1. Introduction
Spirituality, as a dimension of health and health care, has not fitted well in the usual rational or objective medical paradigm that focuses on the physical demands of illness and treatment (
Rumbold 2003). Spiritual health disorders often remain unrecognized due to the lack of healthcare professionals’ knowledge and preparation to meet those requirements, or no attention at all being paid to the spiritual health domain (
Valiuliene 2013).
Despite a high emphasis on spirituality in patients‘ health and nursing care, deliberation about what spirituality is, by a personal and professional understanding of health care specialists, and how it has to be recognized, assessed, and provided for those seeking it, continues. It may be an expression, framework, source of, or searching for, transcendent meaning to life (
Ferrell et al. 2003;
Puchalski et al. 2009). It may be immediate experience or reactions to life (
Lazenby 2010), or it may be the way people “experience their connectedness to the moment, to self, to others, to nature, and to the significant or sacred” (
Puchalski et al. 2009, p. 887).
Stern and James (
2006) compiled a framework, from the point of view of relationships, to exemplify spirituality. This includes the continuum of relationships, ranging from that with self, to others, and the whole world, including God, gods, or nature. This broad view, as the authors’ suggested, underscores the ambiguity of spirituality, which then forces nurses to consider the full realm and intensity of beliefs and practices, rather than oversimplifying or dismissing them.
Lithuanians have a deep and complex history around spiritual expression (
Riklikiene et al. 2016,
2018), which may impact their experience of health and well-being, as well as comprehension of links between spirituality and religiosity. In a country in which Christianity is largely practiced, spiritual matters are closely associated with religion and the practice of faith among healthy or ill people, their relatives and health care professionals. Many people express their spirituality in religious practice, possibly because religion also provides a searching for transcendent meaning, but in a particular way, generally on the basis of belief in a deity. Thus, although not everyone has a religion, everyone who searches for ultimate or transcendent meaning can be said to have a spirituality (
Sulmasy 2002). Simply put, and for the purposes of this study, spirituality is reflected through the meaning or purpose that one individually ascribes to life.
Spiritual health is a fundamental dimension of people’s overall health and well-being, permeating and integrating all the other dimensions of health (i.e., the physical, mental, emotional, social, and vocational). Spiritual health/well-being is understood as a dynamic state of being that is reflected in relationships in four areas, namely with self, others, environment, and/or Transcendent Other (
Fisher 2012).
Nursing tradition goes beyond the medical to integrate physical, mental, social and spiritual dimensions of patients’ lives in care. This holistic paradigm guides nurses towards a careful assessment of a spiritual dimension of human beings, recognizing the fact that expression of any form of spirituality has strong cultural underpinnings. A traditional approach toward spiritual matters affects familiarity of terminology used by a population, adoption, and comprehension of novel concepts, recognition of patients’ spiritual issues as targets for health care providers, finally, the readiness and comfort of individuals to discuss their spiritual health concerns with others unreservedly. Nurses’ understanding of spiritual health domains contributes to the quality of spiritual care and overall care delivery.
To date, there have been no measures and validated tools of spiritual well-being for use with healthy or illness-affected Lithuanian people. This paper reports the translation and validation of the Spiritual Well-Being Questionnaire called SHALOM for its use with Lithuanian respondents regarding self-assessment of spiritual health and needs for spiritual support. The title of the instrument SHALOM was chosen to represent the very essence of Spiritual Well-Being (SWB). The Hebrew word
Shalom means “completeness, wholeness, health, peace, welfare, safety, soundness, tranquillity, prosperity, fullness, rest, harmony, the absence of agitation or discord.” (
Strong 1979). The acronym SHALOM reveals its two components—Spiritual Health Measure (SHM) and Life-Orientation Measure (LOM). The LOM elicits the ‘ideals’ that people have for Spiritual Health in four sets of relationships with self, others, environment, and/or God. The SHM asks people to reflect on ‘lived experience/how they feel each item reflects their personal experience most of the time’ (
Fisher 2010).
