Integrating a Fundus Camera with High-Frequency Ultrasound for Precise Ocular Lesion Assessment

 , , , , , , ,
, , , , , , , 

Abstract
1. Introduction
2. Materials and Methods
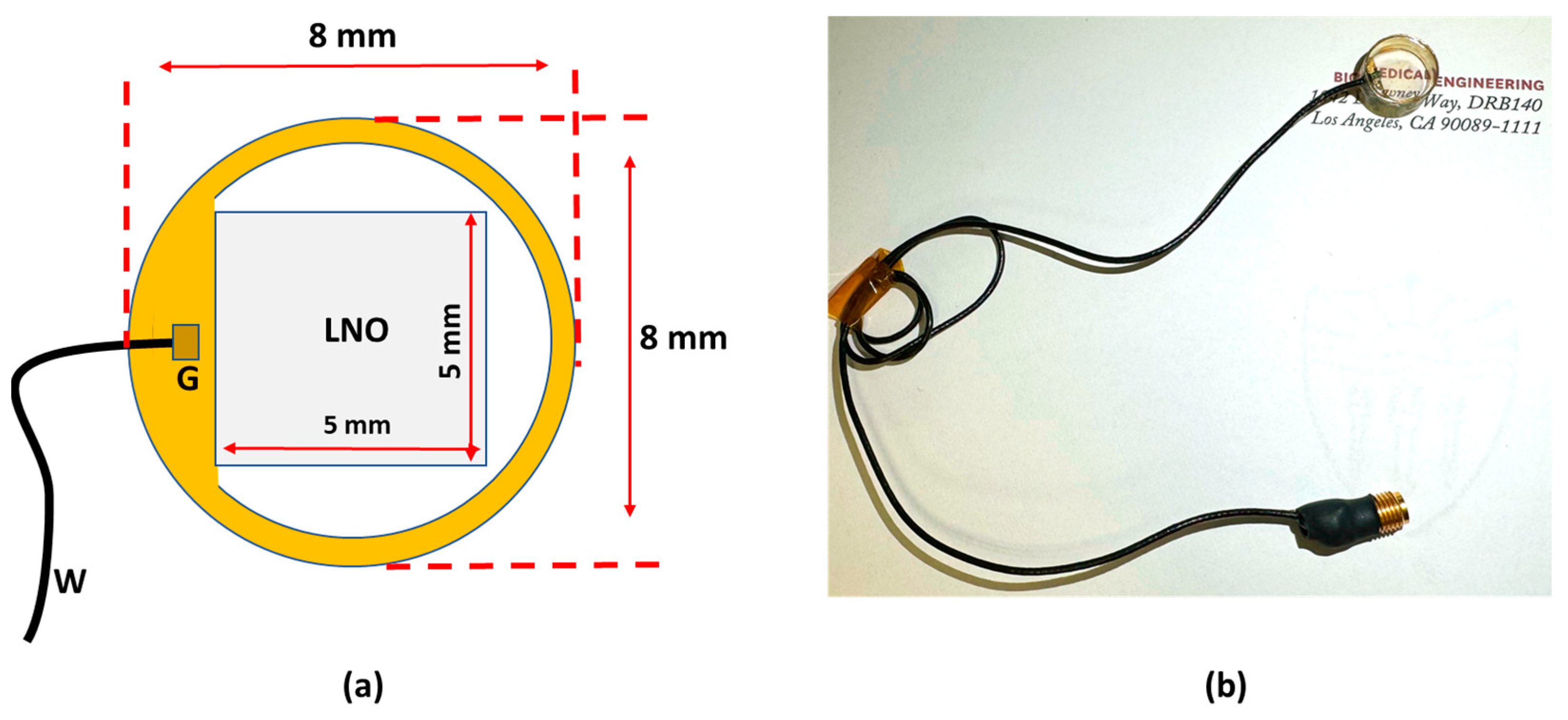
2.1. Design of the Transparent Ultrasound Probe
2.2. Fabrication of the Transparent Ultrasound Probe
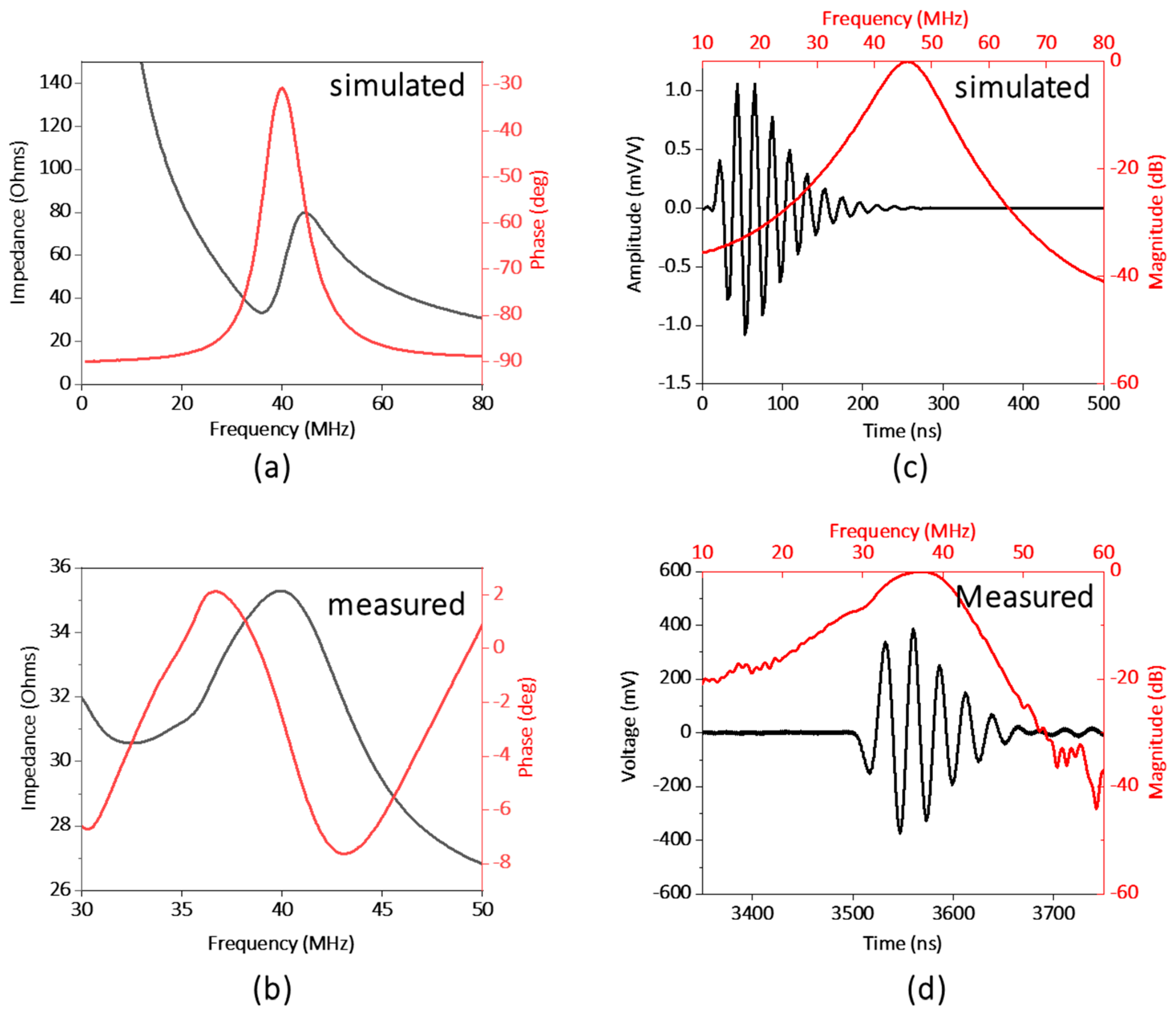
2.3. Testing the Performance of the Transparent Ultrasound Probe
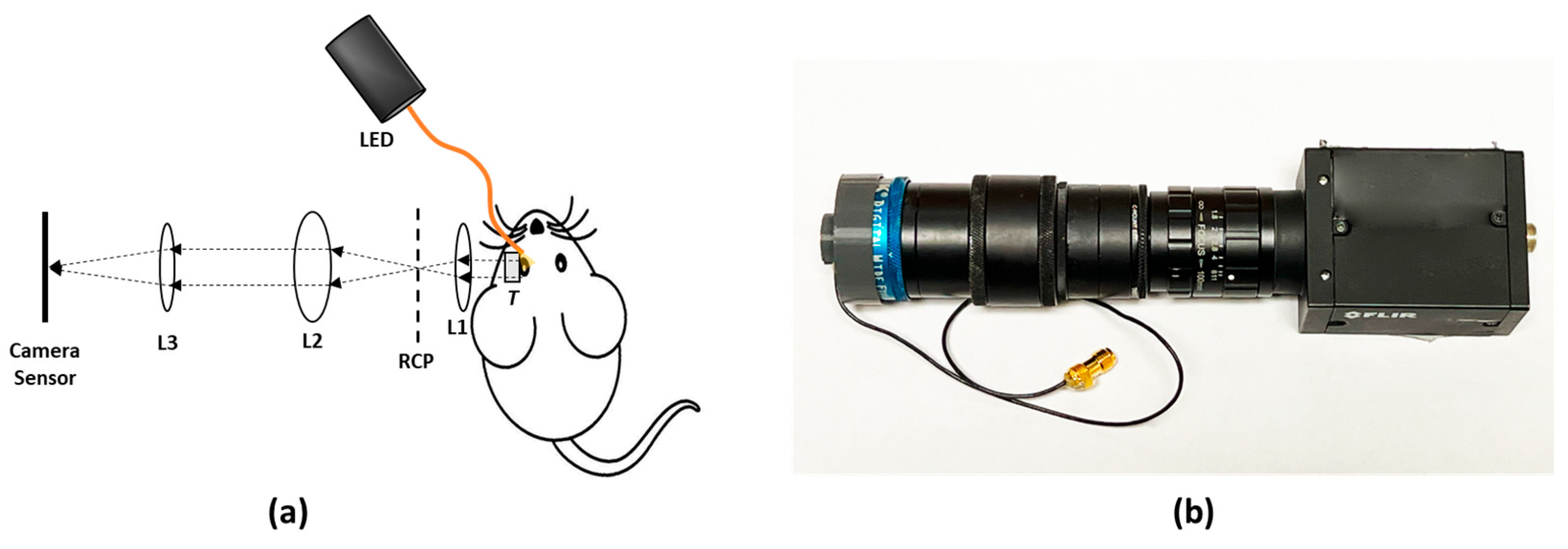
2.4. Experimental Setup
2.5. Animal Preparation
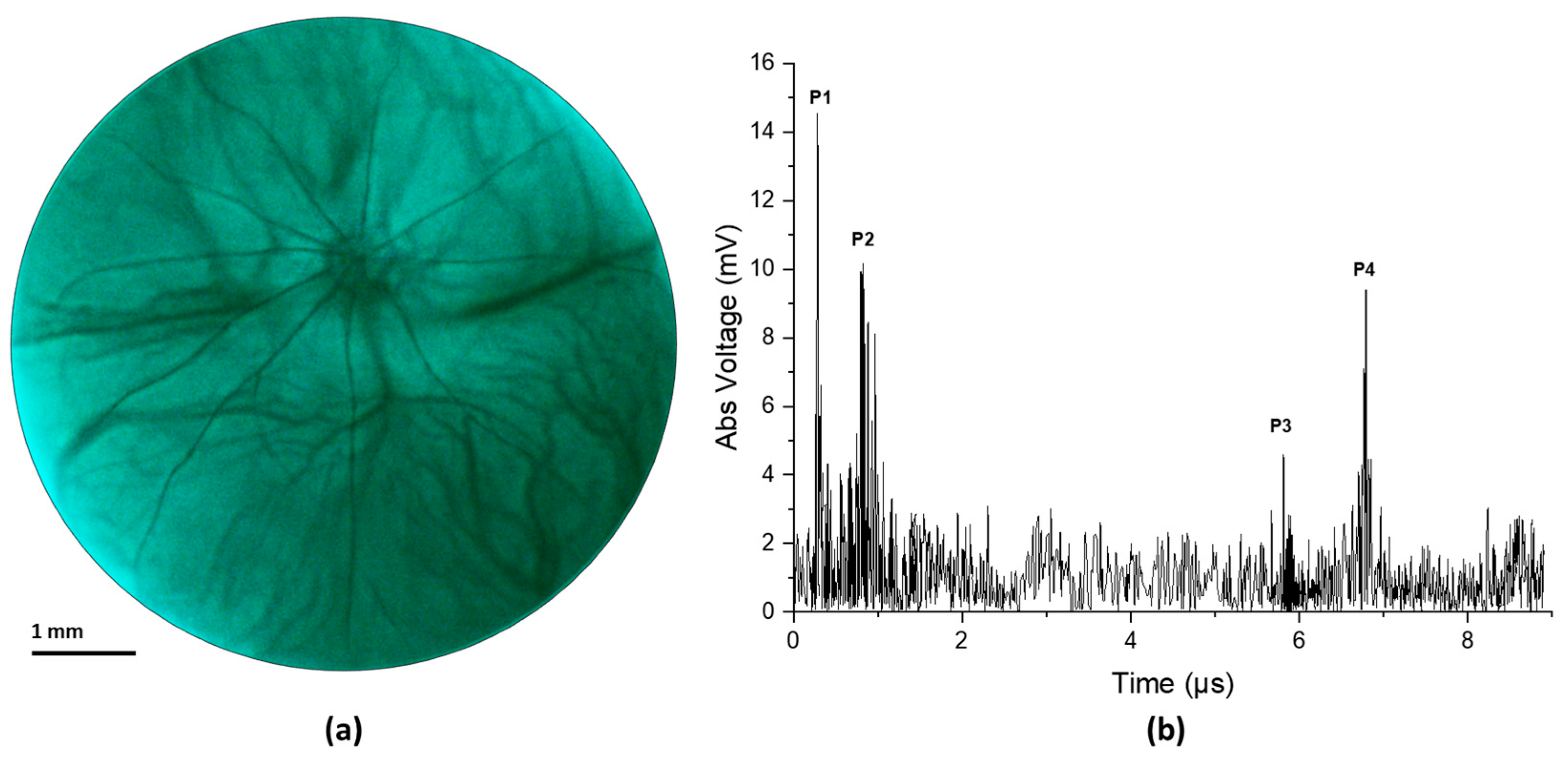
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chien, J.L.; Sioufi, K.; Surakiatchanukul, T.; Shields, J.A.; Shields, C.L. Choroidal nevus: A review of prevalence, features, genetics, risks, and outcomes. Curr. Opin. Ophthalmol. 2017, 28, 228–237. [Google Scholar] [CrossRef]
- Solnik, M.; Paduszyńska, N.; Czarnecka, A.M.; Synoradzki, K.J.; Yousef, Y.A.; Chorągiewicz, T.; Rejdak, R.; Toro, M.D.; Zweifel, S.; Dyndor, K.; et al. Imaging of Uveal Melanoma-Current Standard and Methods in Development. Cancers 2022, 14, 3147. [Google Scholar] [CrossRef]
- Krantz, B.A.; Dave, N.; Komatsubara, K.M.; Marr, B.P.; Carvajal, R.D. Uveal melanoma: Epidemiology, etiology, and treatment of primary disease. Clin. Ophthalmol. 2017, 11, 279–289. [Google Scholar] [CrossRef]
- Cruz-Gálvez, C.C.; Ordaz-Favila, J.C.; Villar-Calvo, V.M.; Cancino-Marentes, M.E.; Bosch-Canto, V. Retinoblastoma: Review and new insights. Front. Oncol. 2022, 12, 963780. [Google Scholar] [CrossRef]
