A Backing-Layer-Shared Miniature Dual-Frequency Ultrasound Probe for Intravascular Ultrasound Imaging: In Vitro and Ex Vivo Validations



Abstract
1. Introduction
2. Materials and Methods
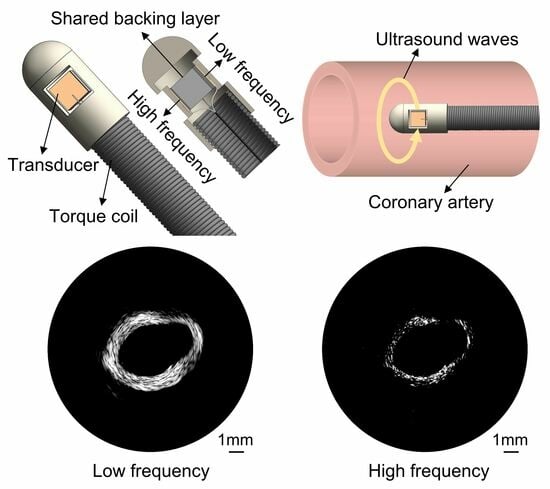
2.1. Transducer Design
2.2. Transducer Fabrication
2.3. Transducer Characterization
2.4. Imaging Evaluation Setup
2.5. In Vitro and Ex Vivo Imaging
3. Results
3.1. Performance of the Dual-Frequency Transducer
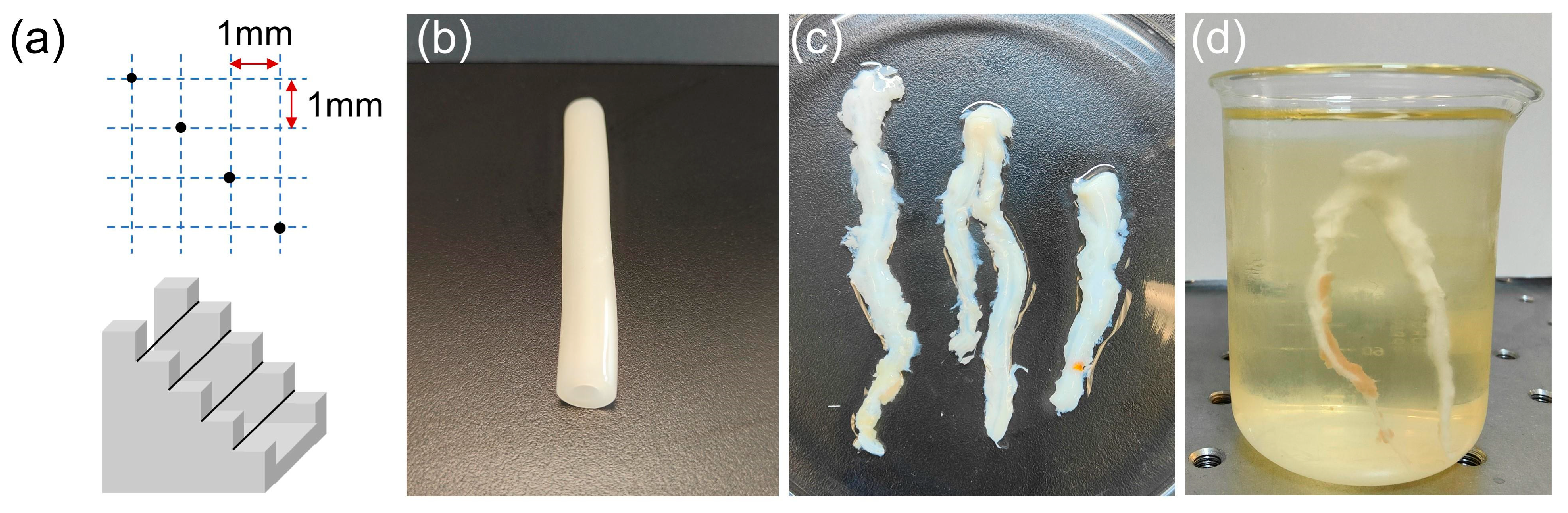
3.2. In Vitro Wire Phantom Imaging
3.3. In Vitro Blood Vessel Phantom Imaging
3.4. Ex Vivo Porcine Coronary Artery Imaging
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frostegard, J. Immunity, atherosclerosis and cardiovascular disease. BME Med. 2013, 11, 117. [Google Scholar] [CrossRef] [PubMed]
- Falk, E.; Nakano, M.; Bentzon, J.F.; Finn, A.V.; Virmani, R. Update on acute coronary syndromes: The pathologists’ view. Eur. Heart J. 2013, 34, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef]
- Stefanadis, C.; Antoniou, C.K.; Tsiachris, D.; Pietri, P. Coronary atherosclerotic vulnerable plaque: Current perspectives. J. Am. Heart Assoc. 2017, 6, e005543. [Google Scholar] [CrossRef]
- Virmani, R.; Burke, A.P.; Farb, A.; Kolodgie, F.D. Pathology of the vulnerable plaque. J. Am. Coll. Cardiol. 2006, 47, C13–C18. [Google Scholar] [CrossRef]
- Aoki, J.; Abizaid, A.C.; Serruys, P.W.; Ong, A.T.L.; Boersma, E.; Sousa, J.E.; Bruining, N. Evaluation of four-year coronary artery response after sirolimus-eluting stent implantation using serial quantitative intravascular ultrasound and computer-assisted grayscale value analysis for plaque composition in event-free patients. J. Am. Coll. Cardiol. 2005, 46, 1670–1676. [Google Scholar] [CrossRef][Green Version]
- Peng, C.; Wu, H.Y.; Kim, S.; Dai, X.M.; Jiang, X.N. Recent advances in transducers for intravascular ultrasound (IVUS) imaging. Sensors 2021, 21, 3540. [Google Scholar] [CrossRef]
- Elliott, M.R.; Thrush, A.J. Measurement of resolution in intravascular ultrasound images. Physiol. Meas. 1996, 17, 259–265. [Google Scholar] [CrossRef]
- Brezinski, M.E.; Tearney, G.J.; Weissman, N.J.; Boppart, S.A.; Bouma, B.E.; Hee, M.R.; Weyman, A.E.; Swanson, E.A.; Southern, J.F.; Fujimoto, J.G. Assessing atherosclerotic plaque morphology: Comparison of optical coherence tomography and high frequency intravascular ultrasound. Heart 1997, 77, 397–403. [Google Scholar] [CrossRef]
