Accuracy Assessment of the GlucoMen® Day CGM System in Individuals with Type 1 Diabetes: A Pilot Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Meal/Insulin Challenge
2.2. Data Analysis
3. Results
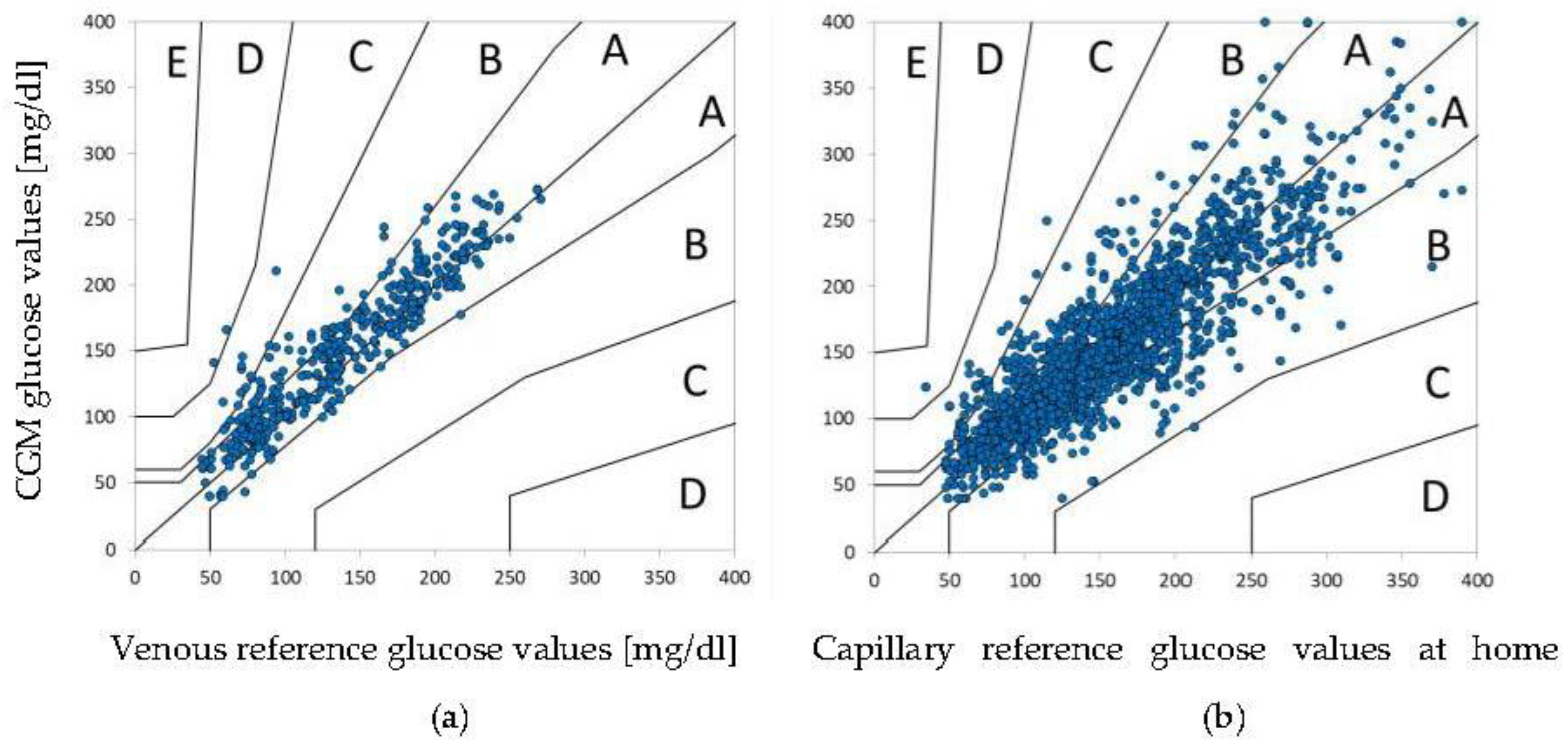
3.1. Accuracy CGM vs. YSI
3.2. Accuracy CGM vs. SMBG
3.3. Sensor Precision
3.4. Usability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group; Tamborlane, W.V.; Beck, R.W.; Bode, B.W.; Buckingham, B.; Chase, H.P.; Clemons, R.; Fiallo-Scharer, R.; Fox, L.A.; Gilliam, L.K.; et al. Continuous glucose monitoring and intensive treatment of type 1 diabetes. N. Engl. J. Med. 2008, 359, 1464–1476. [Google Scholar]
- Lind, M.; Polonsky, W.; Hirsch, I.B.; Heise, T.; Bolinder, J.; Dahlqvist, S.; Schwarz, E.; Ólafsdóttir, A.F.; Frid, A.; Wedel, H.; et al. Continuous Glucose Monitoring vs. Conventional Therapy for Glycemic Control in Adults with Type 1 Diabetes Treated with Multiple Daily Insulin Injections: The GOLD Randomized Clinical Trial. JAMA 2017, 317, 379–387. [Google Scholar] [CrossRef]
- Beck, R.W.; Riddlesworth, T.; Ruedy, K.; Ahmann, A.; Bergenstal, R.; Haller, S.; Kollman, C.; Kruger, D.; McGill, J.B.; Polonsky, W.; et al. Effect of Continuous Glucose Monitoring on Glycemic Control in Adults With Type 1 Diabetes Using Insulin Injections: The DIAMOND Randomized Clinical Trial. JAMA 2017, 317, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Damiano, E.R.; El-Khatib, F.H.; Zheng, H.; Nathan, D.M.; Russell, S.J. A Comparative Effectiveness Analysis of Three Continuous Glucose Monitors. Diabetes Care 2013, 36, 251–259. [Google Scholar] [CrossRef] [Green Version]
- Matuleviciene, V.; Joseph, J.I.; Andelin, M.; Hirsch, I.B.; Attvall, S.; Pivodic, A.; Dahlqvist, S.; Klonoff, D.C.; Haraldsson, B.; Lind, M. A Clinical Trial of the Accuracy and Treatment Experience of the Dexcom G4 Sensor (Dexcom G4 System) and Enlite Sensor (Guardian REAL-Time System) Tested Simultaneously in Ambulatory Patients with Type 1 Diabetes. Diabetes Technol. Ther. 2014, 16, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Laffel, L. Improved Accuracy of Continuous Glucose Monitoring Systems in Pediatric Patients with Diabetes Mellitus: Results from