Transcultural Adaptation and Psychometric Properties of Portuguese Version of the Spiritual Needs Questionnaire (SpNQ) Among HIV Positive Patients in Brazil

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Questionnaire and Translation Process
- Religious Needs (Cronbach’s alpha = 0.92), e.g., praying for and with others, praying alone, participating in a religious ceremony, reading spiritual/religious books, turning to a higher presence (e.g., God, angels);
- Existential Needs (Reflection/Meaning) (alpha = 0.82), e.g., reflecting on one’s life, talking with someone about the meaning of life/suffering, resolving open aspects in life, talking about the possibility of life after death, etc.;
- Need for Inner Peace (alpha = 0.82), e.g., wish to dwell in places of quietness and peace, plunge into the beauty of nature, finding inner peace, talking with others about fears and worries, turning to someone in a loving attitude;
- Need for Active Giving/Generativity (alpha = 0.74), e.g., active and autonomous intention to provide solace to someone, passing along one’s own life experiences to others, and to be assured that life was meaningful and of value.
- Step 1:Translation of the 27-item English version into Portuguese by two bilingual professionals, aware of the objectives of the study, resulting in two Portuguese versions of SpNQ.
- Step 2:The versions were compared by another bilingual researcher, resulting in a reconciled version in Portuguese.
- Step 3:The reconciled version was translated back into English by two other bilingual professionals, and the versions were compared by another bilingual researcher, resulting in an SpNQ reconciled version in English.
- Step 4:The English and Portuguese versions were sent to the author of the instrument for review and approval.
- Step 5:The final version was approved by the author and was revised for Portuguese grammar, punctuation and formatting, obtaining a translated version of SpNQ for the pre-test.
- Step 6:The translated instrument was presented to 26 outpatients in 4 Brazilian health services, and individual interviews were conducted with each of them to identify problems in understanding the instrument’s questions, obtaining the 27-item SpNQ Portuguese final version (27 SpNQ-BR).
2.3. Statistical Analyses
3. Results
3.1. Participants
3.2. Validation of the Questionnaire
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Büssing, Arndt. 2015. Spirituality/Religiosity as a Resource for Coping in Soldiers: A Summary Report. Medical Acupuncture 27: 360–66. [Google Scholar] [CrossRef]
- Büssing, Arndt, Hans-Joachim Balzat, and Peter Heusser. 2009. Spirituelle Bedürfnisse von Patienten mit chronischen Schmerz- und Tumorerkrankungen. Perioperative Medizin 1: 248. [Google Scholar] [CrossRef]
- Büssing, Arndt, Hans-Joachim Balzat, and Peter Heusser. 2010. Spiritual needs of patients with chronic pain diseases and cancer—Validation of the spiritual needs questionnaire. European Journal of Medical Research 15: 266–73. Available online: https://www.ncbi.nlm.nih.gov/pubmed/20696636 (accessed on 19 February 2018).
