

Surgical Antibiotic Prophylaxis: A Proposal for a Global Evidence-Based Bundle


 , , ,
, , ,  , , , , , , ,
, , , , , , ,  ,
,  ,
,  and
and 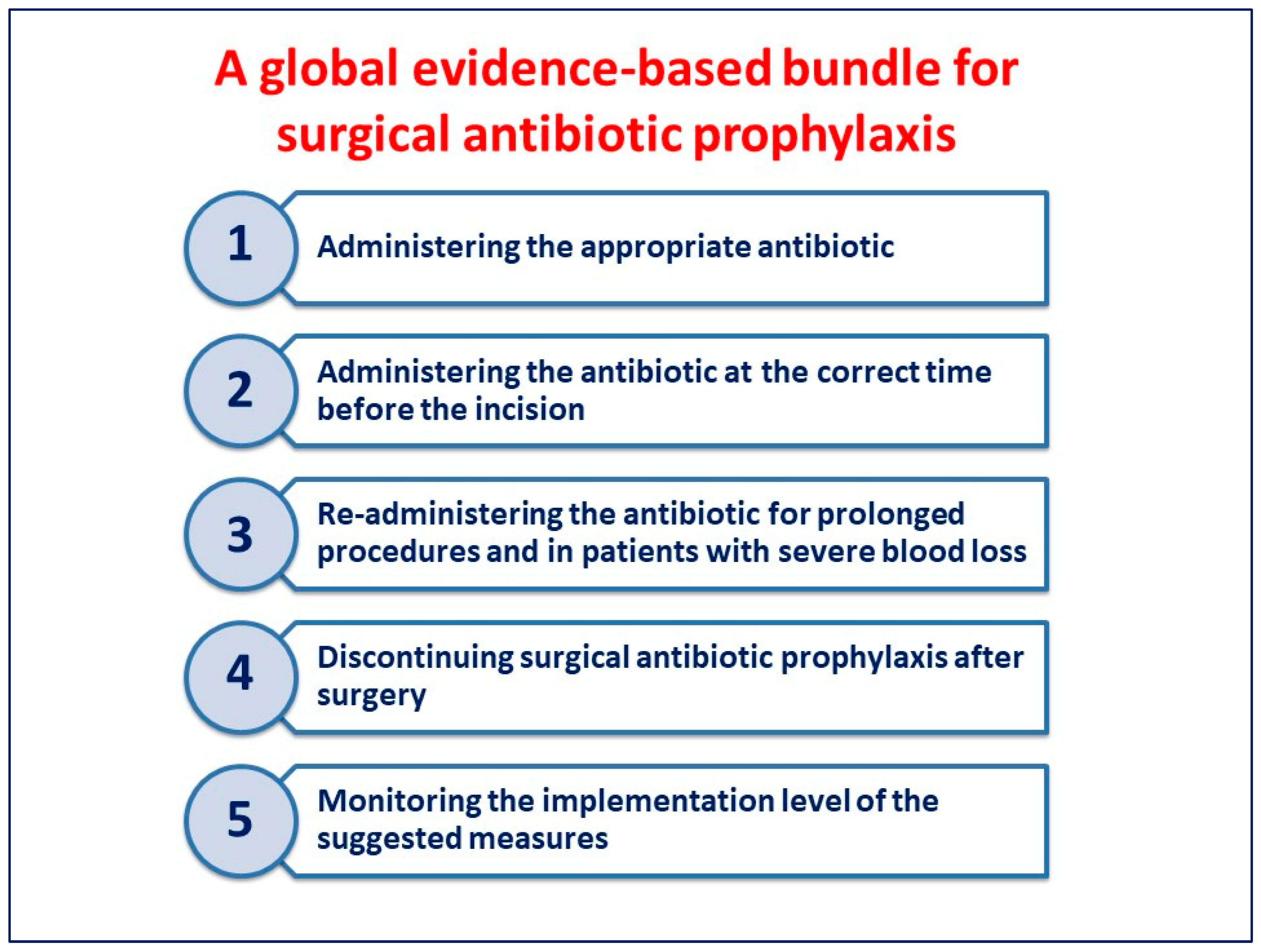{kind=link}
Abstract
1. Introduction
- Prevent SSIs;
- Reduce SSI morbidity and mortality;
- Diminish healthcare duration and cost;
- Not produce any adverse effects;
- Have no aftermath for the patient’s intestinal microbial flora or the healthcare facility.