- Shields, C.L.; Furuta, M.; Berman, E.L.; Zahler, J.D.; Hoberman, D.M.; Dinh, D.H.; Mashayekhi, A.; Shields, J.A. Choroidal nevus transformation into melanoma: Analysis of 2514 consecutive cases. Arch. Ophthalmol. 2009, 127, 981–987. [Google Scholar] [CrossRef]
- Yao, X.; Son, T.; Ma, J. Developing portable widefield fundus camera for teleophthalmology: Technical challenges and potential solutions. Exp. Biol. Med. 2022, 247, 289–299. [Google Scholar] [CrossRef]
- Nagiel, A.; Lalane, R.A.; Sadda, S.R.; Schwartz, S.D. Ultra-Widefield Fundus Imaging: A Review of Clinical Applications and Future Trends. Retina 2016, 36, 660–678. [Google Scholar] [CrossRef]
- Quinn, N.; Csincsik, L.; Flynn, E.; Curcio, C.A.; Kiss, S.; Sadda, S.R.; Hogg, R.; Peto, T.; Lengyel, I. The clinical relevance of visualising the peripheral retina. Prog. Retin. Eye Res. 2019, 68, 83–109. [Google Scholar] [CrossRef]
- Singh, P.; Singh, A. Choroidal melanoma. Oman J. Ophthalmol. 2012, 5, 3–9. [Google Scholar] [CrossRef]
- Torres, V.L.; Brugnoni, N.; Kaiser, P.K.; Singh, A.D. Optical coherence tomography enhanced depth imaging of choroidal tumors. Am. J. Ophthalmol. 2011, 151, 586–593.e582. [Google Scholar] [CrossRef]
- Say, E.A.; Shah, S.U.; Ferenczy, S.; Shields, C.L. Optical coherence tomography of retinal and choroidal tumors. J. Ophthalmol. 2011, 2011, 385058. [Google Scholar] [CrossRef][Green Version]
- Fonkeu, Y.; Singh, N.; Hayden-Loreck, B.; Singh, A.D. Diagnostic A-Scan of Choroidal Melanoma: Automated Quantification of Parameters. Ocul. Oncol. Pathol. 2019, 5, 350–357. [Google Scholar] [CrossRef]