- Büssing, Arndt, J. Janko, Andreas Kopf, Eberhard Lux, and Eckhard Frick. 2012. Zusammenhänge zwischen psychosozialen und spirituellen Bedürfnissen und Bewertung von Krankheit bei Patienten mit chronischen Erkrankungen. Spiritual Care 1: 57–73. [Google Scholar]
- Büssing, Arndt, Xiao-Feng Zhai, Wen-Bo Peng, and Chang-Quan Ling. 2013. Validation of the Chinese Version of the Spiritual Needs Questionnaire. Journal of Integrative Medicine 11: 106–15. [Google Scholar] [CrossRef] [PubMed]
- Büssing, Arndt, Klaus Baumann, Niels Christian Hvidt, Harold G. Koenig, Christina M. Puchalski, and John Swinton. 2014. Spirituality and Health. Evidence-Based Complementary and Alternative Medicine 2014: 682817. [Google Scholar] [CrossRef] [PubMed]
- Büssing, Arndt, Iwona Pilchowska, and Janusz Surzykiewicz. 2015. Spiritual Needs of Polish Patients with Chronic Diseases. Journal of Religion and Health 54: 1524–42. [Google Scholar] [CrossRef]
- Büssing, Arndt, Tânia Cristina de Oliveira Valente, Ana Paula Rodrigues Cavalcanti, Anderson Luís Carvalho Tarocco Jr., and Daniela Rodrigues Recchia. 2016. Brazilian Transcultural of Patient’s Spiritual Needs Questionnaire. Paper presented at 5th European Conference on Religion, Spirituality and Health and 4th International Conference of the British Association for the Study of Spirituality, Gdansk, Poland, May 12–14. [Google Scholar]
- Büssing, Arndt, Daniela Rodrigues Recchia, Harold Koenig, Klaus Baumann, and Eckhard Frick. 2018. Factor Structure of the Spiritual Needs Questionnaire (SpNQ) in Persons with Chronic Diseases, Elderly and Healthy Individuals. Religions 9: 13. [Google Scholar] [CrossRef]
- Coleman, Christopher Lance, Jeanne K. Kemppainen, William L. Holzemer, Lucille Sanzero Eller, Inge Corless, Nancy Reynolds, Kathleen M. Nokes, Pam Dole, Kenn Kirksey, Liz Seficik, and et al. 2006. Gender Differences in Use of Prayer as a Self-Care Strategy for Managing Symptoms in African Americans Living with HIV/AIDS. Journal of the Association of Nurses in AIDS Care 17: 16–23. Available online: https://www.ncbi.nlm.nih.gov/pubmed/16849085 (accessed on 19 February 2018). [CrossRef] [PubMed]
- De Andrade, Maristela Oliveira. 2009. Brazilian Religiosity: Religious Pluralism, Diversity of Beliefs and the Syncretic Process. CAOS-Revista Eletrônica de Ciências Sociais 14: 106–18. Available online: http://www.cchla.ufpb.br/caos/n14/6A%20religiosidade%20brasileira.pdf (accessed on 19 February 2018).
- Glavas, Andrijana, Karin Jors, Arndt Büssing, and Klaus Baumann. 2017. Spiritual Needs of PTSD Patients in Croatia and Bosnia-Herzegovina: A Quantitative Pilot Study. Psychiatria Danubina 29: 282–90. [Google Scholar] [CrossRef] [PubMed]
- Hatamipour, Khadijeh, Maryam Rassouli, Farideh Yaghmaie, Kazem Zendedel, and Hamid Alavi Majd. 2018. Development and Psychometrics of a ‘Spiritual Assessment Scale of Patients with Cancer’: A Mixed Exploratory Study. International Journal of Cancer Management 11: e10083. Available online: http://dx.doi.org/10.5812/ijcm.10083 (accessed on 25 January 2018). [CrossRef]
- Kemppainen, Jeanne, Lucille Sanzero Eller, Eli Haugen Bunch, Mary J. Hamilton, Pamela J. Dole, William L. Holzemer, Kenn Kirksey, Patrice K. Nicholas, Inge Corless, Christopher Lance Coleman, and et al. 2006. Strategies for Self-Management of HIV-Related Anxiety. AIDS Care 18: 597–607. [Google Scholar] [CrossRef] [PubMed]
- Koenig, Harold G. 2015. Religion, Spirituality, and Health: A Review and Update. Advances 29: 11–18. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26026153 (accessed on 19 February 2018).