The purpose of our study was to psychometrically test a translated and validated Lithuanian version of the Spiritual Well-Being Questionnaire SHALOM in non-terminally ill hospitalized oncology patients. This article also provides the primary results on the state of spiritual well-being and its relationship with sociodemographic factors in hospitalized non-terminally ill oncology patients.
2. Material and Methods
2.1. Study Design and Methods
A descriptive, multisite, cross-sectional survey design was employed for this study. A face-to-face individual interview method was employed to investigate the spiritual well-being of non-terminally ill oncology adult patients hospitalized in nursing care and oncology units of a tertiary level hospital in one of the largest city of Lithuania.
2.2. Field Testing
The study sample consisted of patients that were diagnosed with an oncology disease and undergoing treatment at an oncology unit. Before data collection, the principal reseacher provided sufficient consultations with the interviewers regarding instructions for completing the instrument, the specific language, and the meaning of terms. The researcher and her assistant (last year student of a university nursing program) visited the hospital and introduced the study to nurse managers at the units. The managers directed the researchers to patients that met the inclusion criteria: oncology illness diagnosed, non-terminal phase of the disease, patient is conscious, able to understand the informed consent, and to answer the questions. During face-to-face interviews, trained interviewers (oncology nurse and final year bachelor of nursing student) administered the questionnaire on a one-to-one basis, at the most convenient time for patients, in a calm and private place, for an average duration of 5–10 min, depending on the health status and the age of the respondent.
2.3. Participants
Responses were obtained from 171 patients in nursing and supportive treatment units at public hospitals. Response rate was 100% because of the face-to face interview method that was applied for the survey. The results are therefore not necessarily representative of the institutions surveyed.
There were more female patients (55.6%) than male. The age of patients varied from 25 years to 96 years, mean age was 65.82 ± 12.15 years. Most of the patients (N = 140) were affiliated with the Roman Catholic religion (95.9%), two (1.4%) patients were Russian Orthodox, and three (2.1%) were Old Believers (
Table 1). The duration of chronic disease varied from one month to 59 years (mean 3.98 ± 3.33).
2.4. Study Instrument
After written permission for SHALOM translation and validation into Lithuanian was granted by the author, Fisher’s Spiritual Health And Life-Orientation Measure (SHALOM) was used for the study (
Fisher 2010). The 20-item questionnaire sought two responses to indicate: (1) patients’ ideals for SWB where participants rate the importance of each item for their optimum spiritual health as well as (2) the lived experience where participants rate how they feel each item reflects their personal experience most of the time. Comparing these two responses provides a measure of spiritual harmony or dissonance in each of the four domains of SWB. The set of sociodemographic characteristics was collected using an investigator-developed form.
2.5. Procedures
The SHALOM questionnaire was forward-translated into the Lithuanian language and back-translated into English following the methodological considerations for double translation and reconciliation (
Maneesriwongul and Dixon 2004). A nurse educator and nursing student were invited, as two native, local culture and language translators, to make the initial translation of the instrument from the original, English, language to the target language—Lithuanian. An in-depth knowledge of culture, English language proficiency and confidence in health care practice was essential for maintaining cultural equivalence of the translated items and concepts. Later, both of the translated Lithuanian versions were compared and a consensus reached during group conversation with a third translator—a nursing professor with fluent knowledge of English, rich clinical experience, as well as competence of subject matter and knowledge of instrument development/translation/adaptation principles. Afterwards, the back translation of the newly translated version of SHALOM was conducted by English language specialists, for identification of errors in meaning of terms, concepts and constructs, before validity and reliability testing of the new version of SHALOM (
Jones et al. 2001). During the translation and adaptation processes linguistic, psychological, and cultural differences in the Lithuanian population and peculiarities in health care practices were considered through the choice of experts with relevant expertise, e.g., spiritual services, knowledge of anthropology, and proficiency in Lithuanian language. The equivalency checking between the original and translated versions of the instrument was accomplished by the author (J. Fisher), following the three level congruence structure that was defined in advance by the researchers. Any discrepancies were corrected seeking greatest agreement. During the translation procedure the Lithuanian language style, syntax, and grammar were corrected several times. Field validation of the SHALOM-Lithuanian version was conducted with hospitalized oncology patients in November 2017–February 2018.