Two Studies. Diabetes Technol. Ther. 2016, 18, S2-23–S2-33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsh, J.B.; Gao, P.; Derdzinski, M.; Puhr, S.; Johnson, T.K.; Walker, T.C.; Graham, C. Accuracy, Utilization, and Effectiveness Comparisons of Different Continuous Glucose Monitoring Systems. Diabetes Technol. Ther. 2019, 21, 128–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Facchinetti, A. Continuous Glucose Monitoring Sensors: Past, Present and Future Algorithmic Challenges. Sensors 2016, 16, 2093. [Google Scholar] [CrossRef]
- Forlenza, G.P.; Argento, N.B.; Laffel, L.M. Practical Considerations on the Use of Continuous Glucose Monitoring in Pediatrics and Older Adults and Nonadjunctive Use. Diabetes Technol. Ther. 2017, 19, S13–S20. [Google Scholar] [CrossRef] [Green Version]
- Beck, R.W.; Brown, S.A.; Lum, J.W.; Kovatchev, B.P. Nonadjunctive Use of Continuous Glucose Monitoring: The End of Fingersticks? Diabetes Technol. Ther. 2020, 22, 67–68. [Google Scholar] [CrossRef]
- Panel, FDA Advisory. FDA Advisory Panel Votes to Recommend Non-Adjunctive Use of Dexcom G5 Mobile CGM. Diabetes Technol. Ther. 2016, 18, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.C.; Foster, N.C.; Maahs, D.M.; Raghinaru, D.; Bergenstal, R.M.; Ahmann, A.J.; Peters, A.L.; Bode, B.W.; Aleppo, G.; Hirsch, I.B.; et al. Real-Time Continuous Glucose Monitoring Among Participants in the T1D Exchange Clinic Registry. Diabetes Care 2014, 37, 2702–2709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klonoff, D.C.; Heinemann, L.; Cook, C.B.; Thompson, B.M.; Kerr, D.; Han, J.; Krisiunas, E.P. The Diabetes Technology Society Green Diabetes Initiative. J. Diabetes Sci. Technol. 2020, 14, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Freckmann, G.; Pleus, S.; Grady, M.; Setford, S.; Levy, B. Measures of Accuracy for Continuous Glucose Monitoring and Blood Glucose Monitoring Devices. J. Diabetes Sci. Technol. 2018, 13, 575–583. [Google Scholar] [CrossRef]
- EN ISO 15197:2015; In Vitro Diagnostic Test Systems-Requirements for Blood-Glucose Monitoring Systems for Self-Testing in Managing Diabetes Mellitus. International Organization for Standardization: Geneva, Switzerland, 2015.