- Kawasaki, M.; Bouma, B.E.; Bressner, J.; Houser, S.L.; Nadkarni, S.K.; MacNeill, B.D.; Jang, I.K.; Fujiwara, H.; Tearney, G.J. Diagnostic accuracy of optical coherence tomography and integrated backscatter intravascular ultrasound images for tissue characterization of human coronary plaques. J. Am. Coll. Cardiol. 2006, 48, 81–88. [Google Scholar] [CrossRef]
- Bourantas, C.V.; Garcia-Garcia, H.M.; Naka, K.K.; Sakellarios, A.; Athanasiou, L.; Fotiadis, D.I.; Michalis, L.K.; Serruys, P.W. Hybrid intravascular imaging. J. Am. Coll. Cardiol. 2013, 61, 1369–1378. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Yu, M.Y.; Chen, Z.Y.; Fei, C.L.; Shung, K.K.; Zhou, Q.F. Multi-frequency intravascular ultrasound (IVUS) imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. 2015, 62, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, J.W.; Jing, J.; Ma, T.; Liang, S.S.; Zhang, J.; Mohar, D.; Raney, A.; Mahon, S.; Brenner, M.; et al. Integrated IVUS-OCT imaging for atherosclerotic plaque characterization. IEEE J. Sel. Top. Quantum Electron. 2014, 20, 196–203. [Google Scholar] [CrossRef]
- Ono, M.; Kawashima, H.; Hara, H.; Gao, C.; Wang, R.T.; Kogame, N.; Takahashi, K.; Chichareon, P.; Modolo, R.; Tomaniak, M.; et al. Advances in IVUS/OCT and future clinical perspective of novel hybrid catheter system in coronary imaging. Front. Cardiovasc. Med. 2020, 7, 119. [Google Scholar] [CrossRef]
- Bourantas, C.V.; Jaffer, F.A.; Gijsen, F.J.; van Soest, G.; Madden, S.P.; Courtney, B.K.; Fard, A.M.; Tenekecioglu, E.; Zeng, Y.; van der Steen, A.F.W.; et al. Hybrid intravascular imaging: Recent advances, technical considerations, and current applications in the study of plaque pathophysiology. Eur. Heart J. 2017, 38, 400–412. [Google Scholar] [CrossRef]
- Maresca, D.; Adams, S.; Maresca, B.; van der Steen, A.F.W. Mapping intravascular ultrasound controversies in interventional cardiology practice. PLoS ONE 2014, 9, e97215. [Google Scholar] [CrossRef]
- Frijlink, M.E.; Goertz, D.E.; Vos, H.J.; Tesselaar, E.; Blacquiere, G.; Gisolf, A.; Krams, R.; van der Steen, A.F.W. Harmonic intravascular ultrasound imaging with a dual-frequency catheter. Ultrasound Med. Biol. 2006, 32, 1649–1654. [Google Scholar] [CrossRef]
- Chandrana, C.; Kharin, N.; Vince, G.D.; Roy, S.; Fleischman, A.J. Demonstration of second-harmonic IVUS feasibility with focused broadband miniature transducers. IEEE Trans. Ultrason. Ferroelectr. Freq. 2010, 57, 1077–1085. [Google Scholar] [CrossRef]