2.6. Ethical Considerations
The Lithuanian Regional Committee on Bioethics issued permission to conduct the study (5 December 2017, No. BE-2-84). Participants received written and oral information about the aim of the survey and gave their informed consent by participating in the face-to-face interview. Data confidentiality was guaranteed by no identifying information being recorded on answers.
2.7. Statistical Analysis
Data were recorded and analyzed using the Statistical Package for Social Sciences (IBM SPSS Statistics) version 22.0. Descriptive statistics and parametric tests for two and more than two independent samples (
t-test and One-Way ANOVA with post hoc Tukey multiple comparisons) were used. We used Paired samples
t-test to compare spiritual dimensions’ mean scores between the Ideals and Lived Experience sections. A
p-value of 0.05 or less was used to define statistical significance. To assess the psychometric properties of the scale, Cronbach’s alpha, split half test, average inter-item, and item-total correlations were calculated for internal consistency. Cronbach’s alpha coefficient was calculated for both individual domains and the whole scale in two sections; internal consistency that exceeds α 0.6 was considered to be acceptable (
Bland and Altman 1997). Test-retest was conducted with 28 student nurses, with an interval of one week, and construct stability-in-time was tested using Spearman-Brown coefficient; the value of 0.80 and above identified adequate construct stability, or 0.90 and above—good construct stability of the instrument (
Kaplan and Saccuzzo 2001). Items scoring below 0.15 have poor inter-item correlations, suggesting that they are really not that well related to each other. Items that correlate above 0.50 tend to be very similar to each other.
An exploratory factor analysis was used to confirm the construct validity of the translated version of SHALOM. Principal Component Analysis with Varimax rotation was applied. The Kaiser-Meyer-Olkin and Bartlett’s Test of Sphericity were used to assess the appropriateness of the sample for the factor analysis. Eigen values of above one and the scree plot were used to determine the number of factors.
3. Results
3.1. Face and Content Validity of the SHALOM Lithuanian Version
A specific language constitutes a symbolical expression of tradition and culture of a particular geographical territory. Lithuanian language is related to Latvian and dead Prussian, and it is the Eastern Baltic language with the highest number of users. Lithuanian, as a separate branch of Eastern Baltic languages, started to be developed from the VIIth century. The oldest known Lithuanian script—“Tractatus sacerdotalis“—originated at the begining of 1600s. The strong roots of the Lithuanian language have led to it retaining ancient grammar forms and morphology and, from a linguistic perspective, it is as worthy to study as Latin or ancient Greek. Lithuanian grammar is very similar to all ancient Indo-European language forms and even older language forms. The Lithuanian language has the greatest resemblance to its archaic forms than any other Indo-European language in use.
SHALOM was developed in the belief that an instrument should have appropriate language and conceptual clarity for studies of Spiritual Health within general populations and individuals. Homogeneity of cultures usually results in separate linguistic systems, whose identity rests on a typical, essential for a given language, grammatical and intonation system and lexical resources. The advantage of SHALOM relates to its construction of items. The instrument lists the items in a very short form using a single or a few words—not a sentence. That is much easier for ill patients to get the sense of what is being asked rather than listening to long sentences.
During the translation process, primary attention was assigned by the researchers to instrument applicability and comprehensiveness. Expressions such as awe at a breathtaking view, peace with God, prayer life, meaning in life, kindness towards other people and a sense of ‘magic’ in the environment were difficult to find culturally and linguistically appropriate equivalents, that would be familiar to the general public. Consultations between the Lithuanian researchers and the author of SHALOM (J. Fisher) provided a wider exploration of meaning, which led to an accurate interpretation and avoidance of semantic errors, during the translation process. Achievement of equivalency and congruence was achieved when the authors of SHALOM made a comparison of both English versions: original and back translated, providing comments on discrepancies and their corrections.