- Active against the most likely bacteria that can contaminate the surgical field;
- Provided in an appropriate dosage and time that ensures adequate serum and tissue concentrations amid the whole operation;
- Safe;
- Administered for the shortest effective period, minimising adverse effects, opportunistic infections, antimicrobial resistance (AMR) development, and costs.
2. Methods
3. A Proposal for a Global Evidence-Based Bundle
3.1. Administering the Appropriate Antibiotic
3.2. Administering the Antibiotic at the Correct Time before the Incision
3.3. Re-Administering the Antibiotic for Prolonged Procedures and in Patients with Severe Blood Loss
3.4. Discontinuing SAP after Surgery
3.5. Monitoring the Implementation Level of the Suggested Measures
4. Discussion
- Tracking compliance with hospital care bundles and conducting qualitative research into reasons for non-compliance with bundles;
- Incorporating checklists and care bundles into the informed consent process to make them as transparent as possible;
- Developing surveillance methods with shared SSI definitions and indicators that can be reliably interpreted in clinical practice and that can promote a benchmarking analysis of anonymised individual surgeon SSI rates;
- Updating national and local guidelines as new evidence evolves;
- Recognising compliant surgery/operating theatre work teams;
- Incorporating checklists and care bundles;
- Planning effective communication strategies with healthcare providers.
- Administering the appropriate antibiotic. SAP should be prescribed for surgical procedures at high risk of SSIs, such as clean–contaminated and contaminated surgical procedures or for clean surgical procedures where SSIs, even if unlikely, may have devastating consequences, such as in procedures with prosthetic implants. SAP should also be prescribed in patients with medical conditions associated with a higher risk of SSI, such as immunocompromised patients. The most commonly used antibiotics for SAP are first- and second-generation cephalosporins, including cefazolin, cefuroxime, cefoxitin, or the combination of cefazolin plus metronidazole, when it is necessary to cover anaerobes such as in colorectal surgery. Patients known to be colonised or to have had past infection with MDR bacteria must be treated on a case-by-case basis, taking into account multiple considerations. Future well-designed clinical studies will assess the SAP effectiveness in patients colonised with MDR bacteria. Although topical antibiotic prescription remains common among surgeons, it should be discouraged.
- Administering the antibiotic at the correct time before the incision. Adequate tissue concentrations of antibiotics should be present at the surgical site throughout the surgical procedure. The first antibiotic dose should always be administered within 60 min before surgical incision for most commonly used antibiotics (including cefazolin). This can guarantee appropriate tissue concentrations during the surgical intervention. Only drugs with more extended half-lives, such as vancomycin, should be issued more than 60 min before the incision.
- Re-administering the antibiotic for prolonged procedures and in patients with severe blood loss. Intraoperative doses should be issued for procedures exceeding two antibiotic half-lives or for procedures associated with blood loss (more than 1.5 L). This can guarantee that the antibiotic concentration is maintained above the minimal inhibitory concentration at the surgical site throughout the procedure.
- Discontinuing SAP after surgery. SAP aims to prevent SSIs and should be administered and maintained at sufficiently high concentrations at the surgical site during the time that the incision is open. Erroneously, some surgeons believe that prolonging SAP after that the surgical incision has been closed can protect the patient from post-operative infections. On the contrary, SAP administration should not be prolonged after the operation completion to prevent SSIs.