- Nejat, Nazi, Lisa Whitehead, and Marie Crowe. 2016. Exploratory Psychometric Properties of the Farsi and English Versions of the Spiritual Needs Questionnaire (SpNQ). Religions 7: 84. [Google Scholar] [CrossRef]
- Nuraeni, Aan, Ikeu Nurhidayah, Nuroktavia Hidayati, Citra Windani Mambang Sari, and Ristina Mirwanti. 2015. Kebutuhan Spiritual pada Pasien Kanker. Jurnal Keperawatan Padjadjaran 3: 57–66. Available online: http://jkp.fkep.unpad.ac.id/index.php/jkp/article/view/101 (accessed on 2 February 2018). [CrossRef]
- Offenbaecher, M., N. Kohls, L. L. Toussant, C. Sigl, A. Winkelmann, R. Hieblinger, A. Whalter, and A. Büssing. 2013. Spiritual Needs in Patients Suffering from Fibromyalgia. Evidence-Based Complementary and Alternative Medicine 2013: 178547. Available online: http://dx.doi.org/10.1155/2013/178547 (accessed on 25 January 2018). [CrossRef] [PubMed]
- Puchalski, Christina M., Robert Vitillo, Sharon K. Hull, and Nancy Reller. 2014. Improving the Spiritual Dimension of Whole Person Care: Reaching National and International Consensus. Journal of Palliative Medicine 17: 642–65. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24842136 (accessed on 19 February 2018). [CrossRef] [PubMed]
- Puchalski, Christina M., Robert J. Vitillo, and Najmeh Jafari. 2016. Global Network for Spirituality and Health (GNSAH): Seeking More Compassionate Health Systems. Journal for the Study of Spirituality 1: 106–12. [Google Scholar] [CrossRef]
- Tuck, Inez, Nancy L. McCain, and Ronald K. Elswick Jr. 2001. Spirituality and psychosocial factors in persons living with HIV. Journal of Advanced Nursing 33: 776–83. [Google Scholar] [CrossRef] [PubMed]