The conversational manner of the data collection enabled interviewers to obtain criticisms of the Lithuanian version of SHALOM itself. The field notes and the oral feedback from interviewers revealed the fact that younger patients of better health status and no feeling of pain were easier to interview. Those respondents who experienced difficulty concentrating well enough on the items, because of their weak condition, noticed the repetition of rather similar aspects and had difficulty distinguishing between them. It was also noted by interviewers that for older, and usually rural, respondents, the items sense of ‘magic’ in the environment, connection with nature, harmony with the environment appeared strange as they had never given thought to this. American English terms and combinations a sense of identity, self-consciousness, oneness with nature, inner peace, meaning in life were rather novel for older Lithuanians. A patient of an oncology unit asked the interviewer to explore the meaning of those concepts. The reflection from the interviewers was that respondents nearly always associated spirituality with religiosity.
To test the face validity of the Lithuanian version of the SHALOM, the clarity of the instrument, firstly, was discussed in a group with the student nurses (N = 28), who participated in a test-retest study. To ensure that item content had similar meaning for the intended population, the pilot testing of the instrument was conducted with non-terminally ill oncology hospitalized patients during the first two weeks of the survey. Additional minimal corrections were incorporated in response to the interviewers‘ comments and suggestions.
3.2. Field Testing of the Lithuanian Version of SHALOM
To prove that the Lithuanian version of SHALOM measures the spiritual well-being concept in reproducible fashion, a set of tests were employed to assess the psychometric properties of the the newly translated instrument.
Internal consistency. The four domains of two SHALOM sections (SHALOM-Ideals and SHALOM-Lived Experience) had Cronbach’s alpha (α) values ranging from 0.578 to 0.949. The Personal domain in both sections had the lowest values of alpha in relation to other domains (
Table 2).
Item-total correlations were inspected for the five items in each of the four domains comprising SHALOM. For the Personal domain, the corrected item-total correlation ranged from 0.238 to 0.632 in the SHALOM-Ideals section and from 0.167 to 0.440 in the SHALOM-Lived Experience section; the item-total correlation of this domain was the lowest in comparison with the other three domains. For the Transcendental domain, the corrected item-total correlation was the strongest and ranged from 0.806 to 0.911 in the section for Ideals and from 0.782 to 0.871 in the section of Lived Experience (
Table 2).
Stability in time. Test-retest correlation with seven days interval showed good construct stability of the SHALOM Lithuanian version. The correlation (Spearman-Brown coefficient) between the responses of the two surveys was 0.927 on Ideals and 0.942 on Lived Experiences.
Average inter-item correlation was calculated. In the Personal domain of Ideals, the correlation coefficient ranged from 0.009 to 0.609; the Communal domain correlation coefficients ranged from 0.525 to 0.731; in the Environmental domain—0.35–0.738 and in the Transcendental domain correlation coefficients varied from 0.721 to 0.871. The inter-item correlation in Lived Experiences section was: in the Personal domain from 0.096 to 0.538, in the Communal domain from 0.369 to 0.538, in the Environmental domain from 0.278 to 0.711 and in the Transcendental domain inter-item correlation ranged from 0.679 to 0.821.
Construct validity. The goal of factor analyses was to confirm the equivalence of the structure of the SHALOM Lithuanian version. The Kaiser-Meyer-Olkin (KMO) values indicated that data and sample size were adequate for factor analysis. Moreover, the approximate Chi-square values of Bartlett’s test of sphericity confirmed that the factor model is appropriate. These two tests showed the suitability of the respondent data for exploratory factor analysis, which was performed on the 20 Ideal and Lived Experience items using the principal component factor analysis with Varimax rotation.