- Monitoring the implementation level of the suggested measures. To improve compliance with prevention measures and ensure their long-term sustainability, frequent assessment of working practices and timely result feedback to stakeholders is crucial. As a multimodal strategy to implement HAI prevention, bundles are among the most commonly used methods to adapt guidelines in the local context and transfer best practices into routine clinical care. The proposed bundle contains a set of evidence-based interventions for SAP administration. It is easy to apply, promotes collaboration, and includes measures that can be adequately followed and evaluated in all hospitals worldwide. Major efforts should be made in all hospitals around the world to verify that the proposed measures are implemented in the context of a bundle strategy.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Suetens, C.; Latour, K.; Kärki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikäinen, O.; et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: Results from two European point prevalence surveys, 2016 to 2017. Euro Surveill. 2018, 23, 1800516. [Google Scholar] [CrossRef]
- Haque, M.; Sartelli, M.; McKimm, J.; Abu Bakar, M. Health care-associated infections—An overview. Infect. Drug Resist. 2018, 11, 2321–2333. [Google Scholar] [CrossRef]
- Schreiber, P.W.; Sax, H.; Wolfensberger, A.; Clack, L.; Kuster, S.P. The preventable proportion of healthcare-associated infections 2005–2016: Systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2018, 39, 1277–1295. [Google Scholar] [CrossRef]
- Badia, J.M.; Casey, A.L.; Petrosillo, N.; Hudson, P.M.; Mitchell, S.A.; Crosby, C. Impact of surgical site infection on healthcare costs and patient outcomes: A systematic review in six European countries. J. Hosp. Infect. 2017, 96, 1–15. [Google Scholar] [CrossRef]
- GlobalSurg Collaborative. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: A prospective, international, multicentre cohort study. Lancet Infect. Dis. 2018, 18, 516–525. [Google Scholar] [CrossRef]
- Ahmed, N.J.; Almalki, Z.S.; Alfaifi, A.A.; Alshehri, A.M.; Alahmari, A.K.; Elazab, E.; Almansour, A.; Haseeb, A.; Balaha, M.F.; Khan, A.H. Implementing an Antimicrobial Stewardship Programme to Improve Adherence to a Perioperative Prophylaxis Guideline. Healthcare 2022, 10, 464. [Google Scholar] [CrossRef]
- Allegranzi, B.; Zayed, B.; Bischoff, P.; Kubilay, N.Z.; de Jonge, S.; de Vries, F.; Gomes, S.M.; Gans, S.; Wallert, E.D.; Wu, X.; et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: An evidence-based global perspective. Lancet Infect. Dis. 2016, 16, e288–e303. [Google Scholar] [CrossRef]
- Allegranzi, B.; Bischoff, P.; de Jonge, S.; Kubilay, N.Z.; Zayed, B.; Gomes, S.M.; Abbas, M.; Atema, J.J.; Gans, S.; van Rijen, M.; et al. New WHO recommendations on preoperative measures for surgical site infection prevention: An evidence-based global perspective. Lancet Infect. Dis. 2016, 16, e276–e287. [Google Scholar] [CrossRef]
- Global Guidelines for the Prevention of Surgical Site Infection, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/handle/10665/277399 (accessed on 4 April 2023).
- Berríos-Torres, S.I.; Umscheid, C.A.; Bratzler, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for disease control and prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg. 2017, 152, 784–791. [Google Scholar] [CrossRef]
- Ban, K.A.; Minei, J.P.; Laronga, C.; Harbrecht, B.G.; Jensen, E.H.; Fry, D.E.; Itani, K.M.; Dellinger, E.P.; Ko, C.Y.; Duane, T.M. American College of Surgeons and Surgical Infection Society: Surgical site infection guidelines, 2016 update. J. Am. Coll. Surg. 2017, 224, 59–74. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Surgical Site Infections: Prevention and Treatment. NICE Guideline [NG125]. Available online: https://www.nice.org.uk/guidance/ng125 (accessed on 4 December 2023).
