
Biocompatibility of Subperiosteal Dental Implants: Changes in the Expression of Osteogenesis-Related Genes in Osteoblasts Exposed to Differently Treated Titanium Surfaces

 , ,
, ,  and
and 
Abstract

1. Introduction
2. Materials and Methods
2.1. TiO2 Samples and Surface Treatments
2.2. Cell Culture
2.3. Cell Viability Assay
2.4. Alizarin Red Assay
2.5. Gene Expression of Osteoblast Mineralization Markers
2.6. Expression of Osteoblast Adhesion and Mineralization Markers
2.7. Release of Osteoprotegerin (OPG)
2.8. Statistical Analysis
3. Results
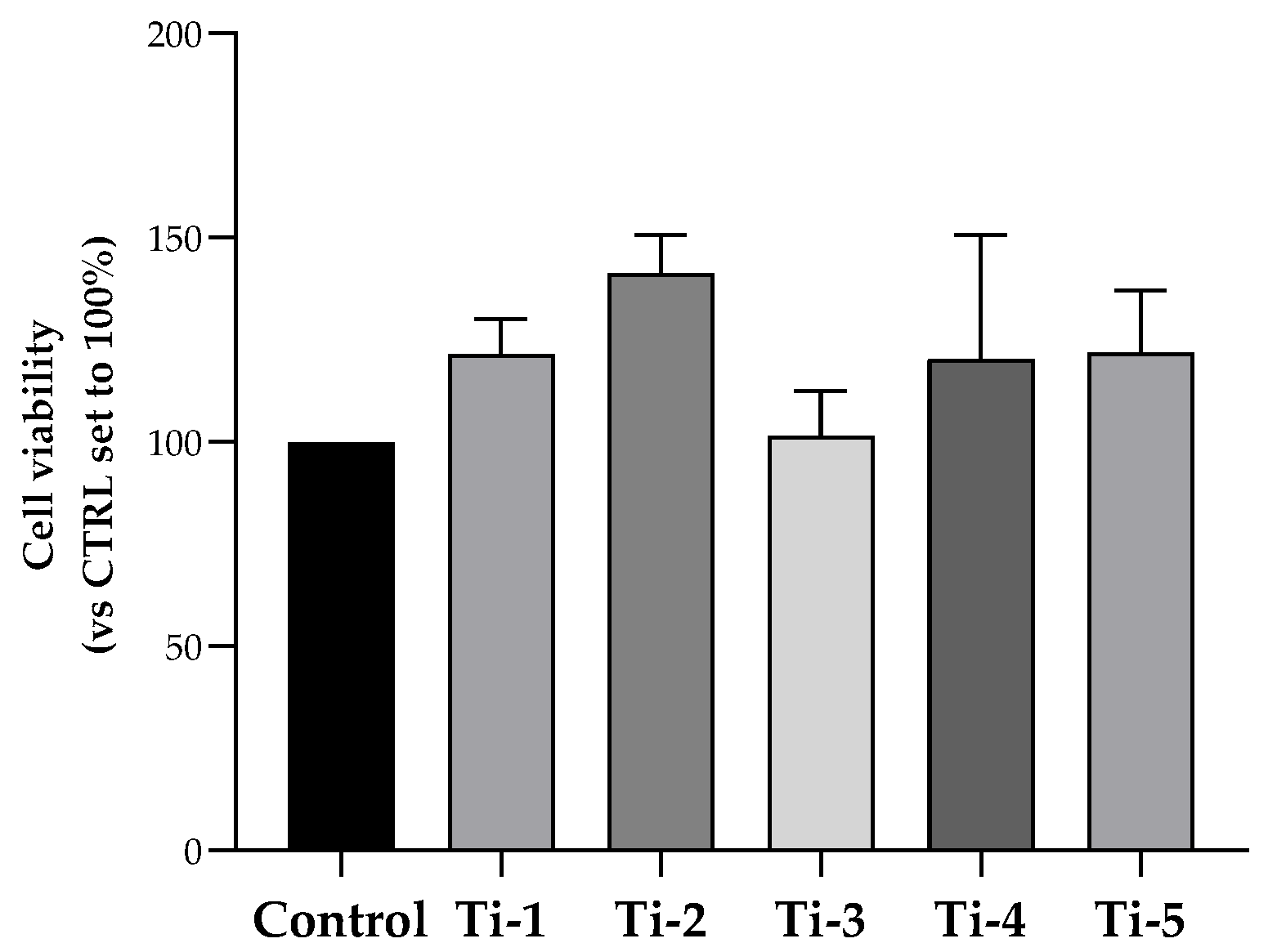
3.1. Evaluation of HOB Viability
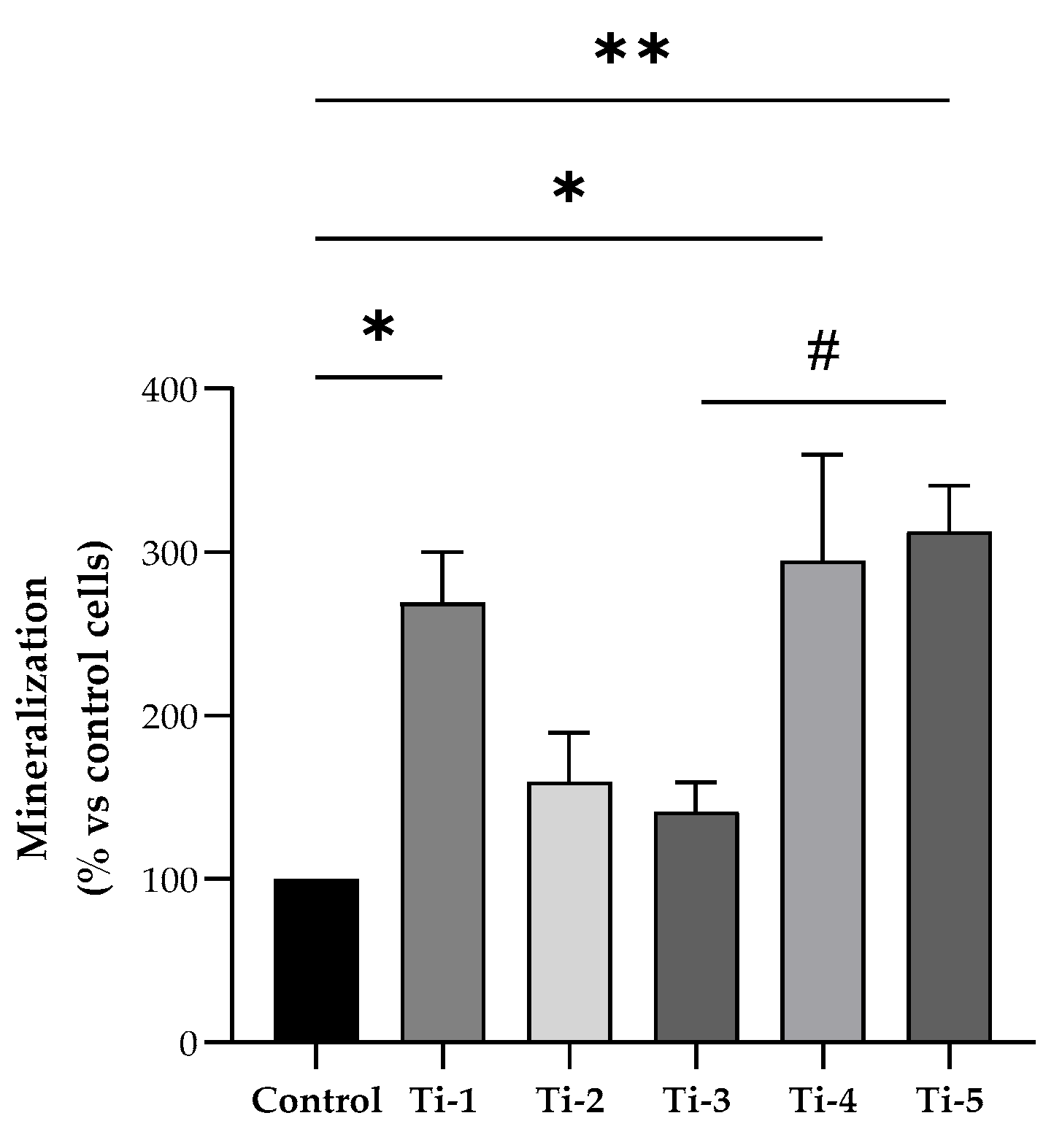
3.2. Evaluation of Mineralization
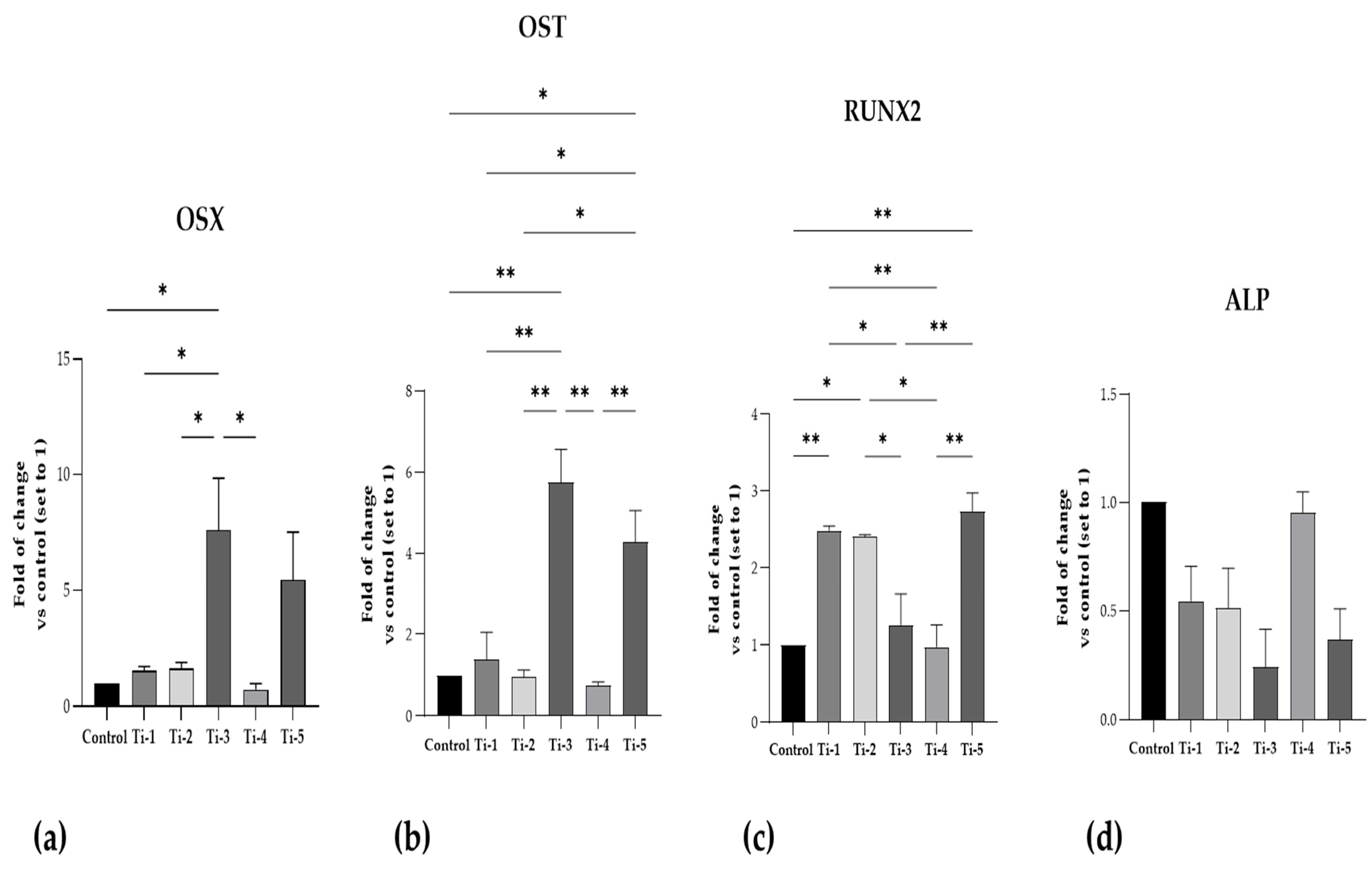
3.3. Evaluation of Osteoblast Adhesion and Mineralization Markers
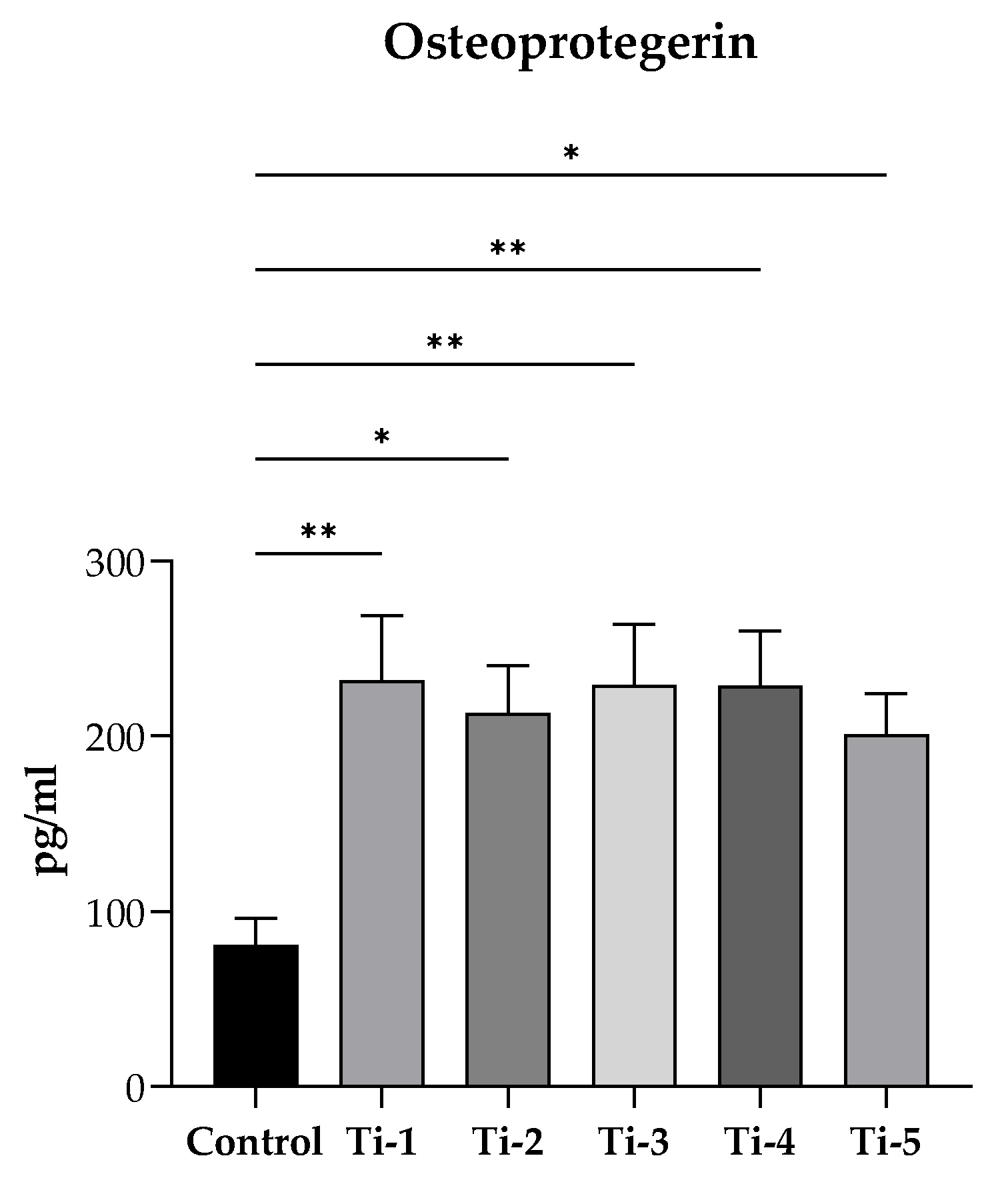
3.4. Evaluation of OPG Release
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Esposito, M.; Grusovin, M.G.; Felice, P.; Karatzopoulos, G.; Worthington, H.V.; Coulthard, P. The efficacy of horizontal and vertical bone augmentation procedures for dental implants—A Cochrane systematic review. Eur. J. Oral Implant. 2009, 2, 167–184. [Google Scholar] [CrossRef]
- Silvestri, K.D.; Carlotti, A.E. Subperiosteal implant: Serving the dental profession for over 50 years. Rhode Isl. Dent. J. 1995, 28, 11–23. [Google Scholar]
- Linkow, L.I.; Wagner, J.R.; Chanavaz, M. Tripodal mandibular subperiosteal implant: Basic sciences, operational procedures, and clinical data. J. Oral Implant. 1998, 24, 16–36. [Google Scholar] [CrossRef]