- Ma, J.G.; Martin, K.H.; Li, Y.; Dayton, P.A.; Shung, K.K.; Zhou, Q.F.; Jiang, X.N. Design factors of intravascular dual frequency transducers for super-harmonic contrast imaging and acoustic angiography. Phys. Med. Biol. 2015, 60, 3441–3457. [Google Scholar] [CrossRef]
- Tranquart, F.; Grenier, N.; Eder, V.; Pourcelot, L. Clinical use of ultrasound tissue harmonic imaging. Ultrasound Med. Biol. 1999, 25, 889–894. [Google Scholar] [CrossRef]
- Lee, J.; Shin, E.J.; Lee, C.; Chang, J.H. Development of dual-frequency oblong-shaped-focused transducers for intravascular ultrasound tissue harmonic imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. 2018, 65, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, S.; Gorman, B.; Charboneau, J.W.; Tradup, D.J.; Beck, R.J.; Kofler, J.M.; Groth, D.S. Comparison of tissue harmonic imaging with conventional US in abdominal disease. Radiographics 2000, 20, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Anvari, A.; Forsberg, F.; Samir, A.E. A primer on the physical principles of tissue harmonic imaging. Radiographics 2015, 35, 1956–1965. [Google Scholar] [CrossRef]
- Lee, J.; Chang, J.H. Dual-element intravascular ultrasound transducer for tissue harmonic imaging and frequency compounding: Development and imaging performance assessment. IEEE Trans. Biomed. Eng. 2019, 66, 3146–3155. [Google Scholar] [CrossRef]
- Park, J.; Li, X.; Zhou, Q.F.; Shung, K.K. Combined chirp coded tissue harmonic and fundamental ultrasound imaging for intravascular ultrasound: 20-60 MHz phantom and ex vivo results. Ultrasonics 2013, 53, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wu, W.; Chung, Y.; Shih, W.Y.; Shih, W.H.; Zhou, Q.F.; Shung, K.K. 80-MHz intravascular ultrasound transducer using PMN-PT free-standing film. IEEE Trans. Ultrason. Ferroelectr. Freq. 2011, 58, 2281–2288. [Google Scholar] [CrossRef]
- Munding, C.E.; Cherin, E.; Jourard, I.; Weyers, J.J.; Goertz, D.E.; Courtney, B.K.; Foster, F.S. Development of a 3 French dual-frequency intravascular ultrasound catheter. Ultrasound Med. Biol. 2018, 44, 251–266. [Google Scholar] [CrossRef]
- Munding, C.E.; Cherin, E.; Alves, N.; Goertz, D.E.; Courtney, B.K.; Foster, F.S. 30/80 MHz bidirectional dual-frequency IVUS feasibility evaluated in vivo and for stent imaging. Ultrasound Med. Biol. 2020, 46, 2104–2112. [Google Scholar] [CrossRef]