- Calderwood, M.S.; Anderson, D.J.; Bratzler, D.W.; Dellinger, E.P.; Garcia-Houchins, S.; Maragakis, L.L.; Nyquist, A.C.; Perkins, K.M.; Preas, M.A.; Saiman, L.; et al. Strategies to prevent surgical site infections in acute-care hospitals: 2022 Update. Infect. Control Hosp. Epidemiol. 2023, 44, 695–720. [Google Scholar] [CrossRef]
- Worldwide Antimicrobial Resistance National/International Network Group (WARNING) Collaborators. Ten golden rules for optimal antibiotic use in hospital settings: The WARNING call to action. World J. Emerg. Surg. 2023, 18, 50. [Google Scholar] [CrossRef]
- Sartelli, M.; Duane, T.M.; Catena, F.; Tessier, J.M.; Coccolini, F.; Kao, L.S.; De Simone, B.; Labricciosa, F.M.; May, A.K.; Ansaloni, L.; et al. Antimicrobial Stewardship: A Call to Action for Surgeons. Surg. Infect. 2016, 17, 625–631. [Google Scholar] [CrossRef]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg. Infect. 2013, 14, 73–156. [Google Scholar] [CrossRef]
- Pereira, L.B.; Feliciano, C.S.; Siqueira, D.S.; Bellissimo-Rodrigues, F.; Pereira, L.R.L. Surgical antibiotic prophylaxis: Is the clinical practice based on evidence? Einstein 2020, 18, eAO5427. [Google Scholar] [CrossRef]
- Schmitt, C.; Lacerda, R.A.; Turrini, R.N.T.; Padoveze, M.C. Improving compliance with surgical antibiotic prophylaxis guidelines: A multicenter evaluation. Am. J. Infect. Control 2017, 45, 1111–1115. [Google Scholar] [CrossRef]
- Bull, A.L.; Worth, L.J.; Spelman, T.; Richards, M.J. Antibiotic prescribing practices for prevention of surgical site infections in Australia: Increased uptake of national guidelines after surveillance and reporting and impact on infection rates. Surg. Infect. 2017, 18, 834–840. [Google Scholar] [CrossRef]
- Mousavi, S.; Zamani, E.; Bahrami, F. An audit of perioperative antimicrobial prophylaxis: Compliance with the international guidelines. J. Res. Pharm. Pract. 2017, 6, 126–129. [Google Scholar] [CrossRef]
- Ou, Y.; Jing, B.Q.; Guo, F.F.; Zhao, L.; Xie, Q.; Fang, Y.L.; Cui, J.; Xiao, W.; Wu, D.W.; Zhou, W. Audits of the quality of perioperative antibiotic prophylaxis in Shandong Province, China, 2006 to 2011. Am. J. Infect. Control 2014, 42, 516–520. [Google Scholar] [CrossRef]
- Nabor, M.I.P.; Buckley, B.S.; Lapitan, M.C.M. Compliance with international guidelines on antibiotic prophylaxis for elective surgeries at a tertiary-level hospital in the Philippines. Healthc. Infect. 2015, 20, 145–151. [Google Scholar] [CrossRef]
- Ierano, C.; Thursky, K.; Marshall, C.; Koning, S.; James, R.; Johnson, S.; Imam, N.; Worth, L.J.; Peel, T. Appropriateness of Surgical Antimicrobial Prophylaxis Practices in Australia. JAMA Netw. Open. 2019, 2, e1915003. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 7th ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Storr, J.; Tyman, A.; Zingg, W.; Damani, N.; Kilpatrick, C.; Reilly, J.; Price, L.; Egger, M.; Grayson, M.L.; Kelley, E.; et al. WHO Guidelines Development Group. Core components for effective infection prevention and control programmes: New WHO evidence-based recommendations. Antimicrob. Resist. Infect. Control 2017, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J.; Padley, W.; Assadian, O.; Leaper, D.; Kiernan, M.; Edmiston, C. Do surgical care bundles reduce the risk of surgical site infections in patients undergoing colorectal surgery? A systematic review and cohort meta-analysis of 8515 patients. Surgery 2015, 158, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Zywot, A.; Lau, C.S.M.; Stephen Fletcher, H.; Paul, S. Bundles Prevent Surgical Site Infections After Colorectal Surgery: Meta-analysis and Systematic Review. J. Gastrointest. Surg. 2017, 21, 1915–1930. [Google Scholar] [CrossRef]