- Valente, Tânia Cristina de Oliveira, Cavalcanti Ana Paula Rodrigues, Büssing Arndt, and Clóvis Pereira Costa Júnior. 2018. Transcultural adaptation and psychometric properties of Portuguese version of the Spiritual Needs Questionnaire among people living with HIV in Brazil. Paper presented at 6th European Conference on Religion, Spirituality and Health and 5th International Conference of the British Association for the Study of Spirituality, Coventry, UK, May 17–19. forthcoming. [Google Scholar]
- Van Wyngaard, Arnau. 2013. Addressing the Spiritual Needs of People Infected with and Affected by HIV and AIDS in Swaziland. Journal of Social Work in End-of-Life & Palliative Care 9: 226–40. [Google Scholar]
- World Health Organization. 1998. WHOQOL and Spirituality, Religiousness and Personal Beliefs (SRPB)—Report on WHO Consultation. WHO/MSA/MHP/98.2, 2-23. Geneva: WHO. [Google Scholar]
- World Health Organization (WHO). 2014. Process of Translation and Adaptation of Instruments. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 19 February 2018).

{kind=link}
| Participants Characteristics | N | % |
|---|---|---|
| GENDER | ||
| Male | 114 | 57 |
| Female | 82 | 41 |
| Other | 4 | 2 |
| AGE | ||
| Less than 29 year | 60 | 30 |
| 30–49 year | 114 | 57 |
| 50–70 year | 26 | 13 |
| EDUCATIONAL STATUS | ||
| Primary School Complete | 6 | 3 |
| High School Incomplete | 67 | 33.5 |
| High School Graduate | 54 | 27 |
| University Incomplete | 49 | 24.5 |
| Missing Values | 24 | 12 |
| RELIGION | ||
| Christian | 46 | 23 |
| Kardecist Spiritist | 54 | 27 |
| Other (Jewish, Ecumenic, Seicho-no-iê, Hare-Krishna, Adventist of the Seventh-day, White Table Rituals, Wicca, Buddhist, Messianic, Jehovah’s Witness) | 17 | 8.5 |
| Prefer not to say/missing values | 83 | 41.5 |
| PRACTICE OF RELIGION | ||
| Organizational | 116 | 58 |
| No-organizational | 43 | 21.5 |
| Missing values | 41 | 20.5 |
| Factors and Items | Mean | SD | Correlation Item-Total | Alfa if Item Deleted | Factorial Loads | ||||
|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | ||||||