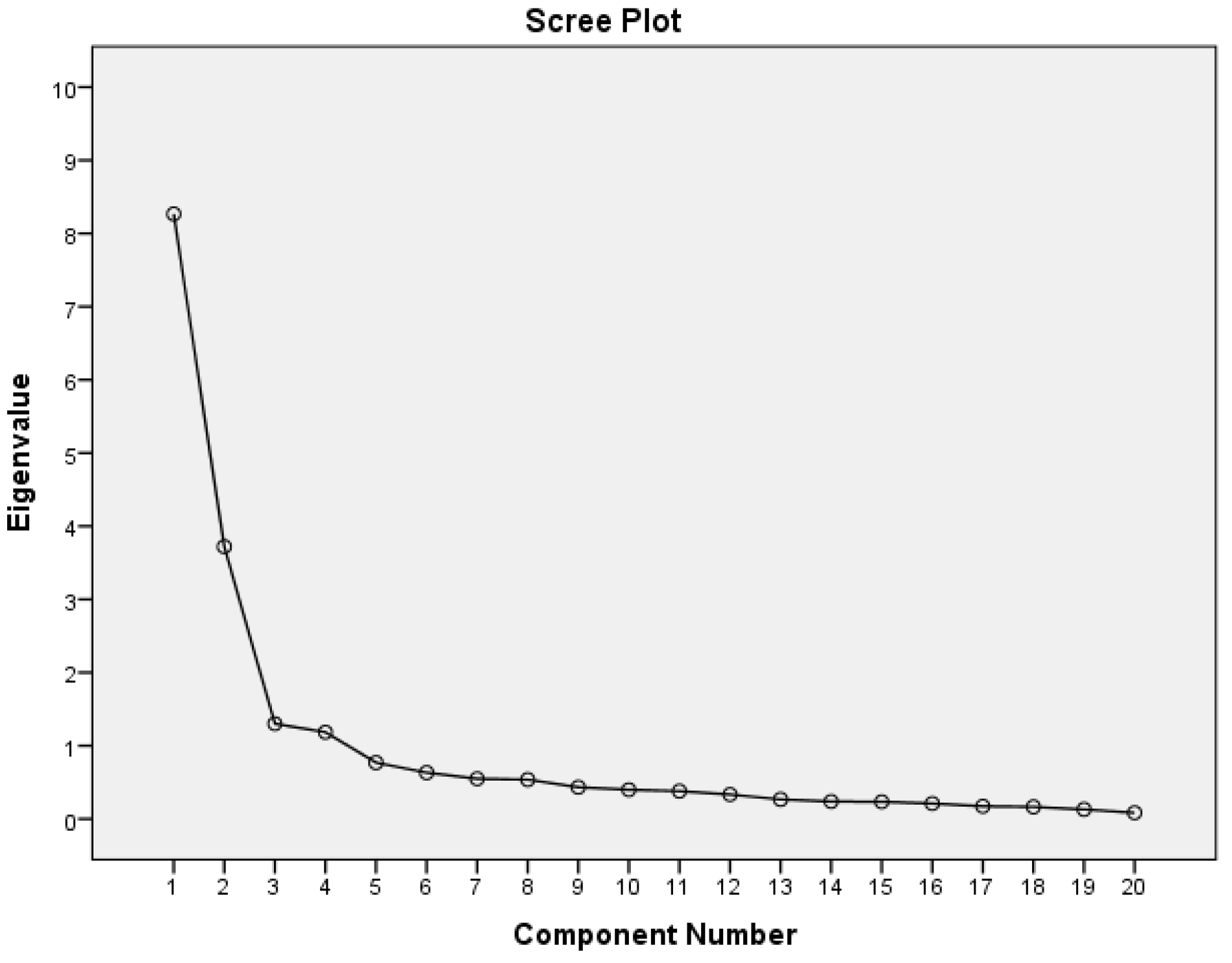
Following the Varimax rotation, the Ideals items loaded significantly on four factors. These four factors had an eigenvalue greater than 1 with an explained variance of 72%. All of the items had a loading range higher than 0.5, above the minimum acceptable value of 0.4. The first factor was related to the communal (1, 3, 8, 17, 19)/personal (9, 14, 16) SWB with one additional item (12) from environmental SWB. The second factor related to the transcendental dimension of SWB and the third factor was for environmental SWB; the fourth factor was associated with personal SWB (
Table 3,
Figure 1).