- Pop-Vicas, A.E.; Abad, C.; Baubie, K.; Osman, F.; Heise, C.; Safdar, N. Colorectal bundles for surgical site infection prevention: A systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2020, 41, 805–812. [Google Scholar] [CrossRef]
- Sartelli, M.; Boermeester, M.A.; Cainzos, M.; Coccolini, F.; de Jonge, S.W.; Rasa, K.; Dellinger, E.P.; McNamara, D.A.; Fry, D.E.; Cui, Y.; et al. Six Long-Standing Questions about Antibiotic Prophylaxis in Surgery. Antibiotics 2023, 12, 908. [Google Scholar] [CrossRef]
- Yin, Y.; Song, T.; Liao, B.; Luo, Q.; Zhou, Z. Antibiotic prophylaxis in patients undergoing open mesh repair of inguinal hernia: A meta-analysis. Am. Surg. 2012, 78, 359–365. [Google Scholar] [CrossRef]
- Al Riyees, L.; Al Madani, W.; Firwana, N.; Balkhy, H.H.; Ferwana, M.; Alkhudhayri, A. Antibiotic prophylaxis against surgical site infection after open hernia surgery: A systematic review and meta-analysis. Eur. Surg. Res. 2021, 62, 121–133. [Google Scholar] [CrossRef]
- Erdas, E.; Medas, F.; Pisano, G.; Nicolosi, A.; Calò, P.G. Antibiotic prophylaxis for open mesh repair of groin hernia: Systematic review and meta-analysis. Hernia 2016, 20, 765–776. [Google Scholar] [CrossRef]
- Orelio, C.C.; van Hessen, C.; Sanchez-Manuel, F.J.; Aufenacker, T.J.; Scholten, R.J. Antibiotic prophylaxis for prevention of postoperative wound infection in adults undergoing open elective inguinal or femoral hernia repair. Cochrane Database Syst. Rev. 2020, 4, CD003769. [Google Scholar]
- Mazaki, T.; Mado, K.; Masuda, H.; Shiono, M. Antibiotic prophylaxis for the prevention of surgical site infection after tension-free hernia repair: A Bayesian and frequentist meta-analysis. J. Am. Coll. Surg. 2013, 217, 788–801.e1-4. [Google Scholar] [CrossRef] [PubMed]
- Boonchan, T.; Wilasrusmee, C.; McEvoy, M.; Attia, J.; Thakkinstian, A. Network meta-analysis of antibiotic prophylaxis for prevention of surgical-site infection after groin hernia surgery. Br. J. Surg. 2017, 104, e106. [Google Scholar] [CrossRef]
- HerniaSurge Group. International guidelines for groin hernia management. Hernia 2018, 22, 1–165. [Google Scholar] [CrossRef]
- Sarkut, P.; Kilicturgay, S.; Aktas, H.; Ozen, Y.; Kaya, E. Routine use of prophylactic antibiotics during laparoscopic cholecystectomy does not reduce the risk of surgical site infections. Surg. Infect. 2017, 18, 603–609. [Google Scholar] [CrossRef]
- Passos, M.A.; Portari-Filho, P.E. Antibiotic prophylaxis in laparoscopic cholecistectomy: Is it worth doing? Arq. Bras. Cir. Dig. 2016, 29, 170–172. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vohra, R.S.; Hodson, J.; Pasquali, S.; Griffiths, E.A.; Chole, S.S.G.; West Midlands Research Collaborative. Effectiveness of antibiotic prophylaxis in non-emergency cholecystectomy using data from a population-based cohort study. World J. Surg. 2017, 41, 2231–2239. [Google Scholar] [CrossRef] [PubMed]
- Jaafar, G.; Sandblom, G.; Lundell, L.; Hammarqvist, F. Antibiotic prophylaxis in acute cholecystectomy revisited: Results of a double-blind randomised controlled trial. Langenbecks Arch. Surg. 2020, 405, 1201–1207. [Google Scholar] [CrossRef]
- Murri, R.; De Belvis, A.G.; Fantoni, M.; Tanzariello, M.; Parente, P.; Marventano, S.; Bucci, S.; Giovannenze, F.; Ricciardi, W.; Cauda, R.; et al. Impact of antibiotic stewardship on perioperative antimicrobial prophylaxis. Int. J. Qual. Health Care 2016, 28, 502–507. [Google Scholar] [CrossRef]
- Koizumi, R.; Kusama, Y.; Asai, Y.; Yoshiaki, G.; Muraki, Y.; Ohmagari, N. Effects of the cefazolin shortage on the sales, cost, and appropriate use of other antimicrobials. BMC Health Serv. Res. 2021, 21, 1118. [Google Scholar] [CrossRef]
