Biomechanical Analysis and Design Method for Patient-Specific Reconstructive Implants for Large Bone Defects of the Distal Lateral Femur



Abstract
:1. Introduction
2. Materials and Methods
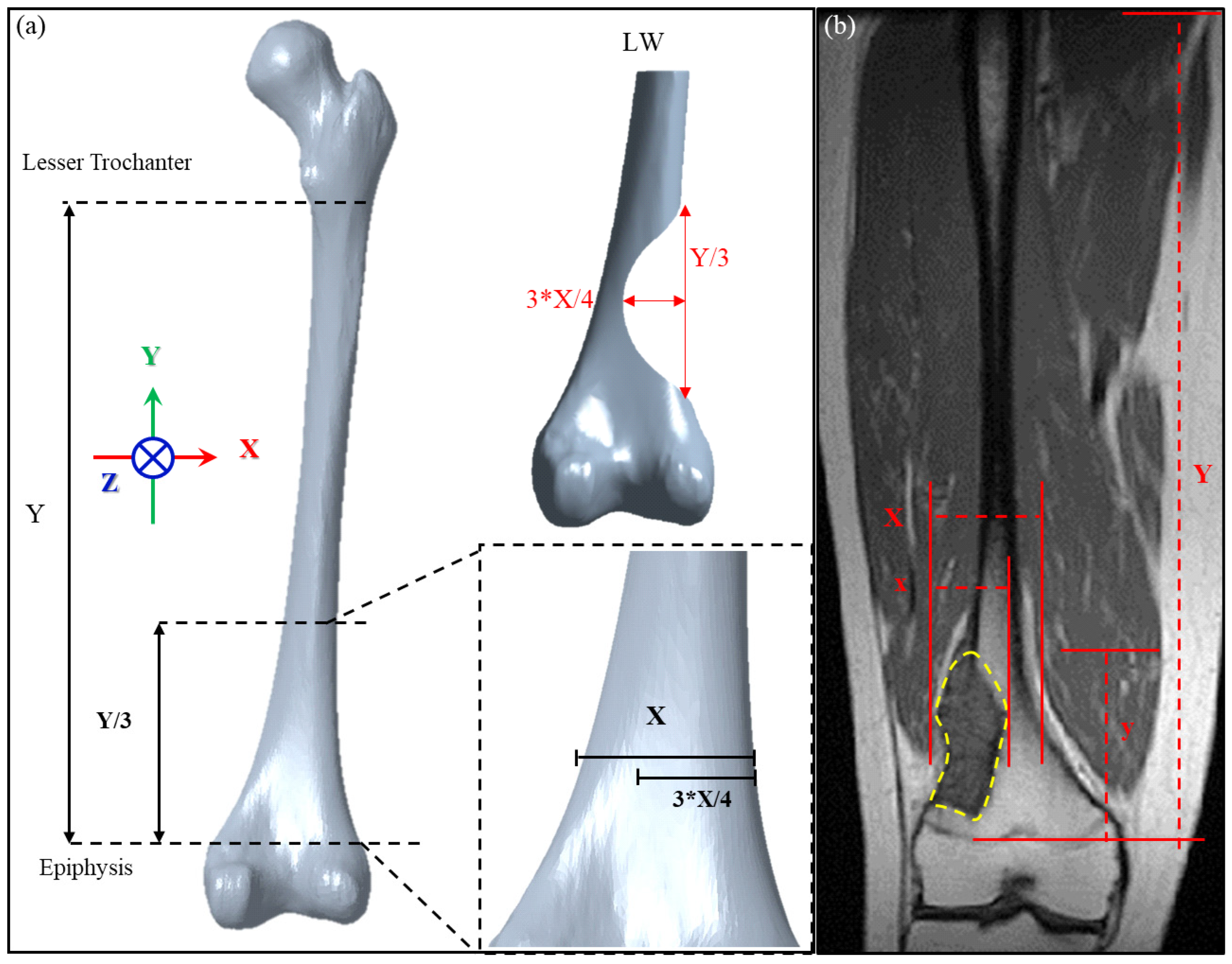
2.1. Definition and Verification of Large Bone Defects in the Distal Femur
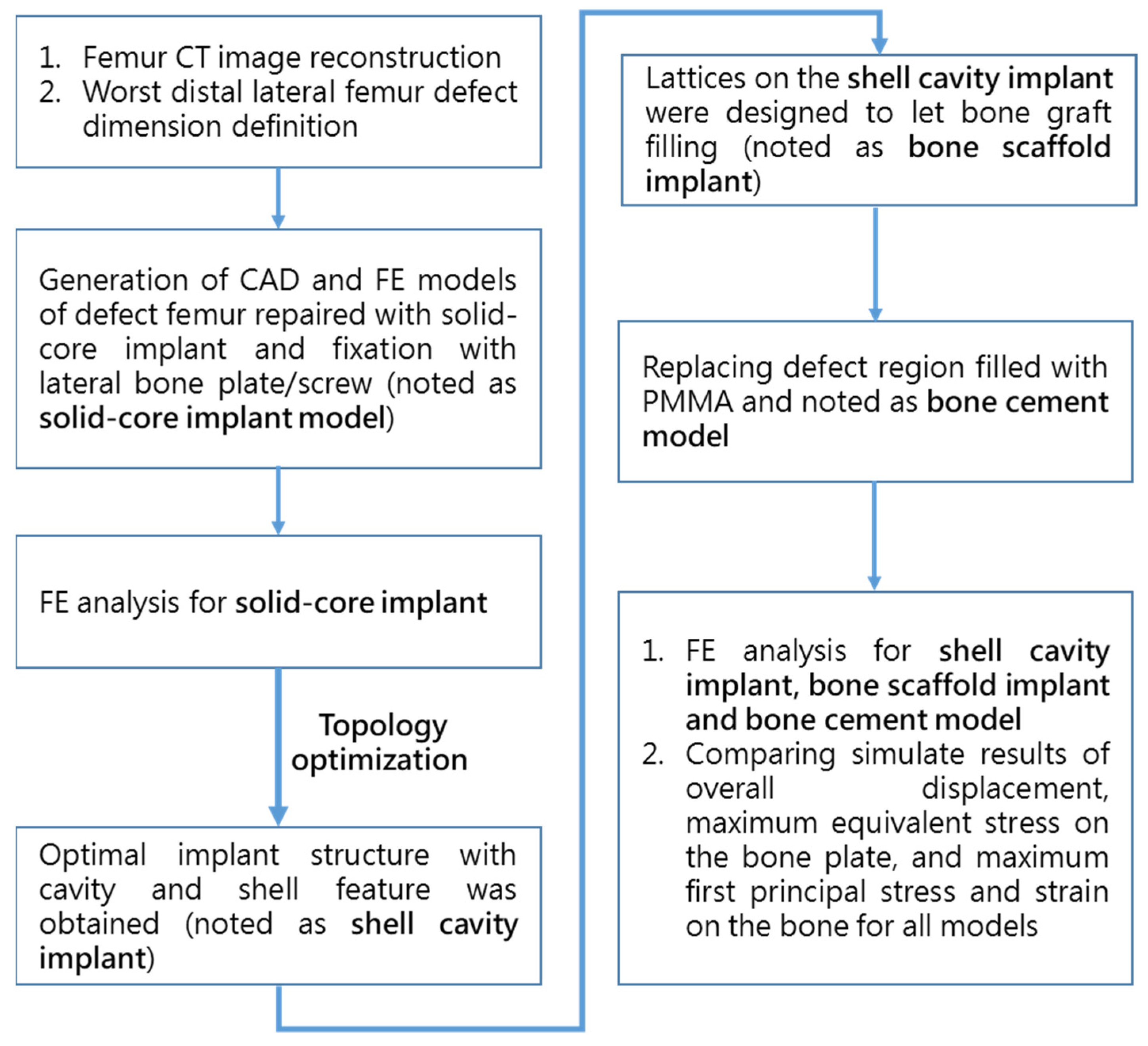
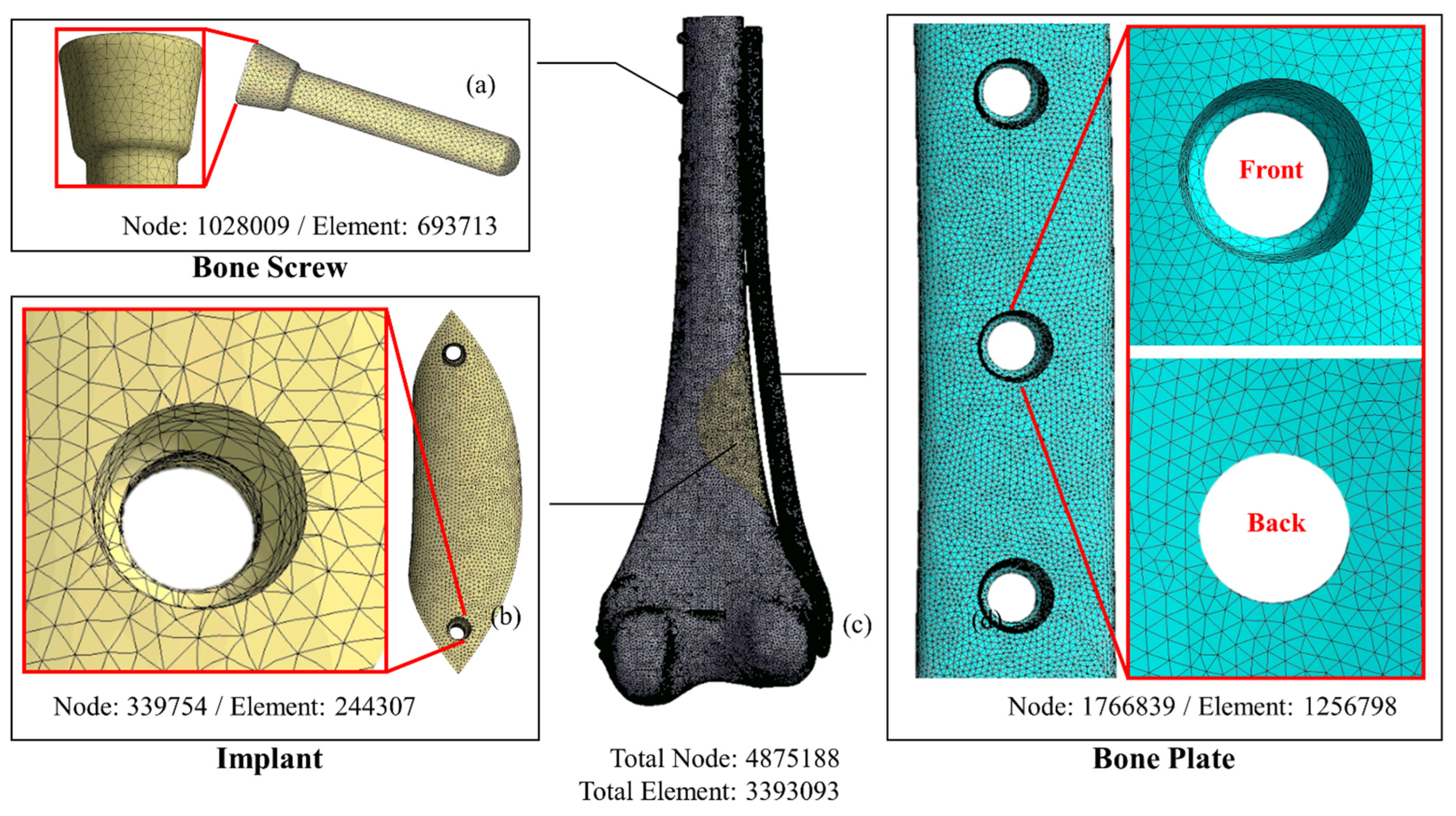
2.2. Implant Construction and Finite Element Analysis
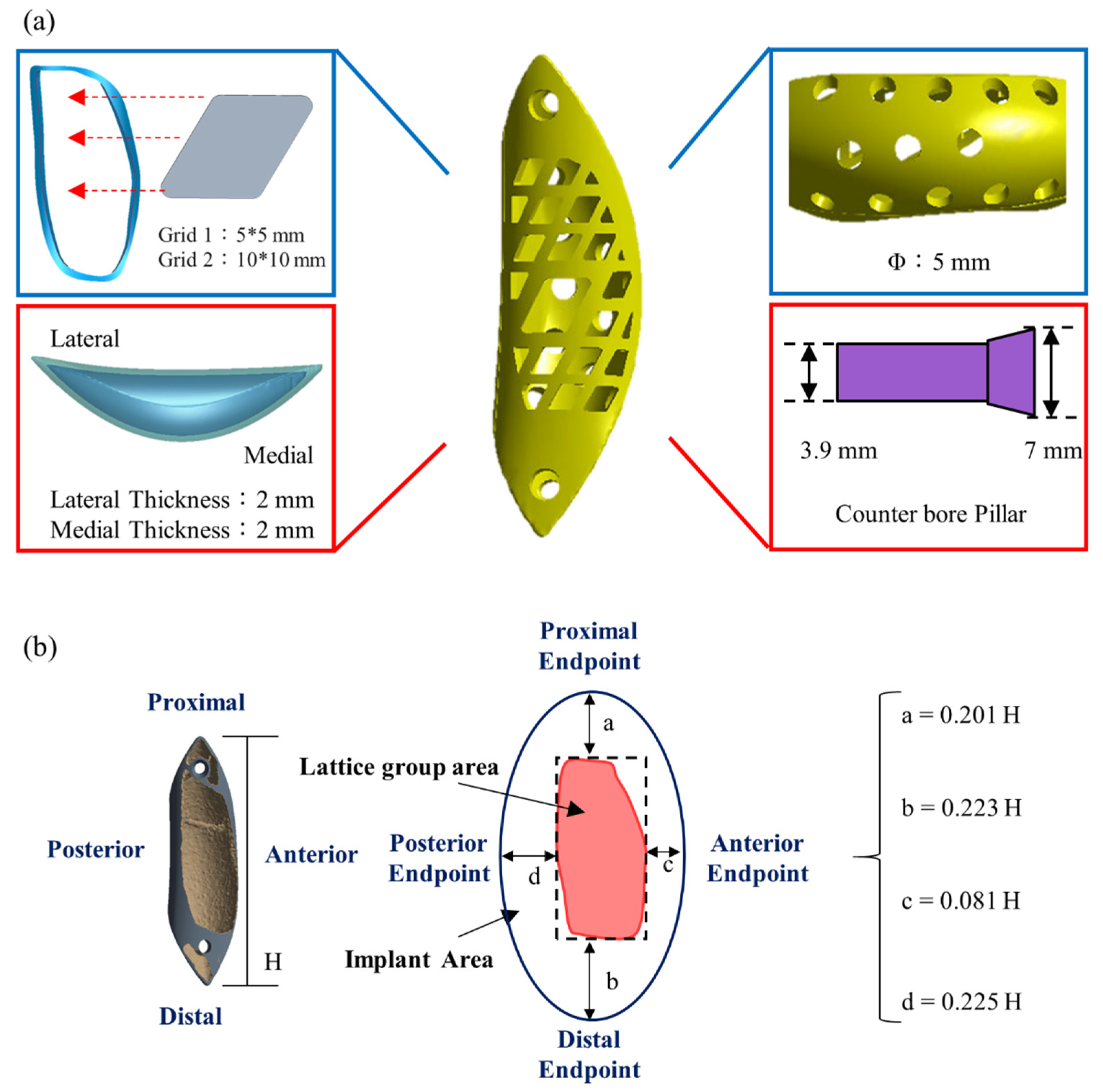
2.3. Topology Optimization and Biomechanical Analysis of the Implants
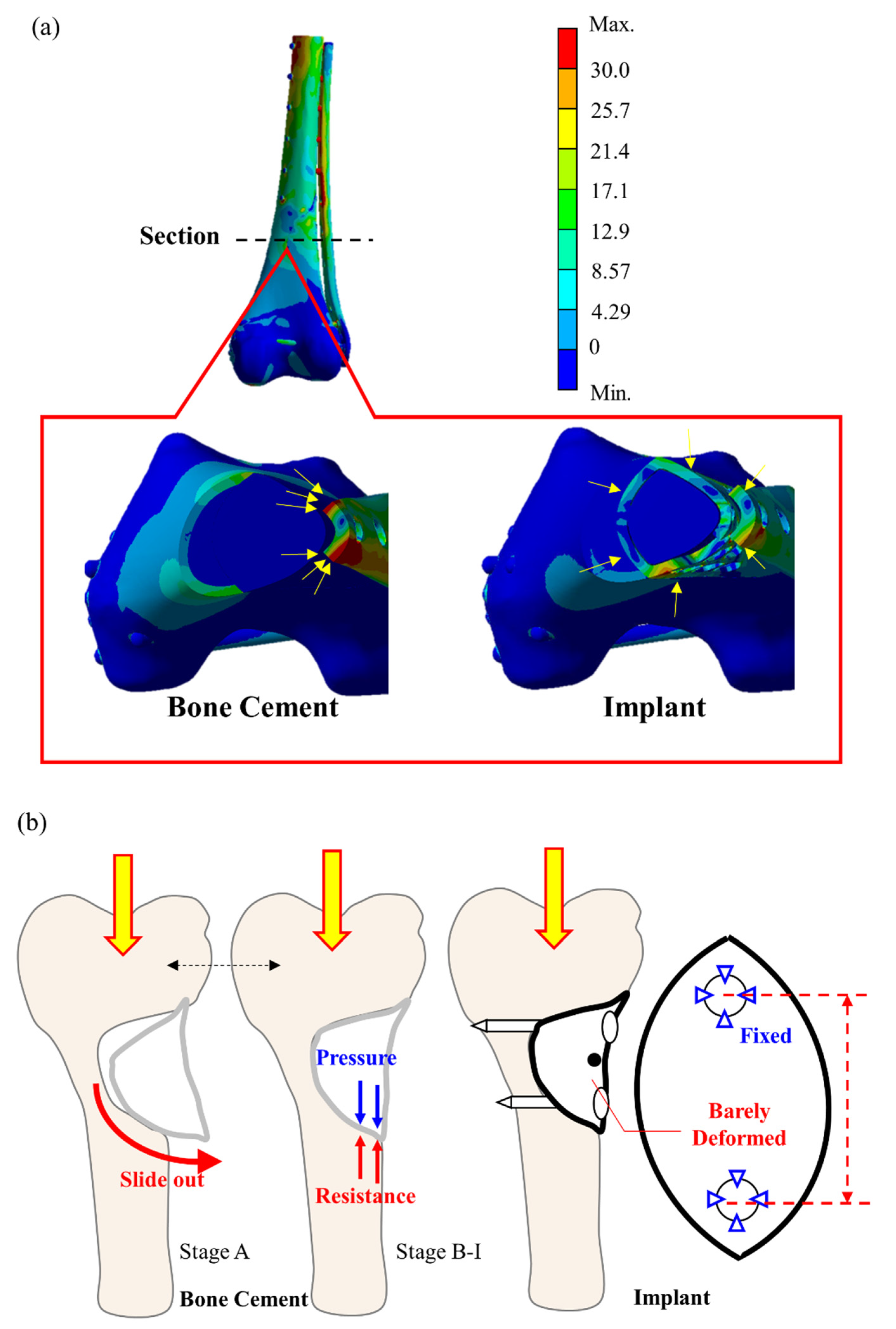
2.4. Comparison of Biomechanical Parameters between Femurs Repaired with the Bone Scaffold Implant and Bone Cement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hung, G.Y.; Yen, H.J.; Yen, C.C.; Wu, P.K.; Chen, C.F.; Chen, P.C.; Wu, H.H.; Chiou, H.J.; Chen, W.M. Improvement in High-Grade Osteosarcoma Survival: Results from 202 Patients Treated at a Single Institution in Taiwan. Medicine 2016, 95, e3420. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.K.; Chen, C.F.; Chen, C.M.; Cheng, Y.C.; Tsai, S.W.; Chen, T.H.; Chen, W.M. Intraoperative Extracorporeal Irradiation and Frozen Treatment on Tumor-bearing Autografts Show Equivalent Outcomes for Biologic Reconstruction. Clin. Orthop. Relat. Res. 2018, 476, 877–889. [Google Scholar] [CrossRef] [PubMed]