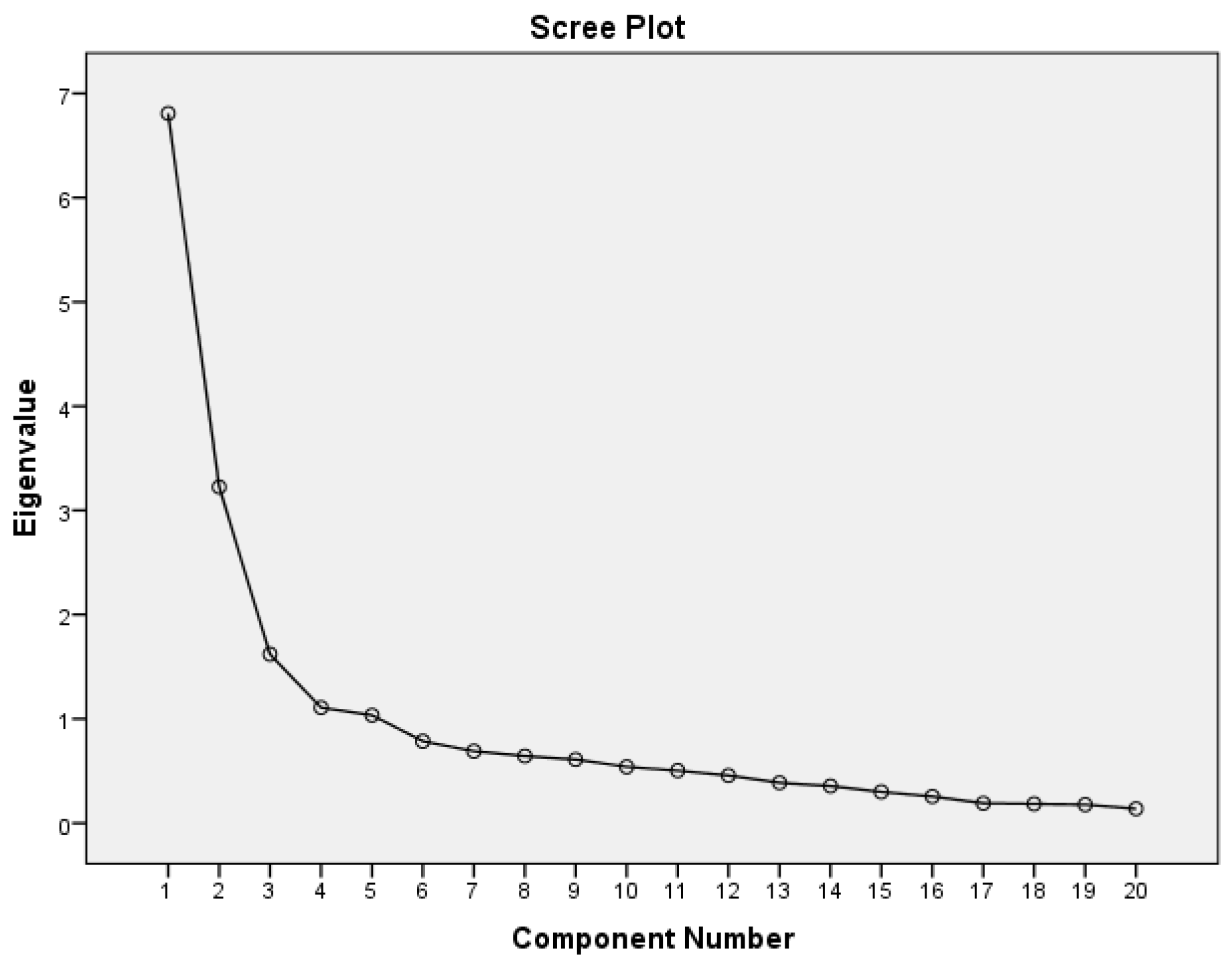
As shown in
Table 3 and
Figure 2, the five factors that reported a eigenvalue greater than 1, accounting for 69 % of variance, were extracted in the section of Lived Experience. Factor 1 and factor 2 items in Lived experience section were consistent with the factor 2 and factor 3 items in the Ideals section and corresponded with the environmental and transcendental domains of the original version of SHALOM. In accordance to factorisation, in Lived experience, factors 4 and 5 together make up/comprise the Personal domain. The results on other domains fit the normal pattern quite well.