- Gündüz, K.; Yeşiltaş, Y.S. Diagnostic Techniques: Angiography. In Clinical Ophthalmic Oncology: Basic Principles; Singh, A.D., Damato, B.E., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 209–234. [Google Scholar]
- Midena, E.; Frizziero, L.; Pilotto, E.; Parrozzani, R. Diagnostic Techniques: Autofluorescence. In Clinical Ophthalmic Oncology: Basic Principles; Singh, A.D., Damato, B.E., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 257–270. [Google Scholar]
- Lorek, B.H.; Aronow, M.E.; Singh, A.D. Diagnostic Techniques: Ultrasonography. In Clinical Ophthalmic Oncology: Basic Principles; Singh, A.D., Damato, B.E., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 271–293. [Google Scholar]
- Kadakia, A.; Zhang, J.; Yao, X.; Zhou, Q.; Heiferman, M.J. Ultrasound in ocular oncology: Technical advances, clinical applications, and limitations. Exp. Biol. Med. 2023, 248, 371–379. [Google Scholar] [CrossRef]
- Safari, A.; Zhou, Q.; Zeng, Y.; Leber, J.D. Advances in development of Pb-free piezoelectric materials for transducer applications. Jpn. J. Appl. Phys. 2023, 62, SJ0801. [Google Scholar] [CrossRef]
- Sun, Y.; Jiang, L.; Chen, R.; Li, R.; Kang, H.; Zeng, Y.; Yan, Y.; Priya, S.; Zhou, Q. Design and Fabrication of 15-MHz Ultrasonic Transducers Based on a Textured Pb(Mg1/3Nb2/3)O3-Pb(Zr, Ti)O3 Ceramic. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2022, 69, 3095–3101. [Google Scholar] [CrossRef]