- Li, C.H.; Wu, C.H.; Lin, C.L. Design of a patient-specific mandible reconstruction implant with dental prosthesis for metal 3D printing using integrated weighted topology optimization and finite element analysis. J. Mech. Behav. Biomed. Mater. 2020, 105, 103700. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.H.; Chiang, M.C.; Hung, C.H.; Lin, S.C.; Chang, H.W. Finite element comparison of retrograde intramedullary nailing and locking plate fixation with/without an intramedullary allograft for distal femur fracture following total knee arthroplasty. Knee 2014, 21, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Completo, A.; Fonseca, F.; Simoes, J.A. Experimental validation of intact and implanted distal femur finite element models. J. Biomech. 2007, 40, 2467–2476. [Google Scholar] [CrossRef] [PubMed]
- Fontenot, P.B.; Diaz, M.; Stoops, K.; Barrick, B.; Santoni, B.; Mir, H. Supplementation of Lateral Locked Plating for Distal Femur Fractures: A Biomechanical Study. J. Orthop. Trauma 2019, 33, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Fernandez de Grado, G.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone substitutes: A review of their characteristics, clinical use, and perspectives for large bone defects management. J. Tissue Eng. 2018, 9, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanke, A.; Baumlein, M.; Lang, S.; Gueorguiev, B.; Nerlich, M.; Perren, T.; Rillmann, P.; Ryf, C.; Miclau, T.; Loibl, M. Long-term radiographic appearance of calcium-phosphate synthetic bone grafts after surgical treatment of tibial plateau fractures. Injury 2017, 48, 2807–2813. [Google Scholar] [CrossRef] [PubMed]
- Mnaymneh, W.; Malinin, T.I.; Lackman, R.D.; Hornicek, F.J.; Ghandur-Mnaymneh, L. Massive distal femoral osteoarticular allografts after resection of bone tumors. Clin. Orthop. Relat. Res. 1994, 303, 103–115. [Google Scholar] [CrossRef]
- Wong, K.C. 3D-printed patient-specific applications in orthopedics. Orthop. Res. Rev. 2016, 8, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuah, H.G.; Abd Rahim, I.; Yusof, M.I. Topology optimisation of spinal interbody cage for reducing stress shielding effect. Comput. Methods Biomech. Biomed. Engin. 2010, 13, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Tetsworth, K.; Block, S.; Glatt, V. Putting 3D modelling and 3D printing into practice: Virtual surgery and preoperative planning to reconstruct complex post-traumatic skeletal deformities and defects. SICOT J. 2017, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.W.; Wu, C.D.; Chien, C.