- Schou, S.; Pallesen, L.; Hjørting-Hansen, E.; Pedersen, C.S.; Fibæk, B. A 41-year history of a mandibular subperiosteal implant. Clin. Oral Impl. Res. 2000, 11, 171–178. [Google Scholar] [CrossRef]
- van Noort, R. The future of dental devices is digital. Dent. Mat. 2012, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative in vitro study. BMC Oral Health 2017, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef] [PubMed]
- Cerea, M.; Dolcini, G.A. Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants: A Retrospective Clinical Study on 70 Patients. BioMed Res. Int. 2018, 2018, 5420391. [Google Scholar] [CrossRef] [PubMed]
- Naujokat, H.; Gökkaya, A.I.; Açil, Y.; Loger, K.; Klüter, T.; Fuchs, S.; Wiltfang, J. In vivo biocompatibility evaluation of 3D-printed nickel-titanium fabricated by selective laser melting. J. Mater. Sci. Mater. Med. 2022, 33, 13. [Google Scholar] [CrossRef]
- Roy, M.; Corti, A.; Dominici, S.; Pompella, A.; Cerea, M.; Chelucci, E.; Dorocka-Bobkowska, B.; Daniele, S. Biocompatibility of Subperiosteal Dental Implants: Effects of Differently Treated Titanium Surfaces on the Expression of ECM-Related Genes in Gingival Fibroblasts. J. Funct. Biomat. 2023, 14, 59. [Google Scholar] [CrossRef]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Prakoso, A.T.; Basri, H.; van der Heide, E. Computational Contact Pressure Prediction of CoCrMo, SS 316L and Ti6Al4V Femoral Head against UHMWPE Acetabular Cup under Gait Cycle. J. Funct. Biomater. 2022, 13, 64. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.W. Titanium Alloys for Dental Implants: A Review. Prosthesis 2020, 2, 100–116. [Google Scholar] [CrossRef]