- Li, R.; Zeng, Y.; Sun, X.X.; Li, C.; Li, R.; Zheng, T.; Jiang, L.; Wu, J. Multidimensional synergy-induced high piezoelectricity and reliability KNN piezoceramics for high-frequency ultrasonic transducers. Sci. China Mater. 2023, 66, 686–695. [Google Scholar] [CrossRef]
- Silverman, R.H. Focused ultrasound in ophthalmology. Clin. Ophthalmol. 2016, 10, 1865–1875. [Google Scholar] [CrossRef]
- Chopdar, A.; Aung, T. Multimodal Retinal Imaging; JP Medical Ltd.: London, UK, 2014. [Google Scholar]
- Ossoinig, K.C. Standardized echography: Basic principles, clinical applications, and results. Int. Ophthalmol. Clin. 1979, 19, 127–210. [Google Scholar] [CrossRef]
- Ossoinig, K.C. Quantitative echography--the basis of tissue differentiation. J. Clin. Ultrasound JCU 1974, 2, 33–46. [Google Scholar] [CrossRef]
- Singh, N.; Fonkeu, Y.; Lorek, B.H.; Singh, A.D. Diagnostic A-Scan of Choroidal Tumors: Comparison of Quantified Parameters. Ocul. Oncol. Pathol. 2019, 5, 358–368. [Google Scholar] [CrossRef]
- Campagnoli, T.R.; Medina, C.A.; Singh, A.D. Choroidal melanoma initially treated as hemangioma: Diagnostic and therapeutic considerations. Retin. Cases Brief Rep. 2016, 10, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Weingeist, T.A. Factors Predictive of Growth and Treatment of Small Choroidal Melanoma: COMS Report No. 5. Arch. Ophthalmol. 1997, 115, 1537–1544. [Google Scholar]
- Chen, R.; Jiang, L.; Zhang, T.; Matsuoka, T.; Yamazaki, M.; Qian, X.; Lu, G.; Safari, A.; Zhu, J.; Shung, K.K.; et al. Eco-Friendly Highly Sensitive Transducers Based on a New KNN–NTK–FM Lead-Free Piezoelectric Ceramic for High-Frequency Biomedical Ultrasonic Imaging Applications. IEEE Trans. Biomed. Eng. 2019, 66, 1580–1587. [Google Scholar] [CrossRef]