-S.; Lee, C.-W.; Yang, T.-H.; Lin, C.-L. Patient-specific 3-dimensional printing titanium implant biomechanical evaluation for complex distal femoral open fracture reconstruction with segmental large bone defect: A nonlinear finite element analysis. Appl. Sci. 2020, 10, 4098. [Google Scholar] [CrossRef]
- Lin, C.L.; Wang, Y.T.; Chang, C.M.; Wu, C.H.; Tsai, W.H. Design Criteria for Patient-specific Mandibular Continuity Defect Reconstructed Implant with Lightweight Structure using Weighted Topology Optimization and Validated with Biomechanical Fatigue Testing. Int. J. Bioprint. 2022, in press. [Google Scholar]
- Wallace, N.; Schaffer, N.E.; Aleem, I.S.; Patel, R. 3D-printed Patient-specific Spine Implants: A Systematic Review. Clin. Spine Surg 2020, 33, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Bendsøe, M.P.; Sigmund, O. Topology Optimization-Theory, Methods, and Applications; Springer: Berlin/Heidelberg, Germany, 2003. [Google Scholar]
- Sutradhar, A.; Park, J.; Carrau, D.; Nguyen, T.H.; Miller, M.J.; Paulino, G.H. Designing patient-specific 3D printed craniofacial implants using a novel topology optimization method. Med. Biol. Eng. Comput. 2016, 54, 1123–1135. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, T.; Wang, L.; Li, D.; Dong, E.; Fan, H.; Fu, J.; Hu, C. A general multi-objective topology optimization methodology developed for customized design of pelvic prostheses. Med. Eng. Phys. 2019, 69, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Chen, H.; Liu, Y.; Wu, N.; Chen, B.; Zhao, X.; Han, Q.; Wang, J. Customized reconstructive prosthesis design based on topological optimization to treat severe proximal tibia defect. Biodes. Manuf. 2021, 4, 87–99. [Google Scholar] [CrossRef]
- Tilton, M.; Lewis, G.S.; Manogharan, G.P. Additive Manufacturing of Orthopedic Implants. In Orthopedic Biomaterials; Li, B., Webster, T., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Kharmanda, G. Integration of multi-objective structural optimization into cementless hip prosthesis design: Improved Austin-Moore model. Comput. Methods Biomech. Biomed. Engin. 2016, 19, 1557–1566. [Google Scholar] [CrossRef] [PubMed]