- Daniele, S.; Lecca, D.; Trincavelli, M.L.; Ciampi, O.; Abbracchio, M.P.; Martini, C. Regulation of PC12 cell survival and differentiation by the new P2Y-like receptor GPR17. Cell Signal. 2010, 22, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Daniele, S.; Da Pozzo, E.; Zappelli, E.; Martini, C. Trazodone treatment protects neuronal-like cells from inflammatory insult by inhibiting NF-κB, p38 and JNK. Cell Signal. 2015, 27, 1609–1629. [Google Scholar] [CrossRef] [PubMed]
- Daniele, S.; Natali, L.; Giacomelli, C.; Campiglia, P.; Novellino, E.; Martini, C.; Trincavelli, M.L. Osteogenesis Is Improved by Low Tumor Necrosis Factor Alpha Concentration through the Modulation of Gs-Coupled Receptor Signals. Mol. Cell Biol. 2017, 37, e00442-16. [Google Scholar] [CrossRef]
- Daniele, S.; Giacomelli, C.; Pietrobono, D.; Barresi, E.; Piccarducci, R.; La Pietra, V.; Taliani, S.; Da Settimo, F.; Marinelli, L.; Novellino, E.; et al. Long lasting inhibition of Mdm2-p53 interaction potentiates mesenchymal stem cell differentiation into osteoblasts. Biochim. Biophys. Acta Mol. Cell Res. 2019, 1866, 737–749. [Google Scholar] [CrossRef] [PubMed]
- Trincavelli, M.L.; Daniele, S.; Giacomelli, C.; Taliani, S.; Da Settimo, F.; Cosimelli, B.; Greco, G.; Novellino, E.; Martini, C. Osteoblast differentiation and survival: A role for A2B adenosine receptor allosteric modulators. Biochim. Biophys. Acta (BBA) Mol. Cell Res. 2014, 1843, 2957–2966. [Google Scholar] [CrossRef]