3.3. Spiritual Well-Being of Non-Terminally Ill Hospitalized Oncology Patients
The results revealed that summative scores of the domain and the mean scores of each item on Ideals were significantly higher than the same domain and the same item on Lived Experience section. Communal domain of spiritual well-being in both of the sections had higher mean scores than the three other domains (
Table 4).
According to
Fisher (
2006), spiritual dissonance is indicated by a difference in mean value of greater than 1.0 between the ‘ideal’ and ‘lived experience’ in any domain of SWB. The result on all four domains of the SHALOM scale indicated limited spiritual dissonance in the Personal domain (
n = 20, 11.7%), Communal domain (
n = 12, 7.0%), Environmental domain (
n = 6, 3.5%), as well as the Transcendental domain (
n = 6, 3.5%).
The scores on each scale of a SWB measure were compared in relation to the sociodemographic characteristics of respondents. The results on Ideals and Lived Experience sections revealed significant differences on two domains of SWB in accordance with patients’ gender: females rated the environmental and transcendental domains more highly than males; on Lived Experience sections the gender difference was additionally determined on the Communal domain. Place of residence was significant for the respondents in assessing the transcendental domain in both sections: the rural respondents rated the items of Ideals and Lived Experience more highly than urban residents. Those respondents who were not able to identify their religiosity rated the items of the transcendental domain of both SHALOM sections lower in comparison with religious but higher in comparison with non-religious respondents. In addition, the communal domain of Lived Experience was rated higher by religious respondents than the non-religious. Scoring of the transcendental domains of both sections, and the communal domain of Ideals, were significantly related to patients’ age (
Table 5 and
Table 6).
The marital status showed no difference on ratings of both sections of SHALOM. No significant difference was shown in Ideals items in relation to the education level of respondents, but the Lived Experience of the transcendental domain was scored significantly higher by those with primary education than those with secondary (
Table 5 and
Table 6).
4. Discussion
It is evident that the development of proper measures and methods to assess subjective attributes, including spiritual well-being, as such, is a complex task and time consuming activity that requires considerable human, technical, and financial resources. Keeping in mind that no instrument can give an absolute measure of spiritual well-being (
Fisher 2016) and by realistically estimating all of the effort required, and challenges to develop an adequate new measure, we decided to make a critical review of the evidence and to find the most appropriate instrument for our study’s aims and research perspectives in the area of spiritual well-being of ill and healthy people. We chose the Spiritual Health And Life-Orientation Measure (SHALOM) relying on the review results of
de Jager Meezenbroek et al. (
2012), with recognition that the multidimensional Spiritual Well-being Questionnaire (SWBQ) from
Gomez and Fisher (
2003) is promising for measuring spirituality as an experience or attitude that transcends any particular religion. The Spiritual Well-Being Questionnaire (SWBQ) is the ‘lived experience’ component of SHALOM (
Gomez and Fisher 2003). This questionnaire has the advantage that it can be used among people who adhere to a faith or no faith at all. This is a strong argument, as our intention for this study was, and for further studies will be, to assess spirituality as a universal phenomenon, not excluding people on the basis of their religious background.