- Abubakar, U.; Salman, M. Antibiotic Use Among Hospitalized Patients in Africa: A Systematic Review of Point Prevalence Studies. J. Racial Ethn. Health Disparities 2023, 1–22. [Google Scholar] [CrossRef]
- D’Angelica, M.I.; Ellis, R.J.; Liu, J.B.; Brajcich, B.C.; Gönen, M.; Thompson, V.M.; Cohen, M.E.; Seo, S.K.; Zabor, E.C.; Babicky, M.L.; et al. Piperacillin-Tazobactam Compared with Cefoxitin as Antimicrobial Prophylaxis for Pancreatoduodenectomy: A Randomized Clinical Trial. JAMA 2023, 329, 1579–1588. [Google Scholar] [CrossRef]
- Liu, Y.; Lan, C.; Qin, S.; Qin, Z.; Zhang, Z.; Zhang, P.; Cao, W. Efficacy of anti-fungal agents for invasive fungal infection prophylaxis in liver transplant recipients: A network meta-analysis. Mycoses 2022, 65, 906–917. [Google Scholar] [CrossRef] [PubMed]
- Righi, E.; Mutters, N.T.; Guirao, X.; Del Toro, M.D.; Eckmann, C.; Friedrich, A.W.; Giannella, M.; Kluytmans, J.; Presterl, E.; Christaki, E.; et al. ESCMID/EUCIC clinical practice guidelines on perioperative antibiotic prophylaxis in patients colonized by multidrug-resistant Gram-negative bacteria before surgery. Clin. Microbiol. Infect. 2023, 29, 463–479. [Google Scholar] [CrossRef]
- Blum, S.; Cunha, C.B.; Cunha, B.A. Lack of pharmacokinetic basis of weight-based dosing and intra-operative re-dosing with cefazolin surgical prophylaxis in obese patients: Implications for antibiotic stewardship. Surg. Infect. 2019, 20, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Ho, V.P.; Nicolau, D.P.; Dakin, G.F.; Pomp, A.; Rich, B.S.; Towe, C.W.; Barie, P.S. Cefazolin dosing for surgical prophylaxis in morbidly obese patients. Surg. Infect. 2012, 13, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Šantavý, P.; Šíma, M.; Zuščich, O.; Kubíčková, V.; Michaličková, D.; Slanař, O.; Urbánek, K. Population Pharmacokinetics of Prophylactic Cefazolin in Cardiac Surgery with Standard and Minimally Invasive Extracorporeal Circulation. Antibiotics 2022, 11, 1582. [Google Scholar] [CrossRef]
- Almeida, R.A.; Hasimoto, C.N.; Kim, A.; Hasimoto, E.N.; El Dib, R. Antibiotic prophylaxis for surgical site infection in people undergoing liver transplantation. Cochrane Database Syst. Rev. 2015, 2015, CD010164. [Google Scholar] [CrossRef]
- Coccolini, F.; Improta, M.; Cicuttin, E.; Catena, F.; Sartelli, M.; Bova, R.; De’ Angelis, N.; Gitto, S.; Tartaglia, D.; Cremonini, C.; et al. Surgical site infection prevention and management in immunocompromised patients: A systematic review of the literature. World J. Emerg. Surg. 2021, 16, 33. [Google Scholar] [CrossRef]
- Graziano, E.; Peghin, M.; Grossi, P.A. Perioperative antibiotic stewardship in the organ transplant setting. Transpl. Infect. Dis. 2022, 24, e13895. [Google Scholar] [CrossRef]
- Bertram, C.M.; Postelnick, M.; Mancini, C.M.; Fu, X.; Zhang, Y.; Schulz, L.T.; Bhowmick, T.; Lee, F.; Blumenthal, K.G. Association of β-Lactam Allergy Documentation and Prophylactic Antibiotic Use in Surgery: A National Cross-Sectional Study of Hospitalized Patients. Clin. Infect. Dis. 2021, 72, e872–e875. [Google Scholar] [CrossRef]
- Chen, P.J.; Hua, Y.M.; Toh, H.S.; Lee, M.C. Topical antibiotic prophylaxis for surgical wound infections in clean and clean-contaminated surgery: A systematic review and meta-analysis. BJS Open 2021, 5, zrab125. [Google Scholar] [CrossRef]
- Willis, M.A.; Toews, I.; Soltau, S.L.; Kalff, J.C.; Meerpohl, J.J.; Vilz, T.O. Preoperative combined mechanical and oral antibiotic bowel preparation for preventing complications in elective colorectal surgery. Cochrane Database Syst. Rev. 2023, 2, CD014909. [Google Scholar] [PubMed]