- Beck, R.W.; Bergenstal, R.M.; Riddlesworth, T.D.; Kollman, C.; Li, Z.; Brown, A.S.; Close, K.L. Validation of Time in Range as an Outcome Measure for Diabetes Clinical Trials. Diabetes Care 2018, 42, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, L.; Schoemaker, M.; Schmelzeisen-Redecker, G.; Hinzmann, R.; Kassab, A.; Freckmann, G.; Reiterer, F.; Del Re, L. Benefits and Limitations of MARD as a Performance Parameter for Continuous Glucose Monitoring in the Interstitial Space. J. Diabetes Sci. Technol. 2019, 14, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Kropff, J.; Bruttomesso, D.; Doll, W.; Farret, A.; Galasso, S.; Luijf, Y.M.; Mader, J.K.; Place, J.; Boscari, F.; Pieber, T.R.; et al. Accuracy of two continuous glucose monitoring systems: A head-to-head comparison under clinical research centre and daily life conditions. Diabetes Obes. Metab. 2014, 17, 343–349. [Google Scholar] [CrossRef]
- Bailey, T.S.; Chang, A.; Christiansen, M. Clinical Accuracy of a Continuous Glucose Monitoring System with an Advanced Algorithm. J. Diabetes Sci. Technol. 2014, 9, 209–214. [Google Scholar] [CrossRef] [Green Version]
- Luijf, Y.M.; Mader, J.K.; Doll, W.; Pieber, T.; Farret, A.; Place, J.; Renard, E.; Bruttomesso, D.; Filippi, A.; Avogaro, A.; et al. Accuracy and Reliability of Continuous Glucose Monitoring Systems: A Head-to-Head Comparison. Diabetes Technol. Ther. 2013, 15, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Wadwa, R.P.; Laffel, L.M.; Shah, V.N.; Garg, S.K. Accuracy of a Factory-Calibrated, Real-Time Continuous Glucose Monitoring System during 10 Days of Use in Youth and Adults with Diabetes. Diabetes Technol. Ther. 2018, 20, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Bailey, T.; Bode, B.W.; Christiansen, M.P.; Klaff, L.J.; Alva, S. The Performance and Usability of a Factory-Calibrated Flash Glucose Monitoring System. Diabetes Technol. Ther. 2015, 17, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Alva, S.; Bailey, T.; Brazg, R.; Budiman, E.S.; Castorino, K.; Christiansen, M.P.; Forlenza, G.; Kipnes, M.; Liljenquist, D.R.; Liu, H. Accuracy of a 14-Day Factory-Calibrated Continuous Glucose Monitoring System with Advanced Algorithm in Pediatric and Adult Population with Diabetes. J. Diabetes Sci. Technol. 2020, 16, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Pandis, M.; Aberer, F.; Kojzar, H.; Hochfellner, D.; Elsayed, H.; Motschnig, M.; Augustin, T.; Kreuzer, P.; Pieber, T.R.; et al. A head-to-head comparison of personal and professional continuous glucose monitoring systems in people with type 1 diabetes: Hypoglycaemia remains the weak spot. Diabetes Obes. Metab. 2018, 21, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Eckstein, M.L.; McCarthy, O.; Deere, R.; Pitt, J.; Williams, D.M.; Hayes, J.; Sourij, H.; Bain, S.C.; Bracken, R.M. Performance of the Freestyle Libre flash glucose monitoring (flash GM) system in individuals with type 1 diabetes: A secondary outcome analysis of a randomized crossover trial. Diabetes Obes. Metab. 2019, 21, 2505–2512. [Google Scholar] [CrossRef] [Green Version]
- Aberer, F.; Hajnsek, M.; Rumpler, M.; Zenz, S.; Baumann, P.M.; Elsayed, H.; Puffing, A.; Treiber, G.; Pieber, T.R.; Sourij, H.; et al. Evaluation of subcutaneous glucose monitoring systems under routine environmental conditions in patients with type 1 diabetes. Diabetes Obes. Metab. 2017, 19, 1051–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rusak, E.; Ogarek, N.; Wolicka, K.; Mrówka, A.; Seget, S.; Kuźnik, M.; Jarosz-Chobot, P. The Quality of Life and Satisfaction with Continuous Glucose Monitoring Therapy in Children under 7 Years of Age with T1D Using the rtCGM System Integrated with Insulin Pump—A Caregivers Point of View. Sensors 2021, 21, 3683. [Google Scholar] [CrossRef]