- Babuska, V.; Moztarzadeh, O.; Kubikova, T.; Moztarzadeh, A.; Hrusak, D.; Tonar, Z. Evaluating the osseointegration of nanostructured titanium implants in animal models: Current experimental methods and perspectives (Review). Biointerphases 2016, 11, 030801. [Google Scholar] [CrossRef] [PubMed]
- Herce-López, J.; Pingarrón, M.d.C.; Tofé-Povedano, Á.; García-Arana, L.; Espino-Segura-Illa, M.; Sieira-Gil, R.; Rodado-Alonso, C.; Sánchez-Torres, A.; Figueiredo, R. Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review. Biomimetics 2024, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Gröbe, A.; Heiland, M.; Ebker, T. Impact of Dental Implant Surface Modifications on Osseointegration. BioMed Res. Int. 2016, 2016, 6285620. [Google Scholar] [CrossRef]
- Pandey, C.; Rokaya, D.; Bhattarai, B.P. Contemporary concepts in osseointegration of dental implants: A review. BioMed Res. Int. 2022, 2022, 6170452. [Google Scholar] [CrossRef]
- Kim, T.I.; Jang, J.H.; Kim, H.W.; Knowles, J.C.; Ku, Y. Biomimetic approach to dental implants. Curr. Pharm. Des. 2008, 14, 2201–2211. [Google Scholar] [CrossRef] [PubMed]
- Tetè, S.; Mastrangelo, F.; Quaresima, R.; Vinci, R.; Sammartino, G.; Stuppia, L.; Gherlone, E. Influence of Novel Nano-Titanium Implant Surface on Human Osteoblast Behavior and Growth. Implant Dent. 2010, 19, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Jensen, E.D.; Gopalakrishnan, R.; Westendorf, J.J. Regulation of gene expression in osteoblasts. Biofactors 2010, 36, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Z.; Duan, N.; Zhu, G.; Schwarz, E.M.; Xie, C. Osteoblast–osteoclast