- de Jonge, S.W.; Gans, S.L.; Atema, J.J.; Solomkin, J.S.; Dellinger, P.E.; Boermeester, M.A. Timing of preoperative antibiotic prophylaxis in 54,552 patients and the risk of surgical site infection: A systematic review and meta-analysis. Medicine 2017, 96, e6903. [Google Scholar] [CrossRef] [PubMed]
- Weber, W.P.; Mujagic, E.; Zwahlen, M.; Bundi, M.; Hoffmann, H.; Soysal, S.D.; Kraljević, M.; Delko, T.; von Strauss, M.; Iselin, L.; et al. Timing of surgical antimicrobial prophylaxis: A phase 3 randomised controlled trial. Lancet Infect. Dis. 2017, 17, 605–614. [Google Scholar] [CrossRef]
- Baseel, D.; Kim, J.; Mohammed, S.; Lowe, A.; Siddiqi, J. The Ideal Time to Administer Pre-operative Antibiotics: Current and Future Practices. Cureus 2022, 14, e24979. [Google Scholar] [CrossRef]
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Global-PPS Network. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: Results of an internet-based global point prevalence survey. Lancet Glob. Health 2018, 6, e619–e629. [Google Scholar] [CrossRef] [PubMed]
- Wolfhagen, N.; Boldingh, Q.J.J.; de Lange, M.; Boermeester, M.A.; de Jonge, S.W. Intraoperative redosing of surgical antibiotic prophylaxis in addition to preoperative prophylaxis versus single-dose prophylaxis for the prevention of surgical site infection: A meta-analysis and GRADE recommendation. Ann. Surg. 2022, 275, 1050–1057. [Google Scholar] [CrossRef]
- de Jonge, S.W.; Boldingh, Q.J.J.; Solomkin, J.S.; Dellinger, E.P.; Egger, M.; Salanti, G.; Allegranzi, B.; Boermeester, M.A. Effect of postoperative continuation of antibiotic prophylaxis on the incidence of surgical site infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2020, 20, 1182–1192. [Google Scholar] [CrossRef]
- Christensen, D.D.; Moschetti, W.E.; Brown, M.G.; Lucas, A.P.; Jevsevar, D.S.; Fillingham, Y.A.; Dartmouth Hitchcock Medical Center. Perioperative Antibiotic Prophylaxis: Single and 24-Hour Antibiotic Dosages are Equally Effective at Preventing Periprosthetic Joint Infection in Total Joint Arthroplasty. J. Arthroplast. 2021, 36, S308–S313. [Google Scholar] [CrossRef]
- Branch-Elliman, W.; O’Brien, W.; Strymish, J.; Itani, K.; Wyatt, C.; Gupta, K. Association of duration and type of surgical prophylaxis with antimicrobial-associated adverse events. JAMA Surg. 2019, 154, 590–598. [Google Scholar] [CrossRef]
- Borgert, M.J.; Goossens, A.; Dongelmans, D.A. What are effective strategies for the implementation of care bundles on ICUs: A systematic review. Implement. Sci. 2015, 10, 119. [Google Scholar] [CrossRef]
- Surveillance of Surgical Site Infections and Prevention Indicators in European Hospitals HAI-Net SSI Protocol, Version 2.2. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/HAI-Net-SSI-protocol-v2.2.pdf (accessed on 4 December 2023).
- Gilhooly, D.; Green, S.A.; McCann, C.; Black, N.; Moonesinghe, S.R. Barriers and facilitators to the successful development, implementation and evaluation of care bundles in acute care in hospital: A scoping review. Implement. Sci. 2019, 14, 47. [Google Scholar] [CrossRef]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Sobalvarro, J.V.; Júnior, A.A.P.; Pereira, L.B.; Baldoni, A.O.; Ceron, C.S.; Dos Reis, T.M. Antimicrobial stewardship for surgical antibiotic prophylaxis and surgical site infections: A systematic review. Int. J. Clin. Pharm. 2022, 44, 301–319. [Google Scholar] [CrossRef]