- Alterini, T.; Diaz-Douton, F.; Burgos-Fernandez, F.J.; Gonzalez, L.; Mateo, C.; Vilaseca, M. Fast visible and extended near-infrared multispectral fundus camera. J. Biomed. Opt. 2019, 24, 1–7. [Google Scholar]
- Lozano, D.C.; Twa, M.D. Development of a Rat Schematic Eye From In Vivo Biometry and the Correction of Lateral Magnification in SD-OCT Imaging. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6446–6455. [Google Scholar] [CrossRef]
- Wu, Y.; Luo, X.; Feng, Y.; Yang, J.; Fan, H.; Cen, X.; Li, W. Comparison of the accuracy of axial length measurement by different imaging methods in Sprague Dawley rats. Front. Neurosci. 2023, 16, 1106904. [Google Scholar] [CrossRef]
- Remtulla, S.; Hallett, P.E. A schematic eye for the mouse, and comparisons with the rat. Vis. Res. 1985, 25, 21–31. [Google Scholar] [CrossRef]
- Hoffer, K.J. Ultrasound velocities for axial eye length measurement. J. Cataract Refract. Surg. 1994, 20, 554–562. [Google Scholar] [CrossRef]
- Shields, C.L.; Shields, J.A.; Kiratli, H.; De Potter, P.; Cater, J.R. Risk factors for growth and metastasis of small choroidal melanocytic lesions. Ophthalmology 1995, 102, 1351–1361. [Google Scholar] [CrossRef]
- Carpenter, C.L.; Kim, A.Y.; Kashani, A.H. Normative Retinal Thicknesses in Common Animal Models of Eye Disease Using Spectral Domain Optical Coherence Tomography. In Book Normative Retinal Thicknesses in Common Animal Models of Eye Disease Using Spectral Domain Optical Coherence Tomography; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; pp. 157–166. [Google Scholar]