The Lithuanian version of SHALOM demonstrated high comprehensiveness and adequate psychometric properties of the instrument. Assessment of the ‘linguistic and cultural distance’ between the source and target language and cultural groups (
van de Vijver and Leung 1997) might include the considerations of differences in language, religion, lifestyle, and values. Such distance is obvious between Western countries and Lithuania in speaking about the developments of health care models, professional competences and scope of practice of medical staff, a history of freedom of thoughts, faith, and human rights. To maximize the cultural suitability of the instrument to the Lithuanian population, the wording of particular items, which were novel or not very familiar to Lithuanians (especially to older populations), should be further tested and modified to feel much more natural and be acceptable, with functional, rather than literal, equivalence. The additional consideration of appropriate Lithuanian terms for ‘identity’, ‘self-confidence’, and ‘inner peace’ is feasible and is recommended.
It is assumed that the response to any one question is subject to error: the person may misinterpret the item, respond in a biased manner, or to make a mistake in transcribing the reply to the answer sheet (
Streiner and Norman 2009). In our study the effect of these errors was minimized by the selection of a conversational approach with respondents being questioned via face-to-face interviews by an experienced researcher or final year nursing student, as a part of her final thesis on the topic. Thus, the interviewer was able to determine if the respondent had any difficulty in understanding any items because of older age, limited intelligence, lower health literacy, problems in concentration because of illness and weak health status, or whether due to unfamiliar terms of spirituality language. Interviewers reflected that they often were asked to rephrase particular questions for better understanding.
In addition to the primary aim of this study, which was to translate and to validate the Spiritual Well-Being Questionnaire SHALOM in Lithuanian language and culture, a field test also provided results on spiritual well-being of non-terminally ill hospitalized oncology patients. These results are preliminary and confirmation of them by a larger scale study will follow. This paper reports on the main tendencies. The Communal domain of spiritual well-being, representing the individual’s relationship with others, revealed the highest mean score and Transcendental domain the lowest. Significant differences were found between respondents’ Lived experiences and their Ideals. Gender plays a significant role for the sense of spiritual well-being of non-terminally ill oncology patients, with females perceiving their relationship with others, with the environment and with a Transcendent Other, to be better than males, as indicated by more highly-scored responses.
Importantly, the place of residence was significant for the respondents in assessing the Transcendental domain, where individuals from rural areas reported a better relationship with a higher power when compared with the urban population. In addition, patients without a clear identification of their religiosity assess the transcendental domain of spiritual well-being lower in comparison with the religious, but higher in comparison with non-religious, respondents. In addition, the communal domain of Lived Experience was rated higher by religious respondents than non-religious.
The Lithuanian version of SHALOM was translated and validated for its further use in larger scale research studies on terminally ill hospitalized oncology patients and for cross-cultural comparisons, which may be valid only if the same questionnaire is understood in the same way across language and cultural groups. In perspective, the instruments will be applied to other samples as well: student nurses, nurse educators, family caregivers to investigate their spiritual well-being and link it with other influential factors, such as sociodemographic characteristics, religion affiliation, satisfaction with life, happiness, and spiritual needs. Furthermore, qualitative evidence collection from healthy and ill persons, care-providers, and experts would help to clarify the construct of spiritual health/well-being and to know exactly what sense it makes in Lithuanian culture. Deeper understanding of concepts’ interpretation would enable us to minimize the influence of any cultural and linguistic differences that are irrelevant to the Lithuanian uses of the SHALOM.
The process that was used to validate this Lithuanian version of SHALOM has some limitations. Firstly, the instrument requires evidence for its concurrent validity, by comparing the findings with data from other sources and applying congruent or divergent measurement tools. Secondly, the Lithuanian version of SHALOM was only used with one homogenous sample. More variety would be advisable. Thirdly, the face-to-face interview method that was employed during the validation process has to be taken into consideration in making overall conclusions about the reliability of newly adapted instrument. Repeated testing of psychometric properties is recommended for data collected by other means, such as independent responding.






{kind=link}
{kind=link}