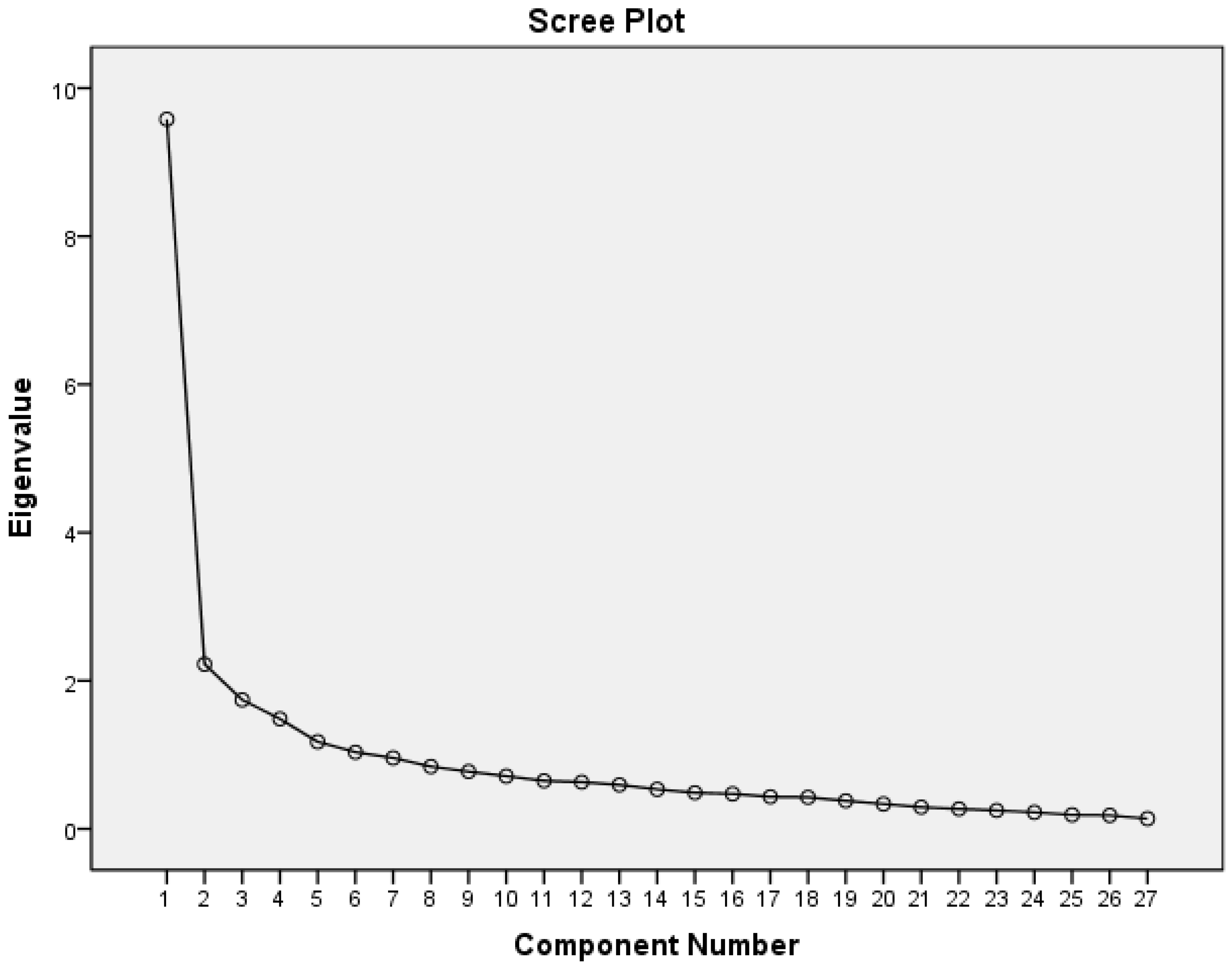
| 1—Religious Needs (eigenvalue 9.58; α = 0.887) | |||||||||
| N21 | Participate at a religious ceremony (e.g., service) | 0.95 | 0.98 | 0.569 | 0.925 | 0.836 | |||
| N23 | Turn to a higher presence (e.g., God, Allah) | 1.36 | 1.00 | 0.656 | 0.923 | 0.836 | |||
| N19 | Someone prays for you | 1.08 | 0.94 | 0.666 | 0.923 | 0.786 | |||
| N20 | Pray for yourself | 0.94 | 0.91 | 0.685 | 0.923 | 0.778 | |||
| N18 | Pray with someone | 0.62 | 0.81 | 0.656 | 0.924 | 0.639 | 0.335 | 0.330 | |
| N03 | Someone of your religious community (e.g., pastor) cares for you | 0.39 | 0.67 | 0.430 | 0.927 | 0.564 | 0.379 | ||
| N22 | Read religious/spiritual books | 0.63 | 0.89 | 0.545 | 0.925 | 0.523 | 0.519 | ||
| 2—Giving/Generativity Needs (eigenvalue 2.22; α = 0.848) | |||||||||
| N10 | Find meaning in illness and/or suffering | 0.60 | 0.85 | 0.540 | 0.925 | 0.692 | |||
| N11 | Talk about the question of meaning in life | 1.07 | 0.90 | 0.657 | 0.923 | 0.377 | 0.617 | ||
| N13 | Turn to someone in a loving attitude | 1.18 | 0.77 | 0.632 | 0.924 | 0.333 | 0.601 | ||
| N12 | Talk about the possibility of life after death | 0.75 | 0.97 | 0.559 | 0.925 | 0.438 | 0.595 | ||
| N17 | Be forgiven | 1.08 | 0.98 | 0.554 | 0.925 | 0.551 | |||
| N14 | Give away something from yourself | 0.98 | 0.82 | 0.510 | 0.323 | ||||
| 3—Inner Peace (eigenvalue 1.74; α = 0.813) | |||||||||
| N07 | Dwell at a place of quietness and peace | 1.78 | 0.77 | 0.501 | 0.926 | 0.837 | |||
| N08 | Find inner peace | 1.86 | 0.80 | 0.546 | 0.925 | 0.835 | |||
| N06 | Plunge into beauty of nature | 1.63 | 0.80 | 0.489 | 0.926 | 0.792 | |||
| N04 | Reflect your previous life | 0.99 | 0.86 | 0.440 | 0.927 | 0.387 | 0.469 | ||
| 4—Family Support Needs (eigenvalue 1.48; α = 0.778) | |||||||||
| N30 | Receive more support from your family | 1.09 | 0.73 | 0.543 | 0.925 | 0.302 | 0.722 | ||