interactions. Connect. Tissue Res. 2018, 59, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Cochran, D.L.; Schenk, R.K.; Lussi, A.; Higginbottom, F.L.; Buser, D. Bone response to unloaded and loaded titanium implants with a sandblasted and acid-etched surface: A histometric study in the canine mandible. J. Biomed. Mater. Res. 1998, 40, 1–11. [Google Scholar] [CrossRef]
- Cooper, L.F. A role for surface topography in creating and maintaining bone at titanium endosseous implants. J. Prosthet. Dent. 2000, 84, 522–534. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Wang, X.; Zhang, N. Microrough surface of metallic biomaterials: A literature review. Bio-Med. Mater. Eng. 1996, 6, 173–189. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontology 2000 2017, 73, 22–40. [Google Scholar] [CrossRef]
- Ottria, L.; Lauritano, D.; Bassi, M.; Palmieri, A.; Candotto, V.; Tagliabue, A.; Tettamanti, L. Mechanical, chemical and biological aspects of titanium and titanium alloys in implant dentistry. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. S1), 81–90. [Google Scholar]
- Rodriguez, R.; Kim, K.; Ong, J.L. In vitro osteoblast response to anodized titanium and anodized titanium followed by hydrothermal treatment. J. Biomed. Mater. Res. Part A Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2003, 65, 352–358. [Google Scholar] [CrossRef]
- Westendorf, J.J.; Kahler, R.A.; Schroeder, T.M. Wnt signaling in osteoblasts and bone diseases. Gene 2004, 341, 19–39. [Google Scholar] [CrossRef]