- Kaku, N.; Hara, K.; Tabata, T.; Tsumura, H. Influence of the volume of bone defect, bone grafting methods, and hook fixation on stress on the Kerboull-type plate and screw in total hip arthroplasty: Three-dimensional finite element analysis. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 321–329. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Young’s Modulus (GPa) | Poisson’s Ratio | Reference |
|---|---|---|---|
| Cortical Bone | 12.4 | 0.3 | [13] |
| Cancellous Bone | 0.104 | 0.3 | [13] |
| Ti6Al4V | 114 | 0.34 | [13] |
| Bone Cement | 2.65 | 0.455 | [21] |
| Bone Graft | 1 | 0.45 | [22] |
| Phase | Loading (100% BW) | Number of Cycles | Frequency (Hz) |
|---|---|---|---|
| A | 0.5–1.0 | 20,000 | 2 |
| B | 0.5–1.5 | 20,000 | 2 |
| C | 0.5–2.0 | 20,000 | 2 |
| D | 0.5–2.5 | 20,000 | 2 |
| E | 0.5–3.0 | 20,000 | 2 |
| F | 0.5–3.5 | 20,000 | 2 |
| G | 0.5–4.0 | 20,000 | 2 |
| H | 0.5–4.5 | 20,000 | 2 |
| I | 0.5–5.0 | 20,000 | 2 |
| Group | Total Deformation (mm) | % Error Relative to Solid Implant | Bone Plate Von-Mises Stress (MPa) | % Error Relative to Solid Implant | Bone Maximum First Principal Stress (MPa) | % Error Relative to Solid Implant | Bone Maximum First Principal Strain (µm/m) | % Error Relative to Solid Implant |
|---|---|---|---|---|---|---|---|---|
| Solid-core Implant | 2.039 | - | 310.2 | - | 38.15 | - | 2903 | - |
| Shell cavity Implant | 2.052 | 0.6% | 335.2 | 8% | 41.58 | 9% | 3089 | 6%3 |