- De Korte, C.; van der Steen, A.; Thijssen, J. Acoustic velocity and attenuation of eye tissues at 20 MHz. Ultrasound Med. Biol. 1994, 20, 471–480. [Google Scholar] [CrossRef]
- Negron, L.A.; Viola, F.; Black, E.P.; Toth, C.A.; Walker, W.F. Development and characterization of a vitreous mimicking material for radiation force imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2002, 49, 1543–1551. [Google Scholar] [CrossRef]
- Bekerman, I.; Gottlieb, P.; Vaiman, M. Variations in eyeball diameters of the healthy adults. J. Ophthalmol. 2014, 2014, 503645. [Google Scholar] [CrossRef]
- Ng, A.; Swanevelder, J. Resolution in ultrasound imaging. Contin. Educ. Anaesth. Crit. Care Pain 2011, 11, 186–192. [Google Scholar] [CrossRef]
- Toslak, D.; Thapa, D.; Chen, Y.; Erol, M.K.; Paul Chan, R.V.; Yao, X. Trans-palpebral illumination: An approach for wide-angle fundus photography without the need for pupil dilation. Opt. Lett. 2016, 41, 2688–2691. [Google Scholar] [CrossRef]
- Rossi, A.; Rahimi, M.; Le, D.; Son, T.; Heiferman, M.J.; Chan, R.V.P.; Yao, X. Portable widefield fundus camera with high dynamic range imaging capability. Biomed. Opt. Express 2023, 14, 906–917. [Google Scholar] [CrossRef]
- Toslak, D.; Liu, C.; Alam, M.N.; Yao, X. Near-infrared light-guided miniaturized indirect ophthalmoscopy for nonmydriatic wide-field fundus photography. Opt. Lett. 2018, 43, 2551–2554. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Center frequency | 40 MHz |