- Anselme, K. Osteoblast adhesion on biomaterials. Biomaterials 2000, 21, 667–681. [Google Scholar] [CrossRef]
- Atkins, G.J.; Kostakis, P.; Pan, B.; Farrugia, A.; Gronthos, S.; Evdokiou, A.; Harrison, K.; Findlay, M.D.; Zannettino, A.C. RANKL expression is related to the differentiation state of human osteoblasts. J. Bone Min. Res. 2003, 18, 1088–1098. [Google Scholar] [CrossRef]
- Hartmann, C. A Wnt canon orchestrating osteoblastogenesis. Trends Cell Biol. 2006, 16, 151–158. [Google Scholar] [CrossRef]
- Gori, F.; Hofbauer, L.C.; Dunstan, C.R.; Spelsberg, T.C.; Khosla, S.; Riggs, B.L. The expression of osteoprotegerin and RANK ligand and the support of osteoclast formation by stromal-osteoblast lineage cells is developmentally regulated. Endocrinology 2000, 141, 4768–4776. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acronym | Treatment |
|---|---|
| Ti-1 | raw machined |
| Ti-2 | electropolished with an acid mixture |
| Ti-3 | sand-blasted (corundum) + acid-etched |
| Ti-4 | new colored AlTiColorTM surface (proprietary procedure) |
| Ti-5 | Anodized |
| Gene | Primer Nucleotide Sequences | Annealing Temperature |
|---|---|---|
| RUNX2 | F: 5′-GGCCCTGGTGTTTAAATGGT3′ R: 5′-AGGCTGTTTGACGCCATAGT-3′ | 55 °C |
| OST | F: 5′-CTGCAAGGACATCGCCTATC-3′ R: 5′-CATCAGTTCTGTTCTTGGGGTA-3′ | 55 °C |
| OSX | F: 5′-TCCCTGCTTGAGGAGGAAG-3′ R: 5′-AAAGGTCACTGCCCACAGAG-3′ | 55 °C |
| ALP | F: 5′-CTGCAAGGACATCGCCTATC-3′ R: 5′-CATCAGTTCTGTTCTTGGGGTA-3′ | 55 °C |