- Haak, T.; Hanaire, H.; Ajjan, R.; Hermanns, N.; Riveline, J.-P.; Rayman, G. Flash Glucose-Sensing Technology as a Replacement for Blood Glucose Monitoring for the Management of Insulin-Treated Type 2 Diabetes: A Multicenter, Open-Label Randomized Controlled Trial. Diabetes Ther. 2016, 8, 55–73. [Google Scholar] [CrossRef] [Green Version]
- Polonsky, W.H.; Hessler, D.; Ruedy, K.J.; Beck, R.W. The Impact of Continuous Glucose Monitoring on Markers of Quality of Life in Adults With Type 1 Diabetes: Further Findings From the DIAMOND Randomized Clinical Trial. Diabetes Care 2017, 40, 736–741. [Google Scholar] [CrossRef] [Green Version]
- Hilliard, M.E.; Levy, W.; Anderson, B.J.; Whitehouse, A.L.; Commissariat, P.V.; Harrington, K.R.; Laffel, L.M.; Miller, K.M.; Van Name, M.; Tamborlane, W.V.; et al. Benefits and Barriers of Continuous Glucose Monitoring in Young Children with Type 1 Diabetes. Diabetes Technol. Ther. 2019, 21, 493–498. [Google Scholar] [CrossRef]
- de Bock, M.; Cooper, M.; Retterath, A.; Nicholas, J.; Ly, T.; Jones, T.; Davis, E. Continuous Glucose Monitoring Adherence. J. Diabetes Sci. Technol. 2016, 10, 627–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, N.C.; Beck, R.W.; Miller, K.M.; Clements, M.A.; Rickels, M.R.; DiMeglio, L.A.; Maahs, D.M.; Tamborlane, W.V.; Bergenstal, R.; Smith, E.; et al. State of Type 1 Diabetes Management and Outcomes from the T1D Exchange in 2016–2018. Diabetes Technol. Ther. 2019, 21, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, L.; Krisiunas, E. Diabetes Technology and Waste: A Complex Problem Piling Up! J. Diabetes Sci. Technol. 2019, 13, 815–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| YSI | SMBG | ||
|---|---|---|---|
| [Glucose] < 100 mg/dL | [Glucose] < 100 mg/dL | ||
| MAD (±SD), mg/dL | 20.5 (+/−18.7) | MAD (±SD), mg/dL | 16.6 (+/−16.8) |
| Median AD [IQR 25th/75th], mg/dL | 16.5 [9.5–24.0] | Median AD [IQR 25th/75th], mg/dL | 12.0 [3.0–23.0] |
| [Glucose] ≥ 100 mg/dL | [Glucose] ≥ 100 mg/dL | ||
| MARD (±SD), mg/dL | 9.7 (+/−9.4) | MARD (±SD), mg/dL | 13.1 (+/−12.8) |
| Median ARD [IQR 25th/75th], mg/dL | 6.7 [2.6–14.6] | Median ARD [IQR 25th/75th], mg/dL | 9.8 [3.5–18.6] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hochfellner, D.A.; Simic, A.; Taucher, M.T.; Sailer, L.S.; Kopanz, J.; Pöttler, T.; Mader, J.K. Accuracy Assessment of the GlucoMen® Day CGM System in Individuals with Type 1 Diabetes: A Pilot Study. Biosensors 2022, 12, 106. https://doi.org/10.3390/bios12020106
Hochfellner DA, Simic A, Taucher MT, Sailer LS, Kopanz J, Pöttler T, Mader JK. Accuracy Assessment of the GlucoMen® Day CGM System in Individuals with Type 1 Diabetes: A Pilot Study. Biosensors. 2022; 12(2):106. https://doi.org/10.3390/bios12020106
Chicago/Turabian StyleHochfellner, Daniel A., Amra Simic, Marlene T. Taucher, Lea S. Sailer, Julia Kopanz, Tina Pöttler, and Julia K. Mader. 2022. "Accuracy Assessment of the GlucoMen® Day CGM System in Individuals with Type 1 Diabetes: A Pilot Study" Biosensors 12, no. 2: 106. https://doi.org/10.3390/bios12020106
APA StyleHochfellner, D. A., Simic, A., Taucher, M. T., Sailer, L. S., Kopanz, J., Pöttler, T., & Mader, J. K. (2022). Accuracy Assessment of the GlucoMen® Day CGM System in Individuals with Type 1 Diabetes: A Pilot Study. Biosensors, 12(2), 106. https://doi.org/10.3390/bios12020106