| Bone scaffold implant | 2.061 | 1% | 313.0 | 1% | 40.14 | 5% | 2804 | 3% |
| Bone Cement | 2.309 | 12% | 420.1 | 34% | 53.50 | 33% | 3711 | 32% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, P.-K.; Lee, C.-W.; Sun, W.-H.; Lin, C.-L. Biomechanical Analysis and Design Method for Patient-Specific Reconstructive Implants for Large Bone Defects of the Distal Lateral Femur. Biosensors 2022, 12, 4. https://doi.org/10.3390/bios12010004
Wu P-K, Lee C-W, Sun W-H, Lin C-L. Biomechanical Analysis and Design Method for Patient-Specific Reconstructive Implants for Large Bone Defects of the Distal Lateral Femur. Biosensors. 2022; 12(1):4. https://doi.org/10.3390/bios12010004
Chicago/Turabian StyleWu, Po-Kuei, Cheng-Wei Lee, Wei-Hsiang Sun, and Chun-Li Lin. 2022. "Biomechanical Analysis and Design Method for Patient-Specific Reconstructive Implants for Large Bone Defects of the Distal Lateral Femur" Biosensors 12, no. 1: 4. https://doi.org/10.3390/bios12010004
APA StyleWu, P.-K., Lee, C.-W., Sun, W.-H., & Lin, C.-L. (2022). Biomechanical Analysis and Design Method for Patient-Specific Reconstructive Implants for Large Bone Defects of the Distal Lateral Femur. Biosensors, 12(1), 4. https://doi.org/10.3390/bios12010004