| N25 | Feel connected with your family | 1.14 | 0.74 | 0.537 | 0.925 | 0.665 | |||
| N28 | Be inserted again on your family concerns | 0.38 | 0.68 | 0.418 | 0.927 | 0.325 | 0.649 | ||
| Factors and Items | Mean | SD | Correlation Item-Total | Alfa if Item Deleted | Factorial Loads | ||||
|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | ||||||
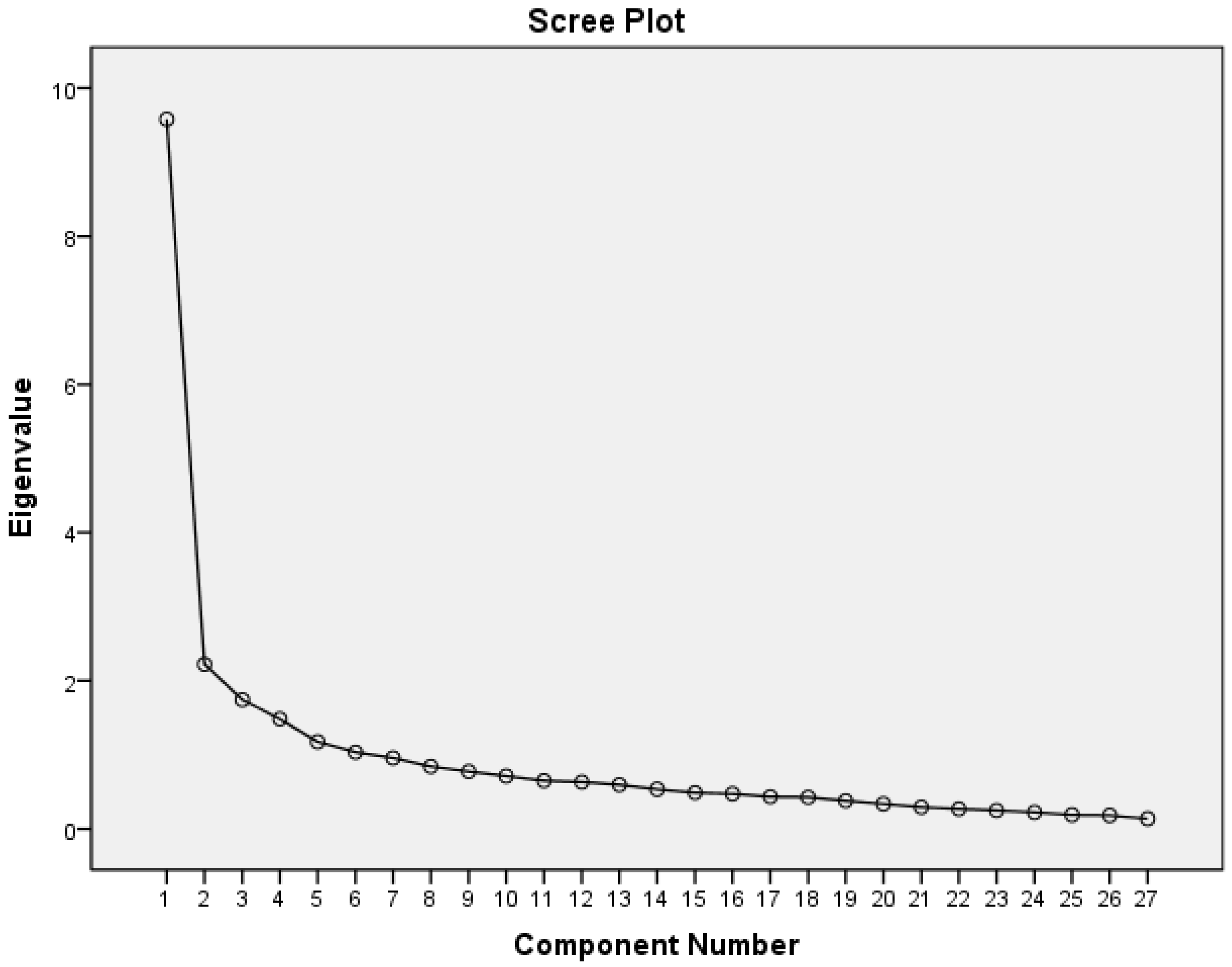
| 1—Religious Needs (eigenvalue 9.58; α = 0.892) | |||||||||
| N23 | Turn to a higher presence (i.e., God, Allah) | 1.36 | 1.00 | 0.680 | 0.908 | 0.809 | |||
| N21 | Participate at a religious ceremony (e.g., service) | 0.95 | 0.98 | 0.594 | 0.910 | 0.780 | |||
| N19 | Someone prays for you | 1.08 | 0.94 | 0.686 | 0.908 | 0.767 | |||
| N20 | Pray for yourself | 0.94 | 0.91 | 0.699 | 0.908 | 0.749 | |||
| N18 | Pray with someone | 0.62 | 0.81 | 0.668 | 0.909 | 0.594 | |||
| N03 | Someone of your religious community cares for you | 0.39 | 0.67 | 0.453 | 0.913 | 0.513 | |||
| 2—Existential Needs (eigenvalue 2.22; α = 0.834) | |||||||||
| N12 | Talk about the posibility of life after death | 0.75 | 0.97 | 0.556 | 0.693 | ||||
| N11 | Talk with someone about the question of meaning in life | 1.07 | 0.90 | 0.640 | 0.568 | ||||
| N22 | Read religious/spiritual books | 0.63 | 0.89 | 0.551 | 0.567 | ||||
| N10 | Find meaning in illness and/or suffering | 0.60 | 0.85 | 0.522 | 0.547 | ||||
| N13 | Turn to someone in a loving attitude | 1.18 | 0.77 | 0.610 | 0.527 | ||||
| N26 | Pass own life experiences to others | 1.00 | 0.81 | 0.673 | 0.415 | ||||
| 3—Inner Peace (eigenvalue 1.74; alpha = 0.876) | |||||||||
| N08 | Find inner peace | 1.86 | 0.80 | 0.515 | 0.819 | ||||
| N07 | Dwell at a place of quietness and peace | 1.78 | 0.77 | 0.484 | 0.813 | ||||
| N06 | Plunge into the beauty of nature | 1.63 | 0.80 | 0.485 | 0.727 | ||||
