Response in Patients with Urothelial Carcinoma. Biology 2021, 10, 674. https://doi.org/10.3390/biology10070674
Chiang P-J, Xu T, Cha T-L, Tsai Y-T, Liu S-Y, Wu S-T, Meng E, Tsao C-W, Kao C-C, Chen C-L, et al. Programmed Cell Death Ligand 1 Expression in Circulating Tumor Cells as a Predictor of Treatment Response in Patients with Urothelial Carcinoma. Biology. 2021; 10(7):674. https://doi.org/10.3390/biology10070674
Chicago/Turabian StyleChiang, Pei-Jhang, Ting Xu, Tai-Lung Cha, Yi-Ta Tsai, Shu-Yu Liu, Sheng-Tang Wu, En Meng, Chih-Wei Tsao, Chien-Chang Kao, Chin-Li Chen, and et al. 2021. "Programmed Cell Death Ligand 1 Expression in Circulating Tumor Cells as a Predictor of Treatment Response in Patients with Urothelial Carcinoma" Biology 10, no. 7: 674. https://doi.org/10.3390/biology10070674
APA StyleChiang, P.-J., Xu, T., Cha, T.-L., Tsai, Y.-T., Liu, S.-Y., Wu, S.-T., Meng, E., Tsao, C.-W., Kao, C.-C., Chen, C.-L., Sun, G.-H., Yu, D.-S., Chang, S.-Y., & Yang, M.-H. (2021). Programmed Cell Death Ligand 1 Expression in Circulating Tumor Cells as a Predictor of Treatment Response in Patients with Urothelial Carcinoma. Biology, 10(7), 674. https://doi.org/10.3390/biology10070674