| β-actin | F: 5′-GCACTCTTCCAGCCTTCCTTCC-3′ R: 5′-GAGCCGCCGATCCACACG -3′ | 55 °C |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roy, M.; Chelucci, E.; Corti, A.; Ceccarelli, L.; Cerea, M.; Dorocka-Bobkowska, B.; Pompella, A.; Daniele, S. Biocompatibility of Subperiosteal Dental Implants: Changes in the Expression of Osteogenesis-Related Genes in Osteoblasts Exposed to Differently Treated Titanium Surfaces. J. Funct. Biomater. 2024, 15, 146. https://doi.org/10.3390/jfb15060146
Roy M, Chelucci E, Corti A, Ceccarelli L, Cerea M, Dorocka-Bobkowska B, Pompella A, Daniele S. Biocompatibility of Subperiosteal Dental Implants: Changes in the Expression of Osteogenesis-Related Genes in Osteoblasts Exposed to Differently Treated Titanium Surfaces. Journal of Functional Biomaterials. 2024; 15(6):146. https://doi.org/10.3390/jfb15060146
Chicago/Turabian StyleRoy, Marco, Elisa Chelucci, Alessandro Corti, Lorenzo Ceccarelli, Mauro Cerea, Barbara Dorocka-Bobkowska, Alfonso Pompella, and Simona Daniele. 2024. "Biocompatibility of Subperiosteal Dental Implants: Changes in the Expression of Osteogenesis-Related Genes in Osteoblasts Exposed to Differently Treated Titanium Surfaces" Journal of Functional Biomaterials 15, no. 6: 146. https://doi.org/10.3390/jfb15060146
APA StyleRoy, M., Chelucci, E., Corti, A., Ceccarelli, L., Cerea, M., Dorocka-Bobkowska, B., Pompella, A., & Daniele, S. (2024). Biocompatibility of Subperiosteal Dental Implants: Changes in the Expression of Osteogenesis-Related Genes in Osteoblasts Exposed to Differently Treated Titanium Surfaces. Journal of Functional Biomaterials, 15(6), 146. https://doi.org/10.3390/jfb15060146