| Surface area | 5 mm × 5 mm |
| Lithium niobate (LNO) thickness | 70 µm |
| Matching layer (Parylene) thickness | 10 µm |
| Backing layer (Epo-Tek 301) thickness | 5 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, A.; Zeng, Y.; Rahimi, M.; Son, T.; Heiferman, M.J.; Gong, C.; Sun, X.; Soleimani, M.; Djalilian, A.R.; Humayun, M.S.; et al. Integrating a Fundus Camera with High-Frequency Ultrasound for Precise Ocular Lesion Assessment. Biosensors 2024, 14, 127. https://doi.org/10.3390/bios14030127
Rossi A, Zeng Y, Rahimi M, Son T, Heiferman MJ, Gong C, Sun X, Soleimani M, Djalilian AR, Humayun MS, et al. Integrating a Fundus Camera with High-Frequency Ultrasound for Precise Ocular Lesion Assessment. Biosensors. 2024; 14(3):127. https://doi.org/10.3390/bios14030127
Chicago/Turabian StyleRossi, Alfa, Yushun Zeng, Mojtaba Rahimi, Taeyoon Son, Michael J. Heiferman, Chen Gong, Xin Sun, Mohammad Soleimani, Ali R. Djalilian, Mark S. Humayun, and et al. 2024. "Integrating a Fundus Camera with High-Frequency Ultrasound for Precise Ocular Lesion Assessment" Biosensors 14, no. 3: 127. https://doi.org/10.3390/bios14030127
APA StyleRossi, A., Zeng, Y., Rahimi, M., Son, T., Heiferman, M. J., Gong, C., Sun, X., Soleimani, M., Djalilian, A. R., Humayun, M. S., Zhou, Q., & Yao, X. (2024). Integrating a Fundus Camera with High-Frequency Ultrasound for Precise Ocular Lesion Assessment. Biosensors, 14(3), 127. https://doi.org/10.3390/bios14030127