- Tiri, B.; Bruzzone, P.; Priante, G.; Sensi, E.; Costantini, M.; Vernelli, C.; Martella, L.A.; Francucci, M.; Andreani, P.; Mariottini, A.; et al. Impact of Antimicrobial Stewardship Interventions on Appropriateness of Surgical Antibiotic Prophylaxis: How to Improve. Antibiotics 2020, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Madriz, J.P.; Zavaleta-Monestel, E.; Villalobos-Madriz, J.A.; Rojas-Chinchilla, C.; Castrillo-Portillo, P.; Meléndez-Alfaro, A.; Vásquez-Mendoza, A.F.; Muñoz-Gutiérrez, G.; Arguedas-Chacón, S. Impact of the Five-Year Intervention of an Antimicrobial Stewardship Program on the Optimal Selection of Surgical Prophylaxis in a Hospital without Antibiotic Prescription Restrictions in Costa Rica: A Retrospective Study. Antibiotics 2023, 12, 1572. [Google Scholar] [CrossRef] [PubMed]
- Tomsic, I.; Heinze, N.R.; Chaberny, I.F.; Krauth, C.; Schock, B.; von Lengerke, T. Implementation interventions in preventing surgical site infections in abdominal surgery: A systematic review. BMC Health Serv. Res. 2020, 20, 236. [Google Scholar] [CrossRef]
- Gouvêa, M.; Novaes Cde, O.; Pereira, D.M.; Iglesias, A.C. Adherence to guidelines for surgical antibiotic prophylaxis: A review. Braz. J. Infect. Dis. 2015, 19, 517–524. [Google Scholar] [CrossRef]
- Badge, H.M.; Churches, T.; Naylor, J.M.; Xuan, W.; Armstrong, E.; Gray, L.; Fletcher, J.; Gosbell, I.; Lin, C.; Harris, I.A. Non-compliance with clinical guidelines increases the risk of complications after primary total hip and knee joint replacement surgery. PLoS ONE 2021, 16, e0260146. [Google Scholar] [CrossRef]
- Sartelli, M.; Bartoli, S.; Borghi, F.; Busani, S.; Carsetti, A.; Catena, F.; Cillara, N.; Coccolini, F.; Cortegiani, A.; Cortese, F.; et al. Implementation Strategies for Preventing Healthcare-Associated Infections across the Surgical Pathway: An Italian Multisociety Document. Antibiotics 2023, 12, 521. [Google Scholar] [CrossRef] [PubMed]
- Ariyo, P.; Zayed, B.; Riese, V.; Anton, B.; Latif, A.; Kilpatrick, C.; Allegranzi, B.; Berenholtz, S. Implementation strategies to reduce surgical site infections: A systematic review. Infect. Control Hosp. Epidemiol. 2019, 40, 287–300. [Google Scholar] [CrossRef] [PubMed]
- Horgan, S.; Hegarty, J.; Drennan, J.; Keane, D.; Saab, M.M. The effect of interventions on the incidence of surgical site infections in acute care settings: A systematic review. J. Tissue Viability 2023. [Google Scholar] [CrossRef] [PubMed]
- Leaper, D.J.; Tanner, J.; Kiernan, M.; Assadian, O.; Edmiston, C.E., Jr. Surgical site infection: Poor compliance with guidelines and care bundles. Int. Wound J. 2015, 12, 357–362. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sartelli, M.; Coccolini, F.; Labricciosa, F.M.; Al Omari, A.H.; Bains, L.; Baraket, O.; Catarci, M.; Cui, Y.; Ferreres, A.R.; Gkiokas, G.; et al. Surgical Antibiotic Prophylaxis: A Proposal for a Global Evidence-Based Bundle. Antibiotics 2024, 13, 100. https://doi.org/10.3390/antibiotics13010100
Sartelli M, Coccolini F, Labricciosa FM, Al Omari AH, Bains L, Baraket O, Catarci M, Cui Y, Ferreres AR, Gkiokas G, et al. Surgical Antibiotic Prophylaxis: A Proposal for a Global Evidence-Based Bundle. Antibiotics. 2024; 13(1):100. https://doi.org/10.3390/antibiotics13010100
Chicago/Turabian StyleSartelli, Massimo, Federico Coccolini, Francesco M. Labricciosa, AbdelKarim. H. Al Omari, Lovenish Bains, Oussama Baraket, Marco Catarci, Yunfeng Cui, Alberto R. Ferreres, George Gkiokas, and et al. 2024. "Surgical Antibiotic Prophylaxis: A Proposal for a Global Evidence-Based Bundle" Antibiotics 13, no. 1: 100. https://doi.org/10.3390/antibiotics13010100
APA StyleSartelli, M., Coccolini, F., Labricciosa, F. M., Al Omari, A. H., Bains, L., Baraket, O., Catarci, M., Cui, Y., Ferreres, A. R., Gkiokas, G., Gomes, C. A., Hodonou, A. M., Isik, A., Litvin, A., Lohsiriwat, V., Kotecha, V., Khokha, V., Kryvoruchko, I. A., Machain, G. M., ... Siquini, W. (2024). Surgical Antibiotic Prophylaxis: A Proposal for a Global Evidence-Based Bundle. Antibiotics, 13(1), 100. https://doi.org/10.3390/antibiotics13010100