| 4—Family Support Needs (eigenvalue 1.48; alpha = 0.778) | |||||||||
| N30 | Receive more support from your family | 1.00 | 0.75 | 0.526 | 0.815 | ||||
| N25 | Feel connected with your family | 1.14 | 0.74 | 0.525 | 0.682 | ||||
| N28 | Be inserted again on your family concerns | 0.38 | 0.68 | 0.401 | 0.538 | ||||
| 5—Giving/Generativity Needs (eigenvalue 1.17; α = 0.821) | |||||||||
| N16 | Forgive someone from a distinct period of your life | 0.95 | 0.92 | 0.482 | 0.913 | 0.759 | |||
| N17 | Be forgiven | 1.08 | 0.98 | 0.545 | 0.912 | 0.736 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valente, T.C.d.O.; Cavalcanti, A.P.R.; Büssing, A.; Costa Junior, C.P.d.; Motta, R.N. Transcultural Adaptation and Psychometric Properties of Portuguese Version of the Spiritual Needs Questionnaire (SpNQ) Among HIV Positive Patients in Brazil. Religions 2018, 9, 135. https://doi.org/10.3390/rel9040135
Valente TCdO, Cavalcanti APR, Büssing A, Costa Junior CPd, Motta RN. Transcultural Adaptation and Psychometric Properties of Portuguese Version of the Spiritual Needs Questionnaire (SpNQ) Among HIV Positive Patients in Brazil. Religions. 2018; 9(4):135. https://doi.org/10.3390/rel9040135
Chicago/Turabian StyleValente, Tânia Cristina de Oliveira, Ana Paula Rodrigues Cavalcanti, Arndt Büssing, Clóvis Pereira da Costa Junior, and Rogerio Neves Motta. 2018. "Transcultural Adaptation and Psychometric Properties of Portuguese Version of the Spiritual Needs Questionnaire (SpNQ) Among HIV Positive Patients in Brazil" Religions 9, no. 4: 135. https://doi.org/10.3390/rel9040135
APA StyleValente, T. C. d. O., Cavalcanti, A. P. R., Büssing, A., Costa Junior, C. P. d., & Motta, R. N. (2018). Transcultural Adaptation and Psychometric Properties of Portuguese Version of the Spiritual Needs Questionnaire (SpNQ) Among HIV Positive Patients in Brazil. Religions, 9(4), 135. https://doi.org/10.3390/rel9040135