- Su, M.; Zhang, Z.Q.; Hong, J.H.; Huang, Y.C.; Mu, P.T.; Yu, Y.Y.; Liu, R.; Liang, S.Z.; Zheng, H.R.; Qiu, W.B. Cable-shared dual-frequency catheter for intravascular ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. 2019, 66, 849–856. [Google Scholar] [CrossRef]
- Hong, J.H.; Su, M.; Yu, Y.Y.; Zhang, Z.Q.; Liu, R.; Huang, Y.C.; Mu, P.T.; Zheng, H.R.; Qiu, W.B. A dual-mode imaging catheter for intravascular ultrasound application. IEEE Trans. Med. Imaging 2019, 38, 657–663. [Google Scholar] [CrossRef]
- Ryan, L.K.; Foster, F.S. Tissue equivalent vessel phantoms for intravascular ultrasound. Ultrasound Med. Biol. 1997, 23, 261–273. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Low Frequency | High Frequency |
|---|---|---|
| Center frequency (MHz) | 30 | 80 |
| Aperture size (mm) | 0.5 × 0.5 | 0.5 × 0.5 |
| Piezoelectric material | PZT-5H | PZT-5H |
| Thickness (µm) | 60 | 25 |
| First matching layer material | Ag/epoxy | Ag/epoxy |
| Thickness (µm) | 20 | 20 |
| Second matching layer material | Parylene C | Parylene C |
| Thickness (µm) | 10 | 10 |
| Backing layer material | E-Solder 3022 | E-Solder 3022 |
| Thickness (µm) | 500 | 500 |
| Center Frequency | Axial Resolution | Lateral Resolution | |
|---|---|---|---|
| Proposed transducer | 30 MHz | 40 µm | 321 µm |
| 80 MHz | 17 µm | 247 µm | |
| Single element | 30 MHz | 50 µm | 349 µm |
| 80 MHz | 12 µm | 182 µm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Y.; Liu, X.; Zhang, J.; Peng, C. A Backing-Layer-Shared Miniature Dual-Frequency Ultrasound Probe for Intravascular Ultrasound Imaging: In Vitro and Ex Vivo Validations. Biosensors 2023, 13, 971. https://doi.org/10.3390/bios13110971
He Y, Liu X, Zhang J, Peng C. A Backing-Layer-Shared Miniature Dual-Frequency Ultrasound Probe for Intravascular Ultrasound Imaging: In Vitro and Ex Vivo Validations. Biosensors. 2023; 13(11):971. https://doi.org/10.3390/bios13110971
Chicago/Turabian StyleHe, Yashuo, Xi Liu, Jiayi Zhang, and Chang Peng. 2023. "A Backing-Layer-Shared Miniature Dual-Frequency Ultrasound Probe for Intravascular Ultrasound Imaging: In Vitro and Ex Vivo Validations" Biosensors 13, no. 11: 971. https://doi.org/10.3390/bios13110971
APA StyleHe, Y., Liu, X., Zhang, J., & Peng, C. (2023). A Backing-Layer-Shared Miniature Dual-Frequency Ultrasound Probe for Intravascular Ultrasound Imaging: In Vitro and Ex Vivo Validations. Biosensors, 13(11), 971. https://doi.org/10.3390/bios13110971